
Abstract
Medical tourism describes the phenomenon of individuals travelling from their home country to another destination with the intention of accessing medical care. It is a rapidly growing industry, with the number of UK citizens seeking medical treatment abroad rising annually. The increasing popularity of medical tourism presents both opportunities and challenges to the individual and the NHS. Therefore, it is imperative that patients make informed decisions regarding travelling abroad for medical treatment. This article will explore the development of medical tourism, focusing on the legal and ethical issues before considering a case scenario.
Case scenario
Mr Smith, a 35-year-old gentleman books an appointment with his GP to discuss weight management options. He explains that he has struggled with his weight for over a decade, having tried various supervised diets, exercise programmes and weight loss medications ordered online. He has had limited long-term success with these efforts to lose weight. His body mass index (BMI) is 45 kg/m2. He is increasingly frustrated by his inability to lose weight and the impact on his physical and mental health. He would like to be referred for weight loss surgery on the NHS; however, he is aware of the long waiting times for treatment. Mr Smith shares a story about his friend who had a gastric sleeve operation in Poland at a reasonable cost and has successfully lost 10 stone since. He asks for your advice on bariatric surgery abroad and wonders if this could be a good option for him. What are the legal and ethical concerns surrounding medical tourism? What advice would you give Mr Smith?
The development of medical tourism
Medical tourism has been popular for centuries. People have travelled all over the world in pursuit of better health. Some 4500 years ago, travellers visited India seeking the ‘body and mind cleansing’ health benefits of traditional medical practices like Ayurveda (Badulescu and Badulescu, 2014; Shi et al., 2021). Ancient Greeks crossed the Mediterranean Sea to visit the Sanctuary of Asklepios at Epidarus for its ceremonial healing practices (Badulescu and Badulescu, 2014). Romans, recognising and valuing the natural curative properties of hot springs and thermal baths, built numerous spas across their empire (Badulescu and Badulescu, 2014). A famous example is the city of Bath in England, which is known as a place of healing and a health tourist hotspot (Shalini et al., 2024). Later, in the early 20th century, wealthy individuals travelled to sanatoriums in the Alps, believing that high altitude and fresh, clean air could cure tuberculosis. Published in 1924, Thomas Mann’s novel, ‘The Magic Mountain’, offered a glimpse into the lives of patients and the treatments they received in the Schatzalp sanatorium in Davos, Switzerland (Riva, 2014).
Traditionally, travelling abroad for medical treatment was an expensive and exclusive privilege reserved for the wealthy and upper social classes. However, in today’s world, the accessibility of international travel has contributed to an explosion in the number of people travelling abroad for advanced medical treatments (Shalini et al., 2024). Propelled by expanding communications worldwide and the internet-driven marketing of medical tourism opportunities, a large and diverse range of individuals now participate in medical tourism. The UK is a popular location for inward medical tourism today, with individuals travelling from all over the world to access high quality medical care and specialised treatments (ONS, 2021). However, there has also been a surge in the number of patients travelling from high and middle-income countries to low-income countries for medical care (Armitage, 2025; Badulescu and Badulescu, 2014). UK outward medical tourism is growing in popularity. The Office for National Statistics estimates there were 523 000 UK residents travelling abroad for medical care in 2024 (ONS, 2025).
In the UK, outward medical tourism is an attractive option for patients wishing to avoid the prolonged NHS waiting times for treatment. Individuals can access medical care unavailable on the NHS and, relative to the UK private healthcare, treatment costs are significantly lower (Armitage, 2025). This is a strong determining factor as most medical tourism arrangements are funded by patients themselves (Snyder et al., 2015). Furthermore, medical tourism can align with patients’ cultural, religious or personal preferences. They can access medical care environments where they feel more comfortable or in a country that shares their ethnic background or language. Many patients also appreciate the opportunity to combine medical care with a holiday destination through ‘medical package holidays’ (Armitage, 2025). The offer of high levels of customer service and luxury healthcare facilities alongside personalised treatment plans appeals to many individuals.
The top 10 most popular destinations for UK outward medical tourists according to the Office for National Statistics are Turkey, with an estimated 196 000 visits for medical treatment in 2024, followed by Poland (64 000), Romania (52 000), Portugal (32 000), India (22 000), Italy (17 000), Lithuania (16 000), Spain (15 000), Greece (11 000) and Czechia (10 000) (ONS, 2025). The medical treatments sought after most often by UK residents are fertility treatments, cosmetic surgery, bariatric surgery and dental procedures (POST, 2020).
Legal issues in medical tourism
In the UK, healthcare facilities, including NHS and private hospitals, GP practices, walk-in centres, out-of-hours services and care homes, are regulated and inspected by the Care Quality Commission (CQC) (POST, 2020). Overseas medical tourism facilities are not subject to the same regulation, but initiatives have been developed to help standardise patient care. International organisations and accreditation bodies have set international standards to promote the safety, quality and ethical practices of medical tourism facilities. For example, the Joint Commission International (JCI) and the International Organisation for Standardisation (ISO) provide internationally recognised guidelines. These guidelines focus on patient safety and care quality, infection control, continuity of care and patient rights (ISO, 2025; JCI, 2025).
The primary legal issue with medical tourism is the lack of adherence by some medical tourism facilities to international standards (Wahed, 2015). Quality assurance systems can vary significantly across different countries. Consequently, destination countries may have different standards of medical care resulting in inconsistencies in the quality of care given to patients. An extreme example of this is the high number of patient deaths after cosmetic surgery (e.g. ‘the Brazilian butt lift’) abroad. The ‘Brazilian butt lift’ is known as ‘the deadliest aesthetic surgery procedure’ (Finkelstein et al., 2024) and inquests have found serious issues with the quality of care received by patients (Nugent, 2024; Pazmiño and Garcia, 2023). Poor quality of care may present in a number of ways, including inadequate patient information or poor aftercare. Language barriers, lack of resources and varying legal standards can all limit the quality of care provided (Pillai and Mondal, 2024). Patients should be encouraged to conduct their own research and be well-informed about international standards to recognise facilities that meet these standards.
Another legal issue brought about by medical tourism is the discrepancy in laws around the world on medical malpractice (Kundury et al., 2024). In the UK, when a medical professional or organisation breaches their duty of care towards a patient leading to injury or harm, patients can take legal action claiming medical malpractice with the potential to receive compensation (Bryden and Storey, 2011). However, in some medical tourist destinations, these legal avenues are complex and much harder to navigate making it difficult to seek justice and legal remediation (Wahed, 2015). It is vital that patients conduct thorough research to select reputable, accredited providers backed by clear and easily accessible legal processes to minimise the risk of the legal pitfalls of medical tourism.
There is also a lack of regulation governing the marketing of medical treatment abroad. Patients can be heavily influenced by online advertisements, social media influencers and glossy clinic websites promising miracle medical procedures and quick fixes. GPs can help patients to recognise marketing hyperbole and focus on clinical credibility, long-term outcomes and realistic expectations. This mitigates risks and supports informed decision making, following the GMC’s Good Medical Practice, which states doctors have a duty to support patients to make informed decisions about their care (GMC, 2025).
Another responsibility of medical professionals registered with the GMC is to contribute to continuity of care, promptly sharing all relevant information about patients with others involved in their care (GMC, 2025). A GP must be satisfied that the person providing care has the appropriate qualifications, skills and experience to provide safe care for the patient. Shared care agreements with overseas clinics can pose challenges due to the varying regulatory requirements, differing clinical guidelines and language barriers (Baylis, 2023). GPs should request discharge letters, preferably written in English, from the overseas clinic to facilitate continuity of care.
Following treatment overseas, aftercare processes can be complex. A legal duty and professional responsibility of GPs is to recognise and work within the limits of their competence (GMC, 2025). There can be significant indemnity, jurisdictional and legal risks for doctors providing follow-up care for patients having medical treatment abroad. Medical professionals must only practice under the level of supervision appropriate for their role, knowledge, skills and training (GMC, 2025). If a patient requires follow-up care after treatment abroad, GPs must assess whether they have the competence, adequate information and ability to safely monitor the treatment. If not, patients should be referred to an appropriate specialist in secondary care (Parr, 2023).
Ethical considerations in medical tourism
We will explore the ethical implications of medical tourism using the four pillars of medical ethics: beneficence, non-maleficence, autonomy and justice (Figure 1). The principles of medical ethics are critically important as they provide a clear, balanced framework for ethical decision-making in medicine. Beneficence and non-maleficence encourage doing good and avoiding harm. Autonomy promotes patient-centred care, ensuring patients are active participants in decisions about their own health. Justice ensures that resources are allocated fairly between patients and distributed justly, supporting equity in healthcare.
A diagram depicting the four pillars of medical ethics.
Beneficence
The first ethical principle to consider is the overall beneficence of medical tourism to the patient. Individuals seek healthcare abroad to improve their health and access medical care sooner, therefore enhancing their quality of life (Shalini et al., 2024). Medical tourism can offer access to more advanced care than is available in the UK, including highly specialised procedures or expertise to enhance patient health and recovery. A number of medical treatments are unavailable on the NHS due to poor cost-effectiveness (Armitage, 2025). Medical tourism allows patients to access these treatments at a reasonable cost. For example, cosmetic surgery, which is typically unavailable on the NHS and more affordable overseas, can improve a patient’s life significantly, having a positive impact on mental health and wellbeing (Castle et al., 2002). Another example is the provision of life extending medication Trastuzumab Deruxtecan for the treatment of HER2 positive breast cancer, which is considered too high cost for provision by the NHS. However, it is available in other European countries via medical tourism (Armitage, 2025). In such treatment, medical tourism follows the ethical principle of beneficence by helping people achieve positive outcomes.
Some medical tourism may go against the principle of beneficence because some providers recommend unnecessary or inappropriate procedures to maximise profit, as well as contrary to the patients’ best interests (Badulescu and Badulescu, 2014). Certainly, the quality and oversight of overseas medical providers can vary widely, resulting in discrepancies in the care provided and potentially poorer patient outcomes.
Non-maleficence
The second medical ethical principle to explore is non-maleficence. It can be argued that medical tourism alleviates suffering and minimises harm by enabling patients to access treatment more quickly, avoiding prolonged NHS waiting times. However, overseas procedures can put patients at risk of life-threatening and serious complications because of discrepancies in quality of care (Armitage, 2025). There may be a lack of continuity of care and follow up on return home resulting in an increased risk of harm. To help minimise harm caused to patients, it is important for doctors to provide the necessary information to patients about the procedure they are undergoing alongside the risks and complications associated with it to help patients make well-informed, autonomous decisions about their care (Armitage, 2025).
Autonomy
The third ethical principle is respect for the patient’s autonomy. Medical tourism promotes a patient’s right to make informed decisions about their own care. It offers treatment not available or affordable in their home country and allows individuals to take control of their healthcare decisions and timelines. Patients are not then subject to the uncertainty associated with NHS waiting times. If an individual can understand the risks, benefits and uncertainties of undergoing a procedure overseas and can make informed decisions, these decisions should be valued and protected.
While treatment abroad promotes patient autonomy, there are informed consent risks to consider. These risks arise from language barriers, limited disclosure of risks and cultural differences leading to provision of incomplete or misleading information for patients (Nugent, 2024). Furthermore, understanding legal protections in the host country in the event of medical malpractice is crucial for autonomy (Snyder et al., 2015). It can be challenging for patients to fully comprehend these protections before undergoing treatment. Doctors have a duty to keep their knowledge up to date and provide advice to help patients make autonomous decisions about medical tourism (Armitage, 2025).
As previously discussed, medical tourism provides accessibility to treatments unavailable or prohibitively expensive within an individual’s home country. However, financial strain or desperation can influence decisions about medical care abroad, potentially compromising patient autonomy.
Justice
The final principle of justice ensures resources are distributed equitably between patients based on clinical need (Armitage, 2025). One viewpoint is that medical tourism helps alleviate strain on the NHS due to patients not having treatment at a cost to the NHS and paying themselves to go overseas for medical care. This aligns with the ethical pillar of justice because NHS resources can be distributed to other patients with greater clinical need. Furthermore, in destination countries, the medical tourism industry can fund infrastructure and jobs, boosting long-term public health investment and promoting health equity.
However, it can be argued that medical tourism contradicts the ethical principle of justice by increasing strain on the NHS from complications arising after medical care abroad. It has been estimated that the cost of addressing such complications is greater than the cost of receiving the treatment on the NHS (Armitage, 2025). Furthermore, inward medical tourism in the UK is costly to the NHS. Between 2021 and 2024, over £250 million in charges for NHS medical care provided to overseas patients remains unrecovered. This amount is equivalent to the annual salaries of 3200 GPs or the cost of building 68 new GP surgeries (Wolfson, 2025). This demonstrates how inward medical tourism impacts the potential distribution of NHS resources and the overall sustainability of the NHS.
In destination countries, medical tourism has led to the emergence of two-tier healthcare systems (Wahed, 2015). This occurs when private tourist hospitals are favoured over public local hospitals due to the boost they bring to the economy. A study in India reported that local adults and children have worsening life prospects as they are unable to get the medical care they need due to redirection of resources and healthcare professionals to profitable private tourist hospitals (Meghani, 2013). This highlights how medical tourism can exacerbate healthcare inequalities.
This short exploration of the legal implications and ethical issues of medical tourism is not comprehensive, and there are many more considerations for both patients and medical professionals to consider when looking at the impact of medical tourism at both ends of the patients’ journey.
Case scenario review
It is estimated that approximately 5000 people travel from the UK each year to have bariatric surgery overseas, which is similar to the 4500 patients receiving bariatric surgery on the NHS annually (Aggarwal and Ahmed, 2024).
For the case scenario of Mr Smith, the 2016 National Institute for Health and Care Excellence (NICE) guidance states that ‘bariatric surgery can improve the quality of life and reduce the risk of premature mortality, and is the main option of choice for adults with a BMI of 40 kg/m2 or more, or between 35 kg/m2 and 39.9 kg/m2 with a significant health condition that could be improved if they lost weight’ (NICE, 2016). There are strict eligibility criteria for referral for bariatric surgery on the NHS. Patients must be referred to a specialist weight management clinic first, attempt various non-surgical weight loss methods and be committed to long-term lifestyle changes (NICE, 2016). Once referred for bariatric surgery, patients can face prolonged waiting times of over 1 year (NHS, 2025). Therefore, for Mr Smith, accessing bariatric surgery abroad is an attractive option, avoiding the long waiting times associated with NHS treatment and offering lower costs compared to private healthcare in the UK.
Mr Smith’s case highlights an ethical dilemma between the limitations of the NHS and the individual’s health needs. Applying knowledge of the four pillars of medical ethics, his GP can respect Mr Smith’s autonomy and support his health decision by providing comprehensive, honest and balanced advice. To promote beneficence and non-maleficence, his GP should help Mr Smith to be aware of potential risks and how to reduce them. The patient should be encouraged to conduct thorough research and select medical facilities accredited by reputable organisations and adhering to international guidelines (see examples such as the JCI and the ISO in the References and further information). The final principle to uphold is justice. This involves striking a balance between fairness for all NHS patients and the duty to care for individuals like Mr Smith who have made independent healthcare decisions.
The consultation with Mr Smith should be documented thoroughly, including the risks discussed and his understanding. Reliable informational resources about medical tourism safety, regulatory issues and follow-up needs should also be provided (Figure 2). The patient should be directed to the NHS website, in particular the ‘Going abroad for medical treatment’ and ‘Treatment abroad checklist’ pages (NHS, 2023a,b). Another valuable resource for patient information is the ‘Travelling abroad for medical treatment questions’ on the Fitfortravel website (see References and further information). It is important to review this patient in the future and consider referring Mr Smith to an NHS dietician or psychologist to support lifestyle changes, regardless of his decision.
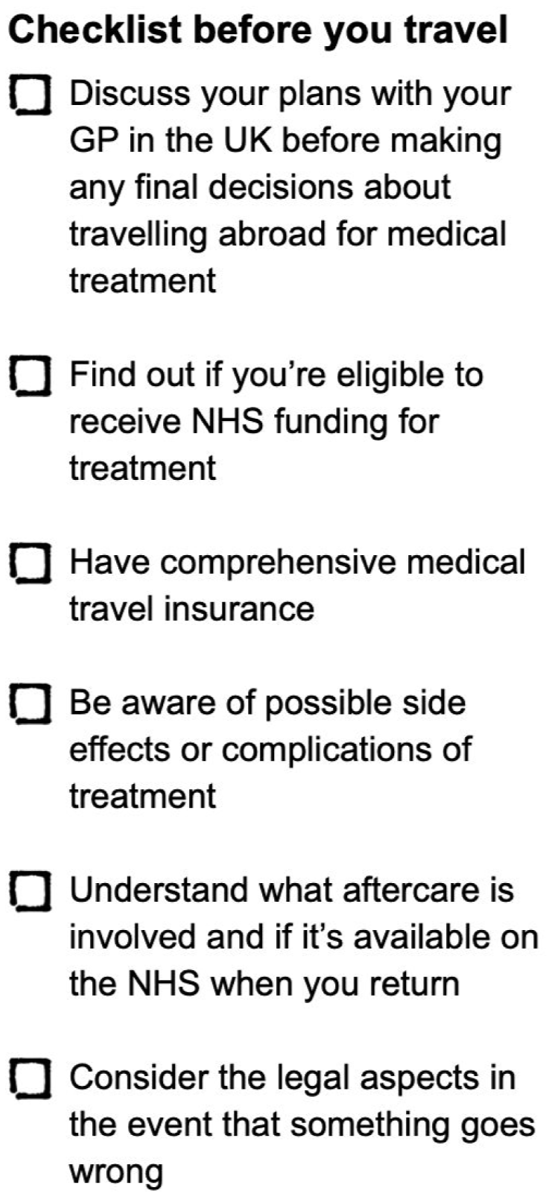
Checklist for patients considering travelling abroad for medical treatment.
Postoperatively, NICE guidance recommends people are offered a follow-up care package for a minimum of 2 years within the bariatric service including ‘monitoring nutritional intake (including protein and vitamins) and mineral deficiencies, monitoring for comorbidities, medications review, individualised dietary and nutritional assessment, advice and support on physical activity, psychological support tailored to the person and information about professionally led or peer support groups’ (NICE, 2016). The guidance recommends follow up ‘as part of a shared-care model with primary care’ for those undergoing bariatric surgery in the UK. For individuals like Mr Smith undergoing bariatric surgery privately abroad, many GP practices are not able to offer routine follow-up services on the NHS (Parr, 2023). Patients are instead advised to seek a private follow-up programme in the UK for a 2-year period (Parr, 2023). NHS coverage for ongoing care after bariatric surgery and other private medical treatment abroad is limited, with follow-up care only covered if it is an urgent or life-threatening emergency. Therefore, prior to patients undergoing treatment in another country, they should be encouraged to plan for follow-up care responsibly, understanding and respecting the limitations of the NHS.
Key points
Medical tourism, the practice of travelling to another country for medical care, is a rapidly growing industry, with the number of UK citizens travelling abroad for medical treatment increasing every year
Medical facilities around the world offer opportunities to avoid prolonged waiting times, access medical care unavailable on the NHS, and have reduced treatment costs relative to the UK private healthcare system
Seeking healthcare elsewhere raises legal and ethical concerns
Medical tourism can improve an individual’s quality of life, but it is important to consider the unique risks associated with destination procedures, such as complications and a lack of continuity of care
Patients considering medical tourism should be encouraged to thoroughly research and select reputable, accredited providers to minimise risks and ensure ethical practices