
Abstract

Case history
Mr Smith, a 65-year-old man, attended a routine general practice appointment complaining of bilateral breast development for 8 months. He did not have any breast pain, nipple discharge, bleeding or irritation. He denied any sexual dysfunction. Although he was not sexually active, he described having normal early morning erections and a normal libido. Mr Smith’s weight had remained stable with no changes in appetite. Mr Smith had a background of hypertension treated with amlodipine. He lived a sedentary life, rarely drank alcohol and did not smoke.
Examination revealed Mr Smith was obese with a body mass index (BMI) 30 kg/m2. He had equal, bilateral gynaecomastia with 3 cm discs of breast tissue under each nipple–areolar complex. There were no palpable masses and the tissue was soft and non-tender to examine. Mr Smith had a notable lack of chest hair. There were no other signs of chronic liver disease. Abdominal and cardiovascular examination was normal. Mr Smith’s testicular examination revealed a significantly atrophied left testicle, which was non-tender to palpate. His right testicle appeared normal in size and shape. There were no testicular lumps, scrotal swellings, erythematous rashes or other skin changes.
Mr Smith had recently had his annual blood tests, which showed normal kidney, liver and thyroid function. His hormone profile showed low testosterone levels but was otherwise normal. An urgent ultrasound scan reported chronic torsion and atrophy of the left testicle. He was subsequently referred to urology for discussions about further management options, including orchidectomy, and possible testosterone replacement therapy.
Discussion
This case highlights an unusual presentation of gynaecomastia with a painless testicular torsion (TT). Gynaecomastia, the benign proliferation of male breast tissue, can have many underlying causes (see Table 1). Assessment of gynaecomastia is usually guided by history and examination findings. When a testicular cause is suspected, appropriate blood tests (see Box 1) and a testicular ultrasound should be undertaken (Dickson, 2012). Suggested blood tests when suspecting a testicular cause of gynaecomastia.
Testosterone, oestradiol, luteinizing hormone, follicle-stimulating hormone levels, sex hormone-binding globulin
Human chorionic gonadotropin, alpha-fetoprotein Sources: Kanakis et al., 2019; Dickson, 2012.
Causes of gynaecomastia.
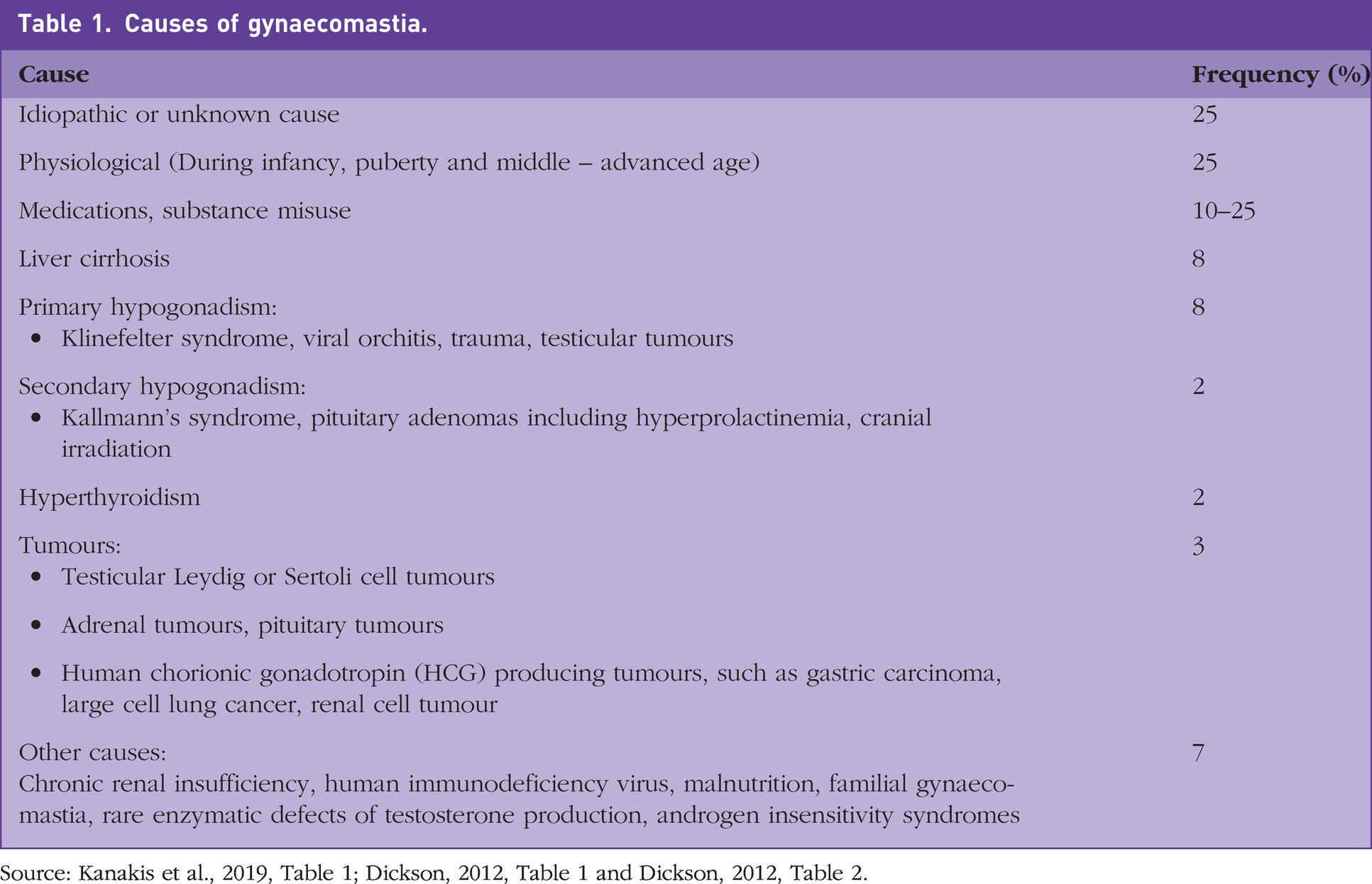
Source: Kanakis et al., 2019, Table 1; Dickson, 2012, Table 1 and Dickson, 2012, Table 2.
Testicular damage reduces testosterone production and the ensuing endocrine changes lead to increased oestrogen which can stimulate gynaecomastia (See Figure 1).
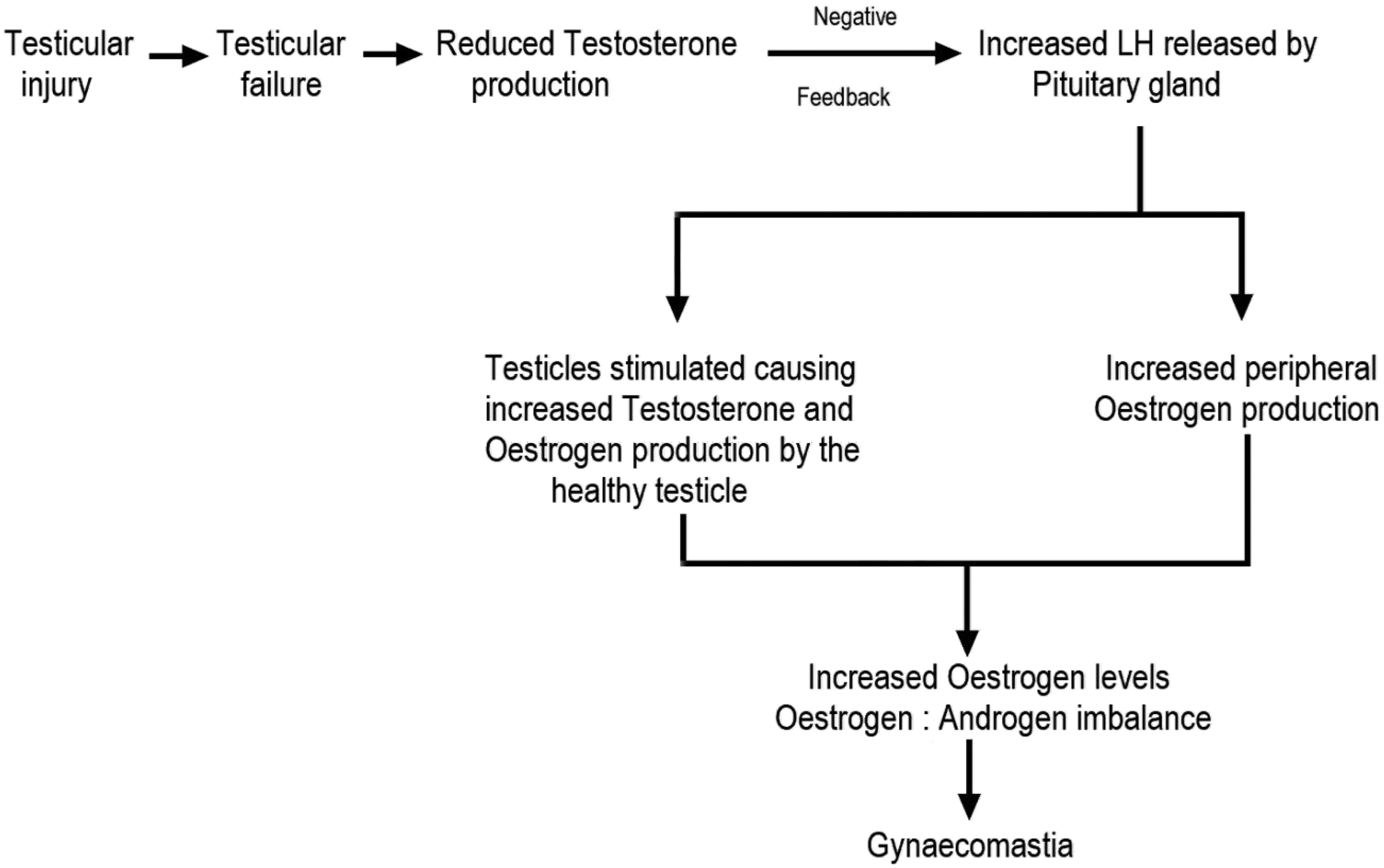
Endocrine changes in testicular failure leading to gynaecomastia.
TT is the twisting of the spermatic cord and its contents causing testicular ischaemia. Testicular failure secondary to painless TT is rare as TT usually presents with sudden, intense unilateral scrotal pain. There may be scrotal swelling, nausea, vomiting, fever and urinary symptoms. Examination may reveal ipsilateral scrotal swelling, indurated, erythematous and warm overlying scrotal skin, testicular elevation and an absent cremasteric reflex, where pinching the medial thigh does not cause the testicle to elevate. The unaffected side is usually normal (Sharp et al., 2013). TT is uncommon after puberty, and adulthood presentation is associated with delayed diagnosis, greater degrees of torsion and increased testicular loss (Ameli et al., 2016; Brungardt et al., 2021).
TT can be associated with trauma, strenuous physical activity and a congenital deformity with abnormal testicular fixation (Sharp et al., 2013). TT with a rotation below 360 degrees disturbs venous outflow, whereas arterial compromise occurs beyond 360 degrees. Presentation severity depends upon the degree of rotation and duration of the torsion. Uncorrected TT can lead to testicular ischemia, necrosis and atrophy (Brungardt et al., 2021; Nakayama et al., 2020).
Symptomatic TT is a clinical diagnosis and requires emergency surgery that should not be delayed for investigations or manual detorsion. While ultrasounds are sensitive at diagnosing TT, testicular salvage rates are time dependent and can drop to 0–10% if more than 24 hours elapses before correction (Al-Kandari et al., 2017; Sharp et al., 2013).
For patients with gynaecomastia without testicular symptoms, testicular examination should be undertaken followed by blood tests and a testicular ultrasound, to identify pathology that may be missed on examination. Findings of painless TT require referral to a urology team with treatment options including an orchidectomy for the damaged testicle, and watchful waiting or testosterone replacement therapy for the gynaecomastia. Patients with severe or distressing gynaecomastia may want to consider surgical breast reductions (Kanakis et al., 2019). This case study demonstrates the importance of testicular examination in cases of gynaecomastia.