
Abstract
Overweight and obesity are defined as abnormal or excessive adipose tissue accumulation that results in a risk to health. This is caused not simply by poor lifestyle, but rather a complex interplay of health inequalities, genetic inheritance, as well as social and environmental factors. Excess weight significantly increases the risk of chronic illnesses, including cardiovascular diseases, diabetes, musculoskeletal disorders, and various types of cancer. Individuals with a body mass index (BMI) of 30–35 kg/m2 experience an average reduction in life expectancy of 2–4 years and for those with a BMI of 40–50 kg/m2, the decrease in life expectancy ranges from 8–10 years. Experts predict that by 2030, the UK will see 11 000 000 more adults affected by obesity, resulting in a significant increase in the cost of treating obesity-related diseases. This article provides a contemporary overview of obesity understanding and management in adults, including brief interventions, motivational interviewing, as well as pharmacological and surgical options.
Clinical case scenario
A 33-year-old man attends your GP surgery for help with weight loss. He recently broke up with his partner, and feels terrible about his self-image. He has an HbA1c of 45 mmol/mol (6.3%). His body mass index is 32 kg/m2.
Definition and classifications
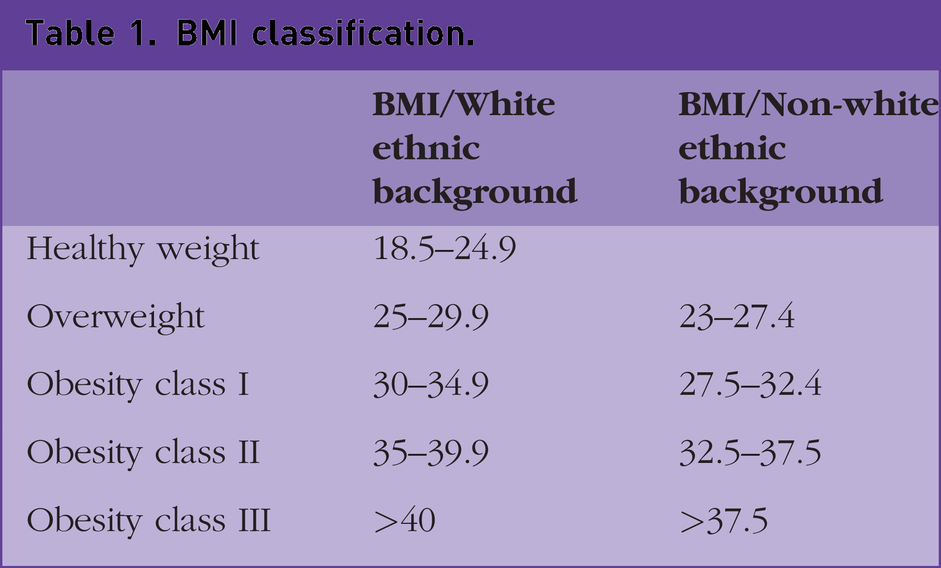
Body mass index (BMI) is the most common classification used in clinical practice to assess obesity. However, individual interpretation may be needed among men with a high muscle mass and people above 65 years in age. In addition, people from specific ethnic backgrounds are prone to central adiposity, and their cardiometabolic risk occurs at lower BMI. Therefore, different BMI thresholds are applied to people from South Asian, Chinese, other Asian, Middle Eastern, Black African or African-Caribbean backgrounds. (National Institute for Health and Care Excellence (NICE, 2017) (Table 1.)
BMI classification.
A waist-to-height ratio is a more sensitive estimate of central adiposity. It should be taken at the waist, which is a midpoint between the bottom of the ribs and the top of the hips (NICE, 2017). Categorisation for waist-to-height ratio is described below:
0.4–0.49: Healthy central adiposity 0.5–0.59: Increased central adiposity, increased cardiovascular and metabolic health risks ≥0.6: High central adiposity, further increased health risk.(NICE, 2023 RCGP, 2023)
Epidemiology
The prevalence of obesity has been steadily increasing over the past 50 years. The World Health Organization (WHO) estimates worldwide around 39% of adults are overweight, and 13% are living with obesity. (Abbafati et al., 2020; WHO, 2023) Overweight and obesity are now the norm in adults in the UK: 76% of men and 60% of women are overweight or obese. There were 36.2, 36, 37 and 38% overweight people and 28, 23, 29 and 27% people with obesity in England, Wales, Scotland and Northern Ireland, respectively (RCGP, 2023).
Tackling obesity in the UK
A recent UK policy paper on tackling obesity offers a roadmap for addressing the obesity crisis (Department of Health and Social Care, 2020). Strategies include improving the food environment, implementing clearer food labelling, banning offers on high fat, salt and sugar products, and restricting unhealthy food advertising to children. Collaboration between government, industry, healthcare professionals, and communities is emphasised for sustainable change. To date, most of these policy suggestions have not been implemented.
Risk factors
Multiple risk factors are connected to obesity and overweight. They can be modifiable (diet, physical activity levels, sleep), non-modifiable (genetics, age, social and psychological factors, less formal education and low socioeconomic status, menopause and pregnancy) or health-related (gestational weight gain during pregnancy, medical conditions, such as hypothalamic damage, polycystic ovary syndrome or hypothyroidism, and medications such as corticosteroids or anti-psychotics) (Goodarzi, 2018; RCGP, 2023).
Genetics
Genetics plays a significant role in obesity development, with heritability estimates ranging from 40 to 70% in twin and family studies. Obesity can arise from alterations in a single gene, as seen in Prader–Willi syndrome, or multiple gene loci (over 600) that influence energy balance, appetite regulation, metabolism, and fat storage, but do not solely determine weight status. Examples include FTO, MC4R, and POMC. Understanding genetic factors can reveal the complex mechanisms of obesity and potential therapeutic targets (Locke et al., 2015; Goutzelas et al., 2022).
Environment and socioeconomic status
There is a higher prevalence of obesity in areas of greater deprivation (RCGP, 2023). Socioeconomic disparities in diet quality may be partially explained by the higher cost of healthy diets. Foods of lower nutritional value generally cost less per calorie (Darmon and Drewnowski, 2015). Additionally, physical fitness facilities and green spaces are not distributed equally, with access more difficult in deprived areas.
Metabolic set theory
The metabolic set theory proposes that individuals have a genetically predetermined ‘set point’ for body weight and metabolism. The theory suggests that the body strives to maintain a stable weight range, similar to a thermostat regulating temperature. Genetic factors influence the individual set point. When weight deviates, metabolic adaptations such as energy expenditure, appetite regulation, and fat storage occur to restore it. The theory suggests that long-term weight loss maintenance is challenging because the body resists sustained weight loss, triggering responses that promote weight regain (RCGP, 2023).
Hormonal regulation
Appetite regulation and metabolic set theory involve five key hormones. Ghrelin signals hunger and satiety, with levels decreasing after eating to indicate fullness. Individuals with obesity often have blunted ghrelin responses, leading to decreased satiety and increased hunger. Leptin, produced by fat cells, suppresses appetite. Individuals with obesity exhibit leptin resistance, where the hormone's effects are diminished. Weight loss can decrease leptin levels, increasing appetite. Three hormones in the intestines, peptide YY, CCK, and GLP-1, promote satiety. GLP-1 is a target for pharmaceutical interventions to reduce hunger and slow gastric emptying.
Mental health and weight
People with significant mental illness have a higher prevalence of obesity than the general population (Afzal et al., 2021). Second-generation antipsychotics, particularly olanzapine and clozapine, contribute to antipsychotic-induced weight gain (Lee et al., 2022). People on these medications should have annual reviews in primary care once established on their medication. This should include (amongst other investigations) a BMI measurement and markers for cardiovascular disease. The selective serotonin reuptake inhibitor drug mirtazapine is also known to result in weight gain and increased appetite.
Assessment
GPs play a vital role in assessing the impact of increased weight in patients. NICE recommends conducting investigations (including lipids, liver and thyroid function, HbA1c tests) to evaluate overall metabolic health. GPs should also screen and treat any accompanying disorders such as eating or mood disorders (RCGP, 2023).
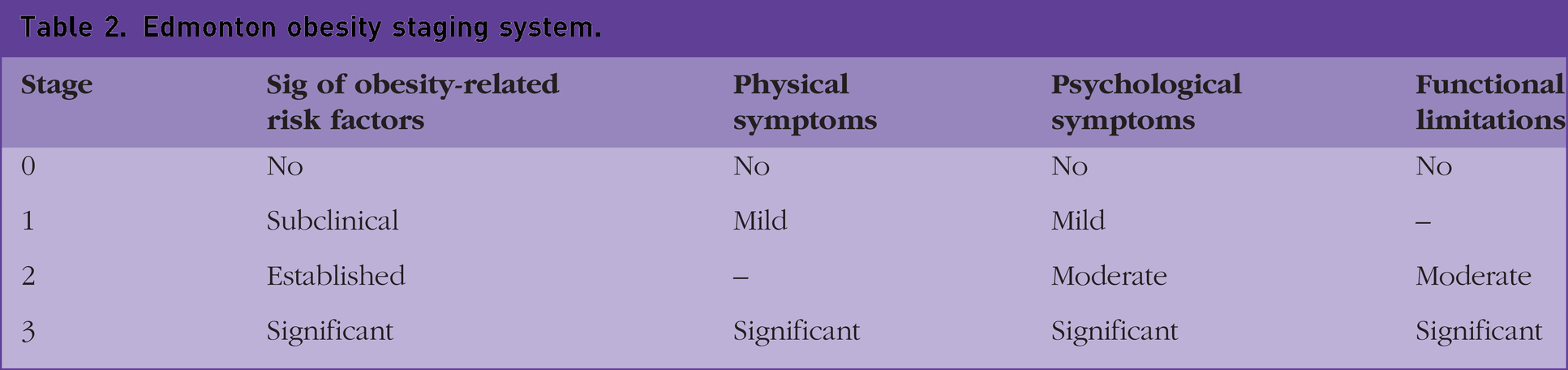
The Edmonton Obesity Staging System (EOSS) is a classification system that assesses the impact of obesity on an individual's health. It goes beyond BMI and considers factors such as obesity-related complications, functional limitations, and quality of life. The EOSS categorises individuals into four stages, offering a holistic approach to understanding obesity-related health (Table 2) (RCGP, 2023; Swaleh et al., 2021).
Edmonton obesity staging system.
Treatment
Treatment benefits
Weight loss of 10 kg in individuals with obesity has been shown to have numerous health benefits. There is an associated 20–25% decrease in total mortality, a 30–40% decrease in diabetes-related deaths, and a 40–50% decrease in obesity-related cancer deaths. Hypertensive individuals experience a 10 mmHg decrease in systolic blood pressure (BP) and a 10–20 mmHg decrease in diastolic BP. Newly diagnosed diabetics see a 30–50% reduction in fasting glucose levels and a 15% reduction in HbA1c levels. Lipid profiles improve, with a 10% decrease in total cholesterol, a 15% decrease in LDL cholesterol, a 30% decrease in triglycerides, and an 8% increase in HDL cholesterol. Other benefits include improved lung function, insulin sensitivity, ovarian function, and reductions in back pain, joint pain, breathlessness, and sleep apnoea (NICE, 2017; RCGP, 2023).
Tier system
The UK employs a comprehensive four-tier system for treating obesity, encompassing various levels of intervention and care.
Tier 1 focuses on population-level prevention strategies, promoting healthy behaviours and raising awareness about obesity risks. This includes educational campaigns, community programmes, and policies to encourage healthier eating and increased physical activity (RCGP, 2023).
Tier 2 in obesity management involves primary care interventions focusing on individuals at risk of or affected by obesity, including brief advice and referral for further support. Weight management programmes vary depending on locality, but may include commercial weight management services, such as Slimming World or Obesity Empowerment Network. These weight management programmes have been shown to efficacious, with an average weight loss (including non-attenders) of over 2 kg, compared with controls (Madigan, 2022). Additionally, a 12-week NHS Digital Weight Management Programme offers online support for individuals with obesity and comorbidities such as hypertension or diabetes (NHS, 2023; RCGP, 2023). Between April 2021 and December 2022, 131 665 participants were referred to adult tier 2 weight management services in England, of which 40% were self-referrals and 29% were GP referrals. Thirty-five percent completed a least 75% of planned interventions and were regarded as having completed the programme. Forty percent of all participants lost weight, and 15% of all enrolled lost at least 5% of body weight (UK Government, 2023).
Tier 3 involves specialised weight management services provided by multidisciplinary teams of healthcare professionals, including dietitians, psychologists, and exercise specialists. These teams collaborate to deliver tailored interventions lasting around 12 weeks. Services may include structured dietary plans, behavioural therapy, supervised physical activity programmes, and, if necessary, medication for weight loss. Patients can self-refer or be referred to this tier (RCGP, 2023).
Tier 4 is the highest level of care for severe obesity and obesity-related complications. It includes specialist services such as bariatric surgery. Surgery is considered for individuals with significant obesity and comorbidities that have not responded to previous interventions. Referrals in England and Scotland are recommended for BMI above 40 kg/m2, or from 35 kg/m2 with comorbidities. In Wales, patients must have had a BMI of 40 kg/m2 for at least 5 years and engaged with previous tiers for at least 2 years without successful weight loss. Patients typically receive specialist Tier 4 care for 2 years after surgery (RCGP, 2023).
Local authorities are funding various services supporting weight loss in Scotland, England and Wales. There is currently no official weight management service in Northern Ireland, and GPs offer weight management support on an ad hoc basis (RCGP, 2023).
Medications
NICE recommends specific medications to complement lifestyle interventions in obesity management. Drug treatment alongside lifestyle interventions can lead to weight loss, maintaining this long-term can be difficult, and potential side effects can impact medication adherence (NICE, 2023).
Medications: Orlistat
Orlistat is a lipase inhibitor that works by reducing the absorption of dietary fat in the digestive system. It inhibits the action of lipase, an enzyme that breaks down fats, thereby decreasing the amount of fat absorbed by the body.
Orlistat can be considered as a treatment option for individuals with a BMI of 30 kg/m2 or higher who have not achieved significant weight loss through lifestyle interventions alone. It may also be appropriate for individuals with a BMI of 28 kg/m2 or higher who have additional risk factors.
Orlistat is typically taken as one 120 mg capsule with each main meal containing fat, usually within an hour before or after the meal. The dose may be adjusted based on individual response, but the recommended daily dose should not exceed 360 mg. Following a reduced-calorie, low-fat diet is important when using orlistat to achieve optimal results. Orlistat 60 mg capsules are also available over the counter (NICE, 2023).
Orlistat is effective for weight loss, but is associated with side effects. These include gastrointestinal discomfort, such as oily stools, increased bowel movements, flatulence, and abdominal pain. These symptoms are caused by undigested fat passing through the digestive system. Rarely, severe liver injury may occur. Orlistat is contraindicated for individuals allergic to the medication or with specific medical conditions such as chronic malabsorption syndrome or cholestasis. Absorption of fat-soluble vitamins (A, D, E, K, and beta-carotene) may be impaired in people taking orlistat and it is therefore important to advise people to have a diet that is rich in fruit and vegetables and consider the use of a multivitamin supplement (to be taken at least 2 hours after orlistat) (NICE, 2023).
Regular monitoring is essential to assess a patient's progress, adherence to prescribed treatment, and identify any potential side effects. If a person does not achieve a weight loss of at least 5% of their initial body weight within 12 weeks of using orlistat, NICE recommends discontinuation of treatment. However, individuals with type 2 diabetes may experience slower weight loss rates, so a goal of losing more than 3% of body weight within 12 weeks may be suitable. These goals should be discussed and monitored regularly. Once the desired weight loss is achieved, there are no specific limitations on the duration of orlistat treatment (NICE, 2023).
GLP-1 receptor agonists
NICE recommends semaglutide, a GLP-1 receptor agonist under specialist supervision (tier 3 or 4 services) for a maximum of 2 years for weight loss. The STEP 1 randomised controlled double-blind trial showed that participants taking semaglutide lost 12% more of their body weight compared with participants taking a placebo. GLP-1 agonists work by reducing appetite and increasing satiety. Side effects include nausea and gastrointestinal disturbance (NICE, 2017). The significant increase in demand for semaglutide (including in the private sector) has led to shortages of the drug. Semaglutide prescriptions for weight loss are currently not able to be initiated in primary care, although semaglutide can still be prescribed for patients with type 2 diabetes.
Other drugs in this class, such as tirzepatide, orforglipron and retatrutide, have also shown promising weight loss in clinic trials, but are not yet available for weight loss in the UK. Orforflipron is available as an oral preparation, in contrast with most other drugs in this class which are injectables (Jastreboff et al., 2023; Wharton et al., 2023).
Procedural management: Gastric balloon
A gastric balloon is a non-surgical weight loss intervention that involves placing a soft silicone balloon in the stomach to reduce its volume and create a feeling of fullness with smaller food portions. The balloon is typically inserted endoscopically through the mouth and filled with a saline solution or gas. It remains in the stomach for around 6 months, promoting weight loss by restricting food intake and reducing hunger. The procedure is considered for individuals with a BMI between 30 and 40 kg/m2 who have not succeeded with traditional weight loss methods. It is used as a bridge treatment before more invasive surgeries. However, the balloon is not a standalone solution, and should be combined with lifestyle modifications. Side effects may include nausea, vomiting, abdominal discomfort, and rare instances of balloon deflation or migration. Close monitoring and follow-up care are necessary during balloon placement, which is similar to the follow-up required after bariatric surgery.
Procedural management: Bariatric surgery
Bariatric surgery may be recommended for patients with a BMI of >40 kg/m2 or a BMI of 35–39.9 kg/m2 with comorbidities that could improve with weight loss (Box 1). It is considered when non-surgical approaches have been unsuccessful in achieving sustainable weight loss. In some cases, patients with a BMI of 30–34.9 kg/m2 and recent type 2 diabetes may also be candidates for bariatric surgery (NICE, 2017). The five most common bariatric surgeries performed in the UK. Roux-en-Y gastric bypass (RYGB): This procedure involves creating a small stomach pouch and rerouting the small intestine to connect to the pouch. It restricts the amount of food intake and reduces nutrient absorption Sleeve gastrectomy: In this surgery, a large portion of the stomach is removed, leaving behind a narrow sleeve-shaped stomach. It promotes weight loss by restricting food intake and reducing hunger hormones Adjustable gastric banding: A silicone band is placed around the upper part of the stomach, creating a small pouch. The band can be adjusted to control the amount of food intake. It works by limiting food volume and creating a feeling of fullness Biliopancreatic diversion with duodenal switch: This complex surgery involves removing a large portion of the stomach and rerouting the small intestine. It restricts food intake and reduces nutrient absorption Mini gastric bypass: Similar to RYGB, this procedure involves creating a small stomach pouch and rerouting the small intestine. Its simplified version of RYGB has gained popularity due to its simplicity and potential effectiveness
The British Obesity and Metabolic Surgery Society (BOMSS) has provided guidance on clinical care after surgery (BOMSS, 2016). The key recommendations include:
Record keeping of the type of procedure and inclusion in the practice obesity registry Postoperative follow-up care should be for a minimum of 2 years in tier 4 services Annual blood tests lifelong (full blood count, urea and electrolytes, liver function test, calcium, vitamin D (ferritinn, folate), parathyroid hormone, vitamin B12 (FBC, UE, LFT, Ca, vit D, ferritin, folate, PTH, B12)) Monitoring and supplementation of nutritional elements, which differ for each surgery (for example, zinc, copper, vit A, or selenium) Pregnancy should be avoided for at least 18 months
Accessing bariatric surgery in the NHS can be difficult, despite its effectiveness in achieving weight loss. In 2017, less than 7000 out of around a million eligible individuals received the surgery. Limited access is due to budget constraints and weight-related stigma, resulting in uneven availability across regions, despite the cost-effectiveness of this surgery (RCGP, 2023).
An increasingly popular option for patients is to have bariatric surgery abroad, which can be more accessible and less expensive than private options in the UK. However, follow-up care can be challenging for those patients, as procedural information may be incomplete, and returning to the same surgeon for follow-up may not be possible. Certain NHS clinics may offer limited follow-up care for these patients (RCGP, 2023).
Consultation skills
GPs should approach the weight discussions with sensitivity. Patients may face various barriers, such as fear of judgment, embarrassment, or lack of motivation to address the issue. GPs may find it difficult to incorporate offers of support for weight reduction in the consultation, due to time constraints and nervousness about the topic. Research has shown that offers of support are better received when a tier 2 service is referred to as a ‘weight management programme/service’ or a commercial name rather than ‘group or club’. Highlighting that support is free and local has also been shown to improve acceptance (Albury et al., 2021).
Motivational interviewing (MI) is a communication technique that helps discussion with patients about excess weight effectively; MI aims to enhance intrinsic motivation and readiness for change. The key elements of MI include partnership, acceptance, compassion, and empowerment. By using MI techniques and addressing potential barriers, GPs can engage patients, boost motivation, and foster a collaborative approach to weight management (RCGP, 2023).
Patient information leaflets and digital resources
Offering additional information about weight management to patients is good practice. NHS and commercial weight management services also include digital/online support. Examples of patient information leaflets and digital resources are provided in Box 2. Patient information leaflet and digital resources. Obesity: https://patient.info/healthy-living/obesity-overweight Obesity in pregnancy: www.rcog.org.uk/for-the-public/browse-all-patient-information-leaflets/being-overweight-in-pregnancy-and-after-birth-patient-information-leaflet Charity: Obesity UK www.obesityuk.org.uk NHS Weight Loss Plan www.nhs.uk/better-health/lose-weight
Key points
Obesity is a global health issue and prevalence is increasing worldwide
The management of obesity in the UK is arranged in a four-tier system that goes beyond simply eating less and exercising more
Obesity is a chronic disease influenced by genetic factors, lifestyle factors and health inequalities - not solely a result of individual choices
An increasing number of drugs are becoming available to treat obesity, in particular GLP-1 agonists such as semaglutide
However, drugs for obesity are currently in short supply and can only be prescribed in secondary care; Orlistat is the only medication that can currently be prescribed for weight loss in primary care
After bariatric surgery, patients need a lifelong follow-up, facilitated by GPs