
Abstract

Introduction
The Simulated Consultation Assessment (SCA) places a strong emphasis on patient-centred care. It is important not only to gather the necessary data to support clinical decision-making, but also to demonstrate the skills required to reach a shared management plan with your patient. The SCA is an exam, currently comprising of approximately nine 12-minute video consultations and three phone consultations.
We have previously discussed how the hourglass model effectively represents the consultation process (Back and Goode, 2014). The hourglass is divided into two parts, mirroring the consultation itself: the first half focuses on data gathering, while the second half is dedicated to agreeing on a management plan with the patient (Figure 1). The hourglass also serves as a reminder to manage time carefully, ensuring time is left to complete the second half of the consultation. Another key component of the SCA is your general consultation skills, including your ability to relate to the patient and understand the psychosocial impact of their condition.
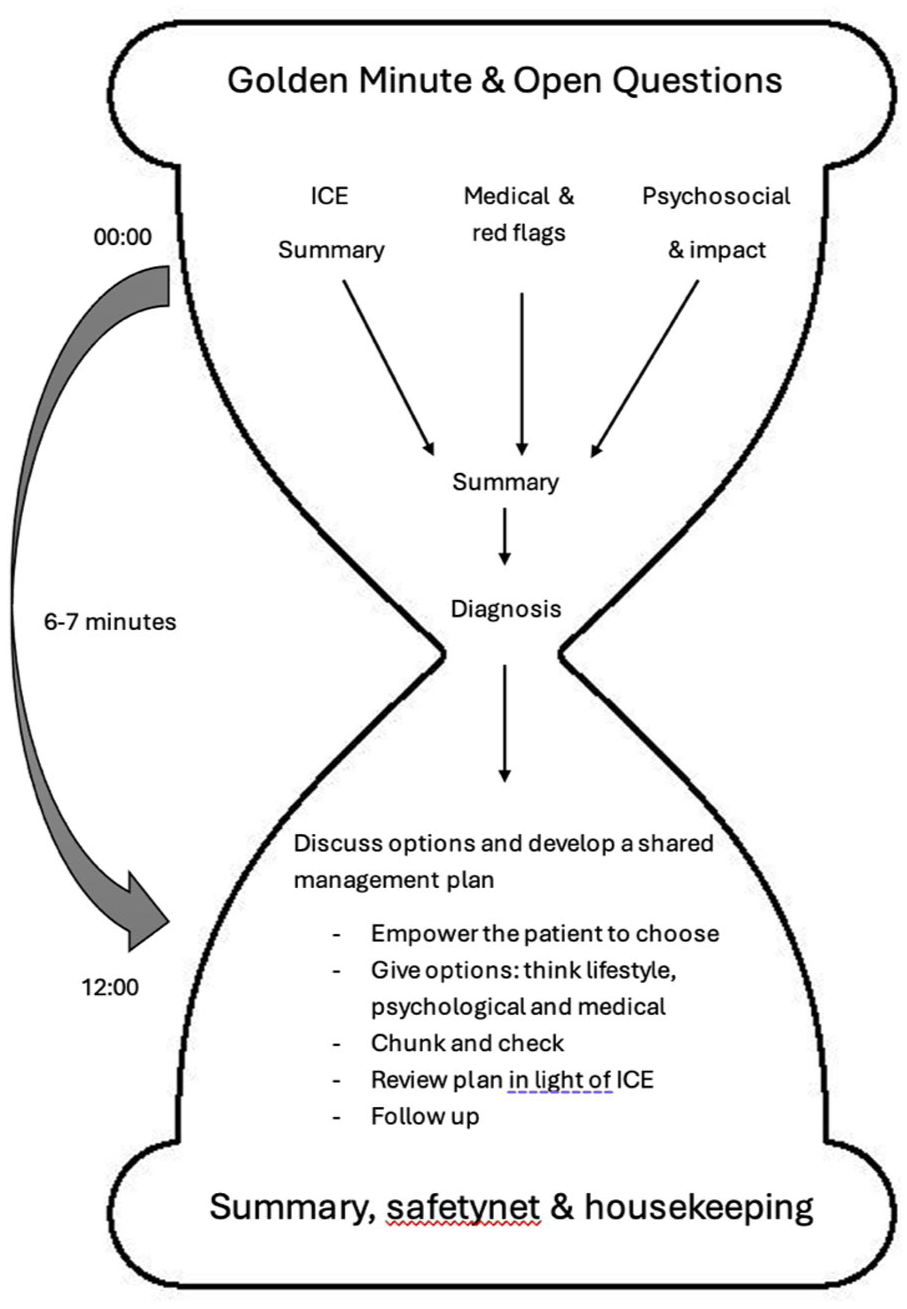
The hourglass model.
Below is a breakdown of the hourglass model, outlining our approach to structuring consultations. This framework is not only valuable for the SCA but also beneficial throughout a GP’s career. This is not new; these concepts were developed by brighter GP’s than us many years ago. We have adapted these concepts and put them into a format that we find useful. Hopefully you do too.
The golden minute
The patient’s initial statement, often called the ‘opening gambit’, typically summarises their problem in one or two sentences. The concept of ‘the golden minute’ highlights the importance of allowing the patient uninterrupted time to speak. While it may be tempting to interject, it is essential to remain silent, maintain good eye contact and use non-verbal encouragement to support the patient. Pay close attention to verbal and non-verbal cues that may provide useful information.
Open and closed questions
It is important to start with broad, open questions and gradually narrow down to more specific closed questions, reflecting the shape of the hourglass. We recommend asking more than one open question, for instance a second question could be ‘tell me more’. Closed questions are typically used to identify red flags and are answered with ‘yes’ or ‘no.’ These usually follow the first summary and exploration of the patient’s ideas, concerns and expectations (ICE) (McKelvey, 2010).
Summary
Roger Neighbour places great importance on summarising the patient’s narrative early in the consultation (Neighbour, 2004). An early summary helps clarify the clinical picture and demonstrates active listening as well as giving the patient the chance to correct any inaccuracies. It may also reveal further insight into the patient’s ICE. At this stage, it is helpful to ask, ‘Is there anything else?’ – this is especially useful if the patient has multiple concerns.
Ideas, concerns and expectations
Ideas, concerns and expectations (ICE) is a widely recognised concept in consultation skills (Pendleton et al., 1984). Understanding the patient’s agenda is key. You may have already elicited this information through earlier questions, but it is important to verify it verbally. Explicitly stating ICE is essential, as marks cannot be awarded for unvoiced insights. Instead of asking the patient directly, ‘What are your ideas, concerns and expectations?’, it is more effective to break it down into manageable sections using alternative phrasing, such as ‘thoughts, worries and hopes’. Additionally, understanding how patients’ issues affect their lives adds psychosocial context, which is important both for patient rapport and the SCA scoring (Edwards et al., 2023).
Further data gathering
Further data gathering involves more targeted, closed questions. Remember to cover all relevant areas, including past medical history, red flags, drug history (including over-the-counter and online medications) and family history.
Psychosocial context
It is important to understand how the patient’s problem impacts their daily life. Consider whether the diagnosis may have implications for the patient. For example, do they do a job that involves driving? Do they live alone? Are they a carer? Are they self-employed? These details are essential for patient safety and will also enhance your overall SCA performance.
Summary
Summarising at the end of data gathering helps ensure that all relevant information has been collected accurately. It also provides an opportunity to ask, ‘Is there anything else on your mind?’ or ‘Is there anything I have not covered?’
Diagnosis and differentials
Aim to transition to the second part of the consultation around halfway through – ideally between 6 and 7 minutes, and no later than 8 minutes. At this stage you should present a working diagnosis, possibly with differentials. It does not need to be a definitive diagnosis but should lead towards a management plan.
Revisiting ICE
Readdressing the patient’s ICE demonstrates strong communication and consultation skills. It is useful to link the patients concerns to the diagnosis – for example, a patient with a headache who fears a brain tumour may actually have a migraine. This is an ideal moment to explain your reasoning and offer reassurance.
Shared management
Patient-focused consulting is important not just in the SCA but also in everyday general practice. It is important to present management options clearly and simply, breaking them down into lifestyle changes, psychological approaches (if applicable), medication or onward referral. This part of the consultation should be a ‘tennis match’, allowing the patient to process the options and provide feedback. As Silverman et al. (2004) advise, avoid presenting all options in one long explanation – instead, ‘chunk and check’ the information.
Follow-up and safety-netting offer
For the SCA it is important to follow up when indicated. Use this time to explain that the condition may change and advise the patient on what to do if it does, including the urgency of any new symptoms. Signposting to out-of-hours services is helpful but avoid unnecessary catastrophising. Follow-up and safety netting should be appropriate for the specific condition.
Summary
Ending your consultation with a brief summary provides a valuable opportunity to confirm that the patient understands the management plan and any necessary follow-up. You can invite the patient to summarize the key points themselves, which reinforces their understanding, though this isn’t always necessary.