
Abstract

Menopause marks the final cessation of ovarian follicular activity and is most often defined retrospectively after 12 months of amenorrhoea. In the UK, the average age at menopause is roughly 51 years. The menopausal transition is a pivotal turning point in women’s cardiometabolic health. Falling oestrogen concentrations drive a redistribution of adipose tissue from a gynecoid to an android pattern, promote dyslipidaemia, insulin resistance, hypertension and a pro-inflammatory state, and trigger vasomotor symptoms (VMS) such as hot flushes and night sweats. VMS appear to signal a higher risk of cardiovascular disease even after adjustment for established risk factors. This article advocates a precision menopause management approach. Such an approach integrates symptom relief with evidence-based interventions to mitigate long-term cardiovascular morbidity. A practical algorithm is proposed for GPs and illustrated with a case vignette. The proposed approach aligns with key guidelines from the British Menopause Society (BMS) and the National Institute for Health and Care Excellence (NICE) guidelines on cardiovascular risk and menopause.
Clinical case scenario part 1
Patient A is a 52-year-old schoolteacher who presents with worsening hot flushes, night sweats and poor sleep. Her last menstrual period was 14 months ago. She reports mood swings and cognitive ‘fog’. Her father suffered a myocardial infarction at 55 years, and a maternal aunt had breast cancer. She is a non-smoker and consumes alcohol moderately. Her body mass index (BMI) is 29 kg/m², and her waist circumference is 92 cm. Her blood pressure in the clinic is 142/88 mmHg. Fasting lipids show total cholesterol 6.2 mmol/L, low-density lipoprotein-cholesterol (LDL-C) 3.8 mmol/L, high-density lipoprotein cholesterol (HDL-C) 1.3 mmol/L and triglycerides 2.0 mmol/L. HbA1c is 39 mmol/mol (5.7%), and liver function tests are normal. Her QRISK3 score is 12%.
Patient A is assessed as post-menopausal with moderate to severe VMS adversely affecting her quality of life. She has central adiposity, borderline hypertension and dyslipidaemia. Her 10-year cardiovascular risk exceeds the 10% threshold for statin therapy (NICE, 2025). There is no personal history of breast cancer or venous thromboembolism, although her family history confers moderate breast cancer risk. Her mood symptoms warrant further assessment.
What is menopause?
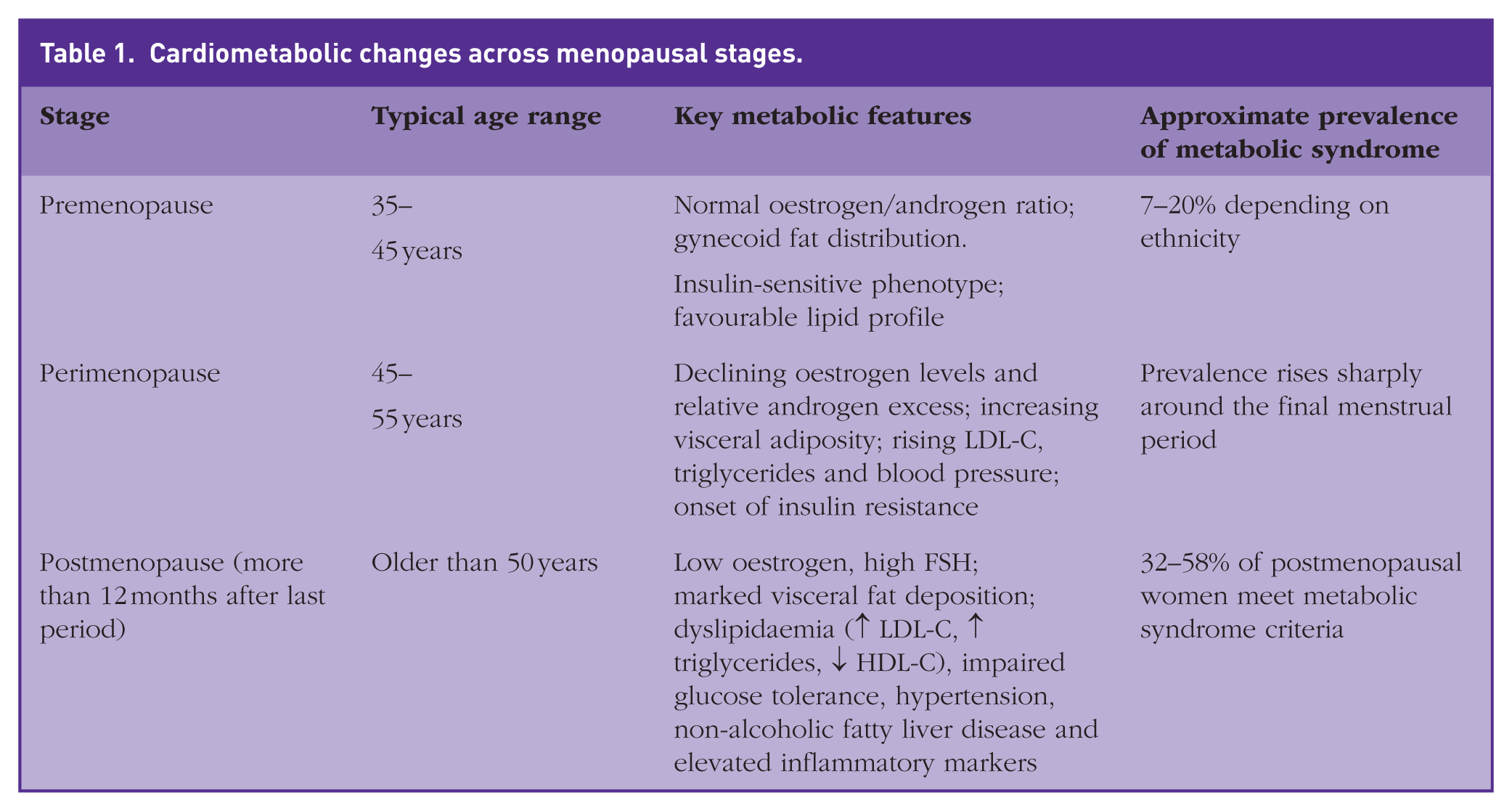
Menopause is diagnosed retrospectively after 12 consecutive months without menstruation and usually occurs between 45 and 55 years of age. In the UK, the mean age is 51 years. Oestrogen deficiency underpins classic symptoms such as hot flushes, night sweats, mood changes, vaginal dryness and sleep disturbance. For many women, the symptom burden is severe and persists for several years. The endocrine milieu shifts from predominantly oestrogenic to relatively androgenic; sex hormone-binding globulin (SHBG) concentrations decline, increasing bioavailable testosterone (El Khoudary et al., 2020). Follicle-stimulating hormone receptors expressed on visceral adipocytes are activated by high circulating follicle-stimulating hormone (FSH) levels, promoting adipocyte hypertrophy and lipogenesis. These hormonal changes explain the centripetal redistribution of fat and tendency towards developing metabolic syndrome; these metabolic disturbances are summarised in Table 1.
Cardiometabolic changes across menopausal stages.
Vasomotor symptoms and cardiovascular risk
There is substantial heterogeneity in the severity and duration of perimenopausal symptoms. An important question is whether women who experience severe menopausal symptoms, particularly VMS, are at increased risk of adverse cardiometabolic outcomes.
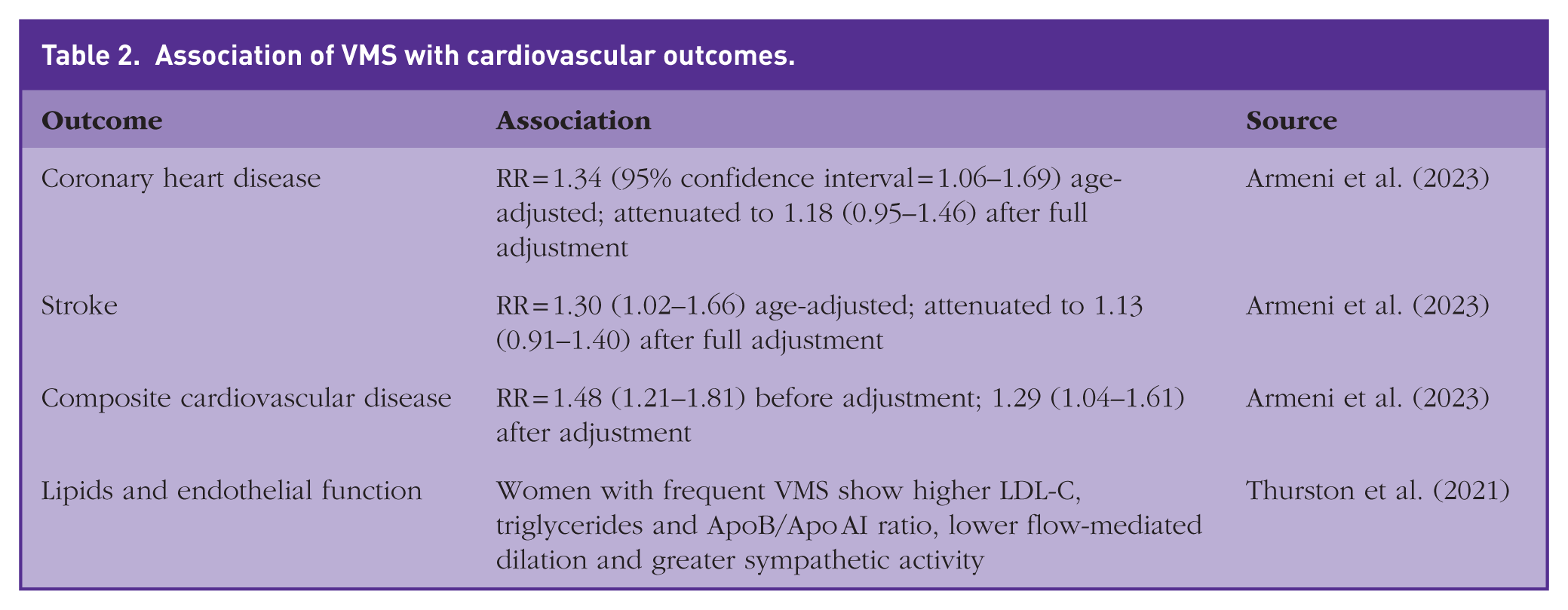
Population-based evidence suggests that VMS may serve as a biomarker of underlying cardiovascular risk. A meta-analysis of ten prospective cohort studies involving >213 000 women demonstrated that the presence of menopausal symptoms was associated with a higher risk of coronary heart disease (relative risk (RR) = 1.34), stroke (1.30) and composite cardiovascular disease (CVD) (1.48) compared with asymptomatic women (Armeni et al., 2023) (Table 2). Adjustment for conventional risk factors attenuated the associations but did not abolish them, indicating that VMS tend to cluster with metabolic risk factors. Data from the Study of Women’s Health Across the Nation (SWAN) further strengthen this link. Women reporting frequent VMS had higher LDL-C, triglycerides and apolipoprotein (Apo) B, and a higher ApoB/Apo A1 ratio than women without VMS (Thurston et al., 2021). These associations persisted after adjustment for demographic factors and endogenous hormones; VMS were also associated with poorer endothelial function and higher sympathetic tone. Higher BMI and central adiposity are also associated with more frequent and severe VMS in cohort studies, suggesting that obesity may exacerbate symptoms, as well as share common pathophysiological pathways with cardiometabolic risk. Thus, the occurrence of VMS should prompt clinicians to undertake cardiovascular risk assessment.
Association of VMS with cardiovascular outcomes.
Evidence for early hormone replacement therapy and the timing hypothesis
The Women’s Health Initiative (WHI) trial published in 2002 enrolled women with a mean age of 63 years and reported increased risks of breast cancer, stroke and venous thromboembolism with conjugated equine oestrogen plus medroxyprogesterone acetate. These findings led to a precipitous decline in hormone replacement therapy (HRT) use and shaped subsequent guideline recommendations. Subsequent analyses and newer trials, however, highlighted that the impact of HRT depends critically on the timing of initiation relative to the menopausal transition.
The ‘timing hypothesis’ proposes that the cardiovascular effects of HRT are critically dependent on the age at initiation and proximity to menopause onset. According to the 2020 American Heart Association Scientific Statement, initiation of HRT in healthy women younger than 60 years or within 10 years of menopause is associated with favourable cardiovascular and survival outcomes. In contrast, delayed initiation beyond this window may attenuate or reverse these benefits (El Khoudary et al., 2020). This concept is reinforced by a systematic review and meta-regression analysis of randomised and observational studies, which demonstrated that early HRT initiation significantly reduced all-cause mortality and coronary heart disease, with no benefit when treatment commenced after age 60 years or more than 10 years post-menopause (Nudy et al., 2019). The Danish Osteoporosis Prevention Study provided long-term randomised evidence supporting this paradigm: among 1006 recently post-menopausal women followed for 16 years, HRT reduced composite cardiovascular events by 52% (hazard ratio = 0.48) and all-cause mortality by 43% after 10 years (Schierbeck et al., 2012).
Collectively, these data support the timing hypothesis as a framework for improving cardiovascular safety when HRT is initiated earlier in the menopausal transition; however, they do not provide sufficient evidence to recommend HRT as a primary or secondary cardiovascular prevention therapy. NICE, North American Menopause Society (NAMS) and the American College of Cardiology (ACC) all interpret these findings to mean that appropriately selected women who start HRT before age 60 years, or within 10 years of menopause, have low absolute cardiovascular risk on treatment, but HRT should not be prescribed with the primary aim of reducing coronary events or stroke (Cho et al., 2023; NICE, 2024; North American Menopause Society [NAMS], 2022).
HRT route and progestogen considerations
The route of oestrogen administration has important implications for safety. Oral oestrogens undergo first-pass hepatic metabolism, increasing clotting factor synthesis and inflammatory markers. The American College of Obstetricians and Gynecologists (ACOG) note that orally administered oestrogen exerts a pro-thrombotic effect, whereas transdermal oestrogen has little or no impact on pro-thrombotic pathways and may even improve inflammatory profiles (ACOG, 2013). A multicentre case–control study reported that oral oestrogen users had a four-fold higher risk of venous thromboembolism (odds ratio ≈ 4.2) compared with non-users, whereas transdermal oestrogen was not associated with increased risk. Synthetic progestins, such as medroxyprogesterone acetate or norethisterone, further increase thrombotic risk; by contrast, micronised (bio-identical) progesterone appears neutral (ACOG, 2013).
Endometrial protection is mandatory when prescribing oestrogen to women with an intact uterus. A systematic review commissioned by the British Menopause Society (BMS, 2024a) concluded that oral micronised progesterone, when given at 200 mg/day for 12–14 days/month, provides adequate endometrial protection for up to 5 years. The BMS emphasises that progestogen dose should be proportionate to oestrogen dose – higher doses of oestrogen require a higher progestogen dose – and that levonorgestrel intrauterine systems provide effective endometrial protection for up to 5 years. Compounded ‘bio-identical’ progesterone creams are discouraged because absorption is unreliable and there is no evidence of endometrial protection.
Types of HRT
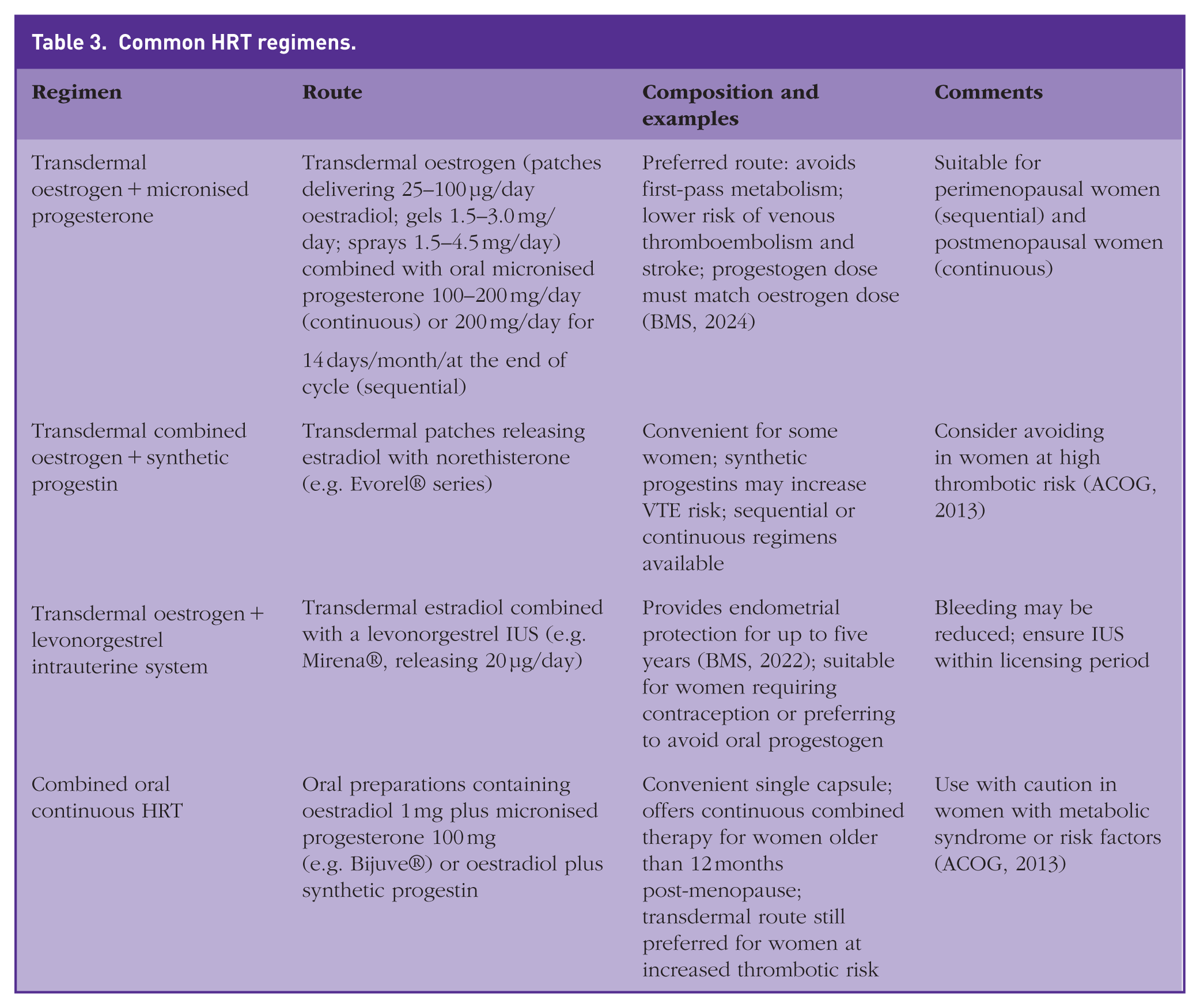
HRT regimens should be individualised according to menopausal status, uterine status and patient preference. Women with an intact uterus require both oestrogen and progestogen; those without a uterus can use oestrogen alone. Transdermal preparations are generally preferred because they avoid first-pass hepatic metabolism and have a lower risk of thrombosis and stroke. Table 3 depicts the commonly used HRT regimens.
Common HRT regimens.
HRT safety, contraindications and breast cancer risk
Absolute contraindications to systemic HRT include known or suspected breast or endometrial cancer, oestrogen-dependent neoplasia, undiagnosed vaginal bleeding, untreated endometrial hyperplasia, previous or current venous thromboembolism or arterial thromboembolic disease, active liver disease and porphyria. The BMS cautions against initiating HRT in women with a 10-year cardiovascular risk of at least 10%, uncontrolled hypertension (exceeding 180/110 mmHg) or severe dyslipidaemia (total cholesterol exceeding 7.8 mmol/l or triglycerides exceeding 4.5 mmol/L) (BMS, 2024). However, for women with stable ischaemic heart disease or after myocardial infarction, low-dose transdermal oestrogen with a non-androgenic progestogen may be considered, provided risk factors are optimised (BMS, 2024b).
The risk of venous thromboembolism is dose- and route-dependent. Oral HRT increases the risk two- to five-fold, whereas transdermal oestrogen does not elevate the risk (ACOG, 2013). Micronised progesterone is neutral, but synthetic progestins increase the risk of thrombosis. Unopposed oestrogen leads to endometrial hyperplasia in up to 62% of women after 3 years; adequate progestogen or an intrauterine device is therefore essential (BMS, 2024a) (Table 4).
Progestogen dose per licensed transdermal oestrogen dose.
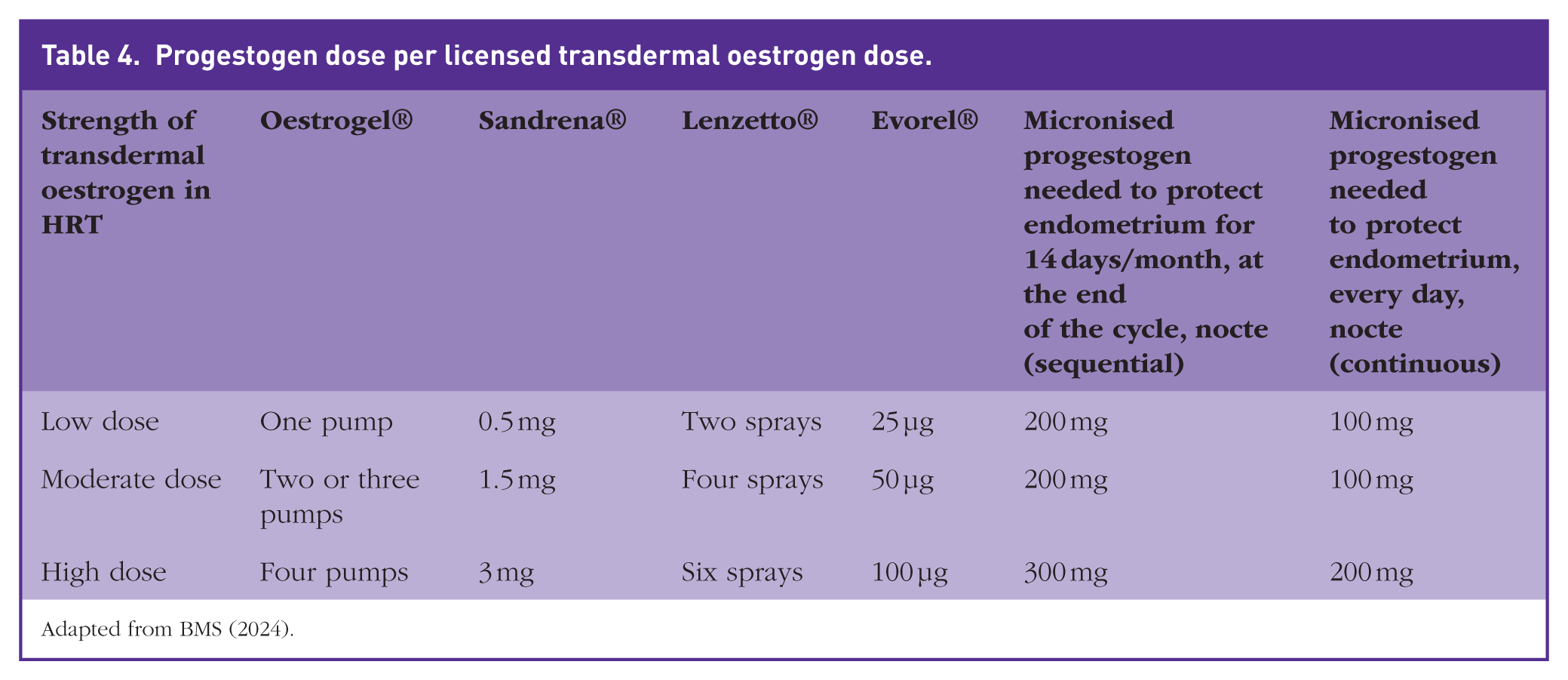
Adapted from BMS (2024).
Breast cancer risk
According to the NICE menopause guideline decision aid (NICE, 2024), the absolute increase in breast cancer risk associated with HRT is low. For women aged 50–69 years, the baseline risk of breast cancer over 5 years is approximately 59 per 1000. Combined oestrogen–progestogen HRT raises this to about 79 per 1000, equating to an additional 20 cases per 1000 women over 5 years. Oestrogen-only HRT increases risk to about 69 per 1000 (i.e. 10 additional cases per 1000 women). These data should be communicated during shared decision-making.
Precision menopause management: a practical framework for GPs
Precision menopause management seeks to tailor therapy to a woman’s symptomatic, metabolic and psychosocial profile. Figure 1 summarises a proposed clinical pathway that integrates cardiometabolic assessment with symptomatic management and shared decision-making.
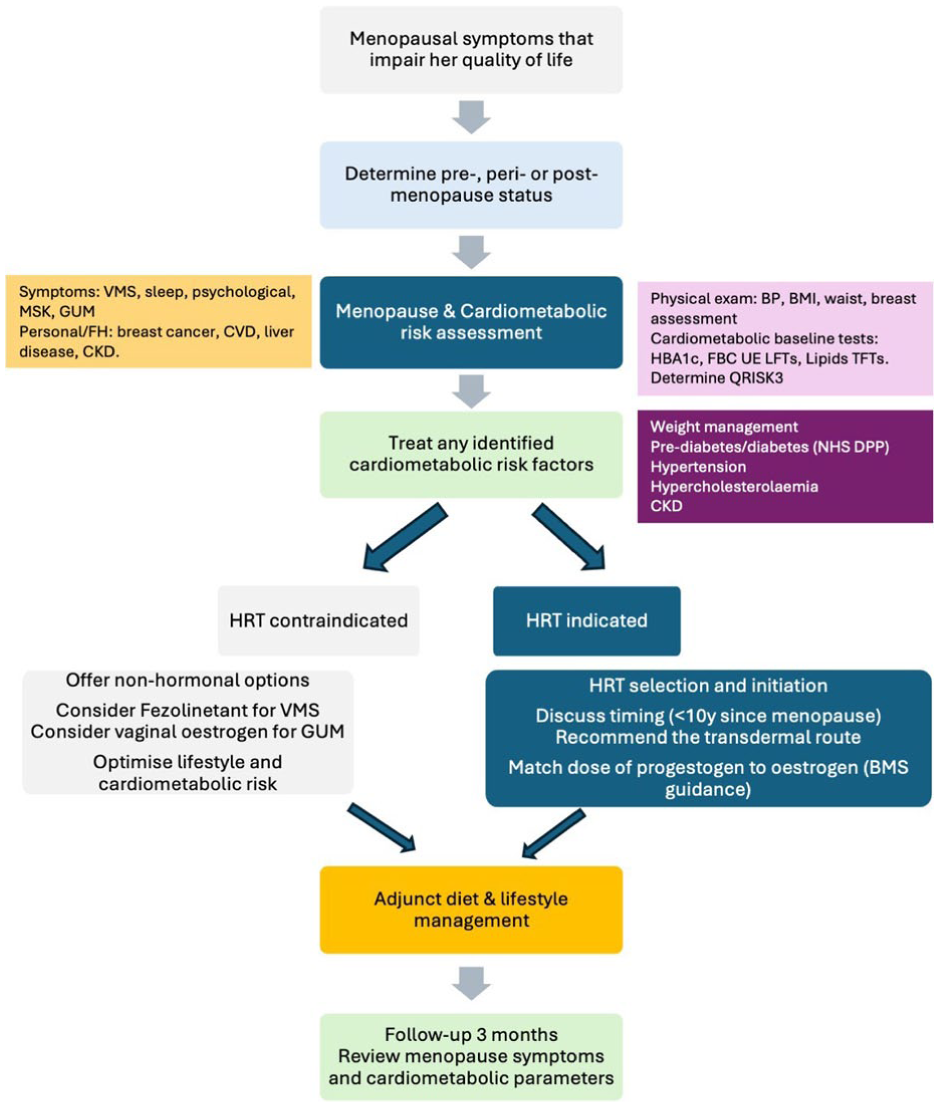
Precision menopause management algorithm.
Precision menopause management algorithm
Menopause confirmation and symptom assessment
Establish whether the woman is perimenopausal (irregular bleeding with symptoms) or postmenopausal (more than 12 months of amenorrhoea). Elicit the frequency and severity of hot flushes, night sweats, sleep disturbance, mood changes, cognitive complaints, sexual dysfunction and urogenital symptoms. Document quality-of-life impact and personal treatment goals. Exclude differential diagnoses such as thyroid dysfunction.
Comprehensive cardiometabolic assessment
Take a detailed medical, family and obstetric history focusing on cardiovascular risk factors (smoking, hypertension, diabetes, dyslipidaemia, premature CVD in relatives), endocrine disorders and history of venous thrombosis or hormone-sensitive cancers. Perform blood pressure measurement, anthropometry (weight, body mass index and waist circumference) and cardiovascular examination. Order baseline investigations: fasting lipid profile, fasting glucose or HbA1c, liver function tests, thyroid function and renal function. Calculate the 10-year cardiovascular risk using the QRISK3 tool (ages 25–84 years). Women with a QRISK3 score of 10% or higher should be prioritised for lifestyle intervention and statin therapy (NICE, 2025). In practice, HRT for severe menopausal symptoms does not always need to be delayed until a full QRISK3 calculation is available, provided there are no obvious contraindications; cardiovascular risk assessment can be completed opportunistically at early follow-up.
Identify contraindications and relative cautions
Review absolute contraindications (breast cancer, endometrial cancer, unprovoked venous thrombosis, severe liver disease) and assess whether symptoms can be managed without hormonal therapy. For women with a uterus requiring oestrogen, ensure endometrial protection with a levonorgestrel intrauterine system (LNG-IUS) or oral micronised progesterone (BMS, 2024a). In women with a history of hormone-sensitive cancer, venous thrombosis or severe cardiovascular disease, consider non-hormonal options and refer to a specialist menopause clinic. High CVD risk (QRISK3 of 10% or higher) is not an absolute contraindication but mandates optimisation of risk factors and a preference for transdermal oestrogen (BMS, 2024b).
Selecting the appropriate HRT regimen
If HRT is indicated and there are no contraindications, discuss the timing hypothesis with the patient. Initiation within 10 years of menopause, or before age 60 years, is associated in some studies with more favourable cardiovascular and mortality outcomes than later initiation, although major guidelines (NICE, NAMS, and ACC) do not recommend HRT as a cardioprotective therapy. Explain the advantages of transdermal oestrogen – stable serum levels, minimal hepatic first-pass effect and lower venous thromboembolism risk – and recommend a LNG-IUS or adding oral micronised progesterone 100–200 mg/day in continuous or cyclical regimens to protect the endometrium (BMS, 2024a). For women who prefer oral therapy, Bijuve® (oestradiol 1 mg + micronised progesterone 100 mg) offers a continuous combined formulation. Counselling should include potential side effects (breast tenderness, bloating, unscheduled bleeding), the small increase in breast cancer risk, and the need for regular review.
Managing cardiometabolic risk factors
Lifestyle modification remains foundational. Advise a Mediterranean-style diet rich in vegetables, whole grains, lean protein and unsaturated fats, while limiting processed foods, refined carbohydrates and free sugars. Encourage at least 150 minutes of moderate-intensity aerobic activity per week and muscle-strengthening activities twice per week. Counsel on weight management, smoking cessation and moderation of alcohol intake. Address sleep hygiene and psychosocial stressors. Monitor blood pressure and treat hypertension to current targets. Offer atorvastatin 20 mg daily for women with a QRISK3 score of 10% or higher as recommended by NICE (2025); consider therapy even at lower scores if there is concern that QRISK3 underestimates risk. Escalate lipid-lowering therapy in line with secondary prevention targets (LDL-C no greater than 2.0 mmol/L or non-HDL-C no greater than 2.6 mmol/L) should cardiovascular disease be subsequently diagnosed. Manage impaired glucose tolerance with metformin and refer to diabetes prevention programmes when appropriate. For women with fatty liver, emphasise weight reduction, limit alcohol and reserve hepatology referral for those with clinical or biochemical features suggestive of advanced liver disease or fibrosis (for example, if FIB-4 ≥ 1.3).
Ongoing follow-up and monitoring
Review women at 3 months after starting HRT to assess symptom control, side effects and blood pressure. Repeat lipid profile and glucose measurements at 12 months and annually thereafter. Reassess QRISK3 periodically. Encourage breast awareness and check that women are up to date with NHS breast-screening invitations. Discuss any abnormal bleeding or new symptoms promptly and investigate for endometrial pathology if bleeding persists beyond 6 months despite optimisation of the HRT regimen in line with BMS (2024a) guidance on unscheduled bleeding. Advise women to discontinue HRT and seek medical attention if they develop jaundice, severe hypertension or symptoms suggestive of thrombosis.
Clinical case scenario part 2 – management plan
Patient A in interested to explore lifestyle measures and weight-reduction goals (5–10% of body weight) She already eatsa Mediterranean-style diet and decides to join a gym to ensure she takes at least 150 minutes of moderate-intensity aerobic exercise per week.
Patient A agrees to start atorvastatin 20 mg daily for primary prevention (NICE, 2025) and agrees to ambulatory blood pressure monitoring.
She agrees to start transdermal oestradiol (50 µg/day patch) with oral micronised progesterone 100 mg nightly as continuous combined therapy.
At her 3-month follow-up, patient A reports marked improvement in VMS and sleep quality. With moderate weight loss and exercise, her blood pressure has improved to 134/82 mmHg, LDL-C has decreased to 2.6 mmol/L and there is no unscheduled bleeding or breast tenderness. Her BMI remains unchanged. She is keen to continue HRT and lipid-lowering therapy, along with lifestyle interventions and has a scheduled review in nine months.
Discussion
Why do current guidelines fall short?
The NICE menopause guideline (NG23) emphasises individualised care but explicitly advises clinicians not to offer HRT for the primary or secondary prevention of cardiovascular disease (NICE, 2024). The NICE guideline does not make separate recommendations for early versus late initiation of HRT, reflecting the fact that the timing data are largely observational or underpowered and have not been judged sufficient to change cardioprotective recommendations. The updated cardiovascular disease guideline (NG238) introduces QRISK3 and recommends statin therapy for individuals with a 10-year risk of 10% or higher (NICE, 2025), but does not mention menopause as a risk modifier.
The case for precision menopause treatment
Precision menopause management recognises that:
Menopause induces adverse metabolic changes
VMS are associated with higher cardiovascular risk
Observational and selected trial data suggest that women who initiate HRT within 10 years of menopause have lower rates of coronary events and mortality than later starters; however, NICE, NAMS and ACC emphasise that these findings do not support using HRT for primary or secondary cardiovascular prevention
Transdermal oestrogen with micronised progesterone minimises venous-thromboembolism and stroke risk (ACOG, 2013)
Dietary, lifestyle, weight management, statins and antihypertensive interventions remain essential when indicated (NICE, 2025)
Knowledge gaps and future directions
Although observational evidence supports the timing hypothesis, few randomised trials are designed to assess cardiovascular outcomes specifically in perimenopausal women. The ongoing Women’s Health Initiative and SWAN follow-ups may yield additional insights into the interplay between VMS, metabolic changes and incident cardiovascular events. Emerging therapies, including selective oestrogen receptor modulators, tissue-selective estrogen complexes and metabolic agents such as glucagon-like peptide-1 receptor agonists, may offer additional options for women with high cardiometabolic risk. Future guidelines should explicitly acknowledge menopause as a critical window for cardiovascular risk assessment and use menopause as a trigger to intensify conventional cardiovascular prevention (lifestyle, statins, blood pressure control), while ensuring that HRT is used for symptom relief with careful attention to cardiovascular safety rather than as a cardioprotective drug.
Key points
Menopause is a cardiometabolic turning point
VMS are associated with increased risk of coronary heart disease and stroke
A request for HRT is an excellent opportunity to address cardiovascular risk
Observational studies and subgroup analyses of randomised trials suggest lower mortality and coronary events when HRT is initiated in recently menopausal women, but NICE, NAMS and ACC all advise that HRT should not be used as a treatment to prevent cardiovascular disease
A precision menopause management strategy that combines symptom relief with rigorous cardiometabolic assessment, lifestyle modification, transdermal HRT with adequate progestogen, and evidence-based lipid and blood pressure management, offers a pragmatic framework for GPs