
Abstract
Heart murmurs are a common finding during the physical examination of a child. Up to 80% of children will have a murmur at some point during their childhood. Murmurs are a reason for referral from primary to secondary care. Most murmurs, particularly beyond infancy, will be innocent murmurs which are not secondary to underlying pathology. The challenge in general practice is to identify those patients at higher risk of underlying heart disease needing further assessment and treatment by paediatric cardiology. This article aims to provide a practical approach to assessing a paediatric patient with a heart murmur in primary care and clinical scenarios comparing innocent versus pathological murmurs.
Clinical case scenario 1
Harry, a 3-year-old boy, attends your GP practice with his mother. His mother notes a 3-day history of cough, coryza, complaints of a sore throat and slightly reduced feeding.
A full set of observations are taken, which are as follows: temperature, 37.9°C; heart rate, 135 beats/min; respiratory rate, 28 breaths/min; and O2 saturations, 99%. On examination, you note erythematous, enlarged tonsils. When auscultating the chest, you note a grade 2 murmur heard primarily over the upper left sternal edge. Harry is otherwise a fit and healthy boy. He has only previously attended the surgery for his routine childhood immunisations and an episode of otitis media 1 year ago. He has no other medical history of note and there is no cardiac family history. You note that on his previous visits to the surgery no murmur was noted on examination. You plot his current weight and height on a growth chart and note that he is tracking along well on the 75th centile.
What is a heart murmur?
Heart murmurs are prolonged or extra heart sounds caused by turbulent blood flow through the heart or the great vessels (McConnell et al., 1999). While often heard in structurally normal hearts, this turbulence may be secondary to an underlying cardiac abnormality. When characterising a murmur during a cardiac auscultation, there are several factors to consider:
Timing
The first step when auscultating a murmur is assessing the precise timing of the murmur (Hoyles et al., 2010). This involves characterising S1 (the first heart sound, caused by closure of the atrioventricular valves) and S2 (the second heart sound, caused by closure of the semilunar, i.e. the aortic and pulmonary valves). A murmur heard between S1 and S2 can therefore be inferred to be systolic in nature, while a murmur auscultated after S2 but before S1 is diastolic in nature. A murmur heard throughout the cardiac cycle can be characterised as a continuous murmur.
Although identifying the timing of the murmur in relation to the heart sounds is useful and informative to work out which valve or structure may be affected, this can be challenging. Babies and younger children have a faster heart rate than adults and heart murmur timing is a skill that requires practice.
Having characterised a murmur as either systolic or diastolic in nature, the next step is to ascertain whether the murmur is heard throughout that cardiac phase or just the initial part (Hoyles et al., 2010). A murmur heard during the initial part of systole is likely an ejection systolic murmur indicative of semilunar valve stenosis or high flow through an otherwise normal valve. A murmur heard throughout the cardiac phase is either pansystolic or pandiastolic. Such murmurs could be secondary to regurgitation through a defective semilunar valve or a stenotic atrioventricular valve.
Location
The next step is to determine where on the chest the murmur is best auscultated (Figure 1). Innocent murmurs are often heard best at the left upper sternal edge. Murmurs affecting the pulmonary valve are loudest heard there. An ejection systolic murmur at this site can indicate underlying pulmonary stenosis or an atrial septal defect. A diastolic murmur here is secondary to pulmonary regurgitation. In young infants, a continuous murmur throughout systole and diastole can be occasionally auscultated at the left upper sternal edge; this is usually pathognomonic of a patent ductus arteriosus (PDA).
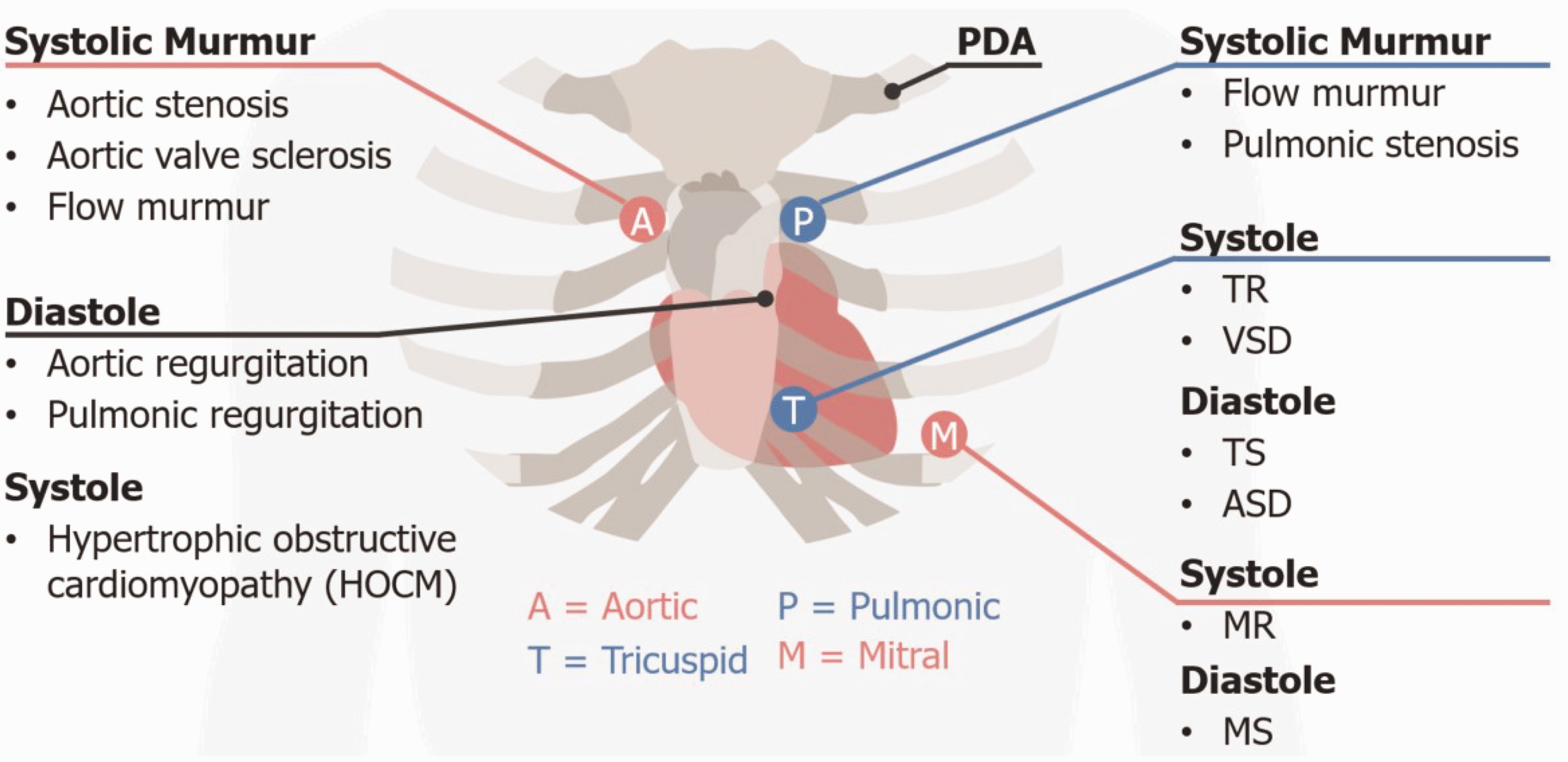
Auscultation areas and associated murmurs that are heard.
Systolic murmurs in the aortic area (i.e. the right upper sternal border are likely secondary to aortic stenosis), while a diastolic murmur there is indicative of aortic regurgitation. In addition to innocent murmurs, murmurs secondary to abnormalities of the tricuspid valve are best auscultated at the left lower sternal border. There, a pansystolic murmur could be indicative of tricuspid regurgitation, while tricuspid stenosis will be associated with a diastolic murmur. Murmurs secondary to ventricular septal defects (VSD) are pansystolic murmurs auscultated best in this region.
Murmurs associated with the mitral valve are best auscultated at the apex. A systolic murmur could indicate underlying mitral regurgitation, while a diastolic murmur could be secondary to mitral stenosis.
There are several other sites which should be auscultated during a cardiovascular examination. Murmurs associated with pulmonary stenosis radiate to the back and can be heard between the scapulae. An aortic stenosis murmur, meanwhile, radiates towards the carotid arteries. Mitral regurgitation murmurs usually radiate to the axilla. A murmur associated with coarctation of the aorta is usually best auscultated on the back.
Intensity
The intensity of the murmur can be graded on a scale of 1–6 (Ford et al., 2022). This involves the intensity of the sound as well as the presence of a thrill (Table 1).
Six different grades of murmurs with respect to the intensity of the sound.
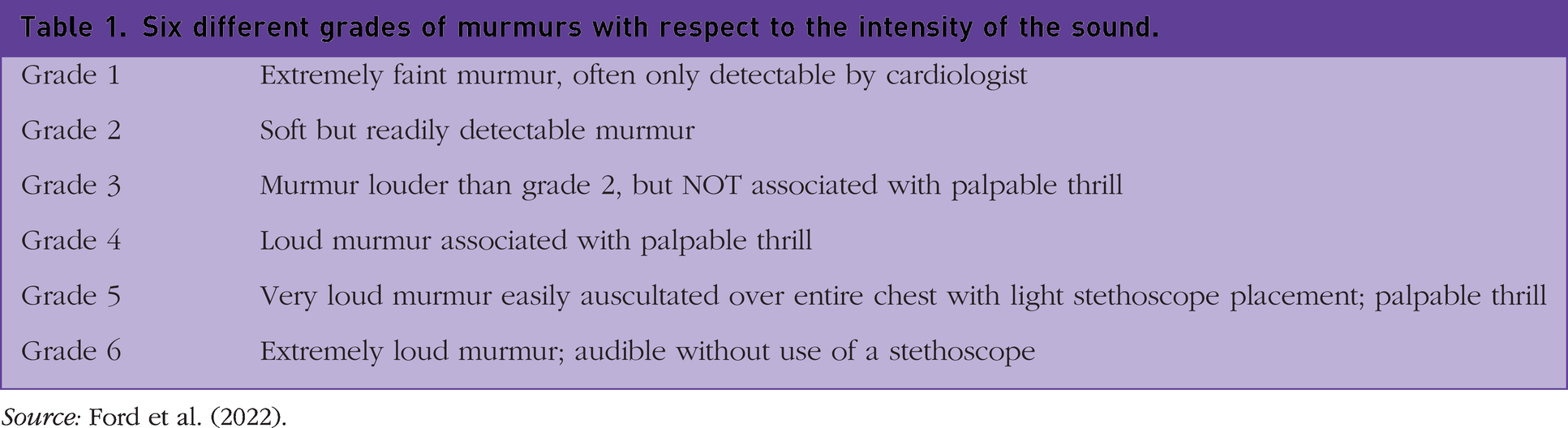
Source: Ford et al. (2022).
Systolic and diastolic murmurs.
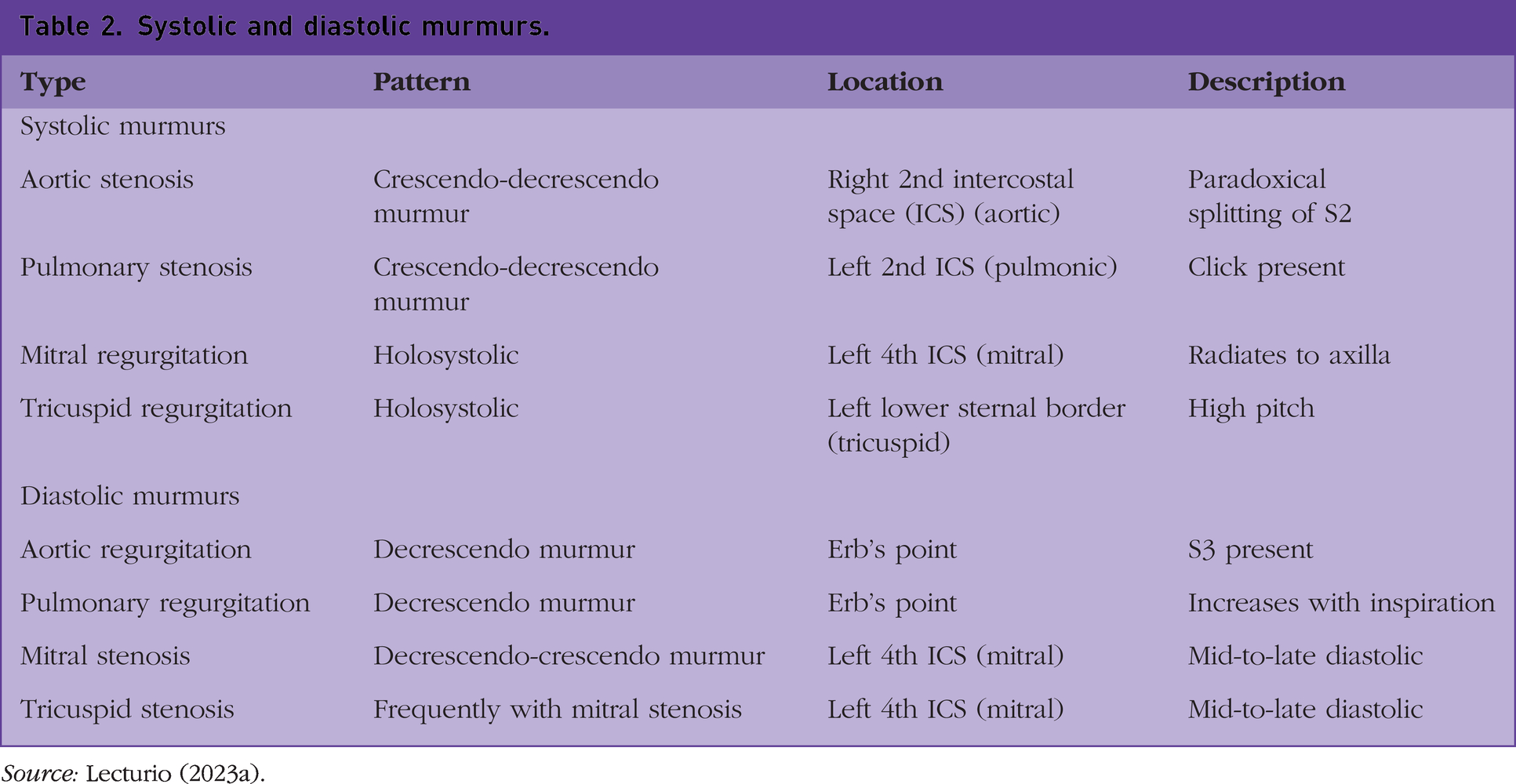
Source: Lecturio (2023a).
Character
While subjective, it is possible to describe the character or quality of the murmur. Innocent murmurs are often described as having a musical or vibratory character. The ejection systolic murmurs of aortic and pulmonary stenosis are said to be harsh in quality. Murmurs of valve regurgitation, meanwhile, are often described as blowing. Finally, the continuous murmur of a patent ductus arteriosus is often described as a machinery murmur (Hoyles et al., 2010).
Extra sounds
Occasionally, extra heart sounds, alongside S1, S2 and a possible murmur, can be auscultated. The S2 heart sound can occasionally be split – in which there is an audible delay between the closure or the aortic and pulmonary valves. This can often be physiological – audible during inspiration in a child with a structurally normal heart but disappearing on expiration. A fixed S2, not varying with respiration, can be indicative of a right ventricular overload, most commonly secondary to an ASD (Gegel, 2023).
Third and fourth heart sounds (S3 and S4) may also be heard on examination. S3 is heard in early diastole shortly after S2. It is caused by the passive flow of blood entering either ventricle and is thus auscultated best at the apex or left lower sternal border for the left and right ventricles, respectively. It is not necessarily indicative of an underlying cardiac structural abnormality and can be secondary to a hyperdynamic state, such as a fever secondary to an underlying infection or patient anxiety. It is also commonly heard secondary to ventricular septal defects. S4, meanwhile, is always pathological. It occurs shortly after S3, in late diastole. It occurs during the flow of blood from the atria to the ventricles during atrial systole. Its presence can indicate a range of conditions including ventricular hypertrophy, tricuspid or mitral valve stenosis, or hypertrophic cardiomyopathy. The presence of S3 and S4 cause a distinct quadruple heart sound, commonly called a gallop rhythm (Hoyles et al., 2010).
History-taking
Following identification of a murmur, a thorough history should be performed, covering medical background, signs and symptoms, and family history. In particular, the identification of potential red flags can help determine whether the murmur is physiological or secondary to cardiac abnormality. Slightly different approaches should be taken in infants compared to older children and adolescents.
Infants
While the majority of murmurs in asymptomatic infants are innocent, a slightly higher proportion of these murmurs are secondary to underlying cardiac abnormality compared to heart murmurs in older children; 2.5% of murmurs in infants require cardiology intervention compared to 1% of mumurs in older children (Ford et al., 2022).
As with any medical history for an infant patient, a thorough antenatal history should be taken. Areas to explore include the number and the results of antenatal imaging – although it should be noted that a normal anomaly scan does not rule out the possibility of congenital cardiac abnormalities. Antenatal ultrasound is highly operator dependant and is thought to identify only 25% of infants with cardiac abnormalities (Onuzo, 2006). Other areas to explore include maternal medication use during pregnancy. A range of medications are associated with increased risk of congenital heart disease including non-steroidal anti-inflammatory drugs (NSAIDs), angiotensin-converting-enzyme (ACE) inhibitors, phenytoin and lithium. Several maternal obstetric complications are associated with congenital heart disease, including gestational diabetes (Turunen et al., 2024), pre-eclampsia (Auger et al., 2015) and advanced maternal age (Liu et al., 2013). Congenital infections are also associated with a greater prevalence of cardiac abnormalities – up to 50% of infants with congenital rubella are diagnosed with cardiac abnormalities, in particular PDA and pulmonary artery stenosis (Reef et al., 2000).
A wide range of genetic disorders are associated with cardiac abnormalities – exploring whether the infant has been diagnosed or is currently being investigated for any particular genetic disorder – may point towards a particular cardiac diagnosis.
A thorough family history should be undertaken, particularly exploring whether any first-degree relatives have been diagnosed with congenital cardiac abnormalities, or whether there has been any unexplained child death in the family.
Following this, an exploration of red-flag symptoms should be performed. In infants, these include poor feeding, excessive sweating and/or breathlessness, particularly during feeding, cyanotic spells, and general failure to thrive/gain weight (Ford et al., 2022) (Table 3).
Red-flag symptoms suggestive of underlying cardiac pathology in infants, children and adolescents.
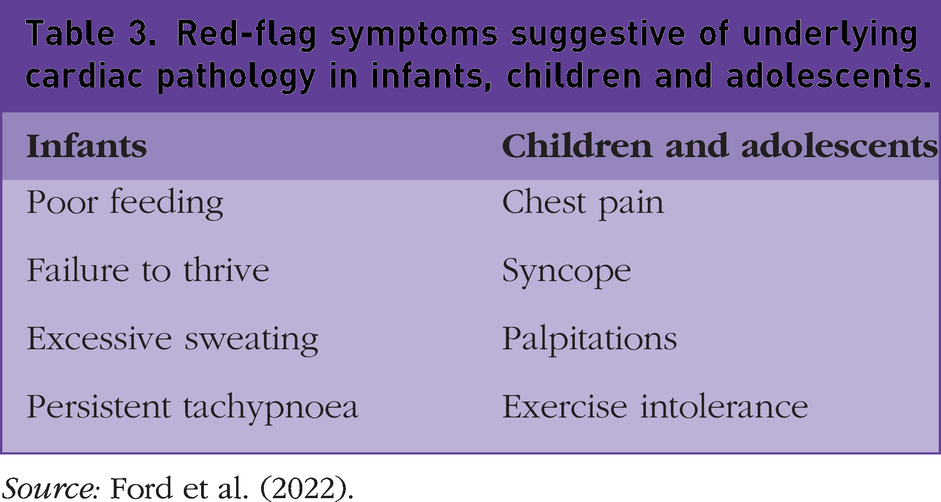
Source: Ford et al. (2022).
Children and adolescents
Murmurs in older children and adolescents are less likely to be the first sign of an undiagnosed congenital cardiac abnormality compared to an infant presenting with a murmur, although this should not be discounted entirely. A brief antenatal history should be taken but the focus should lie on the patient’s current symptoms.
Red-flag symptoms to identify include chest-pain and syncope, particularly if they are exercise-induced. A lower exercise tolerance in general when compared to their peers may also be a sign; for example, asking parents how they feel their child does in physical education during school. Also important is to explore whether the child has any recent or recurrent infections, even if relatively mild; this could point towards an innocent murmur (Yoon et al., 2020).
As with infants, a thorough family history is also warranted – exploring congenital heart disease and sudden unexpected death in young people (which could be indicative of an undiagnosed cardiac condition in this individual). In terms of medical background, it is important to note any confirmed diagnoses of genetic disorders.
Examination
A full cardiovascular examination should be performed in all patients when a murmur has been identified. A full set of baseline observations should be performed. In addition to auscultating the chest as noted above, central and peripheral pulses should be compared. Poor or absent femoral pulses may be indicative of coarctation of the aorta. Signs of heart failure should be identified, including hepatomegaly, peripheral oedema and basal lung crepitations. In infants and young children, plotting current height and weight on a growth chart and comparing to previous measurements will help quantitatively identify a patient with faltering growth.
Careful note should be made of any physical features which could be associated with an underlying genetic or phenotypic syndrome, particularly in patients without an underlying diagnosis. These include, but are not limited to, single palmar creases, facial clefts, low-set ears, slanting palpebral fissures and epicanthic folds.
Innocent murmurs
Clinical case scenario 1 describes a pulmonary flow murmur, a type of innocent murmur which is commonly associated with fever. A useful mnemonic to help differentiate innocent murmurs from pathogenic murmurs is ‘The seven S’s’ (Bronzetti and Corzani, 2010). These are as follows:
Soft – typically grade 2–3 murmurs Systolic – diastolic murmurs are always pathological Small – limited to small area of precordium no radiation Short – not pansystolic Single – no other extra heart sounds Sweet – not harsh in character Sensitive – to changes in position
Innocent murmurs can typically be categorised as one of three types (Mejia and Dhuper, 2023). These include Still’s murmurs, pulmonary flow murmurs and venous hum.
Still’s murmur
The most common of innocent murmurs, typically presenting in young children aged 3–6 years but can persist until adolescence. This murmur is typically auscultated best over the left lower sternal border and apex. It is a systolic murmur, grade 1–3, typically described as a ‘musical’ or crescendo-decrescendo. It is often heard best with the patient supine and is quieter on standing.
Pulmonary flow murmur
These are short, ejection systolic murmurs best heard at the left upper sternal border. They are associated with states of increased cardiac output and turbulence of blood flow, including fever, anaemia, anxiety, hyperthyroidism and physical exertion.
Venous hum
Venous hum murmurs are best auscultated on the upper sternal borders and just below the clavicles. They are continuous in nature and heart best when the child is sat with their head turned away from the murmur or when placing light pressure over the jugular vein.
Congenital heart disease
About 1 in 100 newly born babies are born with a congenital heart disease (CHD) making this a leading cause of death in newborn infants (Bairoliya and Fink, 2018). The incidence of critical congenital heart defects (CCHD) requiring surgical or catheter intervention in the first four weeks of life is around 0.6 out of 1000 births (Van Velzen et al., 2018). Early identification and treatment of these cases prior to neonatal collapse can lead to significantly reduced morbidity and mortality. Common signs and symptoms associated with potential CHD in infants, older children and adolescents are listed in Box 1. Signs and symptoms associated with potential CHD in infants, older children and adolescents.
A cyanotic (dusky) event post birth
A right-hand pulse oximetry <95% in air
A heart murmur noted over the precordium during the immediate post-natal period or at the newborn physical examination
Difficulty to palpate peripheral arterial pulses
An irregular heart rhythm
A first-degree relative family history of congenital heart disease
Antenatally diagnosed congenital heart disease
Chromosomal congenital anomaly or genetic syndrome
Pale grey or blue lips, tongue, or fingernails (depending on the skin colour, these changes may be harder or easier to distinguish)
Rapid breathing
Swelling in the legs, abdomen, or areas around the eyes
Shortness of breath during feeding, leading to poor weight gain
Shortness of breath during exercise or activity
Getting tired very easily during exercise or activity
Fainting during exercise or activity
Swelling in the hands, ankles or feet Source: Galvis et al. (2023).
Congenital heart disease is a group of conditions describing a structurally and anatomically abnormal heart (Galvis et al., 2023). They can be classified into two groups.
Acyanotic heart disease
In acyanotic heart disease, blood flows from the left side of the circulation to the right side through the lesion causing an increase in the pulmonary blood flow. The common finding is that infants appear pink and breathless.
Common lesions in this category are as follows:
Left-to-right shunt
Ventricular septal defect (VSD) Atrial septal defect (ASD) Patent ductus arteriosus (PDA) Atrio-ventricular septal defect (AVSD)
A special category of acyanotic heart disease is where there is obstruction of blood flow from the ventricles towards the rest of the body. The common finding is that infants appear PINK +/– COLD EXTREMITIES (or unable to easily palpate their peripheral pulses).
Common lesions in this category are as follows:
Obstructive lesions
Aortic stenosis (AS) Coarctation of aorta (CoA) Pulmonary stenosis (PS) – only the severely obstructed pulmonary valve will cause critical pulmonary stenosis that will present as cyanosis
Cyanotic heart disease
In cyanotic heart disease, blood flow is obstructed at different levels depending on the defect. Since there is a decrease in the pulmonary blood flow, these babies will appear blue (Figure 2).
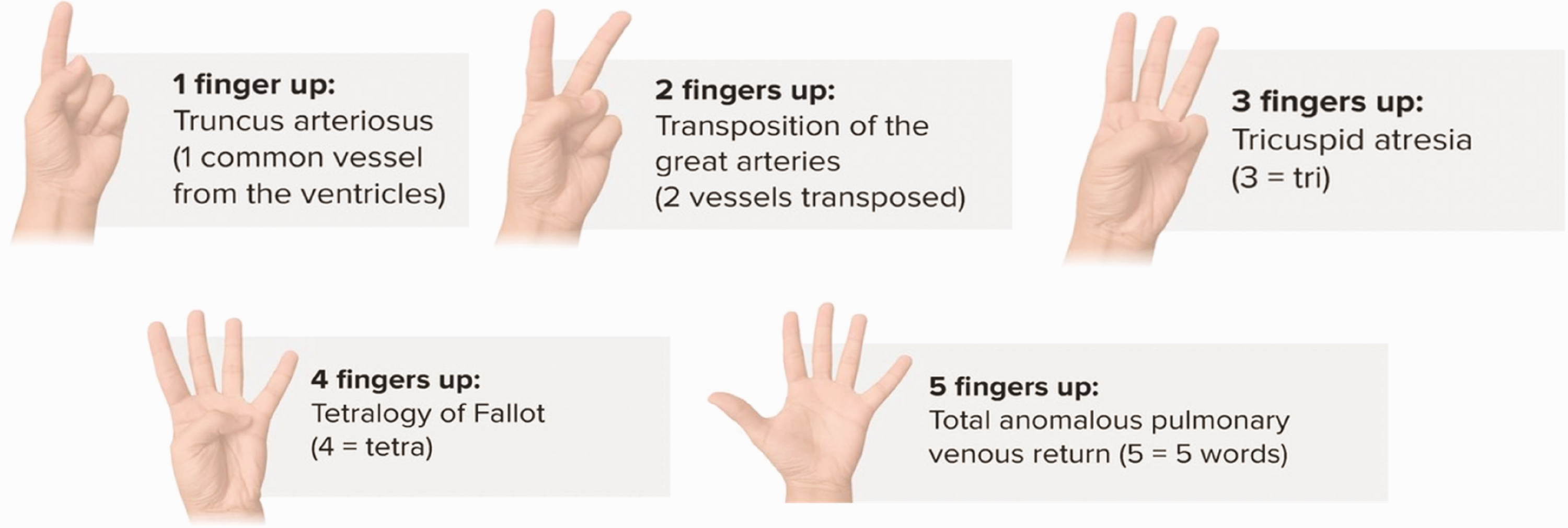
Cyanotic heart disease mnemonic using the 5 T’s + 2 P’s.
To overcome this, there needs to be some other way the blood can flow so as to bypass the obstacle. These babies usually have an associated VSD or ASD. The blood flows from the RIGHT side of the circulation to the LEFT side through these lesions, allowing mixed blood to flow towards the rest of the body.
To keep the lungs oxygenated, the ductus arteriosus needs to remain patent (PDA) to enable blood to flow from the aorta towards the lungs. This is why these defects are called duct-dependent.
Decreased pulmonary flow
Tricuspid atresia (TA) or Ebstein anomaly (EA) Tetralogy of Fallot (ToF) Pulmonary atresia (PA) or critical pulmonary stenosis (PS)
Mixed blood flow
Truncus arteriosus (TA) Transposition of great arteries (TGA) Total anomalous pulmonary venous return (TAPVR) Hypoplastic left heart syndrome (HLHS)
In mixed blood flow defects, blood mixing occurs at different levels at the same time. Blood flow and shunting is more complex (Figure 2).
Possible complications of a congenital heart defect
Congenital heart disease needs to be identified and managed early to prevent long-term complications (Lui et al., 2017). Treatment options commonly include administration of medication (such as prostaglandin E1, which relaxes smooth heart muscle and can keep the ductus arteriosus patent; propranolol, which as a beta-blocker, acts on the heart muscle to slow the heart rate and prevent the heart working too hard; or diuretics for congestive heart failure), non-surgical or minimally invasive procedures (i.e. catheters, stents, and closing devices), open heart surgery or heart transplant.
Possible complications of congenital heart disease derive from the heart defect itself or from the associated treatment (Lui et al., 2017). These include:
Congestive heart failure – including pulmonary hypertension, rapid breathing, gasping breaths, hepatomegaly, and poor weight gain Endocarditis – infection of the heart lining and valves which can lead to stroke or generalised sepsis Arrhythmias – changes in heart signalling derive from the defect itself or from the corrective surgery, which can lead to stroke or sudden cardiac death if left untreated Developmental delay – poor weight gain, generalised growth impairment and potentially neurodevelopmental delay Mental health disorders – anxiety or stress related to developmental delay, activity restrictions or learning difficulties
Differential diagnosis
During diagnostic evaluation, it is important to recognise that signs and symptoms of congenital heart disease can be similar to other conditions (Griffiths and Ellis, 1971). These include includes sepsis, congenital infections, respiratory disorders, hypoxia, meconium aspiration syndrome, persistent pulmonary hypertension of the newborn (PPHN), genetic disorders, alcohol use, drug use, chemotherapeutics/immunosuppressives, radiation, and so on.
Clinical case scenario 2
Kristy is a 5-week-old infant who presents to your surgery with a snotty nose, a cough, and mildly increased work of breathing. Her older sibling has similar symptoms, and the mother tells you that the whole family suffers from a cold. Kristy was born full-term, with a birthweight of 3.6 kg, to a healthy mother. Both the pregnancy and delivery were uncomplicated. No resuscitation was required at birth and she has been healthy up until a week ago. You initially suspect a diagnosis of bronchiolitis. On examination, Kirsty appears pale. Her observations are as follows: heart rate 147 beats/min and O2 saturations 98% in room air with mild subcostal recession. There is a systolic murmur on auscultation which you note is loudest when listening posteriorly and both femoral pulses appear weak.
You suspect coarctation of the aorta and refer urgently to the paediatric emergency department for further investigations – including pre- and post-ductal saturations and blood pressure measurement – and input regarding management from paediatric cardiology
Coarctation of the aorta
Coarctation of the aorta is a form of acyanotic congenital heart disease found in approximately 1 in 2900 live births (Van Der Linde et al., 2011). If the narrowing (coarctation) of the aorta is severe, it may cause damage to the heart, high blood pressure in the heart and brain, and affect the organs in the lower body that don't receive enough oxygenated blood. Symptoms of coarctation of the aorta depend on its severity and the child’s age. Newborns usually present with increased work of breathing, pale appearance, difficulty in feeding, weak femoral pulses and a difference in pre-ductal/post-ductal saturations. A high index of suspicion is required for early diagnosis as most symptoms mimic other common neonatal conditions such as bronchiolitis. Older children usually present with high blood pressure in the upper limbs, a heart murmur which is usually a harsh systolic murmur with radiation to the back, shortness of breath especially when exercising, muscle weakness, leg cramps, cold feet, nose bleeds and headaches (Joshi et al., 2017).
Management and further investigation
Following a thorough history and examination, the decision must be made whether to refer the patient for further assessment with an echocardiogram and a clinical review by a paediatric cardiologist. There is no ‘one rule that fits all; and each patient should be assessed on a case-by-case basis.
Identification of red-flag signs and symptoms from the history and examination can help determine which patients necessitate onwards referral. A lower threshold for referral should be considered for infants, even in the absence of red-flag signs and symptoms, due to the higher likelihood that the heart murmur is secondary to a previously undiagnosed congenital cardiac abnormality.
Older patients, if otherwise clinically well with no concerning signs and symptoms elicited during the assessment, can be safely followed up in primary care initially without tertiary referral. If suspecting a pulmonary flow murmur, it may be useful to re-assess the patient in the following weeks when the potential cause of the murmur, such as fever in clinical case scenario 1, has resolved.
In infants, a cautious assessment includes thorough history taking and physical examination even when the clinical condition mimics a more common presentation such as in clinical case scenario 2. A strong clinical suspicion of congenital heart disease is enough to justify a referral to paediatric cardiology even if there is a report of a normal antenatal anomaly scan.
Previous practice suggested chest X-rays and electrocardiogram (ECG) are useful first steps for further investigation. Evidence suggests that chest X-rays and ECGs were not cost-effective and likely to cause misdiagnosis of a murmur as benign or pathological (Rajakumar et al., 1999). Four-limb blood pressure readings, previously routinely used particularly in infants to help diagnose coarctation, were found to offer poor specificity if a 5 mmHg cutoff was utilised, and poor sensitivity if utilising a 15 mmHg cutoff (Crossland, 2004). In fact, wide variation of up to 20 mmHg can be seen in healthy neonates and, if coarctation of the aorta is suspected, then this can only be excluded or confirmed by echocardiography.
The routine Newborn Infant Physical Examination (NIPE) identifies 53% of CHD cases prior to collapse (Aranguren Bello et al., 2019). Pulse oximetry screening improves detection of critical cases by identifying those with low oxygen saturations and those with a pre-ductal versus post-ductal difference > 2% at any point after 2 minutes of continuous credible trace (Ewer et al., 2011). A meta-analysis of over 457 000 babies has shown that pulse oximetry screening has a 76.3% sensitivity and 99.9% specificity for the detection of CHD (Plana et al., 2018). When used in combination with NIPE examination, the sensitivity for critical CHD detection is estimated to be 87–95% (Aranguren Bello et al., 2019).
In conclusion, all patients with red-flag signs and symptoms, or with a confirmed or suspected genetic diagnosis associated with cardiac abnormalities, should be referred for further assessment by a paediatric cardiologist. Patients in whom an innocent murmur is the most likely diagnosis can be safely followed up in primary care. Cases with clinical doubt or in which the murmur persists for a prolonged length of time justify a discussion with paediatric cardiology.
Key points
Up to 80% of children have a murmur at some point during their childhood
Most of these murmurs, particularly beyond infancy, will be innocent murmurs and not secondary to underlying pathology
Following identification of a murmur, a thorough history should exclude congenital heart defects; covering medical background, signs and symptoms, and family history (specifically of cardiac conditions and/or sudden unexplained child death)
Red-flag symptoms in infants include poor feeding, excessive sweating and/or breathlessness, cyanotic spells, and faltering growth or slow weight gain
Red-flag symptoms in older children include chest pain, syncope, low exercise tolerance and recurrent infections
A strong clinical suspicion of congenital heart disease is enough to justify a referral to paediatric cardiology even if there is a report of a normal antenatal scan
{kind=link}