
Abstract
Case history
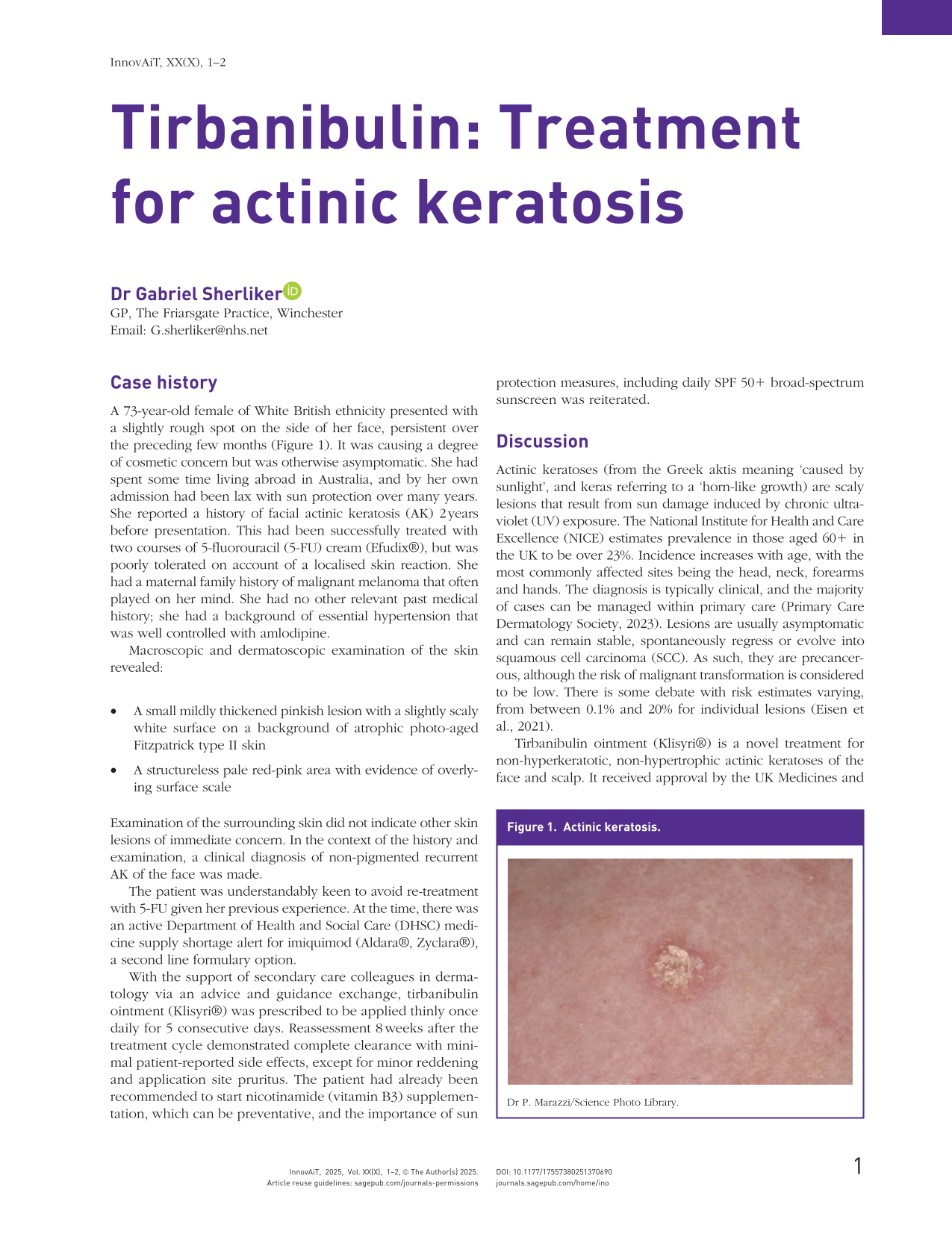
A 73-year-old female of White British ethnicity presented with a slightly rough spot on the side of her face, persistent over the preceding few months (Figure 1). It was causing a degree of cosmetic concern but was otherwise asymptomatic. She had spent some time living abroad in Australia, and by her own admission had been lax with sun protection over many years. She reported a history of facial actinic keratosis (AK) 2 years before presentation. This had been successfully treated with two courses of 5-fluorouracil (5-FU) cream (Efudix®), but was poorly tolerated on account of a localised skin reaction. She had a maternal family history of malignant melanoma that often played on her mind. She had no other relevant past medical history; she had a background of essential hypertension that was well controlled with amlodipine.
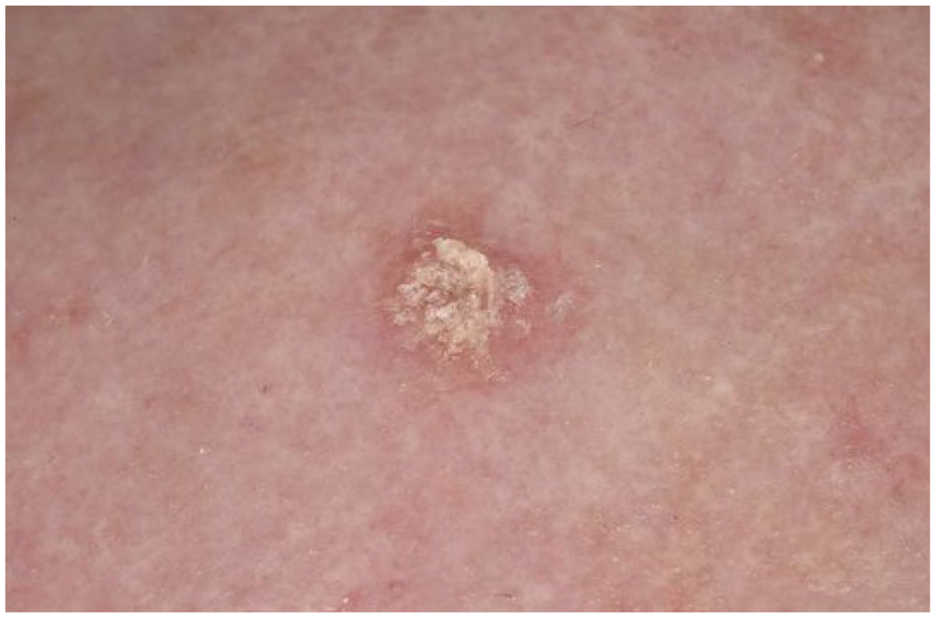
Actinic keratosis.
Macroscopic and dermatoscopic examination of the skin revealed:
A small mildly thickened pinkish lesion with a slightly scaly white surface on a background of atrophic photo-aged Fitzpatrick type II skin
A structureless pale red-pink area with evidence of overlying surface scale
Examination of the surrounding skin did not indicate other skin lesions of immediate concern. In the context of the history and examination, a clinical diagnosis of non-pigmented recurrent AK of the face was made.
The patient was understandably keen to avoid re-treatment with 5-FU given her previous experience. At the time, there was an active Department of Health and Social Care (DHSC) medicine supply shortage alert for imiquimod (Aldara®, Zyclara®), a second line formulary option.
With the support of secondary care colleagues in dermatology via an advice and guidance exchange, tirbanibulin ointment (Klisyri®) was prescribed to be applied thinly once daily for 5 consecutive days. Reassessment 8 weeks after the treatment cycle demonstrated complete clearance with minimal patient-reported side effects, except for minor reddening and application site pruritus. The patient had already been recommended to start nicotinamide (vitamin B3) supplementation, which can be preventative, and the importance of sun protection measures, including daily SPF 50+ broad-spectrum sunscreen was reiterated.
Discussion
Actinic keratoses (from the Greek aktis meaning ‘caused by sunlight’, and keras referring to a ‘horn-like growth) are scaly lesions that result from sun damage induced by chronic ultraviolet (UV) exposure. The National Institute for Health and Care Excellence (NICE) estimates prevalence in those aged 60+ in the UK to be over 23%. Incidence increases with age, with the most commonly affected sites being the head, neck, forearms and hands. The diagnosis is typically clinical, and the majority of cases can be managed within primary care (Primary Care Dermatology Society, 2023). Lesions are usually asymptomatic and can remain stable, spontaneously regress or evolve into squamous cell carcinoma (SCC). As such, they are precancerous, although the risk of malignant transformation is considered to be low. There is some debate with risk estimates varying, from between 0.1% and 20% for individual lesions (Eisen et al., 2021).
Tirbanibulin ointment (Klisyri®) is a novel treatment for non-hyperkeratotic, non-hypertrophic actinic keratoses of the face and scalp. It received approval by the UK Medicines and Healthcare products Regulatory Agency (MHRA) in 2021. It is a tyrosine kinase inhibitor that has an anti-neoplastic mechanism of action by disrupting tubulin polymerisation among several other effects, thereby inducing apoptosis. It is applied topically once daily for 5 consecutive days, and treatment efficacy is best assessed after 8 weeks. It comes in single-use sachets that must be discarded after opening and contain enough ointment for a treatment area of up to 25 cm² (5 × 5 cm) (British National Formulary, 2025).
In phase 3 clinical trials, tirbanibulin demonstrated a favourable side effect profile while proving to be an effective treatment option after only a short duration of use. It is only approved for treatment of lesions on the face and scalp at this time. Common side effects are mild pruritus and discomfort at the site of application. Less common adverse reactions, included erythema, swelling, crusting, flaking, scaling, vesiculation, pustulation, erosion and ulceration. Alternative therapies, however, such as 5-FU, imiquimoid and diclofenac require lengthy topical treatment durations with more severe cutaneous reactions, factors often limiting tolerability and adherence (Dao et al., 2022).
This fictional case study describes a presentation of recurrent facial AK that was effectively managed with a 5-day application of tirbanibulin with minimal patient-reported side effects following previous poorly tolerated use of 5-FU. Tirbanibulin should be considered as a favourable and effective treatment for AK.