
Abstract
Eosinophilic esophagitis (EoE) is a chronic immune-mediated disease in which symptoms correlate imperfectly with histologic and structural activity, necessitating repeated endoscopy for diagnosis and monitoring. As therapeutic options expand, including biologic agents, there is an increasing need for biomarkers that can inform clinical decision-making and support treat-to-target strategies. This narrative review synthesizes current evidence on tissue-based, circulating, and minimally invasive biomarkers in EoE and proposes a compartment-based clinical hierarchy to contextualize their performance in routine practice. While type 2 cytokine pathways define disease biology, their systemic measurement demonstrates limited diagnostic and monitoring value. By contrast, tissue transcriptomic signatures and esophageal-proximal assessments—particularly eotaxin-3 and eosinophil-derived granule proteins—show stronger correlation with mucosal inflammation and therapeutic response. Structural and epithelial markers further highlight that histologic remission does not necessarily equate to restoration of mucosal integrity. Across domains, biomarker utility follows a consistent gradient, with tissue and luminal assessments most closely reflecting active disease, whereas circulating markers serve adjunctive roles. Histologic scoring systems remain the reference standard; however, multimodal integration of molecular and minimally invasive tools may enable remodeling-aware monitoring and reduce endoscopy burden in selected clinical contexts. Prospective validation within clearly defined management algorithms is required before routine implementation.
Plain language summary
Eosinophilic esophagitis (EoE) is a chronic inflammatory disease of the esophagus that causes swallowing problems and food impaction. Currently, diagnosis and monitoring usually require repeated endoscopy with biopsies, which can be uncomfortable for patients and costly for healthcare systems. Researchers are therefore investigating biomarkers—measurable biological signals that reflect inflammation or tissue damage—as potential tools to assess disease activity and treatment response without repeated invasive procedures. This review summarizes current knowledge about different types of biomarkers in EoE, including tissue-based markers, blood markers, and minimally invasive sampling methods such as the esophageal string test. The article proposes a framework that organizes these biomarkers according to how closely they reflect inflammation in the esophagus. Overall, tissue and esophageal-proximal biomarkers appear to provide the most accurate information about disease activity, while blood markers may play a supportive role. Better biomarker strategies could help reduce the need for repeated endoscopy and support more personalized management of patients with EoE in the future.
Keywords
Introduction
Eosinophilic esophagitis (EoE) is a chronic, immune-mediated esophageal disease marked by eosinophil-predominant epithelial infiltration and symptoms of esophageal dysfunction, most commonly dysphagia and food impaction. Symptoms correlate imperfectly with histologic and structural activity, so diagnosis and longitudinal monitoring still rely on repeated endoscopy with biopsy—burdensome for patients and resource-intensive for healthcare systems.
At the molecular level, EoE is dominated by a type 2 helper T-cell (Th2) inflammatory axis characterized by overproduction of interleukin (IL)-4, IL-5, and IL-13, along with downstream induction of eosinophil chemoattractants such as eotaxin-3 (CCL26). Transcriptomic and translational studies have established IL-13 as a central effector cytokine, orchestrating a disease-specific epithelial gene-expression signature that promotes chemokine production, barrier dysfunction, and remodeling.1–3 Overexpression of eotaxin-3 correlates strongly with local eosinophilia and mast cell infiltration,4,5 reinforcing the concept that epithelial activation and chemokine signaling extend beyond simple peak eosinophil counts and contribute to structural disease progression.
Diagnosis integrates symptoms of esophageal dysfunction with ⩾15 eosinophils per high-power field (eos/HPF) in esophageal biopsies after exclusion of secondary causes. Contemporary consensus frameworks no longer require a proton pump inhibitor (PPI) trial; PPI response is now considered a therapeutic phenotype within the EoE spectrum rather than a separate entity. 6 Recent ACG guidance (2025) similarly emphasizes symptom plus ⩾15 eos/HPF after exclusion of alternative causes and recommends monitoring by combining symptom assessment with endoscopic and histologic evaluation. 7
Despite increasing standardization, variability in histologic thresholds, biopsy protocols, and interpretive criteria persists, complicating cross-study comparisons and potentially reducing diagnostic sensitivity given the patchy distribution of inflammation.8–10 Endoscopic features such as rings, furrows, and exudates are specific but insensitive, necessitating histologic confirmation. 11 Importantly, remission based solely on eosinophil density does not necessarily indicate restoration of epithelial integrity or reversal of structural remodeling.12–14
Recent advances have therefore shifted attention toward molecular and minimally invasive diagnostics. The EoE Diagnostic Panel, a gene-expression-based assay, has demonstrated high diagnostic accuracy in pediatric and adult cohorts. 15 Minimally invasive sampling approaches, including the esophageal string test (EST) and brush-based techniques, capture eosinophil-derived proteins and chemokines directly from the site of inflammation and show strong correlation with mucosal activity. 16 This mismatch provides the clinical rationale for tissue-proximal and remodeling-oriented biomarkers in longitudinal monitoring. The therapeutic landscape of EoE has evolved rapidly. Targeted biologic therapies, including IL-4Rα blockade with dupilumab, 17 and an FDA-approved budesonide oral suspension (EOHILIA), 18 introduce response paradigms that extend beyond eosinophil suppression alone. In this context, monitoring must distinguish inflammatory control from persistent epithelial dysfunction and remodeling; however, integration into routine practice remains fragmented, and a structured framework linking biomarker compartments to defined clinical decision points is lacking.
In this narrative review, we synthesize experimental, translational, and clinical evidence on tissue-based, circulating, and minimally invasive biomarkers in EoE and propose a compartment-based hierarchy to interpret their performance in practice. We emphasize how biomarker domains map to key clinical decisions—diagnostic confirmation, longitudinal monitoring, therapeutic stratification, and remodeling risk—according to sampling proximity and monitoring utility.
Search strategy and study selection
This clinically oriented narrative review used targeted searches of PubMed/MEDLINE and Scopus (2000–January 2026) for studies on biomarkers in EoE, including transcriptomics, eotaxin-3/IL-13, eosinophil-derived proteins, the EST, and minimally invasive monitoring. Reference lists of selected articles were screened to identify additional relevant publications. Priority was given to human studies, prospective cohorts, and investigations evaluating diagnostic performance, correlation with histologic activity, therapeutic response, and clinical applicability; mechanistic studies were included when translationally relevant. As a narrative review, formal systematic review methodology was not applied.
Key molecular and cellular interactions underlying type 2 inflammation in EoE and informing compartment-specific biomarker assessment are summarized in Figure 1.

Compartment-specific inflammatory and remodeling pathways in EoE. Schematic of the type 2 inflammatory network in EoE showing epithelial barrier disruption, release of alarmins (TSLP, IL-33, IL-25), Th2 cytokine activation (IL-4, IL-5, IL-13), and IL-13-driven induction of eotaxin-3 (CCL26), promoting eosinophil recruitment/degranulation and progressive remodeling through TGF-β-associated fibrotic signaling. The figure highlights how distinct components of this cascade correspond to specific biomarker compartments: tissue transcriptomic signatures (e.g., CCL26, CAPN14), luminal eosinophil-derived granule proteins (MBP, ECP, EDN, EPX), and structural remodeling markers (e.g., periostin and barrier protein alterations). Together, these interactions provide the biologic rationale for a compartment-based hierarchy of biomarker performance in clinical monitoring.
Molecular pathogenesis and key biomarker axes
The molecular framework of EoE reflects a coordinated interaction between epithelial barrier dysfunction, type 2 cytokine activation, and eosinophil recruitment. These processes not only define disease biology but also establish distinct biomarker compartments that differ in their proximity to mucosal inflammation and structural remodeling.
The Th2 inflammatory axis
EoE is driven by a Th2-skewed immune response in which IL-13, IL-5, and IL-4 coordinate epithelial activation, chemokine induction, and eosinophil recruitment. Among these cytokines, IL-13 functions as a central effector mediator. It induces CCL26 (eotaxin-3) via STAT6-dependent signaling, promotes eosinophil recruitment, and impairs epithelial barrier integrity, thereby linking inflammatory activation with structural remodeling.19–21
Overexpression of eotaxin-3 correlates strongly with local eosinophilia and mast cell infiltration,1–4 reinforcing the concept that epithelial chemokine signaling integrates inflammatory burden with tissue injury. Single-cell analyses further demonstrate that type 2 cytokine production is largely compartmentalized to the esophageal mucosa, highlighting that local molecular signatures more accurately reflect disease activity than circulating cytokine measurements. 22
Upstream epithelial-derived alarmins, including thymic stromal lymphopoietin and IL-33, amplify Th2 differentiation and sustain cytokine signaling within the esophageal microenvironment.23,24 Genetic association studies implicate epithelial and cytokine-regulatory pathways in disease susceptibility.25,26 Downstream of IL-13 signaling, esophagus-specific targets such as CAPN14 contribute to epithelial fragility and barrier dysfunction. 27
These mechanisms support tissue-level transcriptomic biomarkers: IL-13-inducible genes such as CCL26 and CAPN14 integrate inflammatory activation with early remodeling and represent proximal indicators of active disease.1–4,27
Eosinophilic activation and degranulation
Eosinophil accumulation within the esophageal mucosa represents a hallmark of EoE. Recruitment and survival are sustained by the Th2 cytokine milieu, particularly IL-5 and IL-13.28–33 Experimental models confirm that IL-5-driven eosinophilia contributes to esophageal remodeling, while IL-5 neutralization reduces tissue eosinophil density without consistently normalizing symptoms,34–37 underscoring the complexity of inflammatory and structural interactions.
Activated eosinophils release cytotoxic granule proteins, including major basic protein (MBP), eosinophil cationic protein (ECP), eosinophil-derived neurotoxin (EDN), and eosinophil peroxidase (EPX).38–40 These mediators disrupt epithelial integrity, increase permeability, and contribute to neuromuscular dysfunction. Importantly, extracellular deposition of granule proteins may persist even after reductions in viable eosinophil counts, reflecting cumulative mucosal injury rather than instantaneous cellular density.38–40
Eosinophil-derived mediators also interact with mast cells and fibroblasts, amplifying local cytokine signaling and promoting extracellular matrix deposition through TGF-β-associated pathways.32,35,41–43 This interplay contributes to the transition from predominantly inflammatory to fibrostenotic disease phenotypes.
From a clinical perspective, eosinophil-derived granule proteins represent direct indicators of mucosal injury rather than upstream immune activation. Their diagnostic and monitoring performance, therefore, depends strongly on the sampling compartment, with tissue and esophageal-proximal assessments more accurately reflecting active inflammation than circulating measurements.
Together, the Th2 cytokine axis and eosinophil degranulation define interconnected but distinct biomarker domains. These domains vary in their proximity to inflammatory activity and structural remodeling, forming the basis for a compartment-based hierarchy of biomarker performance in EoE.
A summary of the key inflammatory pathways is presented in Table 1.
Key inflammatory pathways in EoE and their relevance for biomarker development.

CCL26, eotaxin-3; ECP, eosinophil cationic protein; EDN, eosinophil-derived neurotoxin; EPX, eosinophil peroxidase; IL, interleukin; MBP, major basic protein; Th2, type 2 helper T-cell; TSLP, thymic stromal lymphopoietin.
Molecular and soluble biomarkers
Cytokine biomarkers: Clinical and translational perspective
Type 2 cytokines constitute the biological core of EoE; however, their clinical utility varies substantially depending on sampling compartment and intended application. Tissue studies consistently demonstrate overexpression of IL-13 and IL-5 in active disease, accompanied by induction of eotaxin-3 (CCL26) and related downstream mediators.1–4,19–21 These signals correlate with mucosal eosinophilia and histologic activity, positioning IL-13- and IL-5-associated pathways as central drivers of epithelial dysfunction and eosinophil recruitment rather than merely inflammatory epiphenomena.19–22,32–37
IL-13 drives a disease-specific epithelial program characterized by CCL26 induction, barrier disruption, and remodeling signatures.1–4,19–21 IL-5 sustains eosinophil survival and activation within the tissue microenvironment.32–34 Importantly, type 2 cytokine production in EoE is largely compartmentalized to the esophageal mucosa, with multiple immune cell subsets contributing to local amplification.22,41 These observations provide a biological rationale for prioritizing tissue-level or tissue-proximal biomarker strategies over systemic measurements.
Therapeutic interventions further validate the centrality of this axis. Topical corticosteroids reduce IL-5, IL-13, and eotaxin-3 expression in parallel with histologic improvement.43,49–52 IL-13-targeted therapies (RPC4046, QAX576, cendakimab) normalize IL-13-dependent transcripts and reduce eosinophil density and endoscopic activity,49–51 while IL-4Rα blockade with dupilumab improves both histologic and symptomatic outcomes. 17 Anti-IL-5 approaches consistently reduce tissue eosinophilia, although symptom responses are variable.35,37 Collectively, these data establish type 2 cytokines as validated therapeutic nodes and mechanistic anchors of disease activity.
By contrast, circulating cytokine measurements show limited diagnostic and monitoring performance. Selected eosinophil-related proteins and chemokines, including MBP and eotaxin-3, may show moderate correlations with tissue eosinophilia in certain cohorts,53–56 but rarely provide stand-alone discrimination. Serum IL-4, IL-5, and IL-13 generally do not reliably distinguish active EoE from controls and show inconsistent change with therapy,56–58 consistent with mucosal compartmentalization of type 2 inflammation.
From a response-enrichment perspective, IL-13-associated tissue signatures appear particularly informative. Patients with elevated IL-13/CCL26 transcript modules derive greater benefit from IL-13 blockade, suggesting a potential role for tissue transcriptomic profiling in therapeutic stratification.49–51 However, such approaches currently remain investigational and require further validation before routine implementation.
Age and atopic comorbidity further influence cytokine interpretation. Pediatric cohorts may demonstrate more pronounced systemic eosinophilia, whereas adult disease often appears more tissue-restricted.57,58 Concomitant atopic inflammation may amplify circulating type 2 signals and reduce specificity for esophageal disease when interpreted in isolation.19–21
Chemokines and adhesion molecules: From tissue signal to clinical utility
Chemokines orchestrate the migration and retention of inflammatory cells in EoE, linking epithelial cytokine activation with tissue eosinophilia. Among these mediators, eotaxin-3 (CCL26) remains the most consistently overexpressed chemokine in active disease and one of the most reproducible epithelial transcripts identified across independent cohorts.1–4,19–21 By contrast, thymus and activation-regulated chemokine (TARC/CCL17), although relevant in other type 2-mediated disorders, has demonstrated inconsistent expression and limited clinical utility in EoE. 54
Across sampling compartments, tissue-based detection of eotaxin-3 provides the most robust diagnostic discrimination. Gene-expression panels and immunohistochemical studies consistently identify CCL26 as one of the strongest epithelial signals distinguishing active EoE from remission or non-EoE controls.1–4,15,19–21 Tissue expression correlates closely with mucosal eosinophil density and reflects direct IL-13-dependent epithelial activation.1,2,19–21,55,59
Esophageal-proximal sampling platforms further translate this biology into clinically actionable tools. The EST captures luminal eotaxin-3 and related inflammatory proteins with strong correlations to peak eosinophil counts and high diagnostic accuracy across pediatric and adult cohorts.44–46,54 By contrast, serum eotaxin-3 measurements show inconsistent elevations and limited correlation with histologic activity or therapeutic response.57,60 Brush-based sampling approaches also demonstrate strong performance in detecting chemokines and eosinophil-derived proteins,54,61 although sensitivity varies with sampling depth and disease phenotype.
Therapeutic modulation provides additional validation of chemokine relevance. Topical corticosteroids reduce mucosal eotaxin-3 expression alongside IL-5, IL-13, and eosinophil density,43,52 and IL-13-targeted biologics similarly downregulate CCL26 and related transcripts.50,51 In minimally invasive platforms such as the EST, composite biomarker panels incorporating eotaxin-3 demonstrate responsiveness to dietary and pharmacologic therapy, supporting their potential role in longitudinal monitoring.46,61
Importantly, eotaxin-3 overexpression reflects active type 2-driven inflammation but does not independently distinguish between classical EoE and patients achieving histologic response to PPI therapy, now recognized as a therapeutic phenotype within the EoE spectrum rather than a separate entity. 62 This highlights that chemokine expression mirrors inflammatory activity rather than defining disease subtype.
Interpretation of chemokine-based biomarkers must also account for atopic background and IgE-mediated sensitization patterns, which may influence systemic type 2 signals without necessarily reflecting esophageal inflammation. 63 Objective mucosal or luminal measurements, therefore, remain essential when integrating biomarker data with allergy testing.
Eosinophil-derived granule proteins: Tissue activity and translational relevance
Eosinophil-derived granule proteins—including ECP, EDN, MBP, and EPX—represent biologically proximate readouts of active mucosal injury in EoE. Unlike upstream cytokines or chemokines, these mediators directly reflect eosinophil activation and degranulation within the esophageal mucosa, thereby linking inflammatory burden with epithelial damage and structural alteration.38–40
Granule proteins are released through piecemeal degranulation and cytolytic mechanisms, both documented in active EoE. 38 Their extracellular deposition contributes to epithelial disruption, increased permeability, and neuromuscular dysfunction, and may persist in tissue beyond reductions in viable eosinophil counts. This biological proximity underlies their appeal as biomarkers of active disease and cumulative mucosal injury.
Among circulating markers, EDN and ECP have been most extensively evaluated. In pediatric and mixed-age cohorts, both are generally elevated in active disease and may decrease following dietary or corticosteroid therapy.54–56,64–69 EDN, in particular, has demonstrated dynamic changes during treatment and rebound following therapy discontinuation in selected cohorts. 67 However, effect sizes vary, and adult-only studies show more inconsistent diagnostic discrimination.54,65,70
MBP correlates with peak eosinophil density and endoscopic severity in selected datasets, 53 suggesting an association with inflammatory burden. Nevertheless, serum MBP levels do not consistently track short-term therapeutic response,53,70 indicating that systemic measurement may incompletely capture localized remodeling and injury.
Performance improves when granule proteins are assessed in tissue-proximal or luminal compartments. Esophageal brushing and string-based sampling demonstrate strong correlations between EDN, MBP-1, and EPX concentrations and mucosal eosinophilia, with high diagnostic discrimination reported in pediatric cohorts.61,68 In some studies, luminal EDN outperformed peripheral blood eosinophil counts in identifying active inflammation. 68 These findings reinforce the importance of sampling compartments when translating eosinophil biology into clinically actionable tools.
Despite their biologic coherence, granule proteins are not universal stand-alone biomarkers: correlations with histology are moderate and cohort-dependent, and systemic levels may be influenced by age, atopic comorbidity, and disease phenotype.53,54,64–71 Their greatest utility appears to lie in adjunctive monitoring—particularly EDN and ECP in pediatric populations—or in minimally invasive esophageal-proximal platforms. A summary of the clinical performance and limitations of granule protein-based biomarkers is presented in Table 2.
Clinical use-cases and performance characteristics of major biomarker domains in EoE.

ECP, eosinophil cationic protein; EDN, eosinophil-derived neurotoxin; EoEHSS, Eosinophilic Esophagitis Histology Scoring System; EPX, eosinophil peroxidase; EST, esophageal string test; IL, interleukin; MBP, major basic protein.
Clinical application across soluble biomarker domains follows a consistent hierarchy. Tissue cytokine signatures are most informative for biologic endotyping and response enrichment; chemokine-based markers such as eotaxin-3 are most useful for diagnostic confirmation and tissue-proximal monitoring; and eosinophil-derived granule proteins function best as indicators of active mucosal injury, particularly in luminal or minimally invasive platforms. Circulating measurements, in contrast, are supportive rather than decisive and are best interpreted in combination with tissue-proximal or histologic assessments.
Histopathological and tissue biomarkers
Quantitative and semi-quantitative histologic scoring (Eosinophilic Esophagitis Histology Scoring System)
Peak eosinophil density has traditionally served as the primary histologic criterion for diagnosing EoE, but alone incompletely captures architectural change and remodeling. The Eosinophilic Esophagitis Histology Scoring System (EoEHSS) addresses this limitation by scoring inflammatory severity (grade) and structural extent (stage) across eight histologic domains.72,73
These domains span inflammatory and structural features (e.g., eosinophilic inflammation with abscesses/surface layering, basal zone hyperplasia, dilated intercellular spaces, epithelial alteration/dyskeratosis, and lamina propria fibrosis), enabling multidimensional assessment beyond peak eosinophil counts.73,74
Across clinical cohorts, composite grade and stage scores discriminate active EoE from remission and from non-EoE comparators such as gastroesophageal reflux disease (GERD).73,74 Importantly, structural domains—particularly basal zone hyperplasia and dilated intercellular spaces—may remain abnormal even when peak eosinophil counts fall below conventional diagnostic thresholds. 12
Correlations between EoEHSS and endoscopic severity further support its translational value. Moderate-to-strong associations with EREFS subscores have been reported, in some cases exceeding correlations observed with peak eosinophil counts alone. 13 In pediatric populations, EoEHSS has demonstrated greater responsiveness to histologic change than peak eosinophil density, particularly when structural domains are incorporated.14,75
Associations between histologic scores and symptom burden remain variable, reflecting the well-recognized dissociation between symptoms and tissue inflammation in EoE.14,74 Nevertheless, remodeling-related domains such as lamina propria fibrosis may provide insight into long-term disease behavior and fibrostenotic risk rather than short-term symptomatic fluctuation. 76
From a clinical perspective, EoEHSS shifts histologic assessment from a binary eosinophil threshold toward a multidimensional evaluation of inflammatory and structural activity. This distinction is particularly relevant when interpreting apparent histologic remission, as persistent epithelial and fibrotic abnormalities may indicate incomplete mucosal recovery. Histologic scoring, therefore, remains the reference framework against which emerging molecular and minimally invasive biomarkers must be validated.
The integration of EoEHSS domains with IL-13-associated epithelial remodeling pathways relevant to clinical interpretation of remission and progression is illustrated in Figure 2.
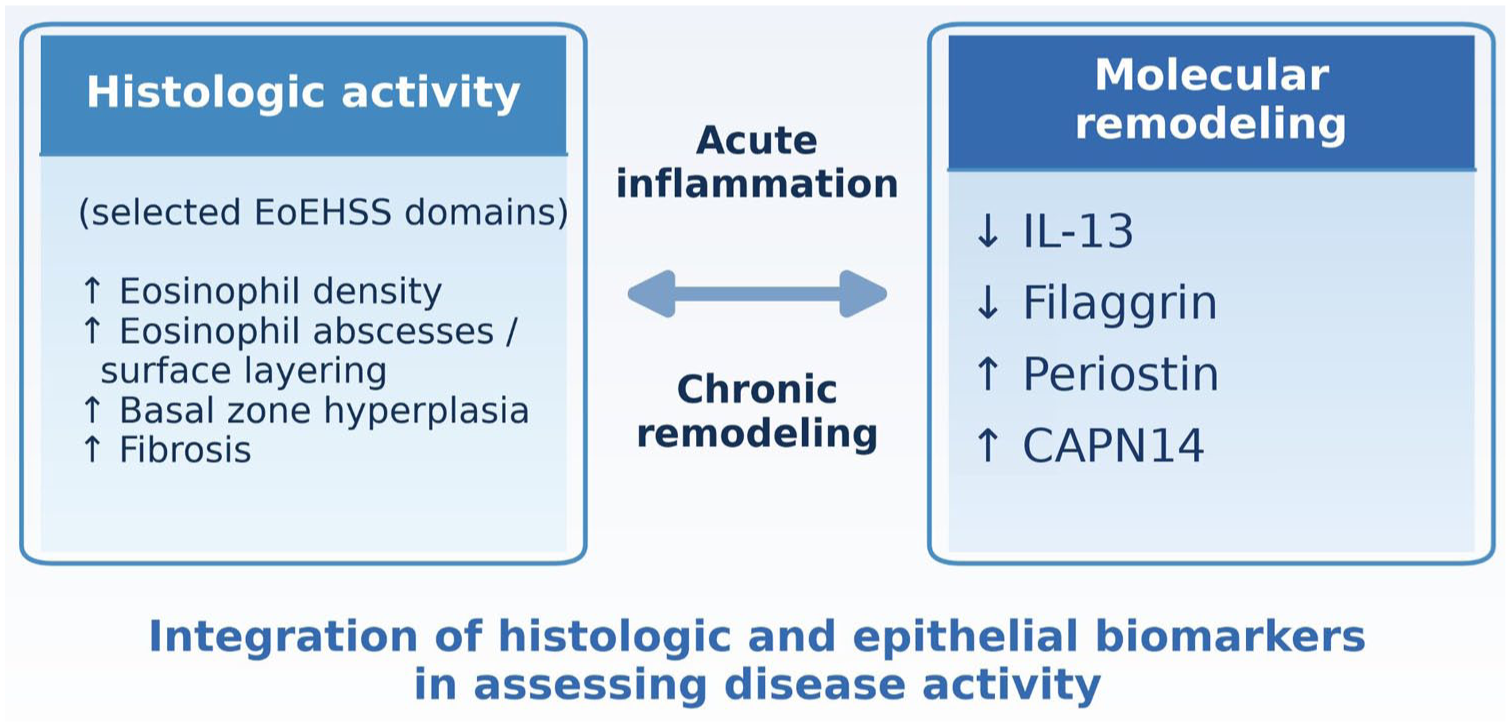
Integration of inflammatory and structural domains in eosinophilic esophagitis. Histologic features captured by EoEHSS—including eosinophil density/degranulation, basal zone hyperplasia, and fibrosis—reflect active inflammatory and remodeling processes. Persistent type 2 signaling, particularly IL-13-associated pathways, contributes to epithelial barrier dysfunction and extracellular matrix deposition even when peak eosinophil counts decline. The figure emphasizes that inflammatory remission does not necessarily equate to structural normalization, highlighting the need to integrate histologic scoring with molecular and remodeling markers in longitudinal disease assessment.
Epithelial and structural markers: Remodeling beyond inflammation
Building on the limitations of eosinophil density and histologic scoring alone, epithelial and structural biomarkers address whether histologic improvement is accompanied by restoration of mucosal integrity. In EoE, persistent epithelial fragility and extracellular matrix remodeling may continue despite reductions in peak eosinophil density, indicating that inflammatory control and structural recovery are not synonymous.
Periostin is among the most consistently upregulated structural markers in active EoE across pediatric and adult cohorts.77–79 As an IL-13-induced matricellular protein, periostin promotes eosinophil adhesion and extracellular matrix deposition 80 and correlates with basal zone hyperplasia and reduced esophageal distensibility in selected cohorts. 79 Periostin overexpression may persist despite histologic remission, indicating incomplete structural normalization even when eosinophil counts decline. 81
Filaggrin, a key epithelial barrier protein, is consistently downregulated in active disease.77,82 IL-13-mediated suppression of filaggrin contributes to impaired barrier integrity and increased permeability. 83 Although topical corticosteroid therapy may partially restore filaggrin expression, normalization appears variable and may depend on chronicity and remodeling burden.78,82 This incomplete reversibility underscores the distinction between inflammatory remission and epithelial recovery.
Desmoglein-1, another critical adhesion molecule, is similarly reduced in active EoE. 77 Loss of desmoglein-1 disrupts epithelial cohesion and contributes to dilated intercellular spaces, a domain captured within EoEHSS. Persistent downregulation has been observed even in patients meeting histologic remission criteria, further illustrating the dissociation between inflammatory endpoints and structural integrity.81,84
CAPN14, an esophagus-specific protease induced by IL-13, represents a particularly compelling remodeling-associated marker. 26 Its upregulation disrupts epithelial cytoskeletal organization and junctional stability, reinforcing barrier fragility. The tissue specificity of CAPN14 and its tight linkage to type 2 signaling suggest potential value in identifying active epithelial remodeling, although routine clinical implementation remains investigational. 85
Persistent epithelial and extracellular matrix alterations may drive luminal narrowing and fibrostenotic transformation (rings/strictures), and together these markers outline a remodeling phenotype that may identify risk despite apparent inflammatory control.
Clinical perspective
Structural and epithelial biomarkers expand assessment beyond inflammatory cell counts and can refine interpretation of remission and remodeling risk, but are not yet suitable as stand-alone monitoring tools. Long-term disease control is best evaluated by integrating histologic, molecular, and functional parameters (Table 3).
Epithelial and structural biomarkers in EoE: remodeling signatures and clinical implications.
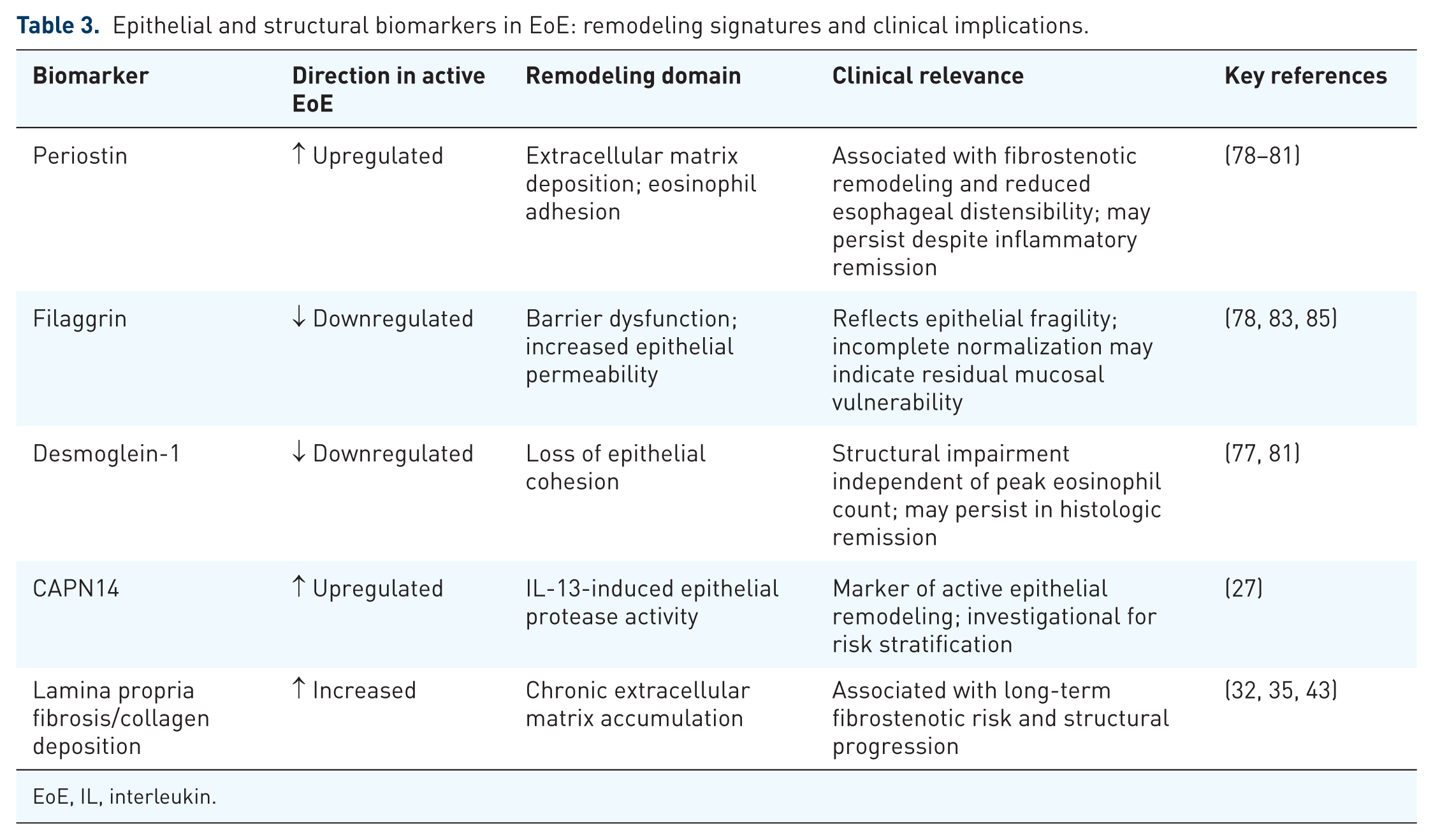
EoE, IL, interleukin.
Circulating and noninvasive biomarkers
Circulating eosinophil-related biomarkers
Circulating biomarkers represent an accessible but biologically diluted compartment in EoE. Absolute eosinophil count (AEC) and eosinophil-derived granule proteins—particularly EDN and ECP—have been most extensively studied as potential noninvasive surrogates of tissue activity.
In pediatric cohorts, AEC and EDN demonstrate moderate correlations with esophageal eosinophil density. 86 However, diagnostic discrimination decreases in adult populations, where systemic eosinophilia often fails to distinguish active disease from remission. 87 These age-dependent differences likely reflect variation in systemic versus tissue-restricted inflammatory patterns.
EDN and ECP may decrease following corticosteroid or dietary therapy in selected cohorts,64–67,69 yet effect sizes are variable and insufficient to support stand-alone monitoring strategies, particularly in adults.54,65,70 Similarly, circulating IL-5 and IL-13 measurements demonstrate limited diagnostic and longitudinal performance despite their mechanistic relevance.44,67
Eosinophil progenitor cells represent a more mechanistically proximal circulating marker and have shown promising specificity in pediatric cohorts. 88 However, data remain limited, and validation in broader adult populations is required.
Clinical perspective
Circulating biomarkers are attractive due to accessibility but lack sufficient sensitivity and specificity to replace histologic assessment. 56 Their role is best considered adjunctive, particularly in pediatric disease or as longitudinal trend indicators rather than definitive markers of mucosal activity.
Luminal and minimally invasive sampling methods
Esophageal-proximal sampling approaches capture biomarkers directly from the site of inflammation and demonstrate superior correlation with mucosal activity.
The EST has shown the most reproducible performance across pediatric and adult cohorts. Luminal concentrations of EDN, MBP-1, EPX, and related proteins correlate with peak eosinophil counts and demonstrate high diagnostic accuracy.54,44–46,89–91 Importantly, EST-derived biomarkers respond dynamically to corticosteroid and dietary therapy, supporting their potential utility in longitudinal monitoring.
Esophageal brushing techniques similarly demonstrate strong discrimination, particularly for EDN in pediatric populations.61,68 Cytosponge-based approaches show moderate performance, although sensitivity may vary depending on sampling depth and mucosal contact.54,61
In addition, esophageal mucosal impedance (MI) provides a functional assessment of epithelial barrier integrity rather than inflammatory protein burden. Distinct impedance patterns have been shown to differentiate EoE from GERD, with more diffuse esophageal involvement in EoE.92,93 Unlike EST-based platforms, MI reflects permeability and structural alteration rather than eosinophil-derived mediators and may therefore complement inflammatory biomarkers. 94 However, longitudinal monitoring data remain limited, and its role is currently adjunctive.
Exploratory modalities, including salivary microRNAs, have demonstrated moderate discrimination but limited correlation with histologic eosinophilia. 95 Other nonendoscopic strategies, such as fractional exhaled nitric oxide and pharyngeal swabs, have not consistently correlated with esophageal inflammation.16,96
Clinical perspective
Among nonendoscopic strategies, esophageal-proximal sampling platforms—particularly the EST—currently provide the strongest alignment with histologic activity and treatment response. While not universally applicable (e.g., in advanced strictures), these approaches represent the most promising pathway toward reducing endoscopy burden in selected monitoring scenarios.
The current evidence on noninvasive and minimally invasive monitoring platforms in EoE is summarized in Table 4.
Monitoring performance and practical considerations of circulating and nonendoscopic biomarker platforms in EoE.
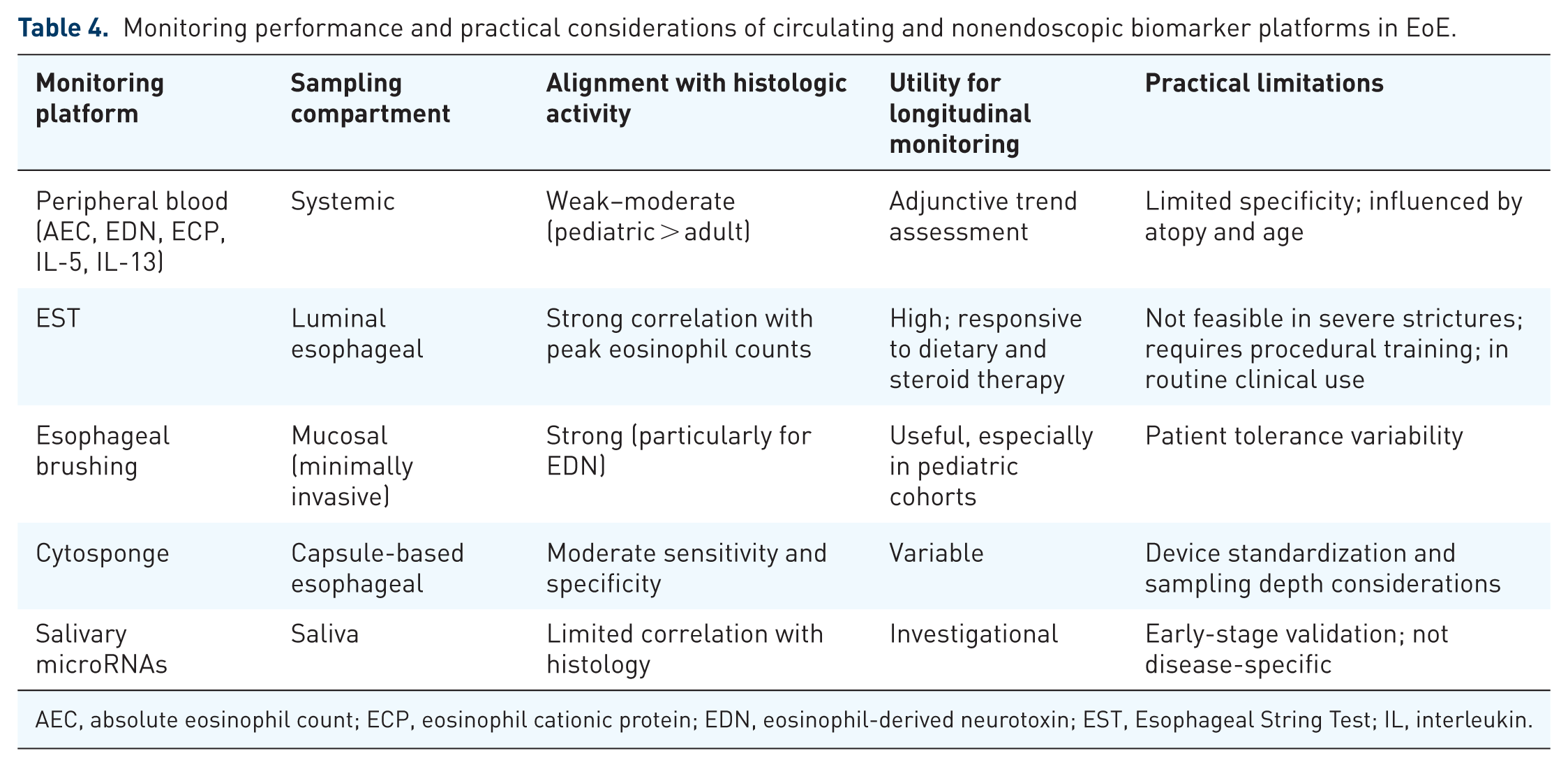
AEC, absolute eosinophil count; ECP, eosinophil cationic protein; EDN, eosinophil-derived neurotoxin; EST, Esophageal String Test; IL, interleukin.
Correlation of biomarkers with disease activity and treatment response
Biomarkers reflecting disease activity
Across biomarker domains, correlation with histologic activity consistently follows a compartment-dependent gradient. Tissue-based and esophageal-proximal biomarkers demonstrate the strongest quantitative alignment with peak eosinophil counts and endoscopic severity indices.44–46,53,97,98 Luminal measurements of eosinophil-derived proteins and chemokines correlate closely with mucosal inflammation and outperform most circulating assays in both pediatric and adult cohorts.
By contrast, circulating markers—including AEC, EDN, and ECP—show moderate correlations in selected pediatric populations but limited discriminatory capacity in adults.86,87 Serum cytokines such as IL-5 and IL-13, despite their mechanistic centrality, do not reliably distinguish active disease from remission when measured systemically.19,44 These findings reinforce that systemic measurements incompletely capture tissue-restricted inflammation.
Structural and remodeling markers add further nuance. Histologic scoring systems, such as EoEHSS, correlate with endoscopic severity and capture epithelial and fibrotic abnormalities beyond eosinophil density alone.12–14 Persistent remodeling features may therefore reflect chronic disease burden rather than short-term inflammatory fluctuations.
These findings support a hierarchy in which tissue and luminal biomarkers best reflect active disease, while circulating markers remain adjunctive.
Biomarkers predicting or monitoring treatment response
Evidence for predictive and longitudinal utility remains limited. Among circulating markers, EDN and AEC demonstrate dynamic changes in selected pediatric and mixed-age cohorts during corticosteroid or dietary therapy.65–67 However, effect sizes are variable and insufficient to replace histologic reassessment.
Tissue transcriptomic signatures, particularly IL-13-associated modules, have shown potential for response enrichment in trials of IL-13-targeted therapies.49–51 These findings suggest a future role for molecular endotyping in therapeutic stratification, although routine implementation remains investigational.
Minimally invasive esophageal-proximal sampling platforms currently provide the most consistent signal for longitudinal monitoring. EST- and brush-based assessments demonstrate responsiveness to therapeutic modulation and strong correlation with histologic improvement.44–46,56,68,99,100
Clinical application
At diagnosis, when symptoms and tissue findings are discordant, and when fibrostenotic progression is suspected, biopsy-based assessment remains necessary. During longitudinal follow-up after treatment initiation in otherwise uncomplicated disease, tissue-proximal luminal tools—particularly EST-based platforms—can serve as first-line monitoring approaches, with repeat endoscopy reserved for discordant biomarker results, persistent symptoms, or concern for remodeling. Circulating biomarkers are best interpreted as adjunctive trends rather than as stand-alone decision-making tools.
A proposed clinical decision framework integrating histologic assessment, molecular biomarkers, and minimally invasive platforms, according to sampling proximity, is presented in Figure 3.
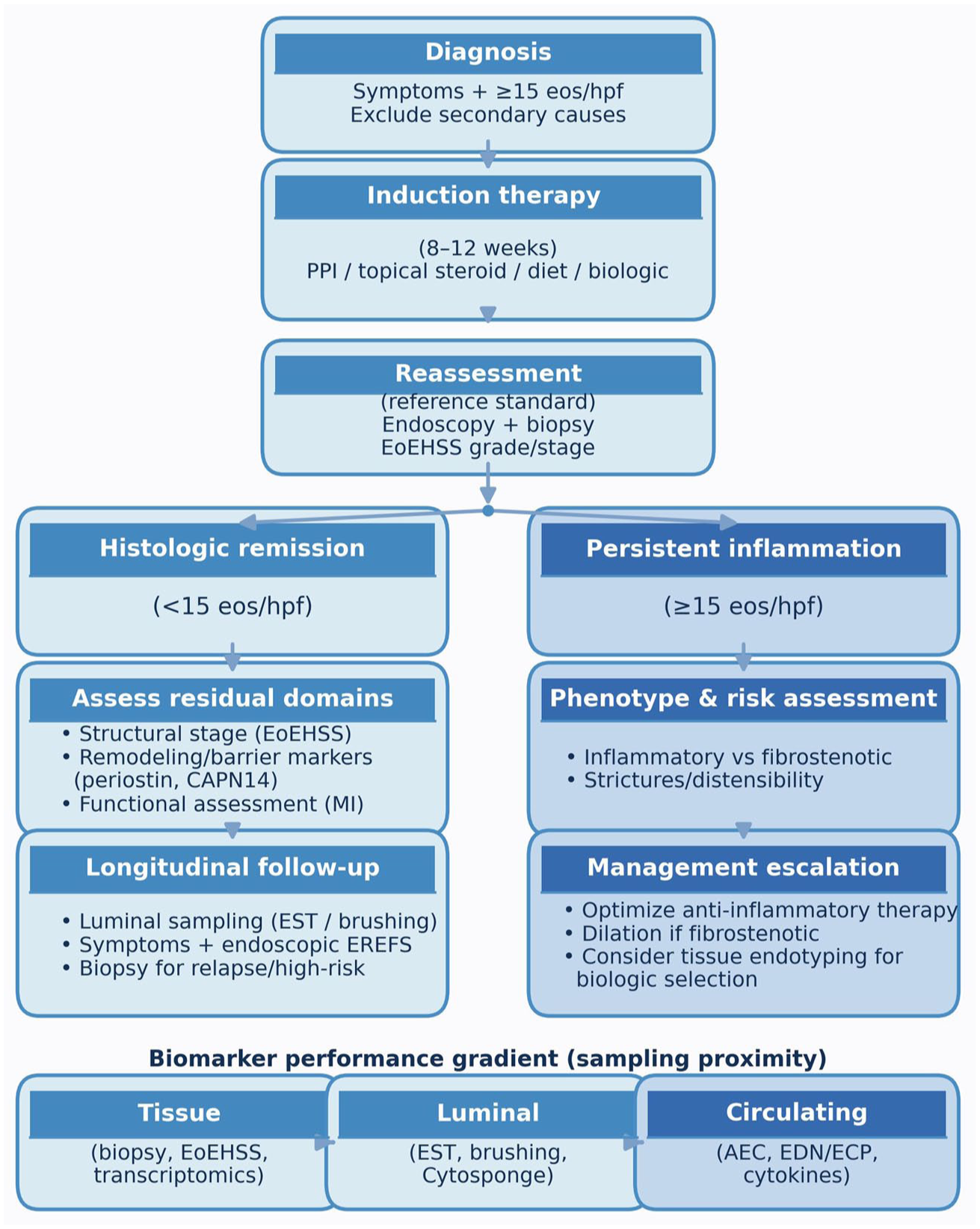
Compartment-based monitoring algorithm in eosinophilic esophagitis. Proposed clinical framework integrating histologic assessment, molecular biomarkers, and minimally invasive platforms according to sampling proximity and monitoring utility. Tissue-based evaluation remains the reference standard, while luminal and circulating biomarkers provide compartment-specific adjunctive information in defined clinical scenarios.
Limitations of current biomarker research
Despite substantial advances, biomarker research in EoE remains limited by methodological heterogeneity and insufficient external validation. Most studies assessing circulating, luminal, and tissue-based markers are single center with small sample sizes, restricting reproducibility across populations.16,54,101–103 Variability in histologic thresholds, biopsy protocols, and remission definitions further complicates comparisons and may introduce misclassification bias.8,104,105
Patient heterogeneity adds complexity. Pediatric and adult cohorts differ in inflammatory patterns, yet age-stratified analyses are inconsistently performed.16,101 Concomitant atopic disease may reduce the specificity of circulating biomarkers,16,106 and inflammatory versus fibrostenotic phenotypes are not uniformly incorporated into threshold development. 62
Technical variability across assay platforms, sampling methods, detection limits, and reporting standards further limits comparability.16,101,103 Even established markers such as EDN and eotaxin-3 demonstrate heterogeneous performance depending on cohort characteristics and sampling approach. As in other immune-mediated diseases, harmonized methodologies and clinically contextualized cutoffs are prerequisites for implementation. 107
Prospective multicenter validation remains scarce. Few platforms have undergone external validation, standardized comparison with histologic scoring systems, or cost-effectiveness analysis.16,54,101
Consequently, while biomarker-guided monitoring cannot yet universally replace biopsy-based assessment in routine practice, emerging evidence suggests that EST-based approaches may reduce the need for repeated endoscopic biopsy in selected monitoring scenarios.89–91
Clinical perspective
The main barriers to implementation are the lack of standardized thresholds, multicenter validation, and integration into clinical algorithms—key steps to transition from biomarker discovery to biomarker-guided management in EoE.
Future perspectives
Future biomarker integration in EoE will likely rely on multimodal frameworks combining histologic, molecular, and minimally invasive assessments. Rather than positioning biopsy and biomarkers as mutually exclusive, future monitoring strategies should integrate histology, molecular profiling, and minimally invasive luminal assessments according to clinical context. Transcriptomic platforms such as the EoE Diagnostic Panel demonstrate high diagnostic accuracy in formalin-fixed specimens. 15 Broader molecular approaches, including RNA sequencing and microRNA profiling, further define disease heterogeneity and endotypes.108,109 Proteomic and multi-omics strategies provide complementary insight into inflammatory and remodeling pathways,110–112 although clinical implementation will require simplified panels, reproducible thresholds, and validation in diverse cohorts.
Artificial intelligence-assisted histologic analysis is another evolving direction. Machine-learning applications to gene-expression datasets and digitized histology enable automated classification and quantitative assessment113,114 and may enhance reproducibility if externally validated.
Implementation remains challenging and requires prospective multicenter validation within standardized clinical algorithms. A near-term goal is to develop compartment-based monitoring pathways in which tissue-derived signatures and esophageal-proximal sampling complement histology while reserving biopsy for high-risk, discordant, or structurally complex cases.
Conclusion
Current evidence supports moving beyond a purely biopsy-centered view of monitoring in EoE toward a compartment-informed, multimodal approach. Tissue-level and esophageal-proximal biomarkers track active mucosal inflammation and treatment response more closely than circulating measures, whereas structural and histologic tools, such as EoEHSS, remain the most informative for assessing remodeling and fibrostenotic risk.
Within this framework, circulating biomarkers are best considered adjunctive trend indicators, while luminal platforms—particularly the EST—have progressed beyond a promising concept. EST has been clinically validated in pediatric and adult cohorts and is now in routine clinical use as a minimally invasive option that can reduce reliance on repeated endoscopy with biopsy in selected monitoring scenarios.
Biopsy-based assessment remains important when diagnostic uncertainty persists, complications or remodeling require direct evaluation, or biomarker and clinical findings are discordant. Future studies should therefore focus less on whether biomarkers have a role in EoE monitoring and more on how best to integrate validated markers into standardized, clinically actionable algorithms.