
Abstract
Background:
Crohn’s disease (CD) involves chronic intestinal inflammation, frequently requiring surgical intervention. CD patients undergoing surgery often undergo increased psychological stress. One of the outcomes of persistent stress is post-traumatic stress (PTS), a mental health concern associated with immune dysregulation and disease progression. However, research on PTS in CD patients following surgery is limited.
Objectives:
This study aims to explore the incidence and associated factors of PTS in CD patients after surgery.
Design:
A retrospective cross-sectional study.
Methods:
This retrospective cross-sectional study investigated 124 patients with CD who underwent surgery between September 2015 and July 2023. Online questionnaires, including the PTSD checklist, 5th edition (PCL-5), Crohn’s and Colitis Knowledge Score, and Short Generic Patient Experience Questionnaire, were employed. The potential risk factors for PTS were evaluated through univariate and multivariate analyses.
Results:
Among sampled individuals, 44 patients (35.5%) were classified into the PTS group. The patients in the PTS group had a significant lower monthly income (27.3% vs 8.8%, p = 0.006), higher Harvey–Bradshaw Index score (3.82 ± 3.25 vs 2.31 ± 2.50, p = 0.009), more occurrence of perianal lesions (36.4% vs 20%, p = 0.047), higher ostomy (36.4% vs 20%, p = 0.047), and laparotomy rates (31.8% vs 15%, p = 0.028). Through logistic regression analysis, we identified postoperative complications and a history of multiple surgeries as independent risk factors for PTS (p = 0.002 and p = 0.019, respectively).
Conclusion:
PTS is common in CD patients requiring bowel resection and multiple surgeries, as well as other postoperative related factors, can invoke psychological and mental stress. These findings provide insights for formulating medical service strategies that prioritize patient mental health.
Introduction
Crohn’s disease (CD) is a chronic gastrointestinal disorder characterized by intestinal inflammation and abnormalities in the immune system.1,2 Up to 75% of CD patients require surgery at least once to manage complex disease conditions or related complications throughout their lifetime.3–5 Repeated studies have found that CD patients undergoing surgery experienced more mental stress, such as anxiety, depression, fear, and poor quality of life, compared to healthy controls.6–8
Post-traumatic stress disorder, referred to as PTSD, is a common mental health concern. In clinical research, the concept of post-traumatic stress (PTS) is often referenced more, as the diagnosis of PTSD requires a professional clinical interview conducted by qualified mental health professionals, which may be less feasible in clinical research.9–11 Early identification and treatment of PTS can help prevent its progression into full-blown PTSD.12,13 PTS assessment tool is currently not only used to diagnose PTSD in traditional acute traumatic events, but also increasingly being applied to assess patients with chronic diseases like inflammatory bowel disease (IBD) who could suffer from severe mental illnesses.14,15 Nineteen percent of a Swiss cohort 16 of 468 CD patients scored above the diagnostic cutoff for PTSD, whereas only 10% reported no evidence of PTSD symptoms. In addition, numerous studies suggested that alterations in immune regulation linked to PTS can instigate disease activity and progression in IBD, thereby adversely impacting various aspects of outcomes for individuals with IBD.17–19 A large-scale study of 797 patients with IBD reported that approximately 25% experienced significant symptoms of PTS. 19 This finding highlights the potential psychological burden faced by individuals living with chronic conditions such as CD. Other studies have further suggested that long-term disease management and the potentially distressing experiences associated with medical treatment may contribute to the development of PTS symptoms in this population.20–23 Medical trauma, especially surgical interventions, is a high-risk factor for PTS in patients.24,25 Therefore, focusing on the postsurgical mental health of IBD patients is crucial.
In recent years, a great deal of attention has been given to the psychological burden of CD patients.16,26–28 However, PTS in CD patients has not attracted widespread attention, and relevant research studies are scarce, particularly for patients experiencing CD-related surgery.12,19 Hence, the purpose of this study is to investigate the incidence of PTS in CD patients after surgery and explore the associated risk factors. Additionally, understanding the relationship between surgery, postsurgical conditions, and PTS symptoms is critical for improving the quality of life and clinical outcomes of CD patients.
Materials and methods
This study is a cross-sectional retrospective investigation involving CD patients who underwent abdominal surgery from September 2015 to July 2023. A total of 235 CD patients were surveyed through online questionnaires. The inclusion criteria for the study were as follows: (1) patients diagnosed with CD, (2) individuals who underwent surgical treatment at the Department of General Surgery, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine. The exclusion criteria were: (1) Patients with a clearly documented history of major traumatic events unrelated to CD (e.g., severe accidents, assault, or bereavement) were excluded, in order to reduce confounding from known non-CD-related sources of PTSD. However, we acknowledge that routine life stressors may still contribute to PTSD symptoms and cannot be entirely ruled out; (2) Patients unable to complete the questionnaire or having difficulty participating in follow-up visits regularly; (3) Patients who underwent surgery at another hospital with incomplete information. Patients who fully understood the questionnaire content and the significance of follow-up procedures, who agreed to participate, and who met the inclusion criteria completed the following questionnaire. The reporting of this study conforms to the Checklist for Reporting Results of Internet E-Surveys (CHERRIES) statement. 29 All questionnaires and tools used in this study were obtained with the necessary permissions from the respective copyright holders.
Demographic and clinical information
To conduct a study on postoperative CD patients, basic demographic information and clinical details were collected. All patients enrolled were identified as Han Chinese and were recruited from Ruijin Hospital in Eastern China, with the majority residing in urban areas. The cohort consisted of 65.3% men and 34.7% women, with an average age of 37.24 ± 11.49 years. In terms of socioeconomic status, 53.2% of patients had attained a bachelor’s degree or higher, 83.1% were covered by urban employee basic medical insurance, and 37.1% were unemployed. Regarding income distribution, 18.5% of patients had a monthly family income below 5000 CNY, while 50.8% had a monthly income exceeding 10,000 CNY. Clinical data included age of onset, postoperative hospitalization duration, preoperative relevant blood indices, previous surgeries (including perianal procedures), disease behavior, perianal involvement, surgical approach (open or laparoscopic), ostomy status, postoperative complications, and time elapsed since surgery.
The PTSD Checklist 5
PCL-5 (Posttraumatic Stress Disorder Checklist-5) 30 is a common tool for assessing symptoms of PTSD. It is part of the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) and primarily aims to evaluate whether individuals have experienced symptoms of PTSD related to a traumatic event and the severity of these symptoms. The PCL-5 comprises 20 items, and responses are scored on a 5-point Likert scale, ranging from 0 to 4, with increasing severity. A score of 0 represents “not at all,” while 4 represents “extremely.” The total symptom severity score (ranging from 0 to 80) is obtained by summing the scores for each item. It covers the four symptom clusters defined in DSM-5 for PTSD: Cluster B: Re-experiencing (items 1–5), Cluster C: Avoidance (items 6–7), Cluster D: Negative alterations in cognitions and mood (items 8–14), Cluster E: Alterations in arousal and reactivity (items 15–20). Typically, the presence of each symptom rated as 2 or higher (“moderate” or above) is considered as an endorsed symptom. According to DSM-5 criteria, a preliminary diagnosis of PTSD requires the following: At least one symptom from Cluster B (re-experiencing), at least one symptom from Cluster C (avoidance), at least two symptoms from Cluster D (negative alterations in cognitions and mood), and at least two symptoms from Cluster E (alterations in arousal and reactivity). These criteria are used to assess whether an individual meets the diagnostic criteria for PTSD based on their responses to the PCL-5 questionnaire.
Crohn’s and Colitis Knowledge Score
The Crohn’s and Colitis Knowledge Score (CCKNOW) 31 is an assessment tool used to measure patients’ understanding of IBDs, including CD and ulcerative colitis. This score is widely used in research and clinical practice to evaluate patients’ knowledge levels of IBDs. The assessment includes a series of questions about these diseases, covering aspects such as symptoms, diagnosis, treatment, and lifestyle management. The questionnaire contains a total of 24 questions, with each correct answer scoring 1 point and each incorrect answer scoring 0 points. A higher total score indicates a greater understanding of IBD.
Short Generic Patient Experience Questionnaire
The Short Generic Patient Experience Questionnaire (PEQ) 32 is a survey designed to measure patients’ opinions and feelings about the quality of healthcare and services. It consists of only four questions: whether healthcare staff are friendly, whether they listen to your explanations and provide clear instructions, whether you are seen promptly, and whether the hospital operates smoothly. Each question offers four response options: “excellent,” “good,” “fair,” and “poor,” with each option corresponding to a score ranging from 3 to 0. The total score of these four questions can reflect the overall patient experience, with a higher score indicating a better experience.
Disease activity assessment
CD activity was assessed using the Harvey–Bradshaw Index (HBI), a widely used clinical tool for evaluating disease severity. The HBI includes five parameters: general well-being (scored 0–4), abdominal pain (scored 0–3), number of liquid stools per day, presence of an abdominal mass (scored 0–3), and complications (such as arthralgia, uveitis, erythema nodosum, aphthous ulcers, anal fissures, new fistulas, and abscesses; 1 point for each). The total score is the sum of these components, with higher scores indicating more active disease. In our study, HBI was used to evaluate the level of disease activity at the time of psychological assessment.
Sample size calculation
The sample size was estimated based on an expected prevalence of PTS in CD patients after surgery of approximately 30%, according to prior studies in chronic illness populations. Using a single proportion sample size formula with a 95% confidence level, a precision (margin of error) of 8%, and an assumed prevalence (p) of 0.30, the minimum required sample size was calculated as follows:

where Z = 1.96 for a 95% confidence interval; p = 0.30; d = 0.08.
The calculation yielded a minimum required sample size of 101 patients. To account for potential incomplete responses and missing data, we increased the sample size by approximately 20%, resulting in a final target sample size of 121 patients. Ultimately, 124 eligible patients completed the questionnaires and were included in the final analysis.
Statistical analyses
After importing data from an electronic questionnaire into an Excel file and quantifying the answers, we calculated the total score of PCL-5 as well as the total scores for the B, C, D, and E symptom clusters. The Crohn’s and Colitis Knowledge Score and the Short Generic Patient Experience Questionnaire total score were also calculated. Patients who met the criteria for PTSD symptoms as defined in DSM-5 and those with at least one symptom from the PTSD symptom clusters (B, C, D, and E) lasting for at least 1 month were categorized as having PTS symptoms, while the rest were considered symptom-free. Data extraction and analysis were performed using IBM SPSS Statistics (Version 26.0; IBM, Armonk, NY, USA) and GraphPad Prism (Version 9.0; GraphPad Software, Boston, MA, USA). Mann–Whitney U tests were employed to compare patient demographic information, clinical data, and surgical details between the two groups. Univariate and multivariate logistic regression analyses were performed to identify the independent predictors of PTS in CD patients following surgery.
Results
Patient characteristics
In this study, questionnaires were distributed to 235 individuals, and 130 completed questionnaires were collected. After organizing and analyzing the questionnaires, it was discovered that three of those lacked personal information, two were hastily completed, and one was incomplete. A total of 124 patients with CD-related bowel surgery were enrolled eventually (Figure 1). A comprehensive summary of the baseline characteristics of the patients is presented in Table 1. Of these patients, the average age is 37.24 ± 11.49 years, with men constituting 65.3% of the cohort, and 62.9% being married. The majority of patients (83.1%) are covered by urban employee basic medical insurance, whereas 37.1% are unemployed. There is considerable variability in the educational backgrounds of the patients, with 53.2% having attained a bachelor’s degree or higher. According to DSM-V criteria, 35.5% of them exhibited at least one PTS symptom (30 men and 14 women). 33 And no statistically significant differences were observed in the aforementioned characteristics. However, roughly 27.3% of patients in the PTS group have a monthly family income below 5000 CNY, compared to 8.8% in the non-PTS group. About 38.6% and 57.5% of patients have a monthly income exceeding 10,000 CNY in the PTS group and the non-PTS group, respectively (p < 0.032).
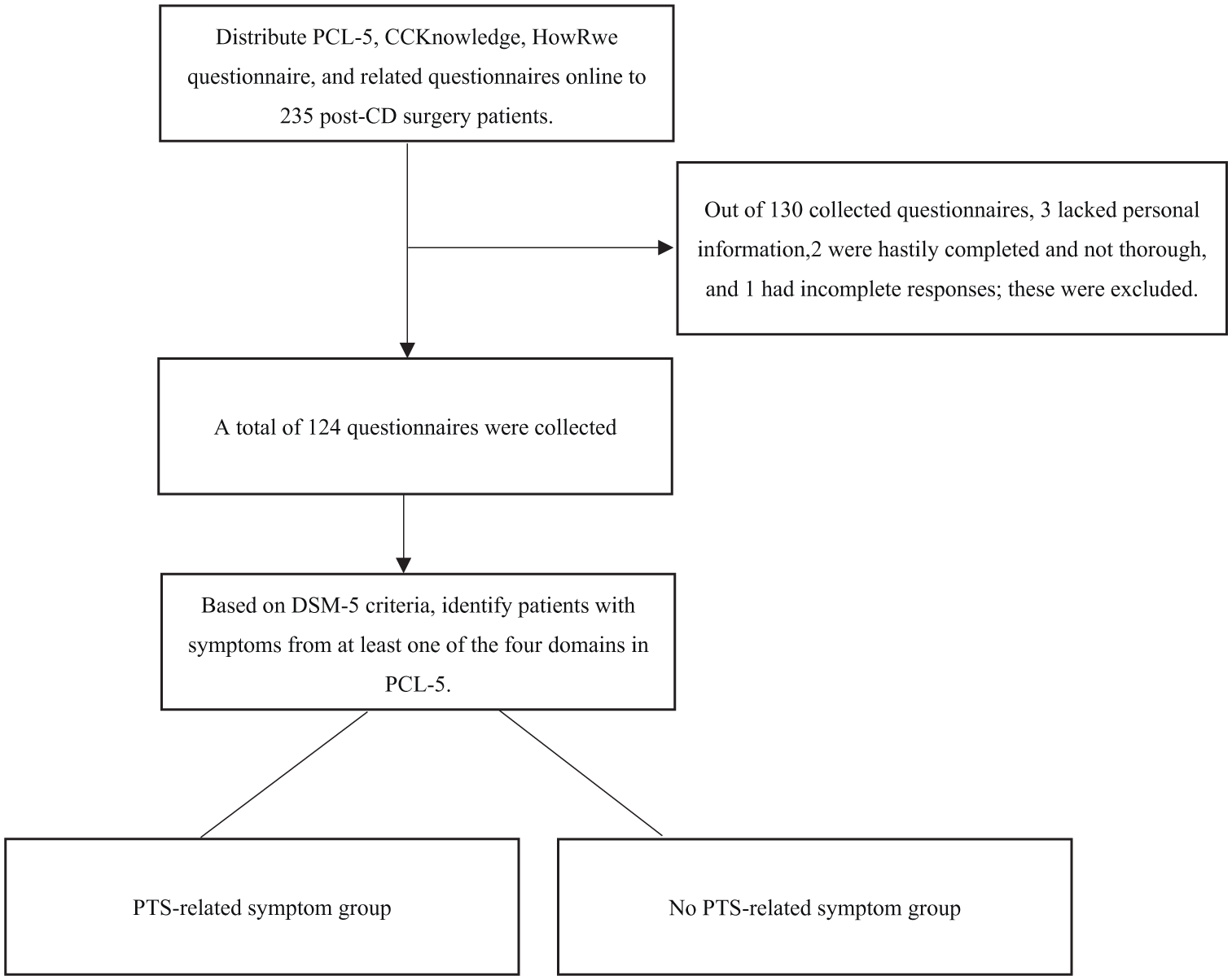
Experimental design flowchart.
Basic characteristics of the patients enrolled in this study.
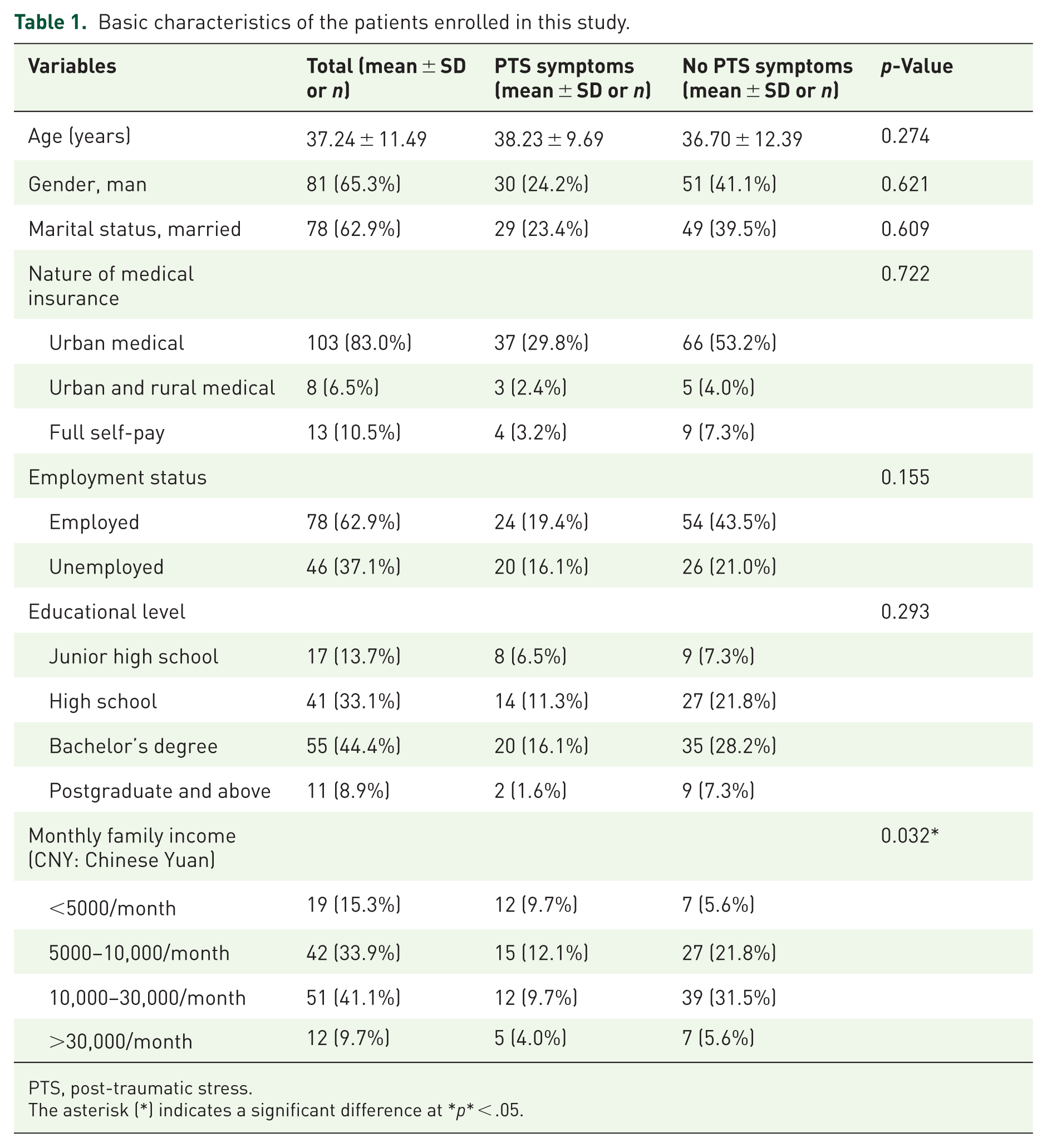
PTS, post-traumatic stress.
The asterisk (*) indicates a significant difference at *p* < .05.
Upon further observation of clinical characteristics (as shown in Table 2), it was noted that patients in the PTS group had a higher frequency of hospitalizations for CD compared to the non-PTS group (3.66 ± 2.20 vs 3.45 ± 1.95), although it did not reach statistical significance. No significant differences were found between the PTS and non-PTS groups in terms of age at diagnosis, disease location, and disease behavior. Based on the HBI scores, patients with PTS symptoms were more likely to have active disease compared to those without (3.82 ± 3.25 vs 2.31 ± 2.50, p = 0.009). In the PTS group, perianal lesions were present in 36.4% patients in the PTS group, significantly higher than the 20% observed in the non-PTS group (p = 0.047).
Clinical features of postoperative patients with Crohn’s disease.
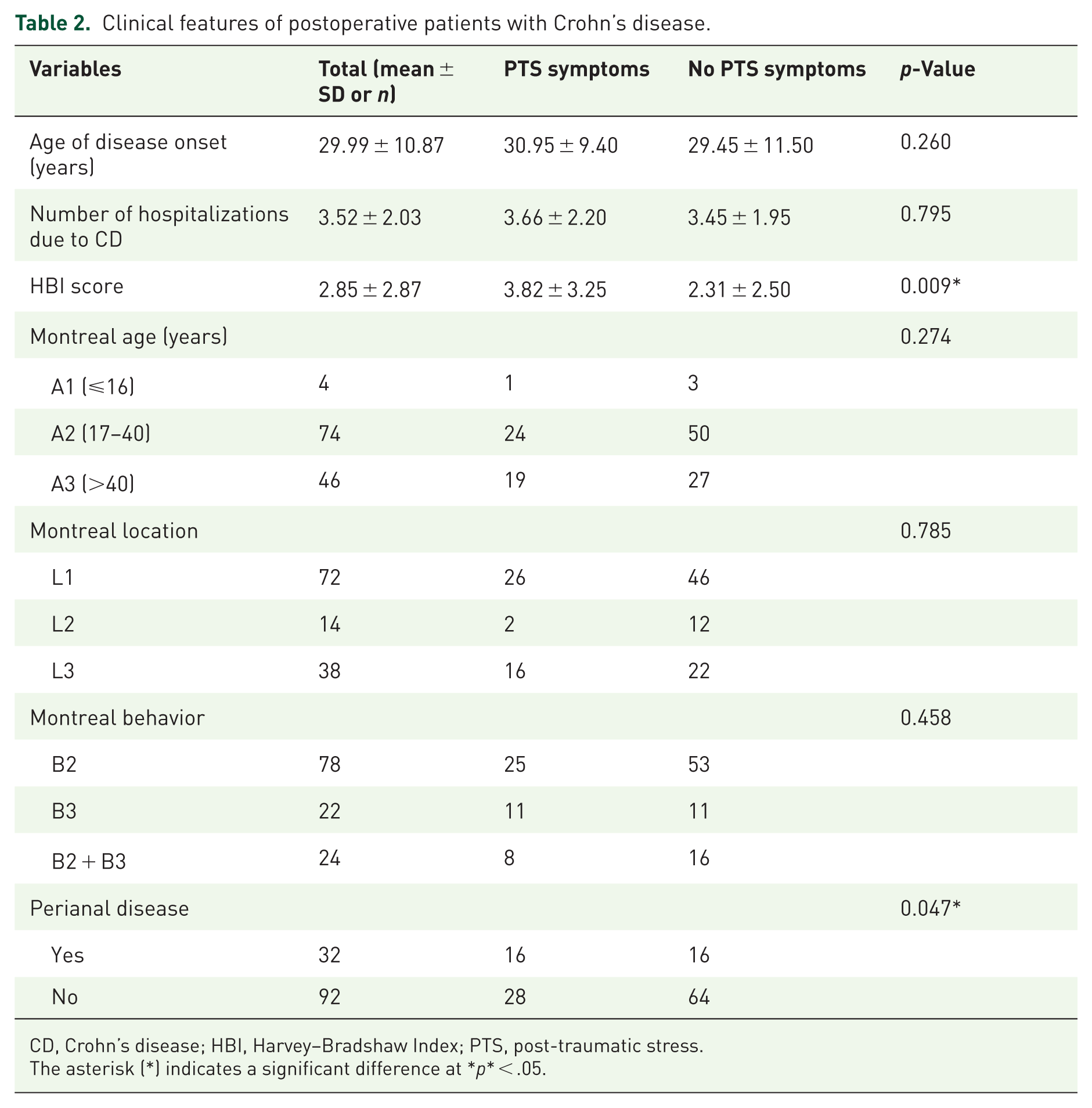
CD, Crohn’s disease; HBI, Harvey–Bradshaw Index; PTS, post-traumatic stress.
The asterisk (*) indicates a significant difference at *p* < .05.
The relationship between CCKNOW and PTS
Improving understanding of disease is thought to help patients adapt more flexibly to their condition, encouraging active participation in treatment decisions and management. However, certain studies reveal that knowledge improvement may not necessarily mitigate patients’ anxiety levels and could potentially be positively correlated with anxiety.34,35 This phenomenon may be attributed to the fact that, with the increase in knowledge, patients develop a deeper understanding of the disease, accompanied by a clearer awareness of potential risks, thereby triggering anxiety. However, upon evaluating patients’ understanding of CD, we observed no significant difference in Crohn’s and Colitis Knowledge Score (CCKNOW) between the PTS and non-PTS groups (10.39 ± 4.51 vs 10.25 ± 4.38, p > 0.05; Supplemental Figure 1). This result may reflect a complex relationship between knowledge disparity and patients’ anxiety levels, and further in-depth research will be needed to elucidate the mechanisms behind this phenomenon.
Short generic patient experience questionnaire and PTS
The inpatient experience has been shown to impact psychological well-being, indirectly affecting the occurrence of PTS. 26 PEQ1 assesses patients’ evaluations of physician attitudes, PEQ2 measures physician patience and the quality of relevant explanations provided to patients, PEQ3 focuses on humane care provided by nurses, and PEQ4 gauges patient satisfaction with nursing care. Upon comparing PEQ scores between the PTS group and the non-PTS group, no statistically significant differences were observed between PEQ1 and PEQ4. However, significant differences were noted in PEQ2 and PEQ3 (p = 0.025, p = 0.039, respectively). The overall patient experience scores of the PTS group were significantly lower than those of the non-PTS group (10.66 ± 1.85 vs 11.34 ± 1.25, p = 0.029; as shown in Figure 2).
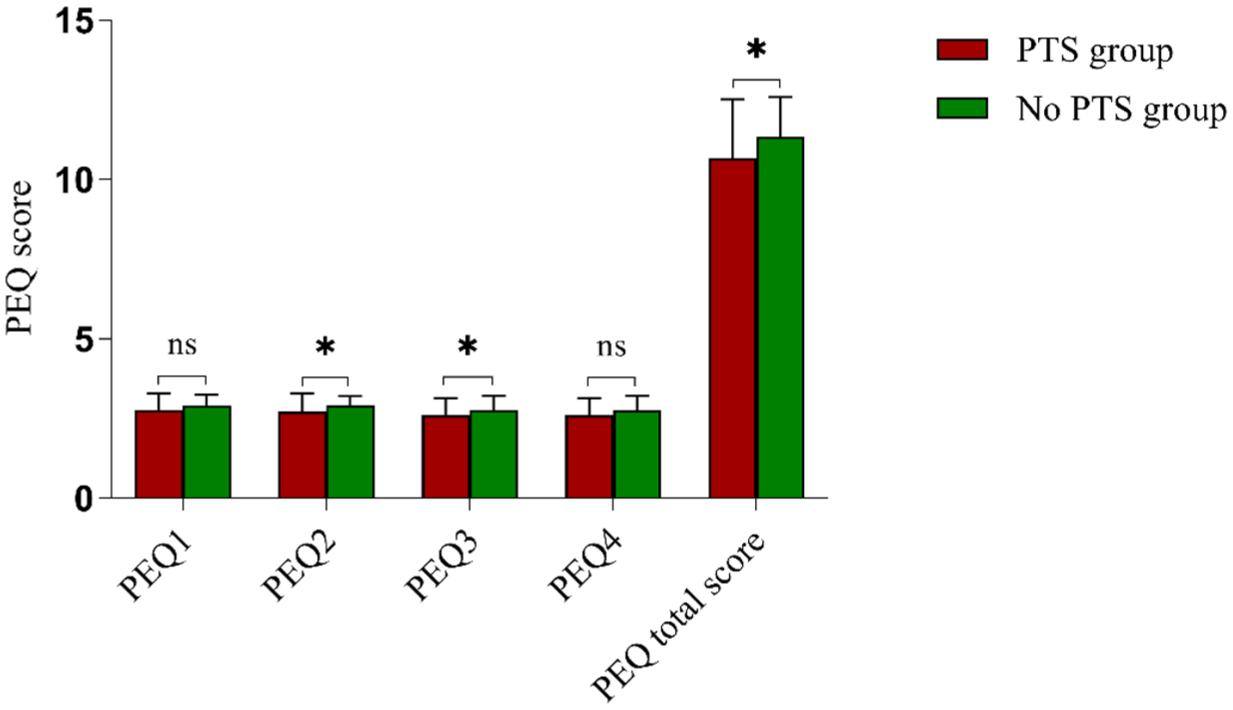
Comparison of scores for each item of the PEQ and the PEQ total score between the PTS and non-PTS groups.
Surgical experience and PTS
The characteristics related to surgery between the PTS and the non-PTS groups in CD patients are detailed in Table 3. Laparoscopic operations were performed in 68.2% of PTS group patients, while colostomy was performed in 63.6%, with a significant difference between the PTS group and the non-PTS group. No significant differences were observed between the two groups in terms of postoperative hospital stay, as well as months since the most stressful hospitalization. Patients with PTS were also likely to have a higher number of hospitalizations for CD than patients without (2.00 ± 1.10 vs 1.73 ± 0.89, p < 0.001). The Prognostic Nutritional Index (PNI) is recognized as a prognostic marker of patients’ nutritional and inflammatory status, with its calculation formula as 10 × ALB (g/dL) + 0.005 × TLC (per mL). A lower PNI value is correlated with a higher probability of postoperative complications. 36 By comparing the PNI values between the two groups, it was found that the PNI value in the PTS group was significantly lower than that in the non-PTS group (41.88 ± 6.30 vs 44.35 ± 7.55, p = 0.043). Consistently, a higher postoperative complication rate of 36.36% (16/44) in the PTS group was observed, compared to the non-PTS group’s rate of 11.25% (9/80, p = 0.001), including infections, anastomotic fistulas, and strictures, among others.
Surgical characteristics of patients with Crohn’s disease.

The asterisk (*) indicates a significant difference at *p* < .05.
The most common PTS symptoms among postoperative CD patients
Based on the PCL-5 scores, we conducted a statistical analysis to calculate the average scores in the domains of Re-Experiencing, Avoidance, Negative Mood, and Increased Arousal for both the PTS and non-PTS groups (Figure 3). Significant differences were observed in the PCL-5 scores for all four symptoms between the two groups (p < 0.05). The average standard scores calculated through the standard formula 24 revealed that the PTS group consistently scored higher than the non-PTS group. Specifically, the symptoms showing the greatest disparity between the PTS and non-PTS groups were Avoidance, followed by Negative Mood. Among patients in the PTS group with CD postsurgery, Re-Experiencing was the most frequently reported symptom, with Negative Mood being the second most prevalent one.
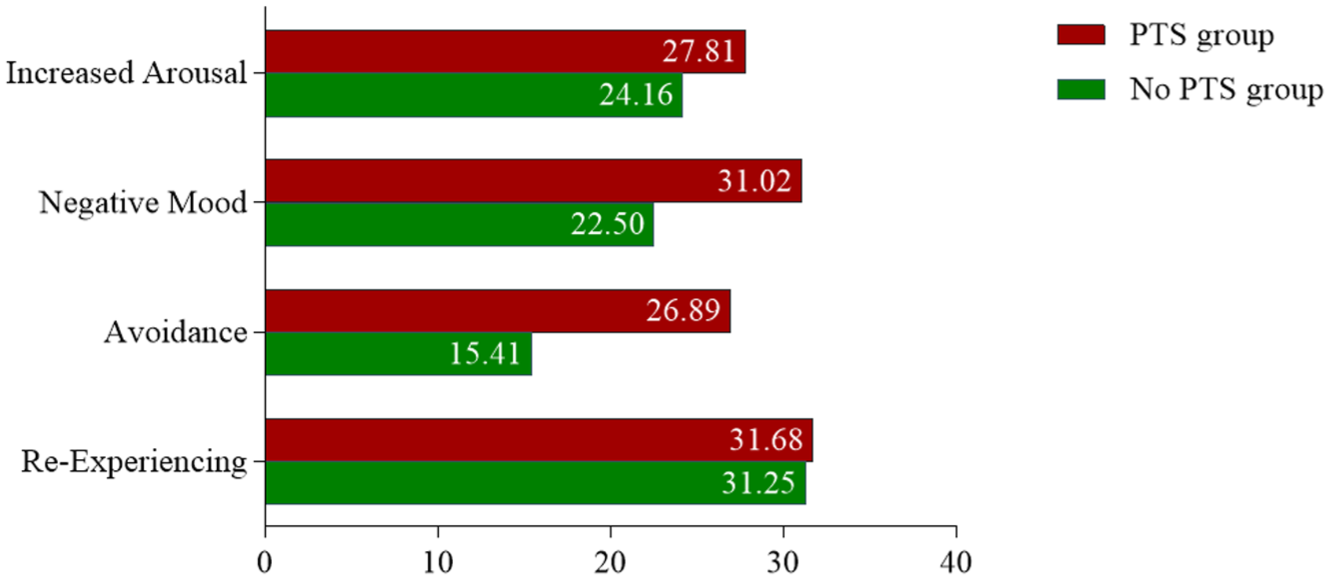
Average standard scores for the four categories of PTS symptoms.
Factors associated with PTS
Statistical analyses were performed to identify potential risk factors for the occurrence of postoperative PTS symptoms in patients with CD. The variables with p < 0.1 from the univariate analysis were further included in a multivariate regression analysis, and the results are presented in Figure 4. The likelihood of an occurrence of PTS symptoms in patients who underwent multiple surgeries was 1.86 times higher than in those who had only a single surgery (95% CI, 1.106–3.140, p = 0.019). Patients experiencing postoperative complications had a 5.55 times higher probability of developing PTS compared to those without complications (95% CI, 1.921–16.125, p = 0.002). Higher monthly family income and a positive inpatient experience were associated with a reduced probability of PTS occurrence (p < 0.05).

Predictors of PTS symptoms in postoperative patients with CD.
Statistical analyses were conducted to examine factors associated with the presence of postoperative PTS symptoms in patients with CD. Variables with p < 0.1 in univariate analysis were included in a multivariate regression model, and the results are presented in Figure 4. Patients who underwent multiple surgeries had higher odds of reporting PTS symptoms compared to those with a single surgery (OR = 1.86, 95% CI, 1.106–3.140, p = 0.019). Similarly, those who experienced postoperative complications were more likely to exhibit PTS symptoms (OR = 5.55, 95% CI, 1.921–16.125, p = 0.002). Conversely, higher monthly household income and more favorable inpatient experiences were associated with a lower likelihood of reporting PTS symptoms (p < 0.05). While these variables were statistically associated with PTS symptomatology, the directionality and causality of these associations cannot be established from the current retrospective data.
Associations between clinical characteristics and PTS symptom dimensions
To further explore the relationship between risk factors and PTS, we reevaluated separate PTS symptoms in postoperative patients with CD, including Re-Experiencing, Avoidance, Negative Mood, and Increased Arousal. The group experiencing postoperative complications showed a significantly higher likelihood of meeting the full PTS criteria compared to the group without complications, including low mood, re-experiencing the event(s) through dreams, flashbacks or intrusive thoughts, physiological hyperarousal, and avoidance behaviors (p = 0.001; Figure 5(a)). PTS symptoms of negative mood, re-experiencing, and increased arousal were associated with having at least 2 CD-related surgery (p < 0.05), whereas Avoidance was considered statistically nonsignificant (p = 0.868; Figure 5(b)).

Distribution of patients meeting PTS symptom cluster criteria, stratified by a history of postoperative complications (a) or multiple surgeries (b).
To further examine the associations between clinical characteristics and distinct PTS symptom dimensions, we analyzed specific symptom clusters in postoperative CD patients, including re-experiencing, avoidance, negative mood, and increased arousal. PTS symptoms—including low mood, intrusive thoughts, nightmares or flashbacks, physiological hyperarousal, and avoidance—were more frequently reported among patients who experienced postoperative complications compared to those who did not (p = 0.001; Figure 5(a)). Additionally, negative mood, re-experiencing, and increased arousal symptoms were more commonly observed in patients who had undergone two or more CD-related surgeries (p < 0.05), whereas avoidance symptoms did not show a statistically significant association (p = 0.868; Figure 5(b)). While these findings highlight potential patterns of association, they do not imply causality. It remains unclear whether these clinical characteristics influence psychological responses or whether shared underlying vulnerabilities contribute to both.
Discussion
PTS has recently emerged as a potential yet underrecognized issue among patients suffering from CD, particularly those undergoing surgical interventions. The present retrospective study sought to examine the occurrence of PTS and its associated clinical and sociodemographic correlates in 124 CD patients following bowel resection. In contrast to the focus of previous studies, the present study placed particular emphasis on the association between specific surgical characteristics and PTS symptoms, a domain that has received scant attention. In the present study, the incidence of PTS symptoms among individuals diagnosed with CD was 35%, which is slightly higher than the previously reported 25%–32% in analogous populations.19,26 This discrepancy may be attributable to the composition of the study population, which consists exclusively of individuals who have undergone surgical interventions. Such procedures are often perceived as physically and emotionally distressing events. However, it is imperative to underscore that while surgery and postoperative complications have been associated with an elevated prevalence of PTS symptomatology, these observations should not be construed as establishing a direct causal relationship. Recent findings suggest a potential link between immune dysregulation and the development of both inflammatory diseases, such as CD, and symptoms associated with PTSD. 37 This finding suggests the possibility of shared underlying mechanisms rather than direct causation.
Our research revealed that symptoms of PTS in patients with CD were frequently accompanied by re-experiencing, such as flashbacks and nightmares, and negative mood, including depression and anxiety. These observations underscore the multifaceted psychological responses associated with CD management and the necessity for supportive care strategies. However, the determination of whether the surgical experience is the primary catalyst for these symptoms or if preexisting vulnerability, such as immune or neuroendocrine dysregulation, plays a more significant role, remains to be elucidated. Contrary to the findings of some prior studies,19,34,35 no statistically significant association was observed between educational background or disease-related knowledge and PTS occurrence. This discrepancy may be indicative of regional or cultural variations in educational distribution and disease awareness, or limitations associated with sample size and study design. Patients with lower household income demonstrated a higher probability of experiencing PTS symptoms. While this may reflect the increased psychological burden associated with financial stress during chronic illness management, we again advise cautious interpretation of the directionality of this relationship. Economic hardship may be a marker of broader psychosocial vulnerability or healthcare access inequities, which are also implicated in psychological stress responses.38,39
Furthermore, patients with elevated disease activity (e.g., HBI and PNI scores) demonstrated an augmented prevalence of PTS symptoms. While it may be tempting to conclude that more severe disease leads to greater psychological burden, it is equally plausible that psychological stress or preexisting immune dysregulation associated with PTS contributes to disease exacerbation. Indeed, previous research has demonstrated links between PTSD and immune dysregulation—including alterations in hypothalamic-pituitary-adrenal (HPA) axis function and inflammatory cytokine expression—even before trauma exposure. 37 These findings underscore the necessity for longitudinal studies to explore the dynamic and potentially reciprocal relationship between psychological and disease-related factors. Patients who underwent multiple surgeries also reported a higher prevalence of PTS symptoms, particularly increased arousal (40%). This phenomenon may be indicative of a cumulative stress effect resulting from repeated invasive procedures. However, it is also conceivable that such elevated stress reactivity may be indicative of a heightened necessity for multiple interventions, attributable to behavioral factors, immune vulnerability, or a combination thereof. A noteworthy finding of the study was the observation that patients who reported fewer positive experiences in the hospital, particularly those who expressed dissatisfaction with the attitudes of the attending physicians and nurses, demonstrated an increased propensity to manifest symptoms consistent with PTS. While subjective perceptions may reflect or exacerbate psychological distress, they could also be modifiable targets for improving patient-centered care and communication, regardless of causality.
The surgical technique was also explored, with open surgery and ostomy associated with a higher PTS symptom burden compared to laparoscopic procedures. These symptoms may include extended recovery periods, observable physical alterations, and heightened discomfort. However, further prospective work is needed to determine whether these associations are due to procedural characteristics themselves or to unmeasured patient-level factors.
A particularly novel finding from our study was the observed association between postoperative complications and PTS symptoms. These patients frequently reported re-experiencing and negative mood symptoms. However, the possibility of bidirectional influence is acknowledged—patients with heightened stress responses or neuroimmune vulnerability may be more susceptible both to complications and to psychological symptoms. Consequently, rather than perceiving complications exclusively as events that induce trauma, it is proposed that they be regarded as components of a comprehensive interactional model that encompasses biological, psychological, and procedural dimensions.
In clinical practice, CD patients who encounter postoperative complications or exhibit other concomitant risk factors should be considered for psychological screening and support. While the data reveal significant patterns of association, they do not permit conclusions about causality. Instead, these observations should be regarded as hypothesis-generating, and further longitudinal and mechanistic studies are necessary to elucidate the underlying processes.
Limitations
The present study has several limitations. Its retrospective design and limited sample size reduce statistical power and prevent causal inferences. The use of online questionnaire distribution may have introduced response bias, and only 124 out of 235 questionnaires were returned (response rate ≈52.8%). Respondents may differ from nonrespondents in ways that influence psychological outcomes, such as disease burden or healthcare engagement, thereby affecting the generalizability of the findings. Despite these limitations, the study raises important hypotheses regarding the interplay between surgical experiences and PTS symptoms in CD patients, which warrant further validation in larger, prospective studies.
Conclusion
Comprehensively, surgery has posed both physical challenges and psychological stress for patients. Therefore, conducting thorough assessments and providing comprehensive care after surgery is crucial in reducing patients’ psychological maladjustment. Prioritizing the holistic needs of patients, which encompass both physical and psychological aspects, may contribute to reducing the incidence of PTS, thereby enhancing the psychological health for postoperative individuals.
Supplemental Material
sj-docx-1-tag-10.1177_17562848251385070 – Supplemental material for Post-traumatic stress disorder symptoms in Crohn’s disease patients following surgery: a cross-sectional study
Supplemental material, sj-docx-1-tag-10.1177_17562848251385070 for Post-traumatic stress disorder symptoms in Crohn’s disease patients following surgery: a cross-sectional study by Lei Jin, Lei Wang, Zhengting Wang, Kingsley Chun Kin Poon, Zirui He, Chen Zhang and Jie Zhong in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-pdf-2-tag-10.1177_17562848251385070 – Supplemental material for Post-traumatic stress disorder symptoms in Crohn’s disease patients following surgery: a cross-sectional study
Supplemental material, sj-pdf-2-tag-10.1177_17562848251385070 for Post-traumatic stress disorder symptoms in Crohn’s disease patients following surgery: a cross-sectional study by Lei Jin, Lei Wang, Zhengting Wang, Kingsley Chun Kin Poon, Zirui He, Chen Zhang and Jie Zhong in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.