
Abstract
When a patient presents with eye trauma, it can be a daunting prospect for the GP, particularly with the potential risks, including of irreversible sight loss. It may be tempting to send patients to the nearest eye emergency service when hearing the patient's presenting complaint. This is understandable given limited access to ophthalmic equipment in primary care, including, for example, a slit lamp or even a working ophthalmoscope. However, taking a relevant and accurate history with a subsequent focussed examination to assess the extent of damage is both useful and vital to ensure the patient is seen by the ophthalmologist within the appropriate timeframe. However, for some types of eye trauma, such as chemical burns, it is best to treat in tandem with history taking.
Clinical case scenario
Margaret is a 58-year-old female woman who presents to her GP with sudden onset of left eye pain, which started approximately an hour ago. She has an associated foreign body sensation, excessive lacrimation, and blurry vision in the same eye. Her right eye is unaffected. She denies any symptoms of discharge and this is the first occasion she has experienced any such ocular symptoms. She also reports a significant gritty sensation in her left eye, as if there is something inside it. She denies any direct injury to her eye. Upon further enquiry, she recalls pruning the hedge in her garden earlier that morning and states that she had to use a ladder to reach the leaves of the tree above her. She wonders whether something might have fallen into her eye. She had a routine eye test a month ago and, other than a small change in her reading glasses prescription, there are no other eye health concerns. She has no significant medical history and is not on any regular medication. She denies any allergies. She expresses concerns that she may have developed a cataract like her mother.
Basic eye anatomy
To enable us to view our surroundings, light reflects off an object and into the eye. The light rays travel through the cornea, the outermost transparent layer covering the iris and pupil, and pass through the inner eye structures, with the pupil acting as a keyhole, coming to a focus on the retina. The photoreceptors of the retina capture the light rays and convert them into electrical signals. These signals are subsequently carried to the brain via the optic nerve (see Fig. 1).
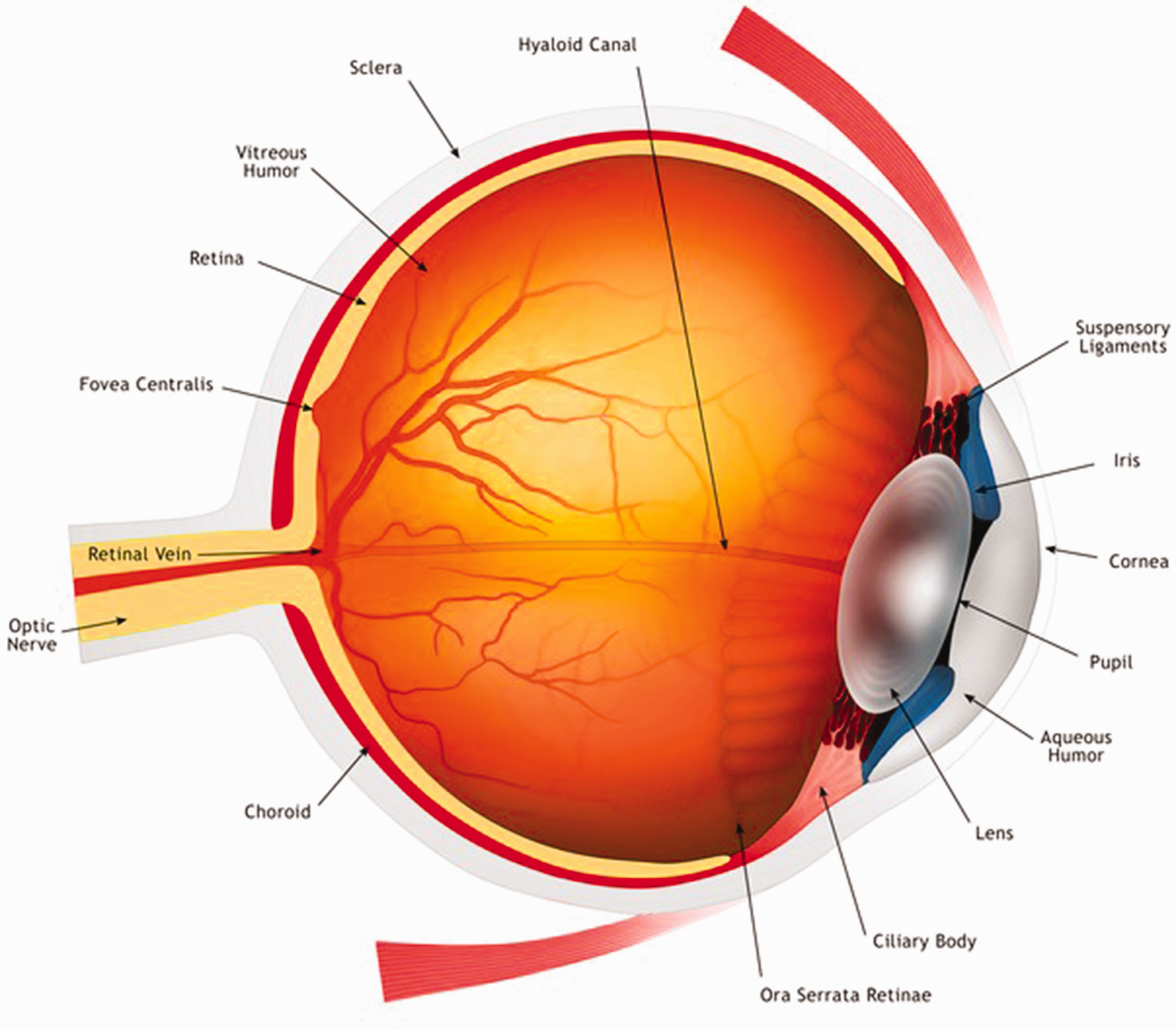
Basic anatomy of the human eye.
History taking
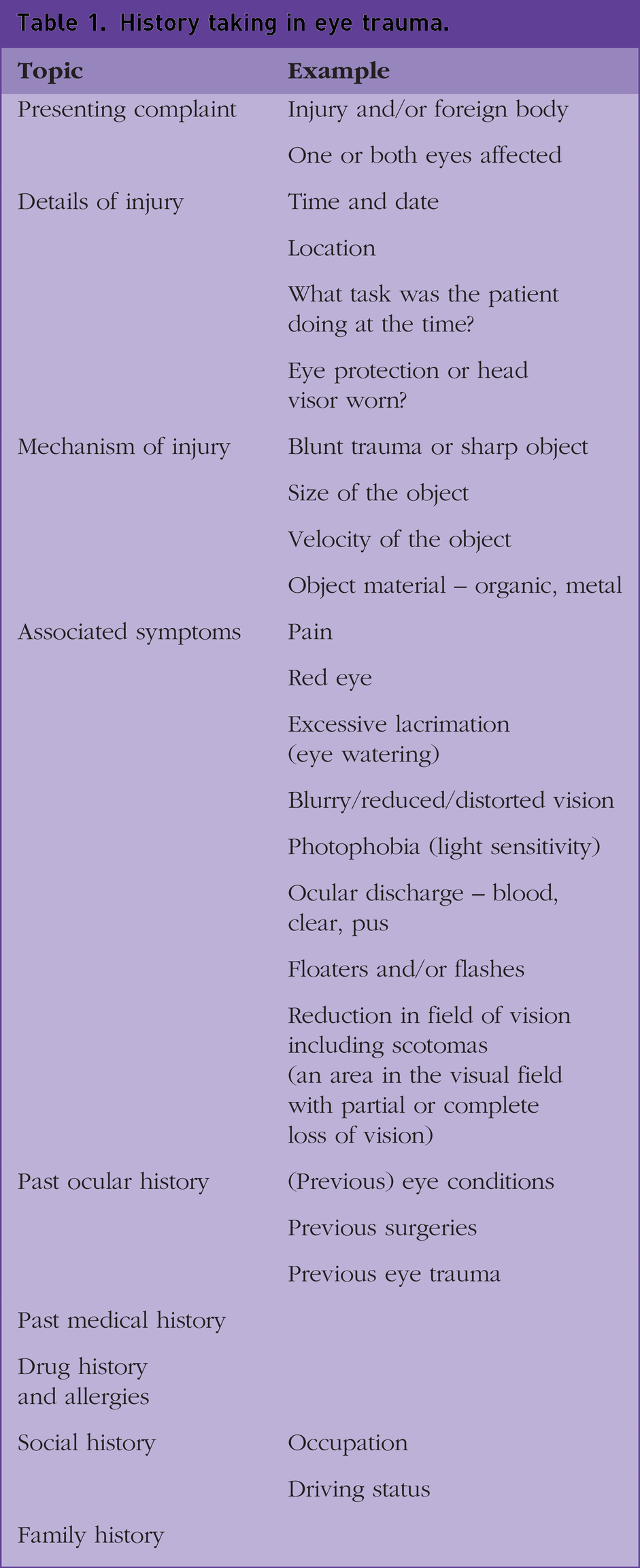
Like any history, take a structured approach with a particular emphasis on the details of the injury (Denniston and Murray, 2018), as in Table 1. This will help determine the extent of damage, aid your examination, and ensure you refer appropriately.
History taking in eye trauma.
Examination and investigations
Direct observation
Clinical observation is crucial in ophthalmic examination. The eye needs to be observed using a bright light source (torch, lamp, or ophthalmoscope) or as much as the patient can tolerate. Do not just view the eye itself, look at all the structures of the outer eye including the eyelids.
Visual acuity
Use the classic Snellen chart to record a patient’s visual acuity (VA). First test without the patient’s glasses then test with them. Each eye is tested separately. The standard testing distance for the Snellen chart is 6 m and you record the VA using the number at the side of the chart. The top line at the top of the chart is recorded as 6/60, which means that at 6 m (numerator) the patient is able to read the letter that a patient with ‘good’ vision can read at 60 m (denominator). 6/6 is considered ‘good vision’. If the patient is unable to read the top line at 6 m, then reduce the testing distance down to 3 m, followed by 2 m, then 1 m. If the patient is unable to see the top line at 1 m, measure the testing distance in cm thereafter. If the patient is unable to read any letters, then measure VA by counting fingers. If the patient is unable to do this, then ascertain if the patient can detect hand movements by waving the hand near the patient’s face. If not, then shine a light into the patient’s eye (via a pen torch) to see if there is light perception. If the patient is unable to see the light, then their VA is classed as ‘no light perception’.
Confrontation visual field testing
This is a very gross test to check for visual field defects. Position yourself 1 m in front of the patient and at the same eye level. Each eye is tested separately, so ask the patient to cover one eye and you, as the examiner, will cover your own eye on the same side (patient’s right eye and examiner’s left eye). Ask the patient to continue looking at your uncovered eye. Then divide the visual field into four quadrants and place your hand in each quadrant, holding up different numbers of fingers in each quadrant. Ask the patient to tell you how many fingers you hold up in each quadrant. Then test the other eye. The visual field may be affected if the patient suffers from blunt eye trauma and possibly a retinal detachment.
Ophthalmoscopy
Using an ophthalmoscope, turn the light source onto the brightest setting or as much as the patient allows. At approximately 10 cm testing distance, use the focussing lenses inside the ophthalmoscope to bring the structures of the outer eye into focus, including the sclera, cornea, iris, and pupil. Assess for any structural abnormalities and or discharge coming from the eye. To view the inner structures of the eye, shine the light through the patient’s pupil, slowly change the power of the focussing lens and slowly reduce the testing distance from 10 cm. As you do this, you will be able to observe the crystalline lens, vitreous humour and finally the retina and optic nerve. To view the retina and optic nerve effectively, the testing distance is usually between 2 and 5 cm. Some patients have very small pupils and shining a light into their eye can lead to reflections which can hinder your view so dilate the eye using topical eye drops (such as tropicamide) where appropriate.
Slit lamp examination
It is a technique that is becoming more commonplace as it provides a three-dimensional view of the eye, has a greater field of view and better magnifying properties compared to ophthalmoscopy. To complete the examination, you will need a slit lamp microscope (usually seen in many Emergency departments) and a hand-held slit lamp lens (which comes in various powers). Compared with ophthalmoscopy, it is technically more difficult to master this examination technique, but it is much more valuable in assessing the eye. Even without the hand-held slit lamp lens, the slit lamp is a brilliant tool to enable effective observation of the outer eye and the wider light beam is particularly useful for locating foreign bodies either on the eye surface or on the inner side of the eyelids.
Fluorescein eye staining
This is a particularly useful test to assess for corneal damage or to locate foreign bodies. It is performed in conjunction with the slit lamp examination. Before conducting this test, check if the patient has any allergies particularly to contrast (i.e. during angiography). Then place one to two drops of topical fluorescein sodium 1% in the eye to be examined. This dye is orange in colour and will stain the outer eye orange for a very short period of time. Then ask the patient to blink a few times to distribute to dye over the ocular surface. Switch the light settings of the slit lamp to blue light (cobalt blue filter) and ask the patient to look straight ahead when positioned at the slit lamp. Foreign bodies or corneal damage are easier to locate with this test as they will show up as fluorescent green as you look through the microscope. Ophthalmoscopes also have a built-in cobalt blue filter in order to do this test as well.
Clinical case scenario continued.
You assess the visual acuity of each eye separately using the Snellen chart and it is 6/6 in the right eye and 6/9 in the left eye. Upon examination of her left eye with the ophthalmoscope, the conjunctiva appears erythematous and there is excessive lacrimation of the eye. She struggles to tolerate the bright light of the ophthalmoscope during examination. There is no blood or pus-like discharge coming from the eye. You evert the upper and lower eyelid and find no abnormalities. The retina and optic nerve look otherwise healthy. The right eye appears healthy as well. Confrontation visual fields do not elicit any gross visual field defects. Instilling fluorescein dye into the left eye and switching the ophthalmoscope light to the cobalt blue filter shows a round fluorescent green lesion just temporal to the centre of the pupil.
In light of a suspected intraocular/embedded foreign body, you refer the patient as an emergency to the nearest eye emergency service.
Corneal abrasions
The cornea is the thin, transparent, avascular, and outermost layer of the eye (see Fig. 1) it is divided into five layers: the epithelium (outermost), Bowman’s layer, stroma, Descemet’s membrane, and the endothelium (innermost). It is also the single-most innervated structure of the human body and is, therefore, very sensitive to an insult.
A corneal abrasion is a scratch to the cornea (see Fig. 2). Common causes are fingernails, damaged contact lenses inside the eye, papercuts, and vegetation such as tree branches. The primary presentation of patients is that of varying degrees of eye pain (may be worse upon blinking), excessive lacrimation and photophobia.
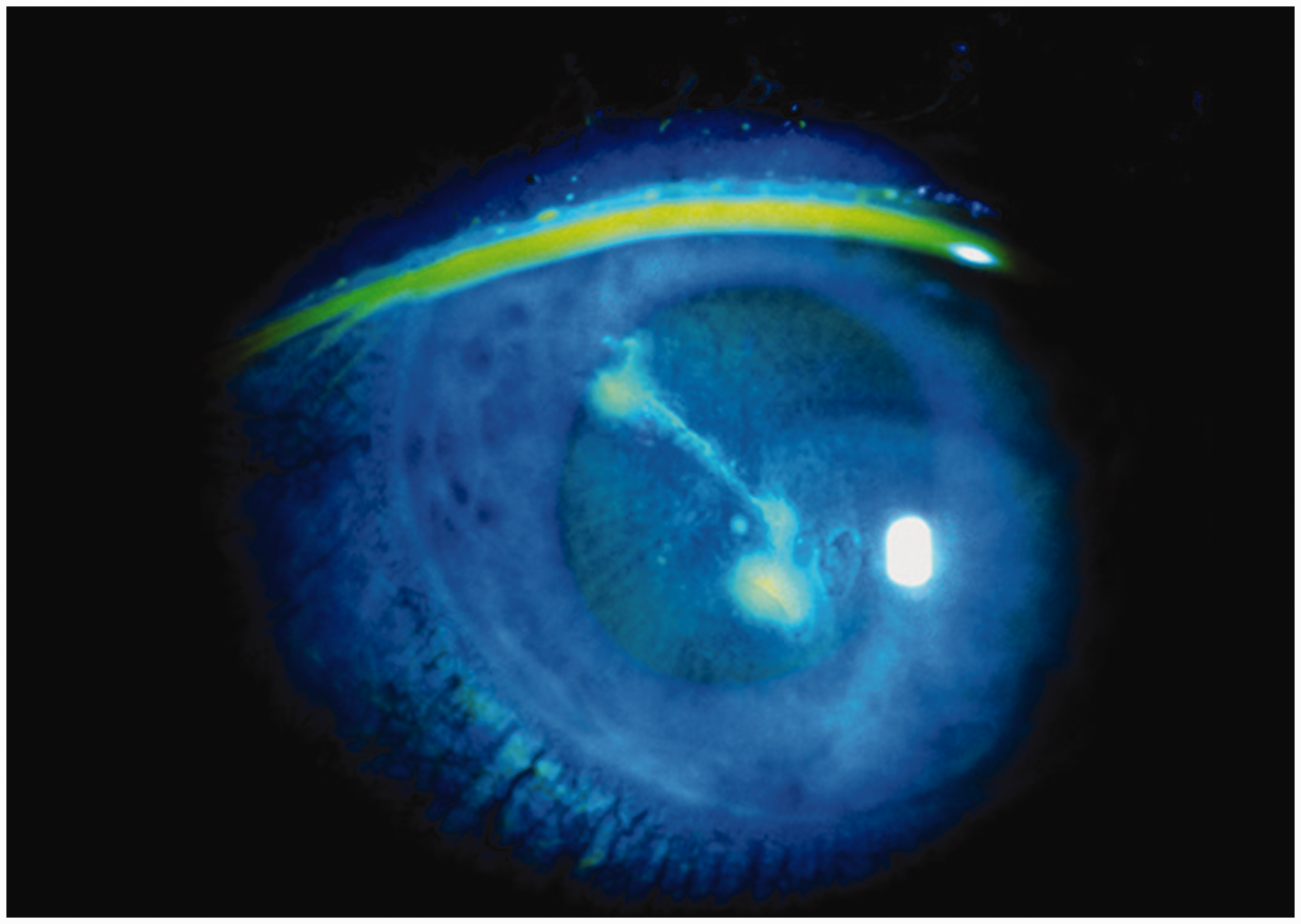
A corneal abrasion in the right eye of a patient as shown with the fluorescein eye stain test. With this test, the abrasion shows up green in colour.
When the patient presents to the GP, the foreign body which caused the abrasion may no longer be present in the eye. However, they can still complain of a foreign body sensation despite this pint, this is due to the cornea being damaged. In such cases, it is vital to evert both the upper and lower eyelids of the affected eye to ensure a foreign body is not embedded on the underside of the eyelid.
To assess the depth of the abrasion, a slit lamp examination with a subsequent fluorescein eye stain test is best. The epithelium can regenerate if damaged, but not the other layers, so if the scratch involves multiple layers of the cornea, it can lead to corneal scarring which could later lead to a hazy-looking cornea. If only the epithelium is damaged, then this will regenerate within 24–48 hours and the patient can be discharged with lubricating eye drops/ointment with a view to re-assess the eye after 2 days to see if it has healed. If the abrasion goes deeper than the epithelium, the patient will need to be referred onwards for more in-depth assessment and management.
Penetrating trauma
Penetrating eye injuries are usually caused by small, sharp objects travelling at high speeds. Therefore, the extent of eye damage can vary depending on the size of the object, the object material, the projection speed, and the eye structure affected.
Upon presentation, patients may or may not complain of a foreign body sensation, but they will give a history of something going into the eye at the time of the injury. The patient can also complain of eye pain, excessive lacrimation, red eye, bleeding, and photophobia. It is common for patients with occupational hazards to present with penetrating trauma, especially if they did not wear any eye protection at the time. In any case, a thorough history needs to be conducted including the materials with which the patient was working. The more toxic materials are copper and iron (see Fig. 3), which can cause lasting damage if left within the eye, either with pigmentary changes or copper deposition within the eye. This then increases the risk of severe eye infection. Other common materials such as glass, plastic and lead are inert and will not pose such a risk.
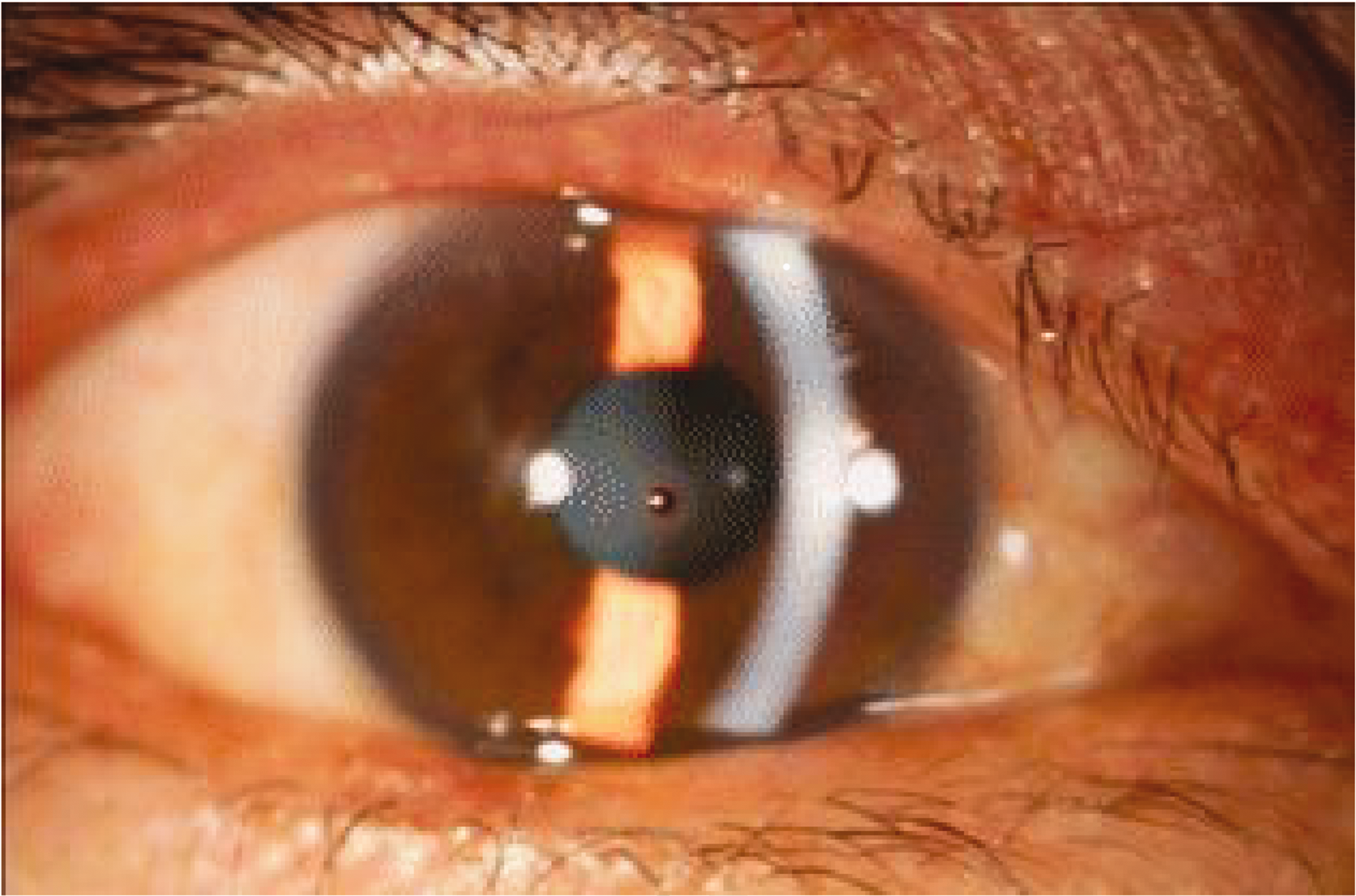
An iron foreign body embedded in the central cornea of the right eye as shown with slit lamp examination. There is also a rust ring and corneal oedema surrounding the foreign body.
Upon examination, observe the eye closely with a bright light source to see if there is any deformity of the ocular structures. Do not forget to evert both eyelids of the affected eye. Perform ophthalmoscopy and slit lamp examination with the pupil being dilated. For embedded corneal foreign bodies, such as the one illustrated in Fig. 3, a useful test to do to assess the situation is the Seidel test. This test also uses the slit lamp and fluorescein stain, but checks for leakage of aqueous humour, the fluid-filled chamber just posterior to the cornea (see Fig. 1). After instilling the topical fluorescein dye, position the patient on the slit lamp and observe for the fluorescein pattern. A positive Seidel test is determined when the fluorescein dye around the foreign body or corneal defect becomes dilute and the fluid starts leaking, which starts cascading down the ocular surface like a waterfall. This indicates that the foreign body has fully penetrated all the corneal layers; a full-thickness corneal perforation (Campbell and Gnugoli, 2022).
To manage such patients, it is imperative that the foreign body is located. If the foreign body has penetrated to the extent that it has reached the retina, there is a risk of retinal detachment, which can cause irreversible sight loss if it is not managed quickly. Penetrating injuries are classed as ophthalmic emergencies (to be seen within 24 hours) so refer the patient to their nearest eye emergency service if they have a convincing history even if you are not able to find the foreign body with a dilated pupil examination.
To locate the foreign body, the patient may need to undergo ocular ultrasound or computerised tomography. Management may include surgery to remove the foreign body and repair any damaged structures and the patient may also be given oral or topical antibiotics as prophylaxis (Denniston and Murray, 2018).
Blunt eye trauma
A blunt eye trauma is the outcome when there is a direct impact to the globe either due to a direct assault (i.e. a punch to the eye) or accidental injury (i.e. fall or road traffic accidents). Any structure in and around the eye can be affected, including the eyelids and orbital bones. The extent of damage to these structures can vary, ranging from peri-orbital bruising to globe rupture. Other injuries include orbital fractures, hyphaema (bleeding in the anterior chamber), traumatic uveitis (inflammation of the iris, ciliary body and/or choroid), or retinal detachment or commotio retinae (traumatic retinopathy). Symptoms depend on the structure that has been affected and the extent of damage, but patients will present with a clear history of trauma and will likely need specialist assessment, imaging and treatment in their nearest eye emergency service.
Chemical burns
Whether the eye has got an acidic or alkalinic substance inside it, irrigation is always the top priority. It is imperative that time is not wasted on taking a detailed history, always treat first. The potential for severe and irreversible damage, such as vision loss, ocular deformities, and extensive scarring, is higher the longer the substance remains inside the eye.
Patients may present with a very recent history of a chemical product splashing into the eye. Common acidic agents in the home environment are vinegar (contains acetic acid) and car battery acid (contains sulphuric acid). Commonly found alkalinic agents are bleach, ammonia-containing hair or cleaning products and oven cleaner (contains sodium hydroxide). Alkalis have a more devastating effect, as they continue to penetrate the eye until the pH has been neutralised (see Fig. 4). Ocular tissue damage due to acidic substances is more localized, and therefore, more limited (Hemmati and Colby, 2023).

Effects of an alkali chemical burn including extensive corneal opacification and abnormal blood vessels encroaching on the cornea (neovascularisation).
The patient would present with a severely painful, red, watery, and swollen eye. Vision is likely to be blurry and there may be obvious ocular deformities. As soon as the patient presents, do continuous irrigation via the eyewash station (saline), or help them position their eye under running tap water. Do not delay by waiting for the eyewash station. During irrigation, evert the upper and lower eyelids as much as you can as the acidic/alkalinic substance can pool inside the conjunctival fornices within the eyelids causing further damage.
The patient should have continuous irrigation for at least 15–20 minutes. Ask a colleague to arrange a blue-light ambulance in order to send the patient to the nearest eye emergency service. After this initial irrigation period, check the pH of the eye using universal indicator paper (Litmus paper), if the pH is between 7 and 7.2, the substance has been neutralised (Hemmati and Colby, 2023). It is important to check the pH of the fellow eye as well for comparison. If not already en-route, the patient needs to be transferred immediately to the nearest eye hospital to assess the extent of damage and provide further management. Ensure you provide oral analgesia and eye lubricants to patients before they are transferred to the ambulance.
Key points
When examining the eyes, never underestimate the value of direct observation and always examine with good lighting For suspected intraocular foreign body, a detailed and concise history is key including occupation history Symptoms of intraocular foreign bodies can include a watery and red eye, a scratchy feeling when blinking (but not always), blurry or loss of vision and light sensitivity For any patient with a suspected intraocular foreign body, refer as an emergency to the nearest eye emergency service even if you were unable to locate the foreign body during the examination With chemical injuries, treat immediately with irrigation first, obtain a detailed history later