
Abstract
In an era of evidence-based practice, primary care teams are increasingly expected to engage with research. Critical appraisal of research literature and development and use of evidence-based guidelines are important in everyday practice. The design of high-quality, real-world studies and the provision of optimal patient-centred care demand an understanding of research methodologies. This article provides an overview of core research methodologies and their applications in primary care. It explores quantitative and qualitative approaches, highlights tools for rapid, rigorous evidence synthesis, and outlines ethical and practical considerations for their use, helping clinicians to interpret and undertake high-quality clinical and epidemiological research.
Foundations of research methodology
What is a research methodology?
A research methodology is the overarching rationale and strategy underpinning the design of a study, guiding what is investigated, why and how. It encompasses the theoretical framework, systematic plan, philosophy, ethical considerations and justification for the selected methods, and is distinct from the methods or specific techniques used for data collection and analysis (e.g. interviews, surveys or statistical tests). A robust methodology strengthens research credibility, transparency and impact by aligning the design with objectives and applying rigorous protocols to maximise validity and reliability while minimising bias. It ensures adherence to ethical guidelines and efficient use of time and resources (Jorge, 2024). The research onion (Saunders et al., 2019) provides a framework for health and epidemiology research, reminding researchers that their methods must align with philosophical assumptions, research aims and practical considerations. Positivist approaches focus on measurable data and testing hypotheses, as in quantitative research, whereas interpretivist approaches explore meanings and experiences, usually in qualitative studies. A pragmatic stance combines both, using the methods that best address the research question, often via mixed methods designs. Research can proceed deductively, testing existing theories with data, or inductively, generating novel insights from observations or patient narratives.
Formulating a research question
A well-defined research question is the foundation for all successful studies, providing clarity, focus and direction for the research process. Research frameworks such as PICO(T/S) (Population, Intervention, Comparison, Outcome, Time, Study Type) for quantitative research (Richardson et al., 1995) and SPIDER (Sample, Phenomenon of Interest, Design, Evaluation, Research type) for qualitative research (Cooke et al., 2012) help to structure research questions clearly, concisely and logically. In primary care, applying the FINER criteria (Elsevier, 2020) helps to ensure that research questions are feasible, interesting, novel, ethical and relevant, to produce robust, impactful and meaningful conclusions. Applying FINER helps ensure that research engages stakeholders, complies with ethical standards and stays relevant to real-world care, improving outcomes in diverse, often underrepresented populations.
Overview of common research designs
Understanding research methods is critical for designing studies that effectively answer clinical questions. Clinical research is classified as primary (pre-clinical, clinical or epidemiological studies collecting new data) or secondary (reviews, meta-analyses synthesising existing data), and may use quantitative (numerical), qualitative (non-numerical experiential, perspectives) or mixed methods depending on the research question, objectives and resources. Table 1 compares the characteristics, relative strengths and weaknesses of qualitative versus quantitative research. Pre-clinical research is non-human or lab-based, and clinical research involves humans. Clinical research focuses on improving the health and biology of individual patients, whereas epidemiological research examines health patterns and determinants in large populations to understand and prevent disease at a community or population level (Grimes and Schulz, 2002).
Key differences between quantitative and qualitative research table.
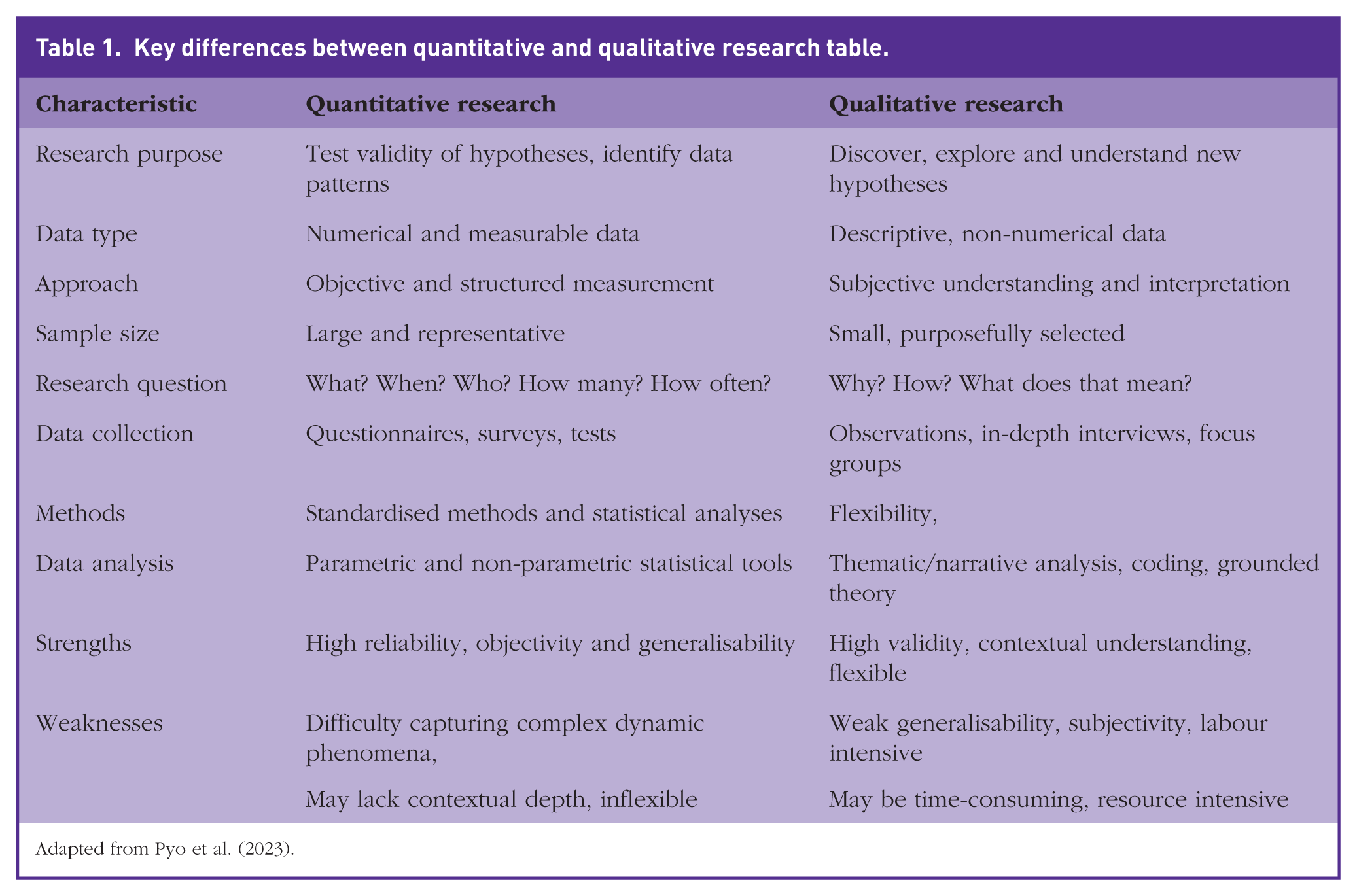
Adapted from Pyo et al. (2023).
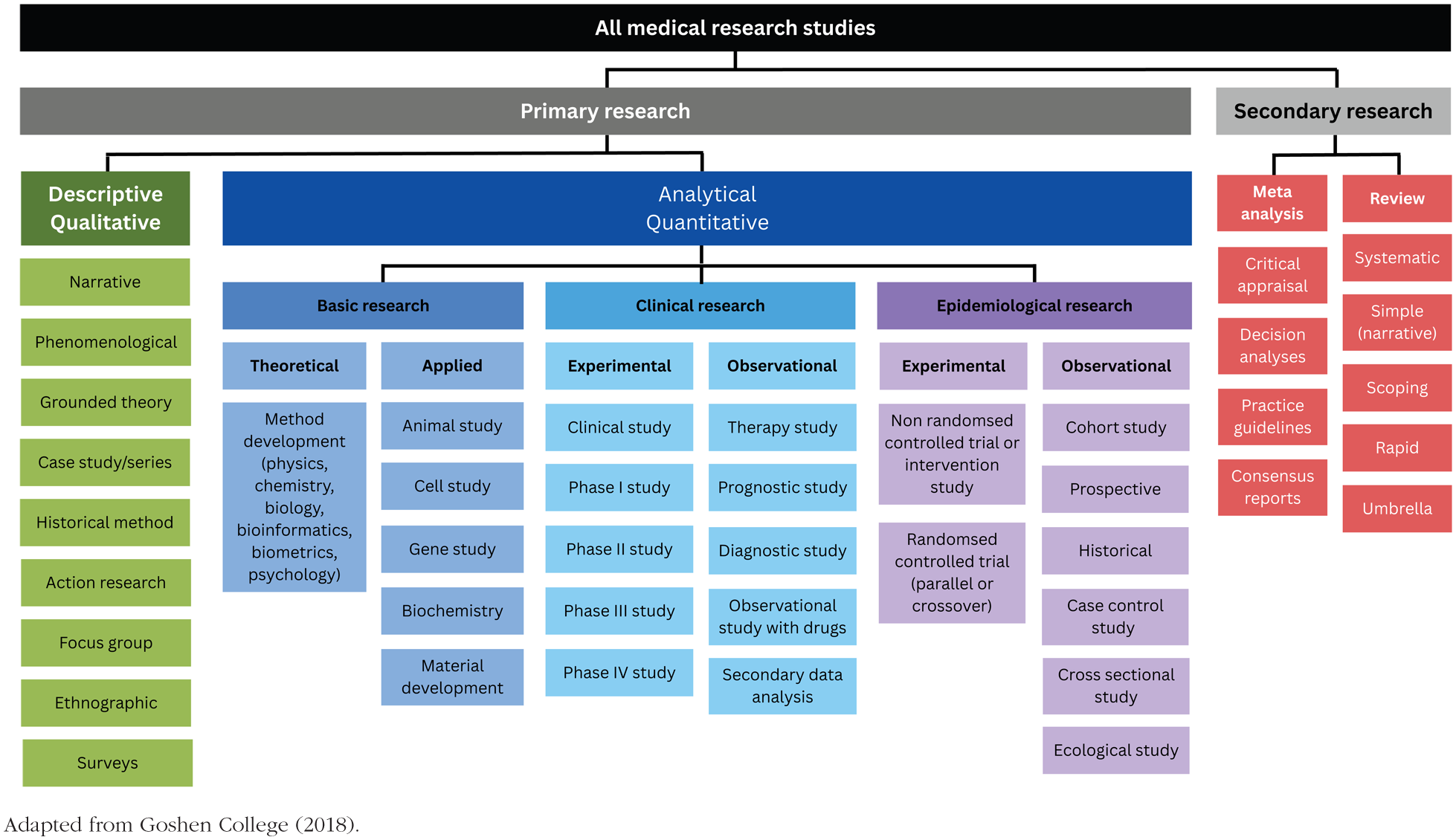
Primary research may be descriptive (describing characteristics of a population of interest) or analytical (quantifying relationships between factors or effects of an intervention, exposure or outcome against a control group). Analytical research may be observational or experimental according to whether the investigator passively or actively assigns exposures. Experimental research may involve animals (pre-clinical) or humans (clinical) and can be randomised or non-randomised according to whether the intervention is randomly assigned. Descriptive studies comprise case reports, case series, qualitative studies and surveys. Analytical studies include case–control, cohort and cross-sectional studies. The strength of evidence of a study is based on the susceptibility to bias of its chosen design (Figure 1). Systematic reviews and meta-analyses are situated higher in the evidence hierarchy, providing stronger evidence and less bias versus case reports and expert opinion at its base, with greater bias and lower strength of evidence (Cochrane, 2025). This classification complements Figure 2, which maps study designs by research categories (descriptive vs analytical; observational vs experimental). Decision trees for the choice of secondary evidence reviews according to the resources available and requirements of the review are useful (Cornell University Library, 2025).
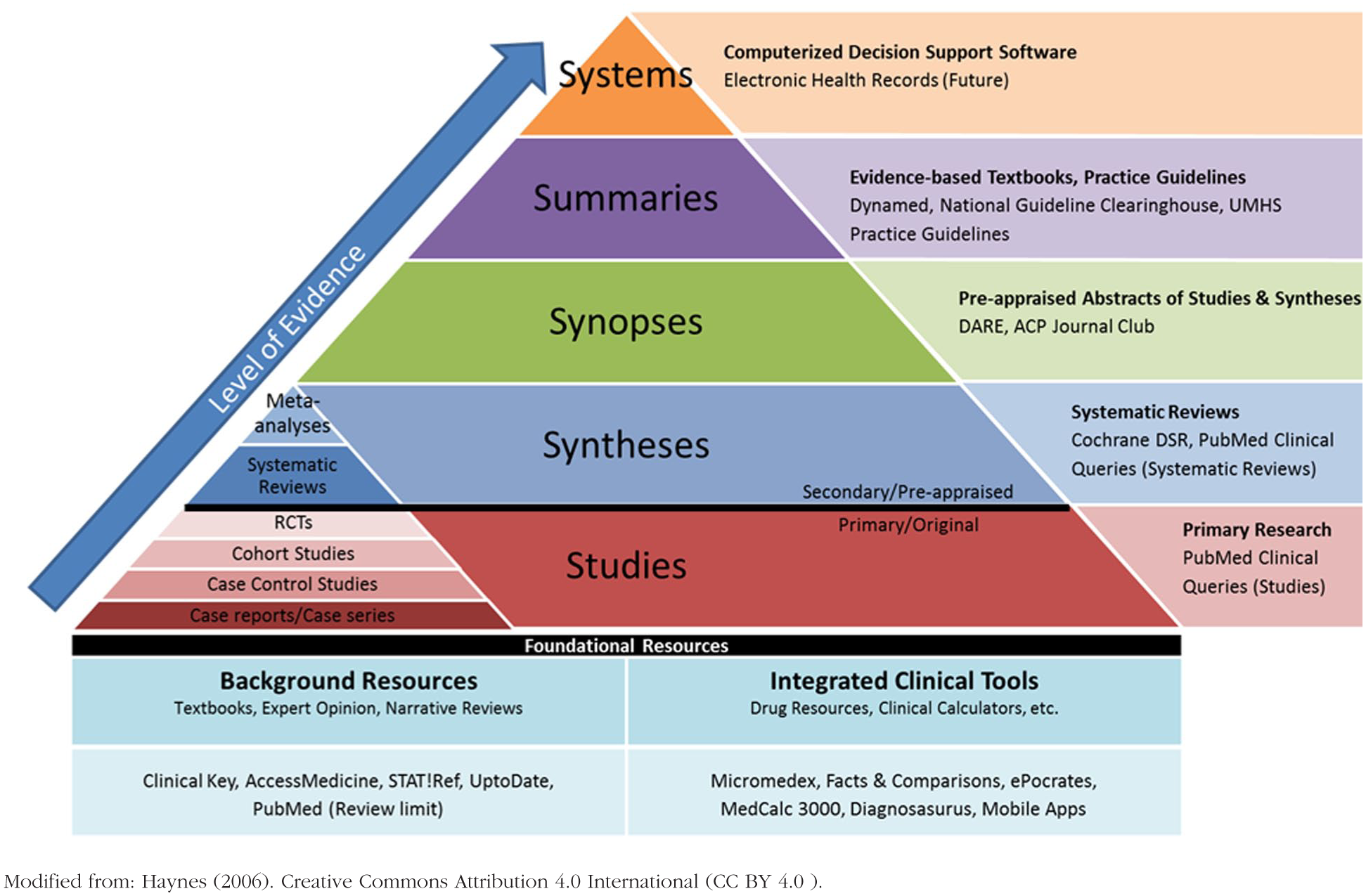
Hierarchy of research evidence.
Classification of research design.
Quantitative methods
Observational cross-sectional, case–control and cohort studies
Cross-sectional studies measure exposures and outcomes in a population at a single time point and are useful to measure the prevalence of disease or health-related outcomes, to generate hypotheses or plan future research. They are inexpensive, quick and simple to conduct using questionnaires or interviews, have fewer ethical difficulties and may be analytical or descriptive. Cross-sectional studies cannot readily assess incidence, study rare disease or causality and are often prone to sampling, non-response, Neyman (Hill, 2003) and recall bias (Wang and Cheng, 2020).
Case–control studies are retrospective, comparing exposure experiences of individuals with a condition or outcome (cases) to those without (controls). Odds ratios are derived to evaluate the association between the exposure and outcome. Case–control studies are inexpensive and quick to conduct, are feasible for rare disease, requiring fewer subjects than cross-sectional studies, but may be prone to confounding and recall or selection bias (Kiani et al., 2022).
Cohort studies are longitudinal, following groups over time to investigate the effects of exposures on outcomes. They are conducted where controlled trials are not feasible or may be unethical, where exposures or outcomes are rare, or to evaluate disease progression and prognosis. They allow calculation of incidence rate, cumulative incidence, relative risk and hazard ratios, and may be prospective or retrospective, offering evidence for causality and allowing evaluation of multiple outcomes associated with an exposure. Potential weaknesses are that prospective cohort studies are time-consuming and expensive, more susceptible to loss to follow up than cross-sectional studies and have greater confounding than randomised controlled trials (RCTs). Large sample sizes and long follow-up intervals are also required for rare diseases (Wang and Kattan, 2020). Retrospective cohort studies use existing data and offer less control over variables, but may be prone to information and recall bias.
Observational designs are used in primary care research to understand disease patterns or evaluate interventions. Confounding is a weakness of non-experimental research, as exposure allocation is not controlled by the researcher and effects may be obscured. Causal inference is complex, relying on use of the Bradford Hill criteria (Shimonovich et al., 2021), regression-discontinuity methods and time series methods.
Experimental randomised controlled trials
RCTs are the gold standard research design for establishing the effectiveness of interventions. They have high internal validity, reducing baseline confounding, selection and allocation bias by random allocation of participants to intervention or control arms and reducing performance bias through blinding. RCTs in primary care have challenges due to patient heterogeneity and recruitment difficulties. They are often costly, time-consuming and ethically challenging, with limited external validity, as controlled conditions are not always generalisable to real-world practice. Post-randomisation bias due to non-compliance and loss to follow up may occur (Fernainy et al., 2024) and intention-to-treat analyses are often required. Cross-over RCT designs where participants receive both therapies reduce confounding bias and aid precision of treatment outcomes and statistical power by comparing within-person responses, meaning that a smaller sample size is needed to achieve the precision of a parallel group trial (Capili and Anastasi, 2024).
Qualitative methods
Interviews, focus groups and thematic analysis
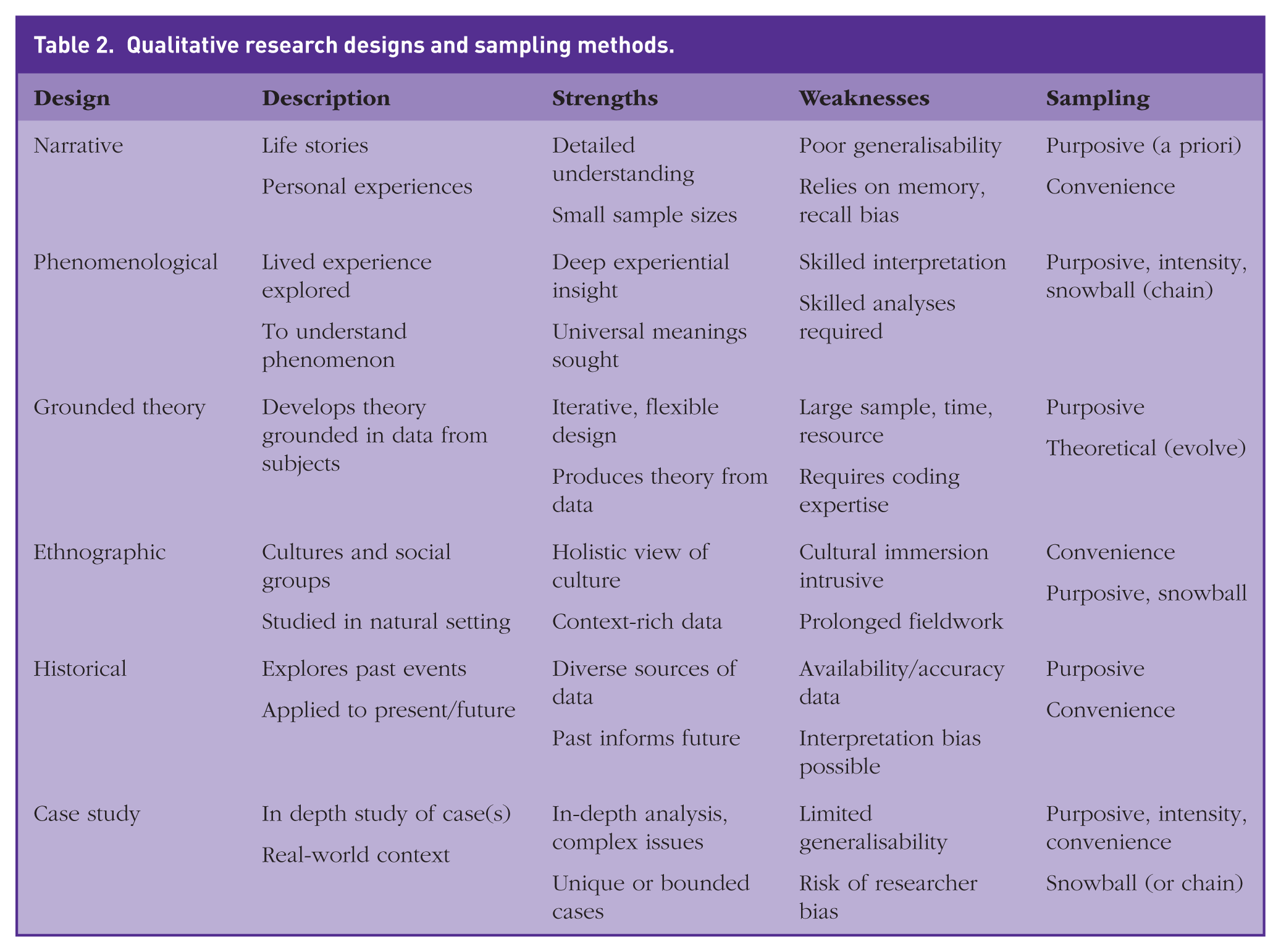
Qualitative research methods explore lived experience, dynamics, health beliefs and patterns of behaviour using open-ended exploratory methods, semi-structured interviews, focus groups or participant observations. Narrative, phenomenological, grounded theory, ethnographic, historical and case study designs are used with purposive, convenience, snowball or intensity sampling (Draper, 2004). Features of these designs and sampling methods are given in Table 2. Sample sizes are small and targeted with non-statistical, descriptive or interpretative data analyses being used. Descriptive results and hypotheses are drawn and tested within quantitative research (Renjith et al., 2021). Techniques to ensure qualitative rigour include reflexivity, triangulation, member checking and data saturation. The Critical Appraisal Skills Programme (CASP, 2024) appraises the quality of studies and transparent reporting is facilitated by the Consolidated Criteria for Reporting Qualitative Research (COREQ) (Tong et al., 2007).
Qualitative research designs and sampling methods.
Mixed methods approaches
Mixed methods research integrates qualitative and quantitative data to give a comprehensive understanding of complex issues. It is often used in health services research for the evaluation of interventions, adding analytical breadth and depth. Qualitative and quantitative combined data help to validate findings through triangulation, enable richer and more nuanced analysis, and can uncover real-world impacts of a policy or intervention. Explanatory sequential, exploratory sequential or convergent mixed methods approaches exist. Disadvantages of mixed methods research include high resource demands, complex data integration, bias and a need for expert involvement to integrate findings coherently.
Applying methodologies in primary care research
Selecting the right method
Choice of research methodology must align with the research question, context, objectives and available resources. A quantitative approach is preferred if statistical evidence is required, whereas a qualitative approach is more suited to providing qualitative insights. Questions about effectiveness of interventions require an RCT, while exploration of patient experiences or beliefs suits a qualitative design. Cluster-randomised trials are often used in primary care research, randomising whole practices to an intervention or control rather than individuals. Diagnostic accuracy studies evaluate system-level changes such as screening initiatives. The feasibility and relevance to clinical practice are important considerations. Practical constraints, time, participant access and analytical skills must be considered, and methods aligned with ethics and objectives. Quantitative studies often demand extensive planning and data entry time, while qualitative research often involves lengthy interviews and transcription (Matheson et al., 2025).
Conducting reviews
Literature reviews are useful to familiarise the researcher with existing literature, identify gaps in knowledge, evaluate the quality of existing research, synthesise findings and justify the need for novel research. Narrative reviews are the simplest review offering a broad overview of existing knowledge (Koch and Iliffe, 2011; Leese et al., 2023). Rapid reviews are streamlined versions of systematic reviews, used when timely evidence is needed (Garritty et al., 2024). Shortcuts may include limiting databases, using single-reviewer screening with verification, or focusing only on key outcomes. They are useful in fast-moving fields such as guideline updates or emerging health threats. Scoping reviews map literature on a broad topic or multiple research questions, to identify key concepts and gaps (Eccles et al., 2024), and umbrella reviews synthesise evidence from multiple existing systematic reviews (Painter et al., 2025), providing a high-level overview of a saturated research landscape, often to compare interventions. A meta-analysis pools data from individual studies to provide a statistically powerful, precise summary.
Using supportive tools and software
Software (e.g. Covidence, Rayaan, Grade-PRO, EPPI-Reviewer) may be utilised to enhance the efficiency of study screening and data extraction when undertaking reviews. The cost, validity, usability, transparency and necessity for oversight should be considered when deciding on their use.
Quality improvement and audit projects
Although not included in formal research designs, quality improvement (QI) and audit projects are frequently used in general practice to improve healthcare delivery, outcomes and efficiency. They facilitate continuous improvement, target real issues in practice and have local relevance. They also support General Medical Council (GMC) regulatory and training requirements, promoting team learning and evidence-based practice. The full clinical audit cycle is defined by the RCGP (2025) and the Model for Improvement by the RCGP (2025), National Health Service England (NHSE, 2023), Health Foundation and Institute for Healthcare Improvement (IHI, 2025).
Ethical and practical considerations in research methodologies
A responsible research environment prioritising ethics safeguards participants and contributes to overall research validity and reliability, advancing knowledge responsibly.
Informed consent and ethical approval
Research involving human participants requires ethical approval. NHS Research Ethics Committees (RECs) guide this process and compliance with Institutional Review Boards (IRB) is mandatory to ensure scientific integrity and to protect study participants. Informed consent is essential to foster trust and transparency, and to ensure all participants fully understand the purpose, nature, risks and benefits involved. Researchers must comply with the General Data Protection Regulation (GDPR) guidelines ensuring consent is voluntary and informed with full information disclosure and decision-making capacity (UK Research and Innovation [UKRI], 2020). Participants may withdraw from the research at any time with no impact on their care. A signed consent form confirms this. Patient and Public Involvement (PPI) throughout the study is ideal, from design to dissemination of results, to align the research with real-world needs, and to improve the relevance, participation and overall impact of the research. NIHR Guidelines offer practical steps for embedding PPI at every stage of healthcare research (NIHR, 2021; Staniszewska et al., 2017).
Confidentiality
Maintaining the confidentiality of participant data is essential under GDPR guidelines, and researchers must ensure that the personal and health information of participants is never disclosed. Anonymisation, pseudonymisation, data minimisation, secure storage, role-based access controls and explicit participant consent are used. Confidentiality enhances participant trust, safety and research integrity and a breach has severe consequences including regulatory action.
Minimising harm
Researchers must minimise any potential harm to participants, whether physical, emotional or psychological. They must assess the risks associated with the research design and implement measures to mitigate them. Conducting thorough risk–benefit analyses ensures that potential benefits of the research outweigh possible harms.
Vulnerable populations
Special ethical considerations apply to any research involving vulnerable populations, including children, prisoners, refugees, homeless individuals, pregnant women, elderly individuals, those who are disadvantaged economically or educationally, and those with disabilities or cognitive impairments. Vulnerable individuals are at greater risk of exploitation or coercion and require additional protections and safeguards to protect their rights and welfare. Researchers must be cautious and ensure that these individuals fully understand the research and are choosing to participate voluntarily. Inclusion of vulnerable groups in research is advantageous, enhancing generalisability and addressing health disparities for conditions of vulnerable communities.
Debriefing participants
Researchers should offer debriefing to inform study participants about the study’s purpose and findings, to aid understanding of their contribution and the overall significance of the research. Debriefing also provides an opportunity to address participants’ questions or concerns about their involvement.
Research misconduct
Researchers must uphold ethical standards in data collection, avoiding any form of misconduct, fabrication, falsification or plagiarism, to uphold trust in the research community and society.
Managing bias and confounding
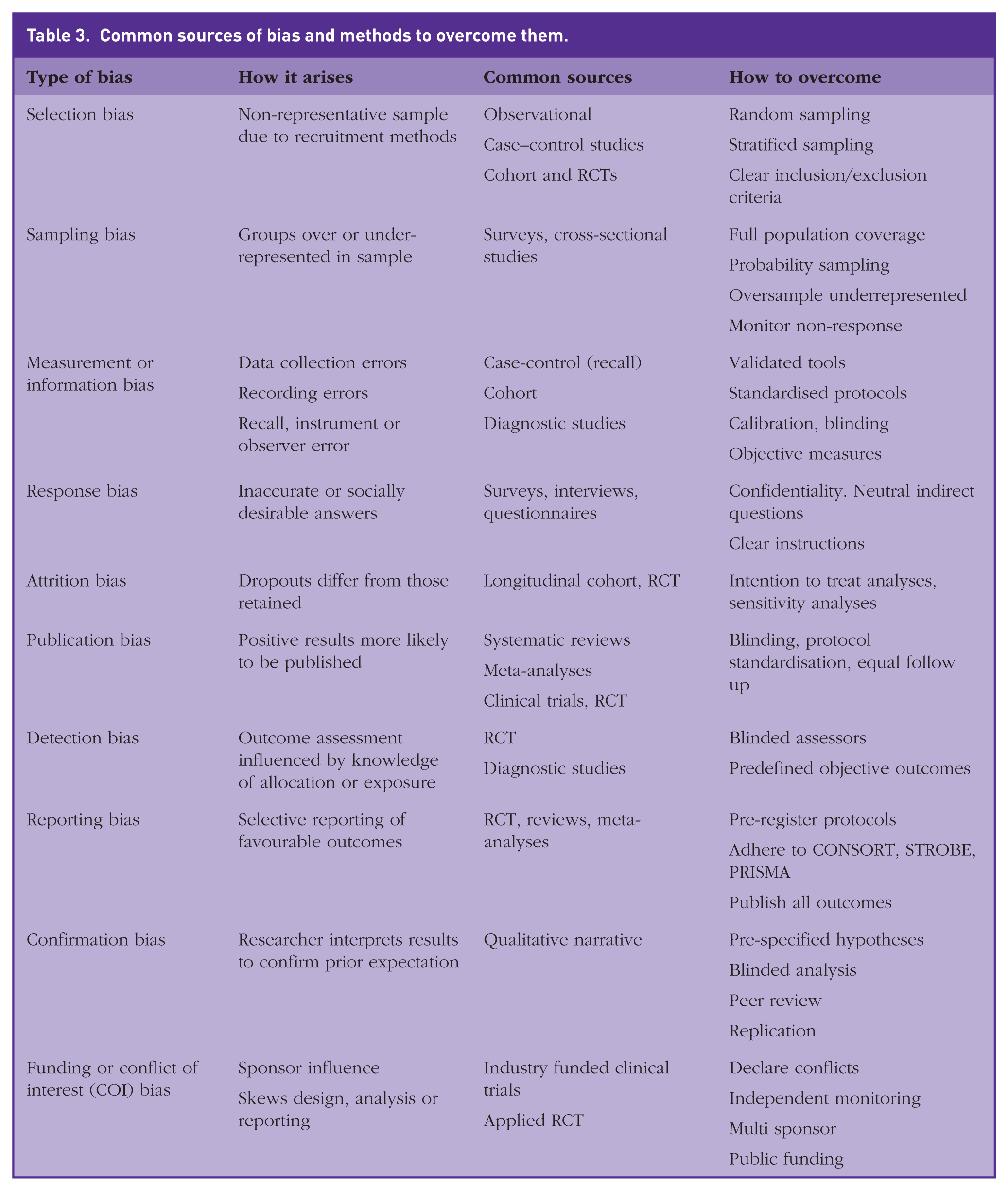
Bias can distort findings and affect generalisability. Common types include selection, sampling, measurement (information), response, attrition and publication bias. Confounding variables obscure true associations. Table 3 explores research strategies to reduce bias include randomisation, blinding, stratified sampling and statistical adjustment.
Common sources of bias and methods to overcome them.
Emerging trends in research design
Data-driven research design
Machine learning and data analytics platforms are increasingly leveraged to enable researchers to uncover patterns and correlations in complex datasets, enhancing precision in quantitative and mixed methods studies, and predicting outcomes through advanced statistical modelling. Such technological innovations accelerate the speed, efficiency and depth of research insights. Digital platforms allow for real-time capture of authentic participant data anywhere via mobile ethnography, online diaries or video interviews, removing geographical barriers to research. Furthermore, computational and multimodal approaches integrating text, images, video and audio provide a richer, more comprehensive understanding of research phenomena.
Artificial intelligence
Artificial intelligence (AI) offers researchers the opportunity to automate literature reviews with tools such as Elicit and Research Rabbit, enhancing survey designs through AI-driven questions, and facilitating data analysis with platforms such as SPSS, IBM and R Studio. AI advantages include accelerated data analysis, real-time insights from electronic health records, and the ability to identify population health trends or treatment outcomes more efficiently, enhancing evidence-based decisions and rapid literature synthesis. Possible disadvantages include bias in training data or algorithmic decisions, and an over-reliance on AI above clinical judgement.
Sustainability and ethical considerations
As global challenges such as climate change and health inequity dominate political agendas, there is a shift to designs that emphasise environmental sustainability, and inclusive methodology that prioritise under-represented populations and voices, with enhanced ethical protocols to address the complexities of digital and cross-cultural research .
Interdisciplinary collaborative and remote approaches
Modern research problems often span multiple disciplines, necessitating collaborative designs merging expertise from many disciplines, with shared frameworks for diverse methodologies. Platforms such as Slack, Trello and Miro facilitate cross-disciplinary communication. The rise of remote technologies has reshaped traditional research practices, enabling longitudinal studies leveraging wearable tech and internet of things (IoT) devices for continuous data, virtual ethnography for social science studies, conducted through digital platforms, and remote experiments using tools such as Prolific or Amazon Mechanical Turk.
Adaptive, agile research frameworks
In response to rapidly changing conditions such as public health crises, research designs now prioritise real-time data collection and analysis for timely insights, flexible methodologies that adapt to evolving hypotheses or external disruptions, and hybrid designs combining qualitative and quantitative approaches to ensure robustness. (Olawade et al., 2023)
Conclusions
Robust research methodologies are critical to addressing complex, real-world challenges in primary care. Methodologies must continue to evolve, combining the rigour of traditional design frameworks with the innovative opportunities of digital and interdisciplinary approaches. Mixed methods integrating qualitative, quantitative, participatory and systems approaches flexibly in research design are vital to deepen public health insights, and to ensure that inclusion, context and complexity are fully understood. Flexible co-design of interventions, knowledge production within affected populations and consideration of cultural contexts are important. This evolution will advance knowledge and equip clinicians with the robust evidence needed to improve patient outcomes, guide decision-making, and deliver effective, ethical, patient-centred care.
Key points
Research methodologies underpin the validity and impact of clinical research
Clear, relevant research questions and appropriate study designs are essential
Quantitative and qualitative methods serve different but complementary purposes
Systematic reviews and meta-analyses provide helpful literature summaries
Online learning platforms, protocol frameworks and software tools aid researchers
Understanding bias and confounding is essential to ensure reliable outcomes