
Abstract
Background:
Delayed bleeding is a frequent and serious complication after endoscopic papillectomy (EP). Second-look endoscopy (SLE) is often scheduled on the following day for wound assessment and prophylactic hemostasis, but its clinical value remains unclear.
Objectives:
This study evaluated the effectiveness of SLE in preventing delayed bleeding after EP.
Design:
This study was a multicenter, retrospective cohort study.
Methods:
We retrospectively reviewed 132 consecutive patients who underwent EP at nine high-volume centers between 2003 and 2024 (SLE group, n = 73; non-SLE group, n = 59). Propensity score matching was performed to balance baseline characteristics. The primary outcome was delayed bleeding, and secondary outcomes were risk factors, the impact of prophylactic hemostasis during SLE, and hospital stay.
Results:
After matching, 43 patients were included in each group. The incidence of delayed bleeding did not differ between the SLE and non-SLE groups (14% vs 9%, p = 0.50). Multivariate analysis identified a lack of preventive clipping closure as the only independent risk factor (odds ratio 15, 95% confidence interval 1.3–177, p = 0.030). Prophylactic hemostasis during SLE did not reduce bleeding but was associated with prolonged hospitalization (13 vs 9 days, p = 0.012).
Conclusion:
Routine SLE after EP does not reduce delayed bleeding. Moreover, prophylactic hemostasis in asymptomatic patients may unnecessarily prolong hospitalization. Hemostasis should be reserved for patients who develop clinical signs of bleeding.
Keywords
Introduction
Endoscopic papillectomy (EP), a widely performed endoscopic treatment for duodenal papillary tumors, is a minimally invasive and safer alternative to surgery. However, owing to the anatomical characteristics of the papilla, it is associated with a high risk of bleeding, with delayed bleeding occurring in approximately 20% of cases.1 –5
Although intraoperative bleeding can be promptly identified and treated with endoscopic hemostatic techniques, delayed bleeding is more challenging to manage and potentially life-threatening. Several prophylactic methods have been proposed to reduce the risk of delayed bleeding, including endoscopic clipping closure, epinephrine injection, hemostatic spraying, and argon plasma coagulation (APC).6 –10 However, adequate control of delayed bleeding remains to be achieved. Owing to the high risk of bleeding, second-look endoscopy (SLE) is routinely performed on the day following EP. However, the efficacy of SLE in preventing delayed bleeding remains unproven, and its clinical significance is unclear. The routine performance of SLE following EP imposes a burden on healthcare costs and human resources; therefore, its necessity warrants further evaluation.
In this multicenter retrospective study, we evaluated the effectiveness of SLE in preventing delayed bleeding. To this end, we enrolled patients who underwent EP and analyzed the bleeding events to determine the association between SLE and delayed bleeding.
Methods
Patients
We retrospectively reviewed consecutive patients who underwent endoscopic papillectomy (EP) at nine high-volume centers between November 2003 and December 2024.
Eligible patients included those with histologically confirmed and endoscopically benign ampullary adenomas, as well as those with lesions suspected to be carcinoma in situ who were not suitable candidates for surgery. Patients in whom biopsy findings suggested a neoplastic lesion but the final pathological diagnosis was non-neoplastic were also included. Patients were excluded if they were younger than 20 years of age, had endoscopically unresectable ampullary tumors, showed extension into the pancreas or bile duct, had tumors arising from the minor papilla, or experienced bleeding within 24 h after EP, perforation, or severe pancreatitis. EP was performed in 136 patients during the study period. After excluding three patients with perforation and one patient with early post-procedural bleeding, 132 patients were included in the final analysis. Clinical data were obtained from the electronic medical records. Written informed consent for treatment was obtained from all patients. The study protocol was approved by the Institutional Review Board of Okayama University Hospital (approval number: 2309-028) and conducted in accordance with the Declaration of Helsinki. This study conforms with the guidelines in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 11
EP procedure
Experienced endoscopists performed all EP procedures using side-viewing endoscopes. All lesions were resected using snares with a high-frequency electrosurgical generator. A blended current was used to transect the lesion. The post-resection ulcer was closed with clips as a means of preventive clipping closure, even in the absence of active bleeding. Preventive clipping closure was not standardized during the early study period but was routinely performed at many participating centers during the later period. The clips were placed in the area extending from the lower side of the pancreatic orifice to the anal verge of the post-EP ulcer, without closing the orifices of the pancreatic and bile ducts. Biliary and pancreatic stents were inserted to reduce the risk of post-procedural cholangitis and pancreatitis. Hemostasis with APC, hemostatic forceps, clipping, or injection of a diluted epinephrine solution was performed in cases where bleeding occurred during the procedure. No prophylactic hemostasis other than clip closure was performed during EP in patients without bleeding. The patients were allowed to consume water 2 h after the procedure and eat a light meal 2 days later, provided no complications occurred. Regarding the clinical course after admission, EP was generally performed on the day after admission, the biliary stent was removed 1 week later, and patients were discharged the following day.
Antiplatelet and anticoagulant drugs were either withdrawn or replaced with unfractionated heparin during the EP from 2003 to 2012. From 2012 onward, these agents were administered during EP in accordance with the Japan Gastroenterological Endoscopy Society (JGES) guidelines. 12 Regarding the use of antiplatelet agents, EP was performed without interruption if the patient was taking aspirin or cilostazol alone. If the patient was receiving clopidogrel, aspirin, or cilostazol, they were replaced. Direct oral anticoagulants (DOACs) were discontinued on the morning of EP, and EP was performed with medication reinitiation the following morning. If the patient was on warfarin, a temporary switch to DOACs was made, if possible; otherwise, warfarin was discontinued, and heparin replacement was used.
Second-look endoscopy
SLE was defined as an endoscopy scheduled for wound confirmation of EP-induced artificial ulcers on postoperative day (POD) 1 in asymptomatic patients. Hemostatic intervention performed during SLE was defined as prophylactic hemostasis. Endoscopic findings during SLE were classified according to the Forrest classification. Spurting bleeding (Forrest Ia) and oozing bleeding (Forrest Ib) were defined as active bleeding, whereas non-bleeding visible vessels (Forrest IIa) and adherent clots (Forrest IIb) were defined as high-risk stigmata. 13 No standardized criteria existed across centers regarding the indication for SLE or prophylactic hemostasis; these decisions were made based on the clinical judgment of each endoscopist. During SLE, CO₂ insufflation was performed at all centers. Even in the absence of apparent bleeding, water irrigation was performed to stimulate careful inspection of the resection site. Clipping, hemostatic forceps, injection of a diluted epinephrine solution, and APC were used for prophylactic hemostasis at the discretion of the endoscopist. In cases of prophylactic hemostasis during SLE, a third-look endoscopy was performed at the discretion of the endoscopist, and the fasting period was extended as needed.
Definitions
The primary outcome was the incidence of delayed bleeding after POD1 in the SLE and non-SLE groups. Post-EP bleeding was classified as intraoperative or delayed bleeding based on its timing. Intraoperative bleeding was defined as bleeding that occurred during the endoscopic papillectomy and required hemostasis. Delayed bleeding was defined as bleeding that required unscheduled esophagogastroduodenoscopy with hemostasis after POD1. Bleeding events occurring within 24 h after EP (POD0) and bleeding observed during scheduled SLE were not considered delayed bleeding. Endoscopic surveillance for delayed bleeding was conducted when apparent bleeding symptoms, such as melena or hematemesis, or a decrease in hemoglobin concentration of at least 2.0 g/dL, were present. The severity grades of bleeding were assessed according to the lexicon and severity grading system of the American Society for Gastrointestinal Endoscopy. 14
The secondary outcomes of this study were the risk factors for delayed bleeding, the impact of prophylactic hemostasis during SLE, and the length of hospital stay. To identify the factors associated with delayed bleeding, the following parameters were considered: age, sex, underlying disease, anti-gastric ulcer drug use, antiplatelet and anticoagulant use, procedure time, neoplastic tumor, lesion diameter, piecemeal resection, intraoperative bleeding, preventive clipping closure, SLE, and procedure year. Among patients who underwent preventive clipping closure, the association between the preventive clipping-closure length rate and the risk of delayed bleeding was evaluated. The preventive clipping-closure length rate was computed as the percentage of the actual area clipped within the available area for clipping at the resected site, extending from the lower side of the pancreatic orifice to the anal verge of the post-EP ulcer. The preventive clipping-closure length rate of the frenulum was analyzed using a cutoff value of 65%, based on our previous report. 15
Statistical analyses
Propensity score matching was used to identify matched cohorts within the two patient groups, minimizing confounding biases. The following covariates were included: age, sex, lesion diameter, final diagnosis, underlying disease, antiplatelet and anticoagulant use, use of anti-gastric ulcer drugs, procedure time, en-bloc resection, preventive clipping closure of the frenulum, intraoperative bleeding, and procedure year.16 –18 Propensity scores were estimated using logistic regression, incorporating prespecified covariates. Patients were matched in a 1:1 ratio using nearest-neighbor matching without replacement, applying a caliper of 0.2 to achieve adequate covariate balance. No missing data were identified for the covariates included in the propensity score model. Categorical variables are presented as frequencies and proportions, whereas continuous variables are expressed as medians with interquartile ranges (IQR). Continuous variables were compared using the Wilcoxon rank-sum test or Kruskal–Wallis test, as appropriate. Categorical variables were compared using Fisher’s exact test. Risk factors for delayed bleeding were analyzed in the following two steps. Univariate logistic regression was used to identify the potential risk factors. Multivariate logistic regression was conducted to adjust for confounding effects, with candidate confounders selected according to the modified disjunctive cause criterion. 19 According to this criterion, all variables, except sex and age, were included as candidate confounders. The factors analyzed are listed below each table. Effect estimates are reported as odds ratios (ORs) with 95% confidence intervals (CIs). Differences were considered statistically significant at p < 0.05.
All statistical analyses were performed using the JMP Student’s Edition version 18 for Mac (SAS Institute Inc., Cary, NC, USA), except for the calculation of standardized mean differences, which was conducted using R software (R Foundation for Statistical Computing, Vienna, Austria).
Results
Patient characteristics
This study included 136 patients who underwent EP for ampullary lesions. After excluding four patients based on the exclusion criteria, 132 patients remained, with 73 and 59 patients allocated to the SLE and non-SLE groups, respectively (Figure 1).
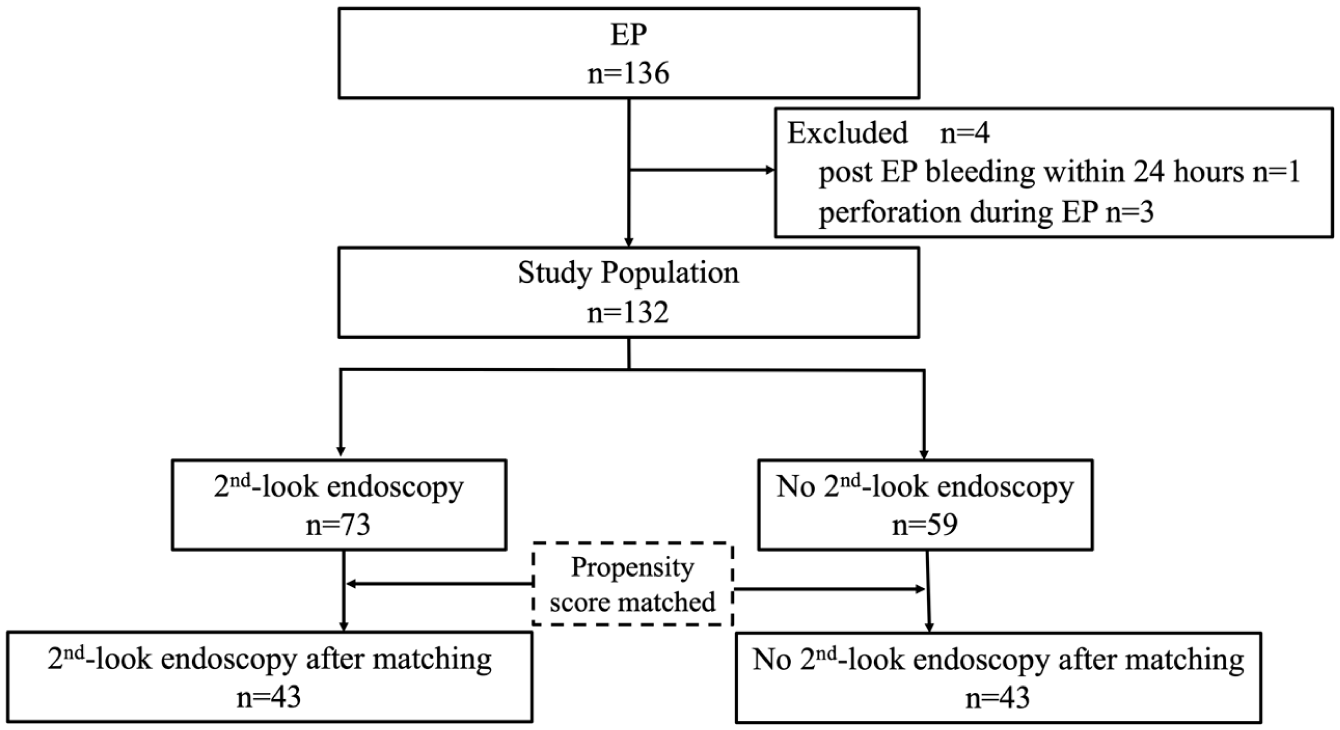
Flowchart of patient inclusion and exclusion in the analysis of delayed bleeding after endoscopic papillectomy. Of the 136 patients who underwent EP for ampullary lesions, four were excluded according to predefined criteria, leaving 132 patients for analysis. Among them, 73 underwent SLE, and 59 did not. After one-to-one propensity score matching, 43 patients were included in each group for the final comparative analysis.
After one-to-one propensity score matching, 43 patients from each group were included in the final analysis. Although a significant difference in lesion diameter, anti-gastric ulcer drug use, and preventive clipping closure of the frenulum was initially observed between the two groups, this imbalance was resolved after matching, resulting in relatively well-balanced patient distribution characteristics (Table 1).
Clinical characteristics of the patients.
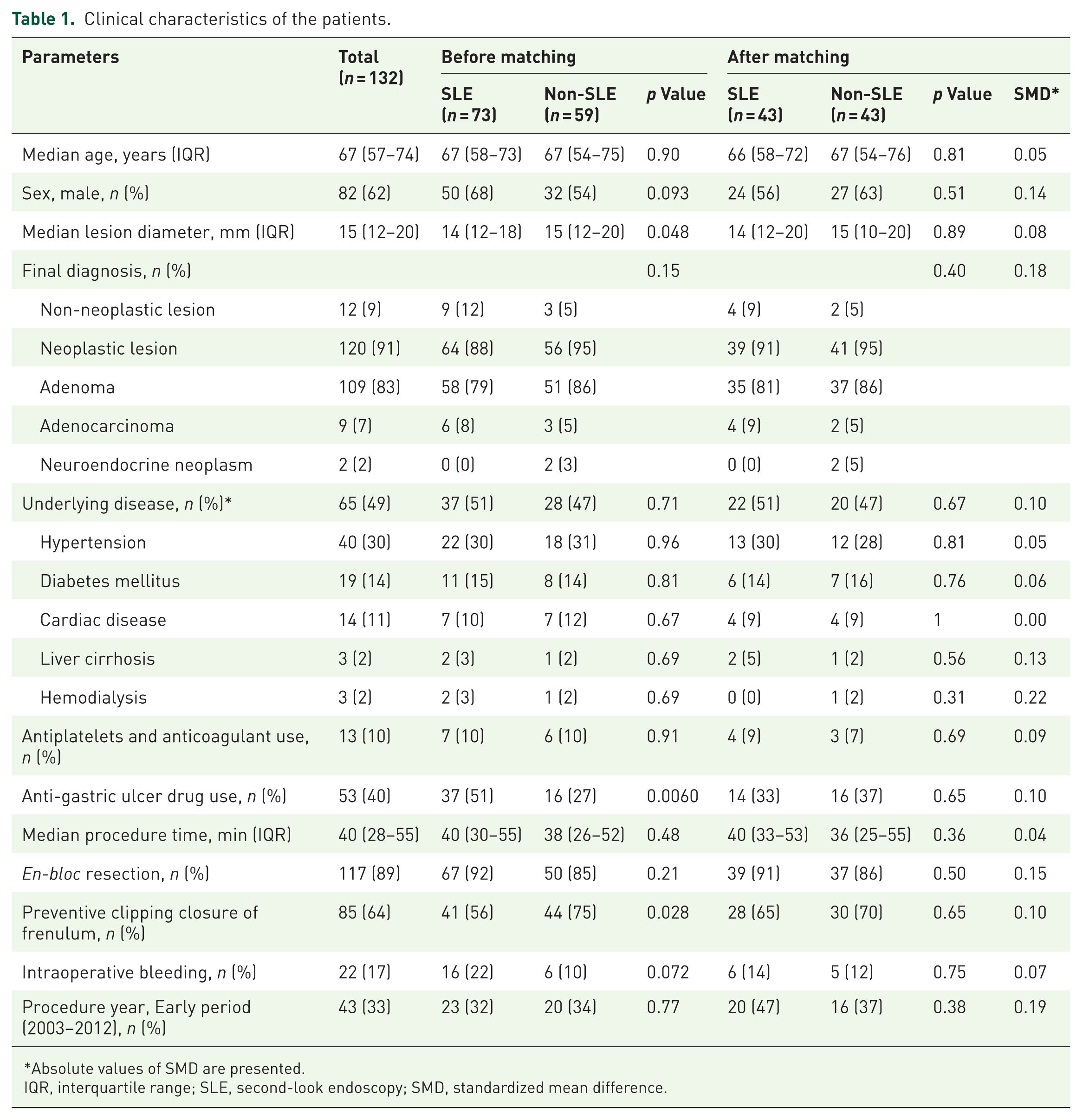
Absolute values of SMD are presented.
IQR, interquartile range; SLE, second-look endoscopy; SMD, standardized mean difference.
SLE versus non-SLE group
The incidence of delayed bleeding was compared between the two groups before and after matching (Table 2). The number of SLE procedures performed at each center is presented in Supplemental Table 1. Delayed bleeding occurred in 16 patients (22%) in the SLE group and 6 (10%) in the non-SLE group before matching (odds ratio (OR) 2.5, 95% confidence interval (CI) 0.90–6.8, p = 0.072). After matching, delayed bleeding occurred in 6 patients (14%) in the SLE group and 4 (9%) in the non-SLE group (OR 1.6, 95% CI 0.41–6.3, p = 0.50). The cumulative incidence of delayed bleeding was not significantly different between the matched groups (log-rank test, p = 0.54; Figure 2). All cases of delayed bleeding were managed with endoscopic treatment alone.
Comparison of delayed bleeding rate between the SLE and non-SLE groups.

CI, confidence intervals; OR, odds ratio; SLE, second-look endoscopy.

Time-to-event curve showing the cumulative incidence of delayed bleeding after endoscopic papillectomy according to SLE status. The cumulative incidence of delayed bleeding did not significantly differ between the SLE group (n = 43) and the non-SLE group (n = 43) after propensity score matching (log-rank test, p = 0.54). All cases of delayed bleeding were successfully managed with endoscopic treatment.
Delayed bleeding was severe in one patient and moderate in the remaining patients. The median period of delayed bleeding was 2.5 days (IQR: 2.0–4.5), and delayed bleeding occurred within 8 days post-EP in all patients.
Among the non-bleeding adverse events, post-EP pancreatitis occurred in 11 (13%) patients (4 in the SLE group and 7 in the non-SLE group), and cholangitis in 2 (2.3%) (zero in the SLE group and two in the non-SLE group) after matching. Patients diagnosed with post-EP pancreatitis were treated with fluid replacement therapy and pancreatic enzyme inhibitors. Although one patient with cholangitis induced by blood clot formation following stent occlusion underwent hemostasis and stent exchange, the other was treated conservatively with fluid replacement and/or antibiotics. None of the patients required surgery or was admitted to the intensive care unit.
Clinical risk factors for delayed bleeding
The clinical characteristics of the patients and lesions were evaluated to identify risk factors for delayed bleeding (Table 3). Multivariate analysis with a selection of confounding factors according to the modified disjunctive cause criterion identified non-clipping closure as the sole risk factor for delayed bleeding (OR, 15; 95% CI, 1.3–177; p = 0.030). However, non-SLE was not associated with the risk of delayed bleeding (OR 0.63, 95% CI 0.17–2.4, p = 0.50). In the multivariate analysis limited to patients who underwent preventive clipping closure, a closure length rate of <65% tended to be associated with a higher incidence of delayed bleeding (OR, 8.2; 95% CI 0.79–87, p = 0.079).
Risk of delayed bleeding after endoscopic papillectomy.

The p value was calculated using Fisher’s exact test.
The multivariate analysis for preventive clipping closure included the following variables as potential confounders: underlying disease, anti-gastric ulcer drug use, antiplatelet and anticoagulant use, procedure time, neoplastic tumor, lesion diameter, piecemeal resection, intraoperative bleeding, preventive clipping closure, SLE, and procedure year.
CI, confidence intervals; NA, not available; OR, odds ratio; SLE, second-look endoscopy.
Comparison of patients based on prophylactic hemostasis in a second-look endoscopy
Prophylactic hemostasis was performed in 33% of patients (14/43) in the SLE group after matching. In the SLE group, delayed bleeding occurred in 21% of patients (3/14) who underwent prophylactic hemostasis and in 10% of those (3/29) who did not. In the non-SLE group, the incidence of delayed bleeding was 9% (4/43). There were no significant differences in the incidence of delayed bleeding between groups after matching (Table 4). Prophylactic hemostasis was performed in four patients with active bleeding (spurting or oozing), six patients with high-risk stigmata (non-bleeding visible vessel or adherent clot), and four patients with no bleeding sign on endoscopic evaluation during SLE (Supplemental Figure 1).
Incidence of delayed bleeding in prophylactic hemostasis during second-look endoscopy.

CI, confidence intervals; OR, odds ratio; SLE, second-look endoscopy.
The length of hospital stay was significantly longer in patients with delayed bleeding (13 vs 10 days, p = 0.012) and in those who required prophylactic hemostasis in the SLE group (13 vs 9 days, p = 0.012; Table 5).
Comparison of hospital stay according to events after matching.
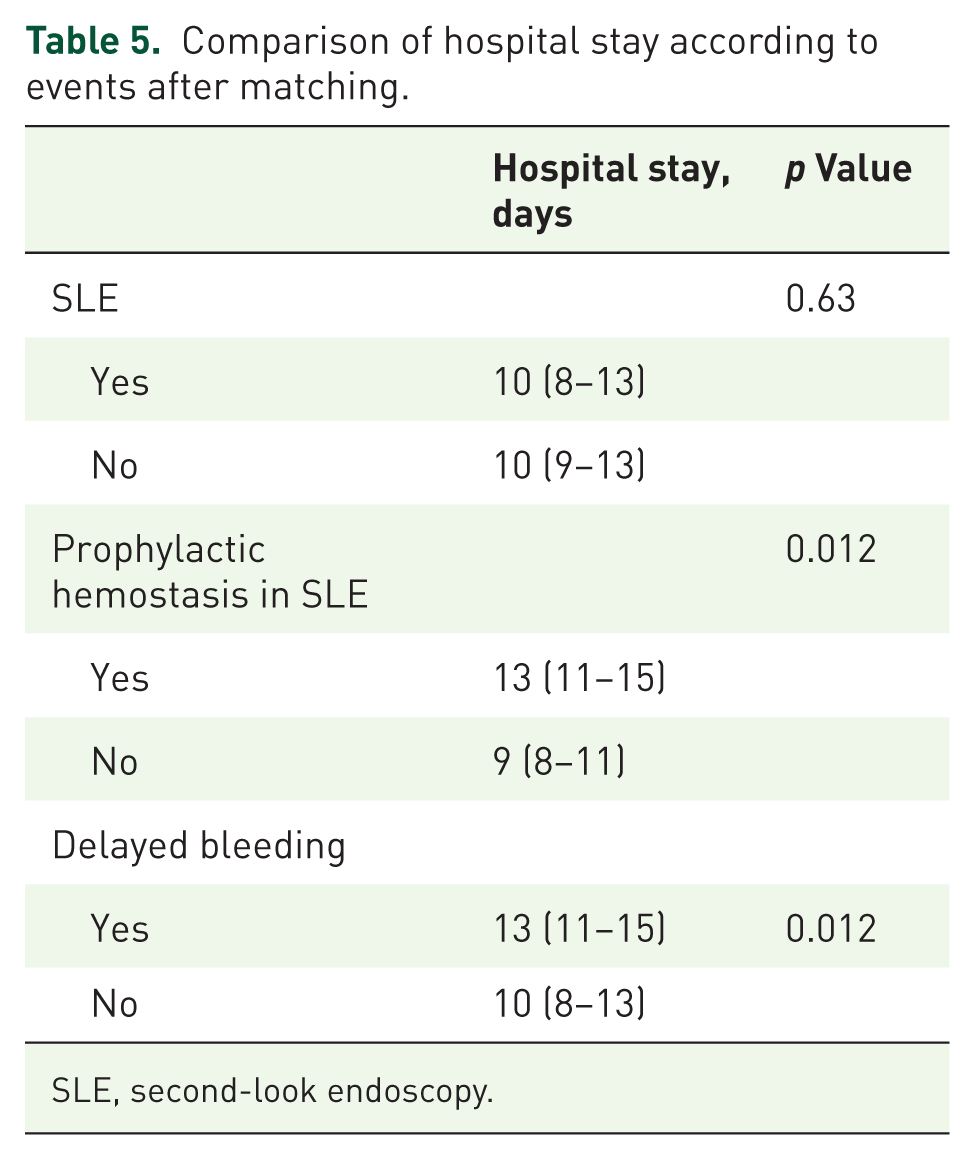
SLE, second-look endoscopy.
Discussion
To our knowledge, this is the first study to investigate whether post-EP SLE reduces delayed bleeding. Herein, the incidence of delayed bleeding in the SLE group did not significantly differ from that in the non-SLE group. Prophylactic hemostasis during SLE may be unnecessary or excessive. Furthermore, prophylactic hemostasis performed during SLE is associated with a significantly prolonged hospital stay. The results of this study suggest that routine SLE may be unnecessary, prompting the reevaluation of established clinical practice. Hemostasis is necessary only in patients with delayed bleeding presenting with clinical symptoms.
Several studies have examined the role of SLE in other endoscopic procedures, focusing on gastric endoscopic submucosal dissection (ESD).20 –24 Randomized controlled trials (RCTs) assessing the efficacy of SLE in gastric ESD have reported that SLE does not provide a clinical benefit for reducing delayed bleeding.22 –24 Moreover, previous studies have shown that scheduled second-look endoscopy does not reduce delayed bleeding, even among patients receiving antithrombotic therapy. 20 In addition, a previous meta-analysis reported that delayed bleeding occurred more frequently in patients who underwent prophylactic hemostatic interventions during SLE than in those who did not. 21 Notably, prophylactic hemostasis did not significantly reduce the risk of delayed bleeding. Furthermore, patients who received prophylactic hemostasis during SLE were found to have a significantly prolonged length of hospital stay compared to those managed without additional hemostatic intervention. 21
Similar results were observed in the present study, which focused on EP. The incidence of delayed bleeding in the SLE group did not significantly differ from that in the non-SLE group. Although the incidence of delayed bleeding did not significantly differ between patients who received prophylactic hemostasis and those who did not, the bleeding rate was higher in patients who received prophylactic hemostasis. One possible explanation is that insufflation or hemostasis during SLE may cause tissue injury, potentially leading to the exposure of submucosal vessels and subsequent bleeding. 21 From this perspective, prophylactic hemostasis during SLE may paradoxically increase delayed bleeding risk. 21 Indeed, patients who underwent prophylactic hemostasis during SLE tended to more frequently exhibit high-risk stigmata of bleeding. However, the incidence of delayed bleeding did not differ between the SLE and non-SLE groups, which suggests that some patients may have received unnecessary hemostatic intervention. Regarding hospital stay, prolonged hospitalization was observed in patients who underwent prophylactic hemostasis in the SLE group, which may be attributed to the need for additional endoscopic procedures to confirm hemostasis as well as the fasting periods implemented until hemostasis was achieved. When performing SLE, the potential for extended hospitalization should be considered. Furthermore, avoiding unwarranted SLE after EP may lead to significant savings in medical costs and human resources, thereby alleviating the overall burden on endoscopy services.
While previous studies focusing on the risk factors for post-EP bleeding are limited, few have listed these risk factors, including the use of anticoagulants, large ampullary tumors, intraoperative bleeding, and non-endoscopic clipping closure.16 –18 Our study revealed the lack of preventive clipping closure as the sole risk factor for delayed bleeding. Non-SLE was not a risk factor for delayed bleeding (p = 0.50). Even when the analysis was restricted to patients with clip closure, SLE did not reduce the incidence of delayed bleeding (SLE group, 12% (5/41) vs. non-SLE group, 9% (4/44); p = 0.64). These results emphasize that SLE has no preventive effect on delayed bleeding, regardless of whether risk factors are present or absent.
This study has several limitations. First, although it was a multicenter study, the sample size after propensity score matching was relatively small, and the number of delayed bleeding events was limited, which may have reduced the statistical power to detect differences. Second, the long study period of more than 20 years inevitably introduced heterogeneity in clinical practice, including perioperative management of antithrombotic agents, the development of endoscopic devices, and institutional protocols, all of which might have affected outcomes. To account for potential temporal bias, the procedure year was incorporated as a covariate in the propensity score model and included in the multivariate analysis. The results were essentially unchanged. Third, the decision to perform SLE and the choice of prophylactic hemostatic method were left to the discretion of individual endoscopists, resulting in a lack of uniformity. The SLE and prophylactic hemostasis groups may have included a higher proportion of patients at an increased risk of bleeding; therefore, the possibility of indication bias cannot be excluded. Although we performed propensity score matching to adjust for measured baseline characteristics, unmeasured confounders, such as the endoscopist’s subjective assessment of bleeding risk and operator experience, may have influenced both the decision to perform SLE and the occurrence of delayed bleeding. In addition, center-level confounders related to institution-specific practice patterns cannot be fully excluded. Despite these limitations, our study included consecutive patients from nine high-volume centers, applied rigorous propensity score matching, and consistently demonstrated that SLE did not confer a preventive effect on delayed bleeding. Therefore, we believe our findings provide meaningful evidence to reconsider the necessity of routine SLE after EP.
Conclusion
SLE did not prevent delayed bleeding following EP. Prophylactic hemostasis in asymptomatic patients was not associated with a reduction in delayed bleeding, but rather, it was linked to prolonged hospitalization. Our findings suggest that routine use of SLE is not necessary. Multicenter prospective studies involving a larger population and further investigations in high-risk bleeding groups remain warranted.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261439231 – Supplemental material for Second-look endoscopy does not reduce delayed bleeding after endoscopic papillectomy: a multicenter propensity score-matched analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848261439231 for Second-look endoscopy does not reduce delayed bleeding after endoscopic papillectomy: a multicenter propensity score-matched analysis by Yuki Fujii, Kazuyuki Matsumoto, Toru Ueki, Hitomi Himei, Ichiro Sakakihara, Eijiro Ueta, Tatsuya Toyokawa, Ryo Harada, Taiji Ogawa, Takeshi Tomoda, Hironari Kato, Toshiharu Mitsuhashi, Ryosuke Sato, Akihiro Matsumi, Kazuya Miyamoto, Daisuke Uchida, Shigeru Horiguchi, Koichiro Tsutsumi and Motoyuki Otsuka in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848261439231 – Supplemental material for Second-look endoscopy does not reduce delayed bleeding after endoscopic papillectomy: a multicenter propensity score-matched analysis
Supplemental material, sj-docx-2-tag-10.1177_17562848261439231 for Second-look endoscopy does not reduce delayed bleeding after endoscopic papillectomy: a multicenter propensity score-matched analysis by Yuki Fujii, Kazuyuki Matsumoto, Toru Ueki, Hitomi Himei, Ichiro Sakakihara, Eijiro Ueta, Tatsuya Toyokawa, Ryo Harada, Taiji Ogawa, Takeshi Tomoda, Hironari Kato, Toshiharu Mitsuhashi, Ryosuke Sato, Akihiro Matsumi, Kazuya Miyamoto, Daisuke Uchida, Shigeru Horiguchi, Koichiro Tsutsumi and Motoyuki Otsuka in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tiff-3-tag-10.1177_17562848261439231 – Supplemental material for Second-look endoscopy does not reduce delayed bleeding after endoscopic papillectomy: a multicenter propensity score-matched analysis
Supplemental material, sj-tiff-3-tag-10.1177_17562848261439231 for Second-look endoscopy does not reduce delayed bleeding after endoscopic papillectomy: a multicenter propensity score-matched analysis by Yuki Fujii, Kazuyuki Matsumoto, Toru Ueki, Hitomi Himei, Ichiro Sakakihara, Eijiro Ueta, Tatsuya Toyokawa, Ryo Harada, Taiji Ogawa, Takeshi Tomoda, Hironari Kato, Toshiharu Mitsuhashi, Ryosuke Sato, Akihiro Matsumi, Kazuya Miyamoto, Daisuke Uchida, Shigeru Horiguchi, Koichiro Tsutsumi and Motoyuki Otsuka in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors thank all members of the participating institutions in the study. The authors thank Kota Sakamoto, PhD, Department of Biostatistics, Division of Data Science, Center for Innovative Medical Research and Development for his statistical support.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.