
Abstract
Allergic rhinitis (AR) is a major public health issue worldwide and one of the top-10 reasons for primary care attendance. AR affects between 10 and 25% of people worldwide, including 10–15% of children and 26% of adults in the United Kingdom. Sneezing, nasal itching, rhinorrhoea, nasal congestion, ocular symptoms (irritation and lacrimation), non-productive cough, Eustachian tube dysfunction and chronic sinusitis are all symptoms of AR. AR can be characterised as seasonal (hay fever), perennial, intermittent, persistent, or occupational, depending on the allergens and the pattern and frequency of symptoms. Asthma and conjunctivitis are significantly associated with AR. A clinical history and physical examination are the most important processes in diagnosis. Skin tests can be used to confirm the diagnosis of AR. Patients with AR may experience changes in their everyday activities, emotions, and sleep habits, to the detriment of quality of life. Early detection and treatment can ameliorate the unpleasant effects of AR. Management includes medication, avoidance of exposure to environmental allergens and when appropriate, measures to help with associated asthma and sinusitis. Psychological interventions can also help in the management of AR.
Clinical case scenario
A 32-year-old male presents to the surgery complaining of excessive sneezing every morning. He reports 15–20 episodes of sneezing, along with eye and throat irritation with excess lacrimation. He complains of sleep disturbance and impairment to his quality of life. He has taken an over-the-counter drug (an antihistamine) assuming that his symptoms are caused by allergies. The medication appears to ease symptoms at first, but after a few weeks, the symptoms return.
Aetiology
The allergic response can be divided into early-phase reactions and late-phase reactions. In its early stages, allergic rhinitis is an inflammatory reaction to inhaled allergens driven by type 2 helper (Th2) cells and mediated by immunoglobulin E (IgE). The host mast cells degranulate as an initial response within 5 to 15 minutes of antigen exposure. One of the mediators released as a result of this is histamine, which is one of the primary mediators of allergic rhinitis (AR). Histamine produces rhinorrhea and causes sneezing through the trigeminal nerve by activating mucous glands. Two other immune mediators that affect blood vessels and exacerbate nasal congestion are leukotrienes and prostaglandins. After the initial response, 4 to 6 hours later, development of the late-phase response is mediated by an influx of cytokines from mast cells, such as interleukins (IL-4 and IL-13). These cytokines then cause nasal edema with subsequent congestion by allowing eosinophils, T-lymphocytes, and basophils to infiltrate the nasal mucosa (Alromai et al., 2022: Pawankar et al., 2011; Skoner, 2001).
Epidemology
AR affects about 15% of the population, based on physician diagnosis. However, a higher prevalence of up to 30% is reported in surveys of patients’ nasal symptoms. It is well known that AR peaks during the second and fourth decades of life and then gradually declines (Wheatley and Togias, 2015). According to a study from 2018, significant work absence is caused by AR (Vandenplas et al., 2018).
History and examination
A good clinical history is important in the diagnosis of AR. Rhinitis is not always caused by allergies and other causes can be determined from the history. A history should detail the frequency and impact of sneezing, nasal symptoms (including discharge and irritation), eye symptoms, throat symptoms and any associated respiratory symptoms, such as a dry cough. Are symptoms confined to a specific season or do they occur all year? Do symptoms occur at home but abate when away from home? Are there identifiable triggers for symptoms, such as food, medication or exposure to pets? Is there a family history of allergies?
Examination may identify mouth breathing, frequent sniffling and/or throat clearing. Is there a transverse supra-tip nasal crease? Are there dark circles under the eyes (‘allergy shiners’)? In children, the nasal supra-tip crease is more prevalent. Typically, anterior rhinoscopy reveals oedema of the nasal mucosa and thin, clear secretions. The nasal mucosa may have a cobblestone appearance and the inferior turbinates may develop a bluish hue.
Endoscopic examination will identify nasal polyps and other structural irregularities. Eustachian tube dysfunction is very prevalent in patients with AR, and can be evaluated with pneumatic otoscopy. Patients with persistent symptoms may feel pain with palpation over the affected sinuses. Patients should be examined for the clinical features of asthma and atopy (Small et al., 2018).
Investigation
The gold standard for identifying atopy is skin prick testing; it has long been thought to be the most sensitive and specific technique for the detection of sensitisation to allergens (Demoly et al., 1991; Neslaon et al.,1993). The detection of allergen-specific IgE in serum using radioallergosorbent testing is also now useful. Specialist clinics may use nasal challenge testing using allergens. These can be useful for identifying the cause of AR when occupational exposure to allergens is suspected, for example. Computerised tomography scan may be necessary in chronic rhinosinusitis, for example to exclude tumours (Varshney and Varshney, 2015).
Management
The Allergic Rhinitis and its Impact on Asthma (ARIA) workshop has suggested a severity scale for AR. A good understanding of patients’ symptoms and the impact of symptoms informs treatment (Fig. 1).
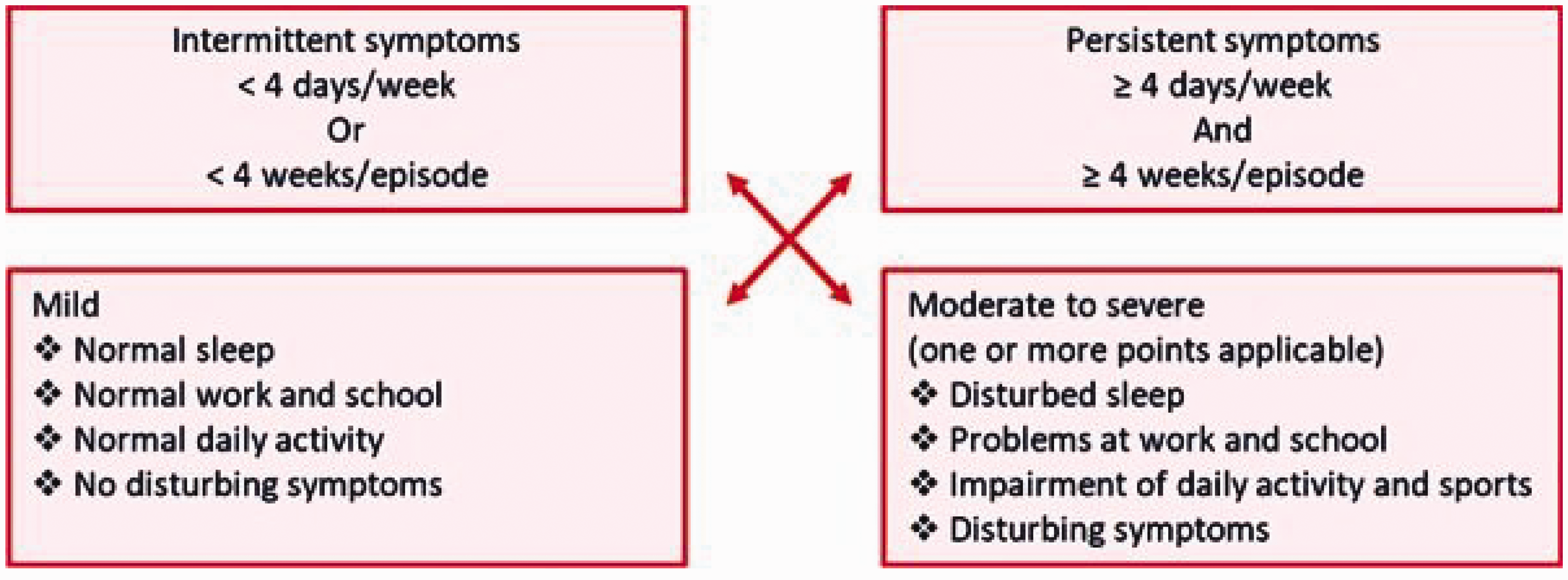
The ARIA classification for allergic rhinitis.
For mild-to-moderate intermittent or mild persistent symptoms, the as required treatment is with intranasal antihistamines or a second-generation, non-sedating oral antihistamine (depending on person’s age and preference) or an intranasal chromone (such as sodium cromoglicate) if antihistamines are contraindicated or not tolerated, is appropriate.
If there are moderate-to-severe persistent symptoms or the initial drug treatment is ineffective, prescribe regular intranasal corticosteroid for use during periods of allergen exposure. There are various options including intranasal mometasone furoate, fluticasone furoate, or fluticasone propionate.
For people with allergies to house dust mite and/or pets, drug treatment should be ongoing throughout the year. For tree, grass, and weed pollens, treatment should start 2–3 weeks before re-exposure to the allergen. If the timing of re-exposure is uncertain, treatment should start several weeks before the expected start of the season. If symptoms persist despite initial treatment review patients after 2–4 weeks and consider stepping up treatment with intranasal decongestant, intranasal corticosteroid and oral antihistamine as necessary.
Consider adding an oral antihistamine, intranasal corticosteroid, leukotriene receptor antagonist (e.g. montelukast), or intranasal anticholinergic (e.g. ipratropium bromide) if regular antihistamine or intranasal corticosteroid use fails to relieve persistent nasal itching and sneezing.
For patients with severe, uncontrolled symptoms that are affecting quality of life significantly, consider use of a short course of oral corticosteroids with appropriate advice and precautions. For adults use prednisolone 0.5 mg/kg in the morning for 5–10 days and for children use prednisolone 10–15 mg in the morning for 3–7 days.
If there are any red flag symptoms (unilateral symptoms, blood-stained nasal discharge, recurrent epistaxis, or nasal pain) then make an urgent 2-week wait referral to the ear, nose and throat (ENT) clinic. If there is a major nasal blockage and/or structural anomaly, make a referral for an ENT appointment. Consider referring to the allergy clinic if symptoms continue despite adequate treatment in primary care. Specialist immunotherapy may be appropriate for people with symptoms after allergen exposure, objective evidence of IgE sensitivity and chronic symptoms caused primarily by one allergen, such as grass pollen or house dust mites. The treatment, which can be given subcutaneously or sublingually, involves exposing the patient to increasing amounts of allergen in order to induce clinical and immunological tolerance (National Institute for Health and Care Excellence (NICE), 2022).
Differential diagnoses
Various forms of rhinitis can mimic AR. Non- allergic rhinitis is distinguished by the presence of nasal symptoms in conjunction with negative allergy skin prick tests, suggesting the absence of allergic disease (Kaliner, 2009).
Drug-induced rhinitis is associated with a wide variety of drugs including, non-steroidal anti-inflammatory drugs, angiotensin-converting enzyme inhibitors, phosphodiesterase type 5 inhibitors, imidazoline receptor agonists, diuretics, calcium channel blockers, psychotropics, local decongestants and anti-thyroid medication (Alromaih et al., 2022).
Rhinitis medicamentosa is an irritation of the nasal mucosa brought on by excessive use of topical nasal decongestants, typically presenting with nasal congestions and irritation (Wahid and Shermetoa,2023).
Work-related rhinitis or occupational rhinitis is a term used to describe the various types of rhinitis connected to the workplace. These can be divided into allergic or non-allergic forms and are brought on by factors and circumstances specific to a workplace. Work-exacerbated rhinitis is characterised as pre-existing rhinitis aggravated by exposure at work (Kotz et al., 2021). Noxious odorants, chemical irritants and cleaning agents can cause chemical rhinitis. For obvious anatomical reasons rhinitis frequently coexists with sinusitis. The most prevalent type of upper respiratory infection, acute viral rhinitis, is typically brought on by viruses rather than bacteria.
Pregnancy-related rhinitis and menstrual cycle-related rhinitis are both examples of hormone-induced rhinitis. Pregnancy rhinitis, which is more prevalent among smokers, manifests during the final 2 months of pregnancy and goes away 2 weeks post-partum. Premenstrual rhinitis has a cyclical relationship with premenstrual symptoms. Although the precise mechanism has not been determined, it is believed that high oestrogen levels cause nasal congestion by vascular engorgement, which in turn, aggravates the symptoms of hormone-induced rhinitis.
A non-allergic, non-inflammatory kind of rhinitis known as gustatory rhinitis is characterised by the abrupt onset of watery or mucoid rhinorrhea brought on by food, particularly spicy food. Among the most popular triggers are hot chilli peppers, red cayenne, Tabasco sauce, onions, chilli, vinegar, red pepper, and mustard (Liva et al., 2021).
Non-allergic rhinitis with eosinophilia syndrome includes symptoms similar to AR in which allergen skin testing has shown no evidence of atopy and nasal cytology investigation shows more than 20% eosinophils. An important characteristic that allergic rhinitis does not share is anosmia (Ellis and Keith, 2006).
Age-related rhinitis, known as senile rhinitis or elderly rhinitis, is characterised by clear, watery anterior rhinorrhea without a known trigger. It is thought to be the result of cholinergic hyper-reactivity and ageing-related anatomical changes in the nose (Liva et al., 2021).
After partial or complete turbinectomy, an uncommon condition known as empty nose syndrome (ENS) can appear. The primary characteristic of ENS is the perception of a paradoxical nasal obstruction despite an empirically broad nasal airway. Dyspnea, nasal dryness, burning, blockage, suffocation, and even concomitant psychological problems can significantly impair patients’ quality of life (Gordiienko et al., 2021).
Patients with atrophic rhinitis present with anosmia (mercifully) and foul-smelling nasal crusting, nasal discharge and nasal obstruction with associated bacterial infection. Vasomotor rhinitis frequently presents with rhinitis symptoms linked to non-allergic, non-infectious stimuli in the absence of an obvious cause. A variety of other conditions may cause symptoms similar to AR, including rhinosinusitis, nasal foreign bodies, cystic fibrosis, primary ciliary dyskinesia and gastroesophageal reflux (Wise et al., 2023).
Conclusion
Sneezing, nasal itching, rhinorrhea, and congestion are symptomatic of AR. AR is an IgE-mediated immune condition brought on by the nasal mucosa's heightened sensitivity to allergens. It can be classified as seasonal (hay fever), perennial, intermittent, persistent, or occupational, depending on the allergens and frequency of symptoms. Asthma and conjunctivitis are often associated with AR. The diagnosis of AR is made from the clinical history, physical examination and skin testing. Management requires more than just medication. Reduced exposure to environmental allergens, preventative measures, management of comorbid illnesses (including sinusitis and asthma) and psychological support are all useful in the treatment of AR.
Key points
Allergic rhinitis is typically an IgE-mediated type 1 hypersensitivity that occurs with exposure to allergens
The most common symptoms are excessive sneezing, nasal congestion, rhinorrhoea, itchy eyes, throat irritation and dry cough
Allergic rhinitis can be triggered by a variety of allergens including pollen, dust mites, mould and animal dander
Diagnosis can be made from history, clinical findings, skin prick testing and allergen-specific IgE serology
Treatment of allergic rhinitis includes identification of allergens, avoidance of allergens and medication including antihistamines, intranasal corticosteroids, corticosteroids and immunotherapy used according to the severity of disease
Psychological counselling is helpful, especially when symptoms are having a significant impact on a patient’s quality of life