
Abstract
Background:
Inflammatory bowel disease (IBD) and celiac disease (CeD) are immune-mediated digestive disorders with shared genetic, immunological, and environmental risk factors.
Objectives:
This study aimed to assess whether the coexistence of CeD and IBD is associated with a differential IBD disease course.
Design:
Multicenter case-control study.
Methods:
This study included patients with both CeD and IBD, and controls with IBD alone in a 1:2 ratio, matched by sex, IBD type, and year of diagnosis. CeD was diagnosed based on a Marsh score >1. Data on IBD phenotype and treatment, mortality and neoplasm development were collected from medical records.
Results:
The study included 66 celiac-IBD patients (30 ulcerative colitis, 6 indeterminate colitis, 30 Crohn’s disease; mean age 30 ± 14 years) and 132 non-celiac-IBD patients (68 ulcerative colitis, 4 indeterminate colitis, 60 Crohn’s disease; mean age 32 ± 14 years). Among patients with CeD, Marsh type 3 was the most frequently observed lesion. No significant differences were observed between celiac and non-celiac-IBD patients in terms of IBD extension, extraintestinal manifestations, or coexisting autoimmune diseases. Similarly, no differences were found in outcomes including perianal disease, use of mesalamine, immunomodulators, biologics, need for surgery, or development of neoplasms. No deaths occurred in either group.
Conclusion:
In this large multicenter cohort, the concurrent diagnosis of CeD and patients with IBD was not associated with a different IBD phenotype or worse outcomes compared to non-celiac-IBD patients. The coexistence of CeD does not appear to alter the natural history of IBD.
Plain language summary
What was already known? Inflammatory bowel disease (IBD), which includes Crohn’s disease and ulcerative colitis, and celiac disease, are digestive disorders caused by an abnormal immune response. Both conditions share some genetic and environmental risk factors and can sometimes occur in the same person. However, it was unclear whether having celiac disease in addition to IBD could make IBD more severe or change its course. What did we want to study? We aimed to compare the course of IBD in patients who also had celiac disease with that of patients with IBD alone, to determine whether the coexistence of both conditions influenced the type of IBD, its severity, or the treatments required. How was the study performed? We conducted a multicenter study including 66 patients with both IBD and celiac disease and compared them with 132 similar patients with IBD without celiac disease. The groups were matched by sex, type of IBD, and year of diagnosis. Medical records were reviewed to collect information on disease extent, symptoms outside the intestine, treatments received, need for surgery, development of cancer, and survival. What did we find? No important differences were observed between patients with and without celiac disease. Both groups showed similar IBD characteristics, including disease extent and behavior. There were also no differences in complications such as perianal disease, use of immunosuppressive or biologic drugs, need for surgery, development of tumors, or mortality. What do these results mean? Having celiac disease in addition to IBD does not appear to worsen the course of IBD or modify its natural history. This information can help reassure patients and clinicians that the coexistence of celiac disease is unlikely to negatively affect IBD outcomes.
Introduction
Inflammatory bowel disease (IBD) comprises a group of chronic, relapsing disorders characterized by an excessive immune response that leads to intestinal injury. The main clinical forms of IBD include ulcerative colitis (UC), Crohn’s disease (CD), and indeterminate colitis (IC). 1 These conditions display a heterogeneous natural history, with some patients experiencing a relatively mild disease course while others progress to more aggressive forms requiring frequent hospitalizations, intensive medical therapy, and surgical interventions.2,3 Identifying subgroups of IBD patients at higher risk for rapid progression or complications remains a critical objective in clinical gastroenterology, as it could inform tailored treatment strategies and improve patient outcomes. Clinical markers such as early disease onset, the need for steroids at diagnosis, and the presence of perianal disease have been associated with poor prognosis; additionally, emerging genetic and serological markers are showing promise in predicting disabling disease courses.4 –9
Celiac disease (CeD), a digestive disorder triggered by an autoimmune response to gluten proteins, is primarily characterized by intestinal villous atrophy.10 –14 Beyond the direct immunogenic effect of gluten, diet has also been recognized as an important factor influencing the pathogenesis of CeD. Dietary components may modulate the composition and function of the gut microbiota, which in turn can affect intestinal permeability, mucosal immune responses, and inflammatory signaling pathways. Increasing evidence suggests that alterations in the gut microbiota and microbial metabolites may contribute to the development and persistence of immune activation in CeD, highlighting the complex interaction between genetic susceptibility, environmental triggers, and intestinal microbial ecosystems.15 –17 The diagnosis of CeD can be particularly challenging in patients already suffering from IBD because both conditions share similar clinical features, such as abdominal pain, diarrhea, and iron deficiency anemia.18 –20 Importantly, CeD and IBD are not mutually exclusive, as they share common genetic, immunological, and environmental factors that contribute to their pathogenesis.21 –23
Nationwide studies and systematic reviews emphasize a bidirectional relationship between CeD and IBD. A meta-analysis by Shah et al. 24 estimated that patients with CeD have an elevenfold increased risk of developing IBD, whereas individuals with IBD face a twofold higher risk of CeD. These findings highlight the interconnection between CeD and IBD. Several studies have reported a significant overlap in genetic risk loci between CD and CeD, suggesting that the coexistence of these disorders might predispose affected individuals to a more aggressive IBD phenotype.25 –28
The primary objective of this study was to evaluate the impact of CeD on the clinical course of IBD. Specifically, we aimed to assess whether the presence of CeD influences the IBD disease phenotype and therapeutic requirements, including the need for immunosuppressive therapy, biologic agents, and surgical interventions.
Material and methods
Study population
This retrospective, observational, longitudinal, multicenter case-control study was conducted across 22 Spanish tertiary hospitals. The study included patients diagnosed before December 31, 2020, and data collection was performed between 2023 and 2024. Cases included patients with a prior diagnosis of IBD who were subsequently diagnosed with CeD (celiac-IBD group). Controls consisted of patients with IBD without CeD (non-celiac-IBD group), matched in a 1:2 ratio by sex, IBD type, and year of diagnosis. The target population comprised adult patients with a confirmed diagnosis of IBD according to the European Crohn’s and Colitis Organization (ECCO) guidelines 29 and, for cases, a diagnosis of CeD, which was determined by a positive CeD-specific serology (including TG2, DGP, and EMA) in patients with villous atrophy (defined by a Marsh score greater than 1). In seronegative patients, HLA typing and histological findings were used to confirm or exclude CeD. 30
Inclusion criteria were: age ⩾18 years; confirmed diagnosis of IBD according to ECCO criteria; for cases, confirmed diagnosis of CeD based on serology and histology; and availability of at least 12 months of clinical follow-up. Exclusion criteria included: primary immunodeficiency disorders or common variable immunodeficiency; incomplete clinical records; and uncertain diagnosis of either IBD or CeD. Patients were consecutively identified from medical records at participating centers.
For patients in the celiac-IBD group, the index date for follow-up was defined as the time of CeD diagnosis, whereas in controls follow-up began at the time of IBD diagnosis. Patients were then followed for at least 12 months to assess disease outcomes. All patients included in the study had documented medical records in the participating hospitals and were diagnosed with both diseases before December 31, 2020.
Potential sources of bias include retrospective data collection, variability across participating centers, and the lack of standardized endoscopic assessment. To minimize confounding, cases and controls were matched by sex, type of IBD, and year of diagnosis.
Study variables and outcomes
In our study, we systematically collected variables to comprehensively assess clinical outcomes in patients with IBD, both with and without coexisting CeD. Demographic data included, age, gender, and disease duration for both IBD and CeD, as well as the presence of other immune-mediated conditions such as diabetes, hypothyroidism, vitiligo, and microscopic colitis.
For IBD-related variables, we recorded the first-degree IBD family history and also detailed the type of IBD and the extent and phenotype of intestinal involvement for CDand UC, based on the Montreal classification.2,22,27 In addition, treatment histories were compiled, including the use of corticosteroids, 5-ASA, immunomodulators (such as thiopurines and methotrexate), and biologics (including anti-TNF agents, vedolizumab, ustekinumab, among others). Changes on colitis extension in UC and disease phenotype by Montreal classification2,22,27 in CD (inflammatory, stricturing, or penetrating) including developed of perianal disease, the need for surgical interventions (abdominal and/or perianal), and the occurrence and timing of extraintestinal manifestations—including rheumatological, ocular and dermatological features—were also documented.
Regarding CeD, we collected the disease duration, age at diagnosis, first-degree family history, and predominant presenting symptoms. The diagnostic confirmation of CeD included positive CeD-specific serology (TG2, DGP, EMA), endoscopic findings, small bowel biopsy results (with histological severity noted), and HLA typing when necessary. 30 Adherence to a gluten-free diet was evaluated through clinician assessment and follow-up antibody analysis, with attention given to the diagnosis of refractory CeD.
Additionally, we recorded the development of neoplasms during the IBD course and mortality, specifying whether these events were related to the underlying diseases or to the treatments administered. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 31 A completed STROBE checklist is provided as Supplemental Material.
Statistics
All data obtained were collected and managed using REDCap electronic data capture tools hosted at Asociación Española de Gastroenterología (AEG; www.aegastro.es). We used descriptive statistics to characterize demographic and clinical characteristics. Quantitative variables were analyzed with means and standard deviations or medians and interquartile ranges. Qualitative variables were described with absolute and relative frequencies (%), along with their 95% confidence intervals. To evaluate differences between variables, the Student’s t test, or their complementary non-parametric versions were used depending on the variable distribution. To compare percentages, the chi-square test was employed. For evaluating predictive factors, both univariate and multivariate analyses with logistic regression were conducted. A p-value of less than 0.05 was considered statistically significant for all analyses. The analyses are performed using the statistical software SPSS 18.0 (IBM Corp). No formal sample size calculation was performed due to the retrospective design. All eligible patients meeting inclusion criteria during the study period were included. Missing data were handled using a complete-case analysis approach. The methodology is described in sufficient detail to allow reproducibility by other researchers.
Results
Study population and IBD phenotype in celiac-IBD cases and non celiac-IBD controls
A total of 217 patients were initially identified from database. After applying exclusion criteria, 198 patients were eligible for analysis. Finally, 66 patients with both CeD and IBD (celiac-IBD cases) and 132 IBD patients without CeD (non celiac-IBD controls) were included in the study (Figure 1).
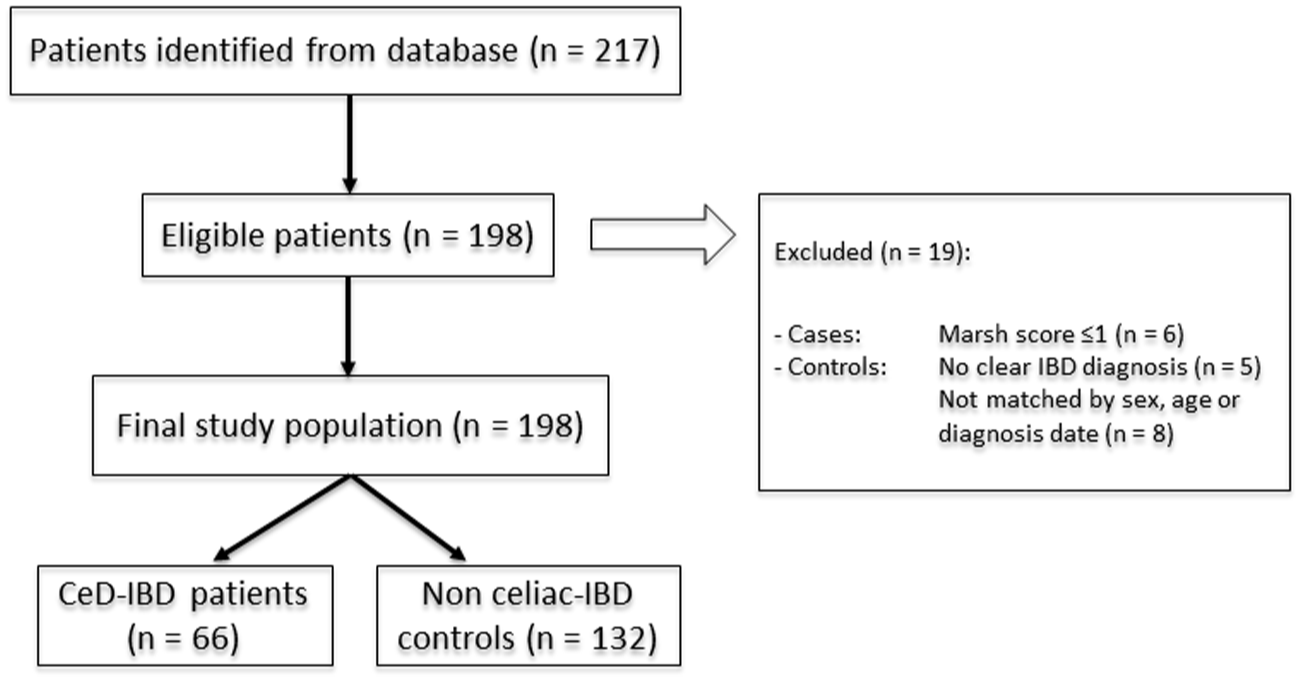
Flow diagram of patient selection and study population. The diagram illustrates the recruitment process according to STROBE guidelines. From an initial database of 217 patients, 19 were excluded based on predefined criteria: 6 cases presented a Marsh score ⩽1, 5 controls lacked a definitive IBD diagnosis, and 8 individuals could not be matched by sex, age, or diagnosis date. The final analytical cohort consisted of 198 patients, categorized into the CeD-IBD group (n = 66) and the non-celiac-IBD control group (n = 132).
The diagnosis of CeD was confirmed by both serology and biopsy results in 79% of CeD cases, whereas only four patients had a diagnosis of CeD recorded in their medical history, with an established gluten-free diet, which cannot be confirmed by reviewable laboratory results or endoscopy. The histological study was available in 93% of cases, with the most frequent histological finding being Marsh type 3 lesions (Figure 2). A majority (87.8%) of the celiac-IBD patients reported following a gluten-free diet either continuously or intermittently and no patient was diagnosed with refractory CeD.
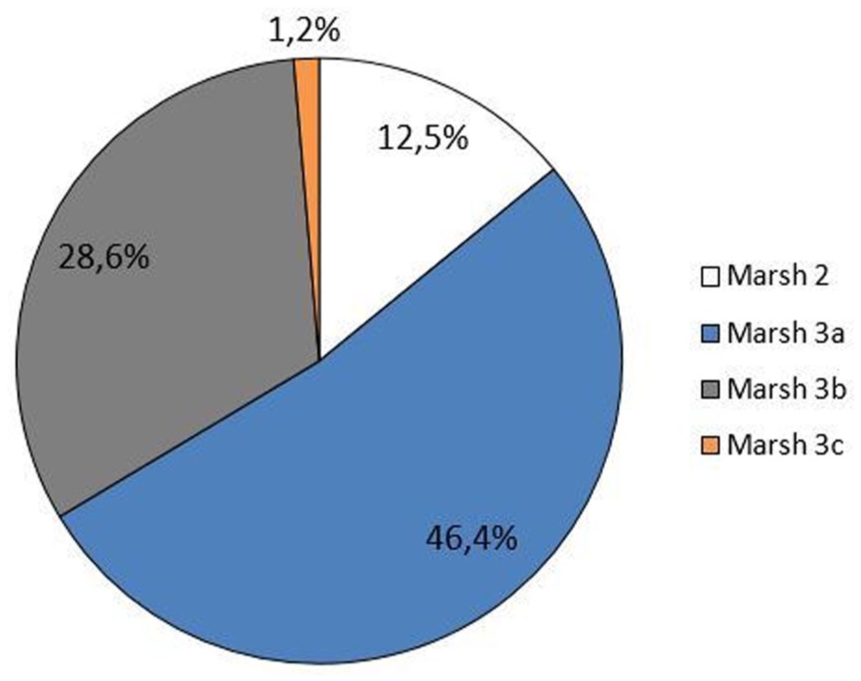
Histological findings at celiac disease diagnosis. Distribution of histological severity according to the Marsh classification in patients with concomitant IBD and CeD. Marsh type 3 was the most frequent histological finding, observed in the majority of the cases.
Matched groups of control and cases showed a mean age at IBD diagnosis of 41 (37–45) years and 43 (40–46) years on celiac-IBD and nonceliac-IBD patients, respectively (p = 0.46). In both groups, there was a numerical higher proportion of women regarding the gender distribution (59.1% and 64.4%; p = 0.34).
There were no differences in IBD duration between both groups, 11 (9–13) years and 9 (9–12) years on celiac-IBD and non-celiac-IBD patients, respectively (p = 0.81).
Overall, there were no significant differences in IBD location (UC (E1/E2/E3): 6 (20.7%)/14 (48.3%)/9 (31%) vs 19 (29.2%)/22 (33.8%)/24 (36.9%); p = 0.39); CD (L1/L2/L3/L4): 17(56.7%)/13(10%)/8(26.7%)/2(6.7%)vs 27(45%)/6(10%)/23(38.3%)/4(6.4%); p = 0.71) between celiac-IBD and non-celiac-IBD, respectively (Table 1).
Overall comparison of celiac inflammatory bowel disease and non-celiac inflammatory bowel disease.

CD, Crohn disease; IBD, inflammatory bowel disease; UC, ulcerative colitis.
Autoimmune diseases and MEIs affecting celiac-IBD cases and non celiac-IBD controls
Other autoimmune diseases developed in 6.7% (2/30) of CD patients with concomitant CeD, compared to 13.3% (8/60) in patients with CD alone (p = 0.64). In the UC cohort, 13.9% (5/36) of patients with CeD developed other autoimmune diseases, whereas 11.1% (8/72) of those without CeD experienced these conditions (p = 0.65).
In patients with CD, extraintestinal manifestations were reported in 16.7% (5/30) of those with concomitant CeD, while a rate of 18.3% (11/60) was observed in patients with CD alone (p = 0.84). Among individuals with UC, extraintestinal manifestations were present in 13.9% (5/36) of patients with CeD compared to 12.5% (9/72) in those without CeD (p = 0.83)
Outcomes of celiac-IBD cases and non celiac-IBD controls
When evaluating disease outcomes between celiac and no celiac-IBD patients, no significant global differences were observed (Figure 3).
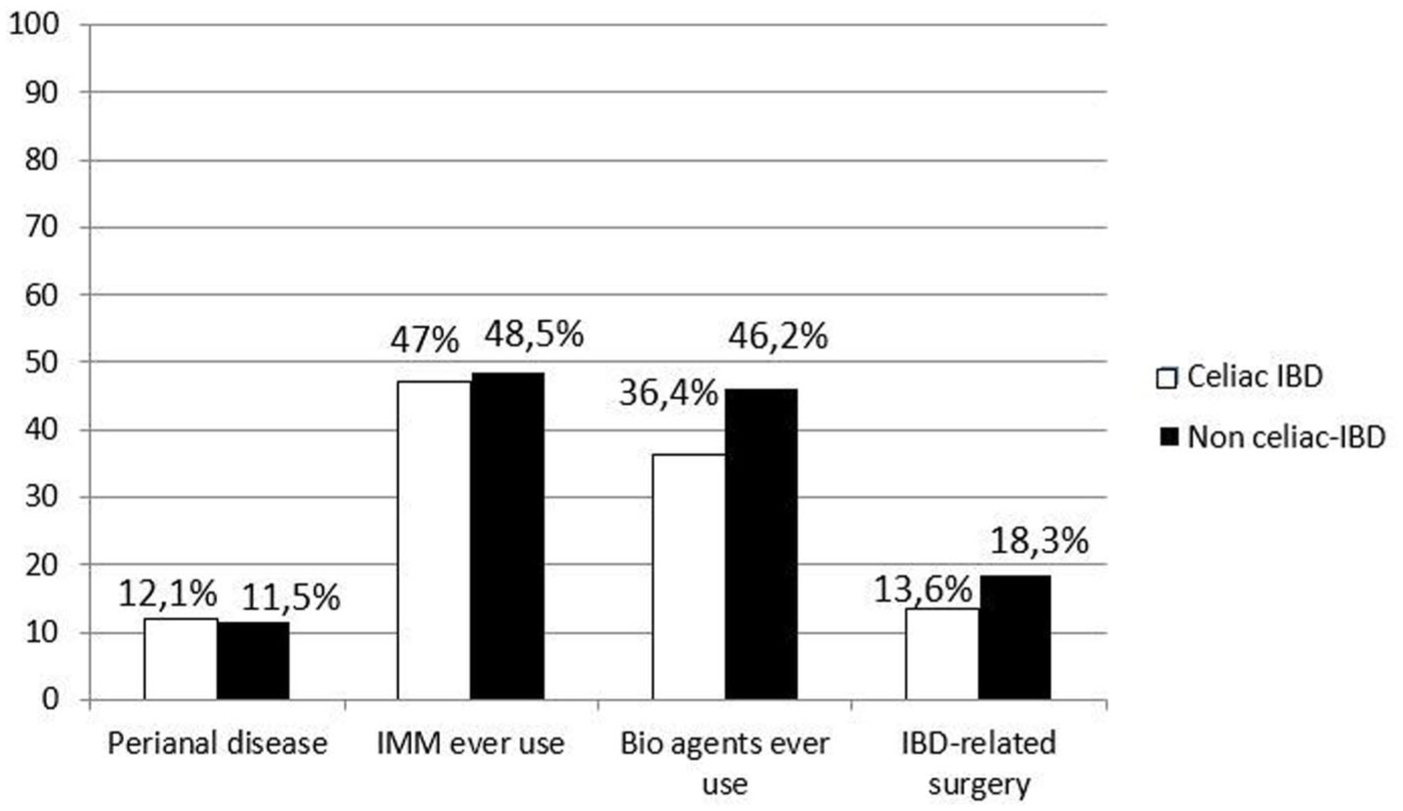
Comparative clinical outcomes between celiac-IBD cases and non-celiac-IBD controls. Forest plot displaying the OR and 95% CI for key disease outcomes, including the use of 5-ASA (mesalamine), IMM, biological agents (BIO), IBD-related surgery, and development of neoplasms. No significant differences were observed between groups across all evaluated clinical endpoints.
In UC, the numerically most frequent form of presentation was left-sided colitis (48.3%) in celiac-IBD compared to extensive colitis (33.8%) in non-celiac-IBD. In CD, the ileal involvement (L1) was the most frequent type of presentation in both celiac-IBD (56.7%) and non-celiac-IBD (45%).
During monitoring, a change of UC extent only occurred in 7% of cases in both cohorts, although a numerical increase in the change in CD phenotype occurred in non-celiac IBD (10%) compared to celiac IBD (3%), but without significant differences (p = 0.26). This lack of distinctiveness was consistent across all IBD subtypes, including UC and CD (Table 2). Particularly, the prevalence of perianal disease did not differ significantly between groups (OR 1.1, 95% CI: 0.7–1.8). Similarly, the use of mesalamine (OR 0.9, 95% CI: 0.6–1.5), exposure to immunomodulators (IMM; OR 1.2, 95% CI: 0.8–1.9), and treatment with biological agents (BIO; OR 1.0, 95% CI: 0.7–1.6) showed no significantly differences (Figure 2).
Comparison of celiac inflammatory bowel disease and non celiac inflammatory bowel disease by IBD type.
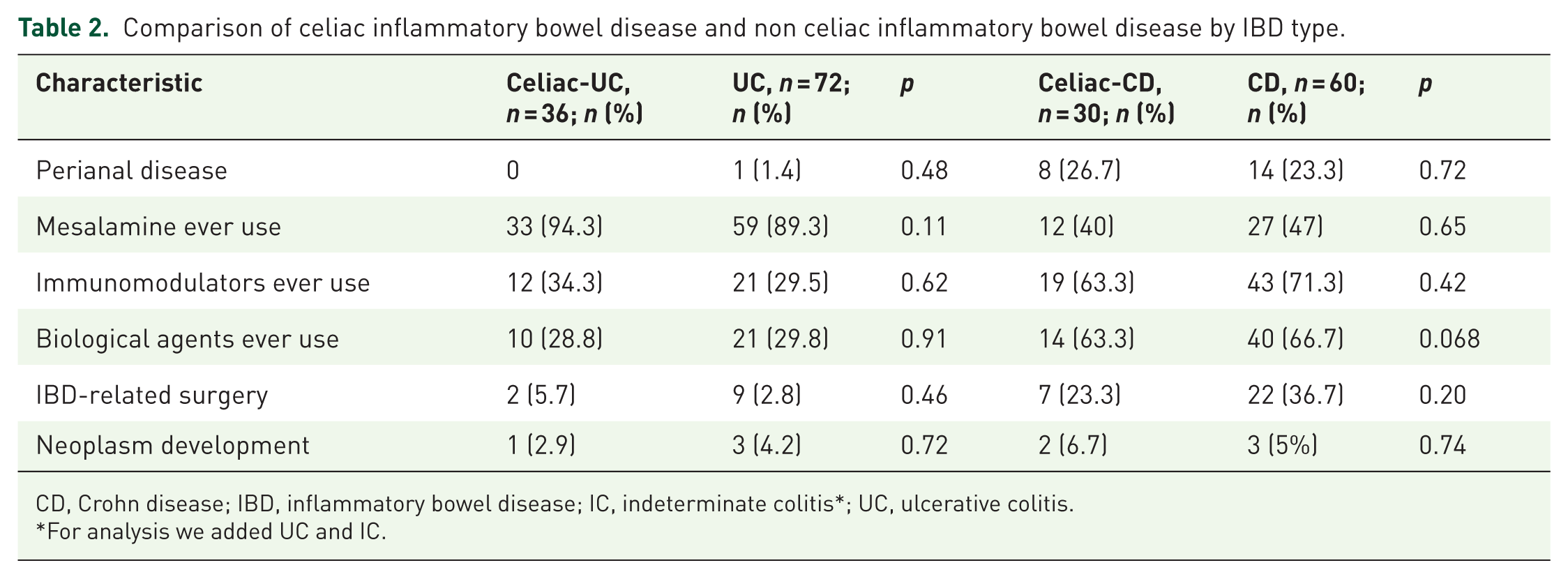
CD, Crohn disease; IBD, inflammatory bowel disease; IC, indeterminate colitis*; UC, ulcerative colitis.
For analysis we added UC and IC.
Moreover, the need for surgical interventions related to IBD was also comparable between cohorts (OR 0.9, 95% CI: 0.5–1.6). In patients with CD, surgery was required in 23.3% of those with concomitant CeD (7 out of 30) compared to 36.7% of those with CD alone (22 out of 60) (p = 0.20), while in the UC cohort, surgery was needed in 5.6% of patients with CeD (2 out of 36) versus 2.8% in those without it (2 out of 72) (p = 0.83).
In rather a similar way, the occurrence of neoplasms during follow-up was similar in both cohorts (OR 1.0, 95% CI: 0.5–2.1; Figure 2). In patients with CD, neoplasia developed during the study follow-up in 6.7% (2/30) of those with concomitant CeD compared to 5.0% (3/60) in those with CD alone (p = 0.74), while in the UC subgroup, neoplasia was observed in 2.8% (1/36) of patients with CeD versus 4.2% (3/72) in patients without CeD (p = 0.72).
Furthermore, no mortality was reported in either cohort throughout the study period follow-up.
Discussion
Our results did not show significant differences in key disease outcomes—including the need for immunomodulators, biologicals, IBD-related surgery, hospitalizations, development of perianal disease, or neoplasms—between IBD patients with and without coexisting CeD.
These findings contrast with prior studies suggesting a more aggressive IBD phenotype in patients with concurrent CeD. Tse et al. 24 observed that such patients had higher rates of extensive UC, increased incidence of primary sclerosing cholangitis, and a greater number of hospitalizations. Kori et al. 26 also reported, using a large Israeli database, that CeD and celiac autoimmunity were more prevalent among IBD patients, particularly children and those with CD, and were associated with earlier escalation to biologic therapies. However, our findings, derived from a Mediterranean cohort with rigorous case-control matching, did not replicate these results, suggesting possible regional or methodological differences.
A strong epidemiological link between CeD and IBD has been repeatedly demonstrated. Shah et al. 24 reported an elevenfold increased risk of IBD in patients with CeD and a twofold increase of CeD among those with IBD. Pinto-Sanchez et al. 27 confirmed this bidirectional association in a meta-analysis including over 60 studies. While these studies provide valuable prevalence data, neither explored the impact of CeD on the natural history or outcomes of IBD. Our results suggest that co-diagnosis alone may not translate into a more severe disease course. Our study adds to the literature by specifically evaluating clinical outcomes rather than only epidemiological associations.
Oxford et al. 2 found that patients with UC and CeD were more likely to present with pancolitis and showed a trend toward increased use of immunosuppressants, while CD behavior appeared unaffected. This partially supports our findings, in which the therapeutic burden—measured by the use of immunomodulators and biologics—was similar between groups, regardless of IBD subtype. Moreover, Zhang et al. 8 showed that serological markers such as anti-Saccharomyces cerevisiae antibodies are associated with more aggressive phenotypes in CD, but whether these profiles are more common in patients with dual CeD-IBD diagnoses remains unclear and warrants further study.
From an immunological perspective, the coexistence of CeD and other autoimmune diseases has been widely reported. Yılmaz Çakmak et al. 32 found that Behçet’s syndrome patients with CeD had significantly higher rates of IBD, fibromyalgia, and osteoporosis, supporting a shared inflammatory background. Similarly, Cottone et al. 21 and Kocsis et al. 22 reported familial clustering of IBD in CeD patients, suggesting possible heritable immune dysregulation. This clustering may reflect shared environmental exposures, microbiome alterations, or polygenic risk.
From a mechanistic perspective, several pathways may link CeD and IBD. Both conditions are characterized by dysregulated mucosal immune responses, involving the activation of pro-inflammatory signaling pathways such as nuclear factor-κB (NF-κB), a key regulator of cytokine production and intestinal inflammation. In addition, accumulating evidence suggests that alterations in the gut microbiota may contribute to the pathogenesis of both disorders. Changes in microbial composition and metabolic activity can disrupt intestinal immune homeostasis and barrier function. 33 In particular, microbiota-derived metabolites such as short-chain fatty acids (SCFAs), including butyrate, propionate, and acetate, have been shown to exert anti-inflammatory effects through modulation of epithelial integrity and regulatory immune pathways. 34 Therefore, disruption of these microbiota-dependent mechanisms may represent a biologically plausible link between CeD and IBD, although the clinical implications of these interactions remain incompletely understood.
We also considered the risk of neoplasia. In our cohort, no differences were observed in cancer incidence between groups. Although CeD has been associated with small bowel lymphoma and small bowel cancers, 35 our findings align with Peters et al., who demonstrated that while CeD increases overall mortality, cancer-specific mortality is modest and influenced by factors such as disease control and nutritional status. 35 In the context of IBD, the risk of malignancy may be more strongly associated with chronic inflammation and immunosuppression than with comorbid CeD.3 –5
A crucial factor that may influence the interaction between CeD and IBD is adherence to a gluten-free diet. Although adherence to a gluten-free diet is a key determinant of disease control in CeD, our study could not assess gluten-free diet adherence in a standardized and quantitative manner due to its retrospective design. Dietary adherence was evaluated qualitatively based on clinical assessment and serological follow-up; however, validated dietary assessment tools were not consistently available across centers. Therefore, this variable was not included in the analytical models, which represents an inherent limitation of real-world retrospective studies. Previous research has shown that strict adherence to a gluten-free diet improves clinical and histological outcomes in CeD and may reduce systemic inflammation, potentially attenuating any impact on IBD.19,20 Furthermore, patient knowledge and health literacy regarding CeD and IBD have been shown to influence adherence and clinical outcomes.36 –38 Therefore, patient education should be considered a key pillar in the management of both conditions.
We acknowledge several limitations. First, the retrospective design restricts causal inference. 39 Second, the follow-up period of 1 year provides only a limited snapshot of the clinical course of IBD, which is a lifelong, chronic condition. 40 Therefore, our findings mainly reflect short-term outcomes and early disease behavior rather than long-term disease evolution. Previous studies exploring the relationship between CeD and IBD have reported longer observation periods; however, many of them have primarily focused on disease prevalence and epidemiological associations rather than on the impact of CeD on IBD outcomes over time. In addition, data on endoscopic severity, mucosal healing, and specific treatment indications were not available, which represents a major limitation, as these are key markers of disease activity and prognosis in IBD. The absence of standardized endoscopic assessment across centers reflects the real-world nature of the study but limits the ability to evaluate subclinical disease activity. Adherence to a gluten-free diet was assessed qualitatively, and anthropometric data such as weight, height, and body mass index were not consistently available and therefore could not be included in the analysis.
However, our study also presents notable strengths, including its real-world design, the involvement of multiple hospitals, and matched controls, which helped limit confounding related to the natural course of IBD.
In conclusion, our findings suggest that the coexistence of CeD and IBD may not be associated with a more aggressive clinical course. However, given the retrospective design and limited sample size, these results should be interpreted with caution and considered hypothesis-generating. Prospective studies are warranted to confirm these observations.
Supplemental Material
sj-doc-1-tag-10.1177_17562848261452511 – Supplemental material for Impact of celiac disease on the clinical course of inflammatory bowel disease: CEL_EII study by GETECCU
Supplemental material, sj-doc-1-tag-10.1177_17562848261452511 for Impact of celiac disease on the clinical course of inflammatory bowel disease: CEL_EII study by GETECCU by Inmaculada Alonso-Abreu, Laura Ramos, Alejandro Hernandez-Camba, Carmen Yagüe-Caballero, Raquel Vicente Lidón, Carlos Taxonera, Miguel A. García-Brenes, Javier P. Gisbert, Maria Chaparro, Lucia Madero Velázquez, Marta Carrillo-Palau, Laura Arranz, Beatriz Castro Senosiain, Irene García de la Filia Molina, María Rojas-Feria, Francisco López Romero-Salazar, Iria Bastón-Rey, María Sánchez-Azofra, Sabino Riestra, Pablo Pérez-Galindo, Silvia Patricia Ortega Moya, Eduard Brunet-Mas, Patricia Sanz Segura, Antonio M. Caballero Mateos, Margalida Calafat, Belén Botella Mateu, Noemí Manceñido Marcos, Iago Rodríguez-Lago, Cristina Suarez Ferrer and Ana Gutiérrez in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
None.
Declarations
ORCID iDs
Artificial intelligence statement
The authors used ChatGPT (OpenAI) to assist with language editing and manuscript refinement. The authors take full responsibility for the content of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.