
Abstract
Evaluation of the small intestine is technically difficult because of its length and anatomy. Capsule endoscopy and device-assisted enteroscopy (DAE) have expanded diagnostic and therapeutic options in recent years. This narrative review summarizes the current indications, therapeutic procedures, safety, and role of enteroscopy compared with other small bowel imaging methods. A literature search was performed in the MEDLINE database covering publications from February 2001 to February 2025, using predefined inclusion and exclusion criteria. The main indications include small intestinal bleeding, inflammatory bowel diseases such as ulcerative colitis and Crohn’s disease, celiac disease, and tumors of the small intestine. Enteroscopy allows identification of bleeding sources, assessment of disease extent and complications, and detection of neoplastic lesions. Capsule endoscopy is usually the first test performed because it is less invasive. However, DAE allows tissue sampling and therapeutic intervention if abnormalities are detected. It can also be useful in cases where non-invasive imaging is inconclusive. The main therapeutic procedures include hemostasis, balloon dilation of short symptomatic strictures, polypectomy, and foreign body removal. Balloon dilation is recommended for selected benign strictures and may reduce the need for surgery. Enteroscopy is considered a safe procedure. The overall risk of complications ranges from 0.4% to 5.5% for both double-balloon and single-balloon enteroscopy, with no significant difference between them. Major adverse events, including perforation, pancreatitis, and bleeding, are uncommon and generally do not exceed 3%. The risk is higher in therapeutic interventions. Elderly patients are more likely to experience sedation-related side effects, including aspiration and hypoxia. Despite its advantages, enteroscopy remains technically demanding and mostly available in specialized centers. Further standardization and wider availability are needed.
Keywords
Introduction
The small bowel diseases represent a significant diagnostic and therapeutic challenge for clinicians. The introduction of capsule endoscopy in 2001 was a breakthrough in this field. The examination is performed using a capsule containing a wireless digital camera, a light-emitting diode lamp and a radio transmitter. The patient swallows the capsule, which passes through the entire digestive tract, like a bite of food. During the examination, the camera records the images captured inside the digestive tract. The obtained pictures are sent to an external receiver, which the patient carries during the whole examination. Specific software is necessary to analyze and evaluate the taken images. Unfortunately, this method does not allow for interventional therapy and the collection of tissue samples. 1
In 2001, double-balloon enteroscopy was described by Yamamoto et al., 2 and in the following years, this method became commercially available, allowing minor therapeutic procedures in addition to small bowel visualization.
The balloon-ended enteroscope, together with a tube equipped with a second balloon, can be inserted in two ways—by the oral or rectal route. The examination itself involves repeatedly inflating and deflating the balloons and moving the enteroscope through the small intestine, which prevents the formation of bowel loops. In 2007 and 2008, single-balloon and spiral enteroscopy methods came into use. 3 The spiral enteroscope additionally has a the spiral fold that helps with the threading of the small intestine and thus moving forward. In 2019, a new version of the spiral enteroscope was released, which is motor-driven and features direct optics. 4
This review’s unique contribution lies in bridging the gap between non-invasive diagnostic mapping (using video capsule endoscopy (VCE), magnetic resonance enterography (MRE), and intestinal ultrasound (US)) and cutting-edge endoscopic interventions, offering clinicians a modern roadmap for when to observe, when to image, and when to intervene. Its goal is to summarize the evolving diagnostic role of enteroscopy, assess the technical success and complication profiles of modern therapeutic enteroscopy, and compare the diagnostic yield of enteroscopy against cross-sectional radiological imaging to define their complementary roles in contemporary clinical pathways.
Currently, one of the most common indications for referring a patient for enteroscopy is the diagnosis of obscure, overt, or occult bleeding. Obscure gastrointestinal bleeding (OGIB) is bleeding that recurs or does not stop, with no defined cause, despite a diagnostic workup including esophagogastroduodenoscopy, ileocolonoscopy, radiologic studies (small bowel passage, classic enteroclysis), arteriography, and scintigraphy. 5
Enteroscopy also provides the opportunity to collect samples from the small intestine for pathologic examination in cases of suspected Crohn’s disease (CD), small bowel tumors, hereditary polyposis, and celiac disease (CD). 6
Enteroscopy may be performed in patients with unexplained anemia, chronic abdominal pain, or diarrhea. 7 However, according to the guidelines of the British Society of Gastroenterology, in those cases, capsule endoscopy should be performed first, and only when small intestine changes are identified, enteroscopy is recommended.8,9
This approach is preferred due to the less invasive nature of capsule endoscopy compared to enteroscopy. 9 In addition, the results of capsule endoscopy allow for more efficient localization of potential pathologies, which helps in guiding the enteroscopy.
Studies describing the results of enteroscopic examinations performed in Canada, Korea, and the United Kingdom indicated that vascular lesions (25.9%–43.5%), inflammatory lesions (42.7%), neoplastic lesions (0.9%–21.7%), ulcerations (36.1%), and polypoid lesions (5%–36.1%) were the most frequent findings.10–12 In addition, single cases of intestinal tuberculosis, lymphoma, blue rubber bleb nevus syndrome, or the presence of human roundworms in the intestinal tract lumen were detected.7,10,12
Methodology
Search for the literature has been performed across the MEDLINE database using search criteria such as (“Crohn’s disease” OR “Ulcerative colitis” OR “Celiac disease” OR “Peutz-Jeghers syndrome” OR “Familial adenomatous polyposis” OR “ischemic enteritis” OR “small bowel tumors” OR “primary sclerosing cholangitis” OR “surgically altered anatomy” OR “biliary pathologies”) AND (“enteroscopy” OR “device-assisted enteroscopy” OR “capsule endoscopy” OR “interventional” OR “guidelines” OR “bleeding” OR “stricture” OR “foreign body” OR “polyps” OR “ERCP” OR “endoscopic retrograde cholangiopancreatography” OR “Roux-en-Y” OR “Billroth II” OR “Whipple”). The earliest publication referenced is from February 2001 and the latest—from January 2026. Inclusion criteria were peer-reviewed original research, systematic and narrative reviews, meta-analyses, clinical trial protocols, case reports, and official clinical guidelines. Studies using endo-anal or endoscopic ultrasonography, in vitro, ex vivo, and animal studies were excluded.
Indications for enteroscopy
Small intestinal bleeding
Small bowel bleeding has a range of many different causes. In a study analyzing the results of capsule endoscopy performed in 385 patients from different age groups with OGIB, distinct age-related differences in etiology were observed. Patients aged 65 and above most commonly presented with vascular anomalies (54.35%), small intestinal ulcers (13.04%), and tumors (11.96%). In individuals aged 41–64 years, vascular anomalies (34.82%) and tumors (31.25%) occurred with comparable frequency, whereas in patients under 40 years, CD (34.55%) was the leading diagnosis, followed by tumors (23.46%) and non-specific enteritis (10.91%). 13 Although these results indicate age-related differences in etiology, they are based on a single cohort of patients with OGIB examined exclusively by capsule endoscopy. Additionally, the lack of comparison with other diagnostic methods limits the assessment of the true diagnostic accuracy across age groups.
In patients with suspected small bowel bleeding of unknown origin, capsule endoscopy is recommended as the first-line diagnostic method. Although this approach is supported by its non-invasive character, it does not allow therapeutic intervention. Double-balloon enteroscopy (DBE) allows for bleeding control and in some cases, tattooing, which determines the bleeding location for subsequent surgery. The diagnostic yield (defined as the percentage of patients with overt bleeding detected with enteroscopy in the total cohort size) of this procedure is estimated at 47%–75%, depending on the type of lesion. In a study evaluating 381 DBE procedures, identified causes included vascular lesions (47%), angiodysplasia (41.9%), ulcers or erosions (9.9%), as well as Dieulafoy lesions, intestinal varices, tumors, polyps, diverticula and vascular malformations.14,15
In cases of occult bleeding and iron deficiency anemia, the diagnostic efficacy of enteroscopy (its ability to correctly identify the cause of the condition under ideal and controlled circumstances) ranges from 52.4% to 75.6%. 14 Efficacy is higher, when it is performed after positive capsule endoscopy. 15 Across studies, the most frequently detected lesions in occult bleeding and iron deficiency anemia are angiodysplasias (Figure 1), erosions, ulcers, and tumors.16–18 Vascular lesions are particularly often seen in the elderly. Among 125 patients diagnosed with angioectasias on capsule endoscopy, the median age was 72.7 years. 19 Therapeutic decisions should therefore be individualized, taking into account anemia severity, bleeding recurrence, comorbid conditions, and overall procedural risk. Endoscopic treatment may be indicated in selected cases, whereas conservative management including oral or intravenous iron supplementation remains appropriate for others. 9
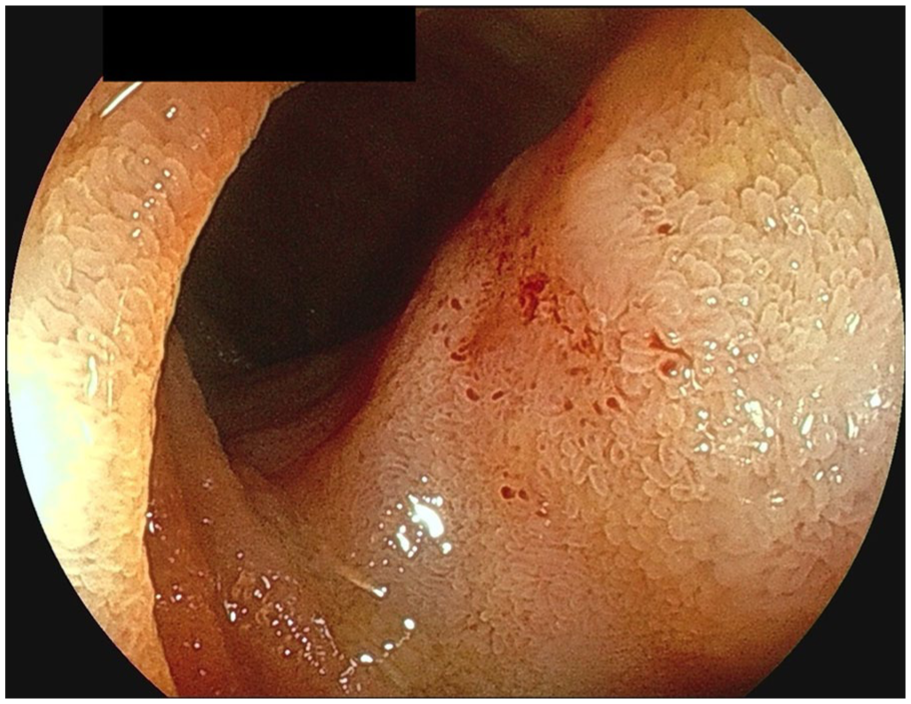
Ileal edema and vascular ectasia.
Inflammatory bowel diseases: Ulcerative colitis and CD
Crohn’s disease usually involves the terminal ileum and colon, but may be limited to the small intestine at the time of diagnosis, primarily in young people. 20 According to current European Society of Gastrointestinal Endoscopy (ESGE) recommendations, ileocolonoscopy should be performed as the first-line investigation in patients with suspected CD. If ileocolonoscopy is noncontributory and small-bowel involvement is suspected based on cross-sectional imaging or small-bowel capsule endoscopy, device-assisted enteroscopy (DAE) with targeted small-bowel biopsies is recommended to confirm the diagnosis. 21 In such cases, enteroscopy is the preferred diagnostic test, due to the higher diagnostic efficacy than radiological techniques such as: small bowel barium contrast, computed tomography enterography (CTE), and MRE 14 (Table 1).
Sensitivity and specificity of the methods used in the inflammatory bowel diseases diagnostics.

CTE involves the use of contrast-enhanced computed tomography (CT) scans while MRE provides detailed soft tissue imaging without radiation exposure, although at a higher cost. Compared to these methods, capsule endoscopy has the highest diagnostic sensitivity. However it can be expensive, particularly if capsule retention occurs. While CTE and MRE have slightly higher specificity (Table 1), capsule endoscopy allows for a direct mucosal examination, identifying subtle lesions such as angiodysplasias or erosions that may be missed by radiological techniques.
In inflammatory bowel diseases (IBD), during enteroscopy, small bowel lesions such as erythema, erosions, ulcers, linear ulcers, and stenosis can be visualized and sampled 28 (Figure 2). Sampling helps distinguish CD from ulcerative colitis (UC) by identifying features like granulomas or metaplasia, and rules out alternative diagnoses such as infections or non-steroidal anti-inflammatory drugs (NSAID)-induced enteropathy. 29 It also differentiates inflammatory from neoplastic changes, especially in long-standing disease, and is key for dysplasia surveillance in high-risk patients, like those with primary sclerosing cholangitis (PSC).29,30 Biopsies of strictures are essential to exclude malignancy and guide management, particularly in UC and CD. 30

Ileal ulcer in Crohn’s disease–Ileal ulcer.
Symptomatic intestinal stenosis develops in up to more than one-third of Crohn’s syndrome patients. 31 In these cases, endoscopic treatment preserves valuable absorptive segments of the small intestine, as opposed to surgery. Surgical bowel dilation is only performed in specific situations, as multiple operations carry the risk of long-term complications such as incisional hernias and adhesions and even short bowel syndrome. Nevertheless, surgery often provides a more durable response with a longer symptom-free period. Surgical treatment is usually considered for complications such as fistulas or abscesses, and in patients with an aggressive disease course, multiple previous operations, or coexisting strictures, as it is associated with a lower risk of subsequent procedures. 32 In a study described by Lan et al., 33 the effectiveness of endoscopic balloon dilation (EBD) was characterized by the high initial technical success rate, defined as successful passage of the endoscope without resistance after dilation (86.3%). However, it was associated with a high incidence of subsequent salvage surgery (44.4%) and a shorter surgery-free survival time: 5.4 years on average. In contrast, ileocecal resection was considered a more durable option. It offered a significantly longer surgery-free survival time (average of 11.1 years) and a lower rate of secondary surgery (21.7%). 33 However, the study was limited by inevitable selection bias, as the choice between EBD and surgery was made at the discretion of individual physicians without a standardized treatment algorithm, despite subgroup analyses performed to reduce its impact.
Celiac disease
Capsule endoscopy is recommended in the guidelines of the ESGE in cases of an equivocal diagnosis of CD. 21 This includes mainly the two groups of patients: those with positive IgA tTG and/or EmA and normal duodenal histology, and those with histologically detected villous atrophy and negative CD serology. 21 In such cases, the detection of Kerckring’s folds reduction or smoothing, scalloping of duodenal folds and a mosaic pattern with nodularity with capsule endoscopy may support the diagnosis. 34
In uncomplicated CD, enteroscopy may reveal typical atrophic features, including reduced number of duodenal folds, mucosal fissures, prominent submucosal vessels, mosaicism, and erosions. 35 However, in this setting, enteroscopy rarely changes management and is therefore not routinely indicated.
Enteroscopy becomes particularly relevant in suspected complicated CD, especially in patients unresponsive to 6–12 months strict gluten-free diet, with alarm symptoms or iron deficiency anemia.14,21 Under these circumstances, VCE allows assessment of the extent of lesions, whereas DAE enables histological confirmation and therapeutic interventions, directly further management (Figure 3).
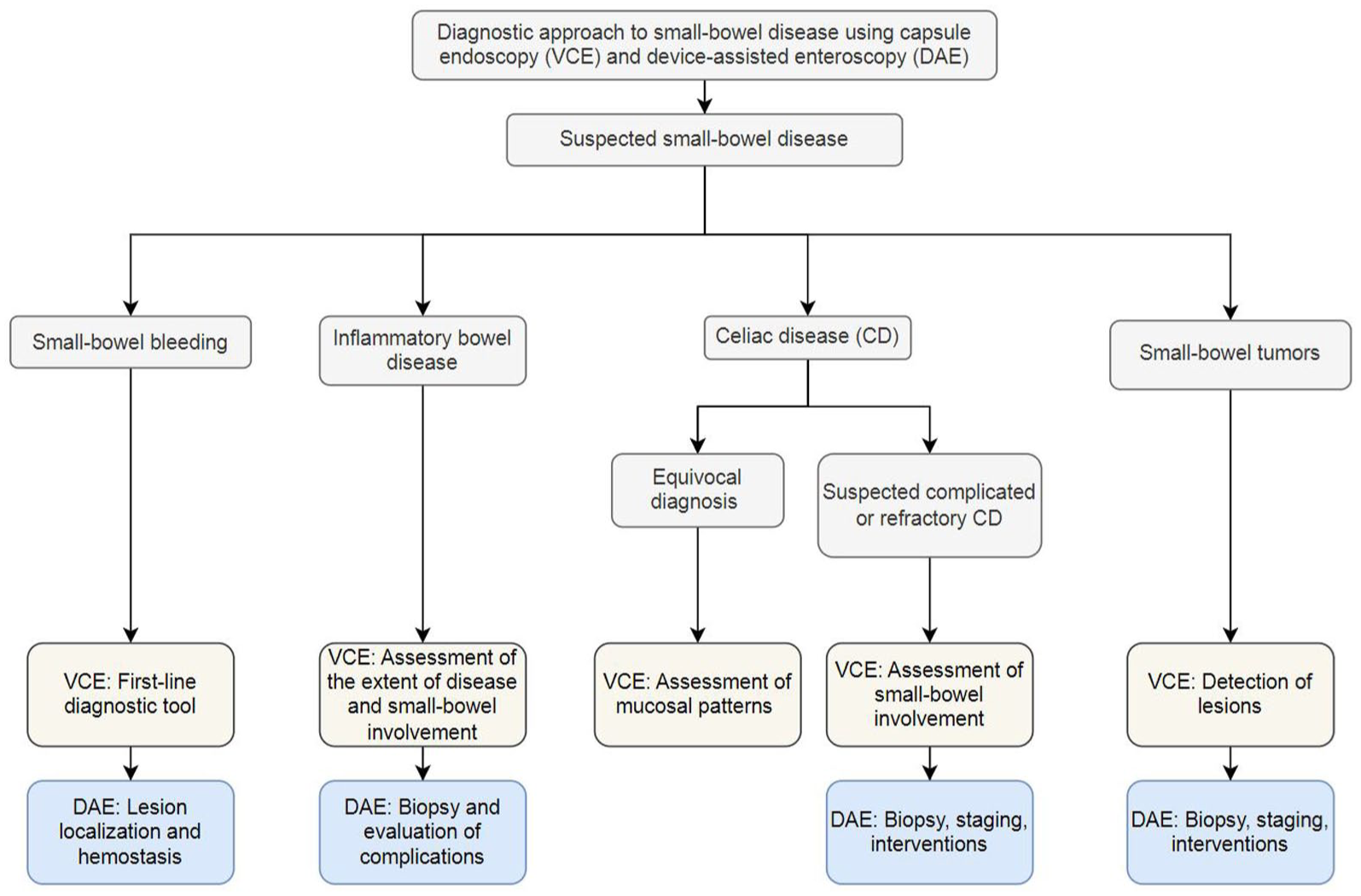
Role of VCE and DAE in small-bowel diseases.
Severe forms of CD include pre-malignant complications such as refractory celiac disease (RCD) type 1 and type 2, ulcerative jejunitis, and collagenous enteritis. In addition, CD neoplastic complications include: enteropathy-associated T-cell lymphoma, abdominal B-cell lymphoma, and small bowel adenocarcinoma.36,37 RCD is diagnosed after exclusion of ongoing gluten exposure and confirmation of persistent villous atrophy on small bowel biopsy. 38 In enteroscopic examination, macroscopic features of villous atrophy and ulceration are often found in both RCD types. A characteristic difference is the more frequent occurrence of large ulcers (>1 cm) and ulcerative jejunitis in patients with type 2 RCD. In addition, in type 2 RCD, lesions suggestive of malignant complications, such as ulcerative mucosal nodules, obstructing masses, or strictures, may appear. 39 Identification of such lesions directly impacts management, prompting histological verification, staging procedures, and referral for oncologic treatment or surgical resection when indicated.
Ulcerative jejunitis, typically associated with type 2 RCD, is characterized by recurrent malabsorption and multiple jejunal ulcerations despite a gluten-free diet. 40 In a group of patients with complicated CD (included patients with diagnosed/suspected or refractory CD with indications other than suspected small bowel bleeding), atrophy was the most common finding, detected in 78.7% with VCE and 65.5% with double-balloon enteroscopy, followed by ulcerations (9.8% with VCE, 15% with DBE) and aphthae (5.1% with VCE, 7.9% with DBE). 41 These findings illustrate the complementary roles of VCE (pan-enteric assessment) and DAE (histological confirmation and intervention).
Overall, current best-practice guidelines position VCE and/or DAE as problem-solving tools in equivocal or complicated CD, particularly when results are expected to alter clinical management (Figure 3). 42 The presence of unexplained alarm symptoms, such as anemia, unintentional weight loss, lack of response to a gluten-free diet, dysphagia, rectal bleeding, or recurrent vomiting warrants enteroscopic evaluation. 43
Tumors of the small intestine
Adenocarcinomas and neuroendocrine tumors account for approximately 40% of small intestinal malignancies each. The remaining are lymphomas (17%), gastrointestinal stromal tumors, and sarcomas (8%).44–46 Malignant lesions in the small intestine can also include metastases, such as melanoma metastasis, as illustrated in Figure 4. Both double-balloon enteroscopy and the capsule method are more effective in detecting malignant lesions than contrast CT (sensitivity 89% vs 79.6%–83.3% vs 40.4%).14,47–49
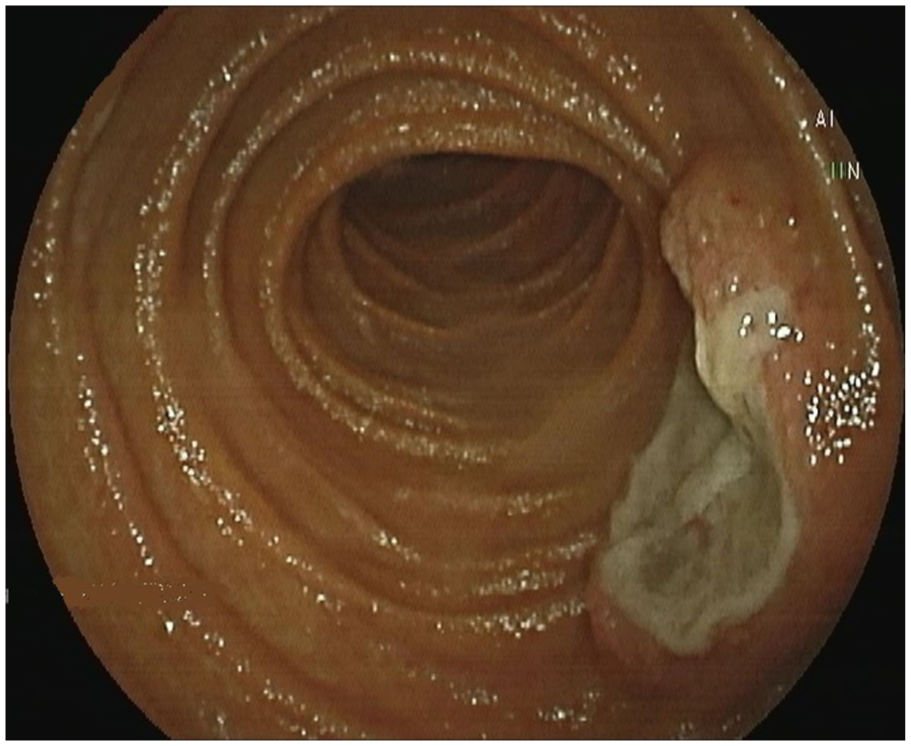
Melanoma metastasis in the jejunum.
Enteroscopy is used to determine the exact location of the lesion, mark it with a tattoo, and take a biopsy sample. Tattooing the lesion makes it easier to monitor it during subsequent examinations and localize at surgery. 6 With enteroscopy, it is also possible to coagulate the bleeding tumor and introduce the palliative treatment, like stenting or balloon dilatation for accompanying stenosis. Sulbaran et al. in a meta-analysis and systematic review, including 15 studies involving 821 patients, showed a high overall incidence of small bowel tumors identified by DAE (single-balloon, double-balloon, and spiral methods). The study was conducted in patients with OGIB, gastrointestinal polyposis, unexplained anemia, chronic abdominal pain, suspected abdominal masses, and diarrhea, achieving a specificity in diagnosing small bowel polyps and tumors as high, as 97% and a sensitivity of 89%. 47 Comparisons were also made between device-assisted and capsule endoscopy methods, and interestingly, false-negative results occurred with both types of procedures—in 16 patients, capsule method missed lesions that were picked up by one of the device-assisted methods, and in 20 cases, it was the VCE that picked up pathology that was not found by DAE. 48
Other diseases
Enteroscopy was also used for the diagnosis of other small bowel manifestations of many diseases, such as tuberculosis, Whipple’s disease, NSAID enteropathy, ischemic enteritis, radiation-induced inflammation, graft-versus-host disease with small bowel involvement, and the presence of Meckel’s diverticulum.14,50 Endoscopy is the gold standard for diagnosing ischemic enteritis, visualizing the mucosal changes, which include: mucosal edema, erosions, ulcers, and stenosis. Biopsy results, as ischemic inflammation with ulcerations, fibrosis, and hemosiderin-loaded macrophages throughout the intestinal thickness, are helpful in confirming the diagnosis and ruling out other pathologies. 51 The depth of the ulceration (grade 2 or 3) and the base of the ulceration lining need to be reported by the pathologist. 52 Differential diagnosis includes CD, Behçet disease (BD), intestinal tuberculosis, ulcers caused by NSAIDs and malignancies. BD is a chronic vasculitis of unknown etiology that can affect almost all organs. It typically manifests with recurrent, painful oral and genital ulcerations, and skin lesions. Macroscopically, ulcerations are mostly seen inside the mouth, on the genital organs and in the gastrointestinal tract, especially in the ileocecal region and ascending colon. 53
Enteroscopic therapeutic procedures
Hemostasis
The most common techniques used in hemostasis are: argon plasma coagulation, thermocoagulation, hemostatic clips, and—much less frequently—topical hemostatic agents, which may be applied at enteroscopy.11,54 The latter—such as Hemospray (TC-325) and PuraStat (TDM-621), based on inorganic powder (Hemospray) or self-aggregating peptides (PuraStat), applied as a spray or pre-filled syringe, respectively—achieve immediate hemostasis in 93% of cases. In comparison, with hemostatic clips and thermocoagulation hemostasis is obtained in 98.5% and 94.5% for, respectively.55–58 Argon plasma coagulation is a non-contact method of tissue thermocoagulation using argon gas as a current conductor. The lack of direct contact with the tissue prevents tissue adhesion to the instrument. The classical contact thermocoagulation achieves a hemostatic effect by direct application of the current source, so heat can spread deeply into the tissue even through already coagulated layers. Argon coagulation, on the other hand, conducts current from a distance of 2–8 mm along tissues with the lowest electrical resistance, which means that once coagulated tissues are insensitive to reapplication and therefore, the risk of perforation is low. 54 Hemostatic clips allow for immediate hemostasis due to mechanical compression of the bleeding vessel, but are connected to the lower primary hemostasis rate than thermocoagulation (88.7% vs 94.5%). On the other hand, clips treatment has a lower risk of rebleeding than thermocoagulation (7.1% vs 13.3%). 57
In patients with acute upper gastrointestinal bleeding, the Glasgow-Blatchford (GBS) score is used to assess the patient’s bleeding risk before endoscopy—patients with a GBS score ⩽1 have a very low risk of rebleeding and can be referred for planned endoscopy. The scale takes into consideration variables such as: blood urea, hemoglobin, systolic blood pressure, heart rate over 100, melena, liver disease, syncope, and heart failure. Patients requiring emergency endoscopy (<24 h) should undergo it only after hemodynamic resuscitation. 59
The favorable maneuverability of balloon-assisted enteroscopy within the distal small bowel readily accommodates therapeutic hemostasis, notably via clipping and argon plasma coagulation. Regarding procedural safety, Hong et al. reviewed 1108 balloon-assisted enteroscopy (BAE) cases and observed a low adverse event rate of 1.1%. The most frequently encountered adverse events included hemorrhage (n = 4), perforation (n = 4), acute pancreatitis (n = 2), and post-polypectomy syndrome (n = 2). 60
Management of small intestinal vascular lesions correlates directly with the six-tiered Yano-Yamamoto classification. 61 Capillary or venous angioectasias (Types 1a/1b) are effectively managed with electrocautery, whereas arterial Dieulafoy’s-like lesions (Types 2a/2b) and arteriovenous malformations (Type 3) typically necessitate mechanical hemostasis via hemoclip placement. Large-caliber lesions unamenable to endoscopic therapy require escalation to transcatheter arterial embolization (TAE) or surgical resection. In such instances, BAE permits preoperative localization of complex pathology (e.g., neoplasms, Meckel’s diverticula) via India ink tattooing, while endoclips can function as radiopaque markers for TAE. For ulcerative bleeding, argon plasma coagulation is preferred for diffuse oozing, and endoclips are indicated for visible vessels. 62 Hemorrhagic lesions such as small hemangiomas or polyps inherent to Peutz-Jeghers syndrome (PJS) are definitively treated with polypectomy. 63
At the same time, bleeding is the most common complication of therapeutic enteroscopy, with the frequency of 3% in case of balloon dilation of strictures and 2.58% for foreign body removal, while in diagnostic enteroscopy, the incidence is up to 0.1%.64–67 Chance of rebleeding itself is higher in patients over 70 years (hazard ratio (HR) = 3.599; 95% confidence interval (CI): 1.364–9.501; p = 0.010), chronic kidney disease (HR = 3.498; 95% CI: 1.265–9.671; p = 0.016), and anticoagulants use (HR = 3.903; 95% CI: 1.542–9.875; p = 0.004).
Stricture dilation
Strictures are the most common complication of CD, causing significant patient discomfort due to pain, constipation, bloating, vomiting, weight loss, and malnutrition. 68 Nearly half of CD patients will develop a stricture during their lifetime, with 30% occurring within the first 10 years.69,70 Balloon dilation is recommended by the European Crohn’s and Colitis Organisation and British Society of Gastroenterology for symptomatic strictures less than 5 cm in length, along with immunosuppressive or biologic therapy.29,71
Endoscopic management of strictures is possible in one of three ways: Balloon dilation, stricturotomy, or stenting. 72 EBD can be achieved in any part of the intestinal tract by inserting orally a balloon-assisted enteroscope, localizing site of the bowel stricture and dilating it with a through-the-scope balloon.30,31 Endoscopic stricturotomy (ES) is an innovative procedure, one in which strictures are cut with electroincision knives in a radial, horizontal, semi-circumferential, or circumferential fashion. A compressed stent is guided over a guidewire through a stricture, and when correct placement is ensured, it expands, widening the previously narrowed lumen. As outlined by the Global Interventional Inflammatory Bowel Disease Group consensus statement, EBD is an effective and safe intervention for primary or anastomotic strictures <4–5 cm. Clinical success and safety margins are notably superior when intervening upon a sparse distribution of adjacent strictures (n < 4) compared to patients presenting with extensive multifocal strictures (n > 4). 29 Lan and Shen 73 demonstrated in 21 patients a higher immediate technical success rate of ES compared to balloon dilation (100% vs 89.5%) in patients with CD, along with superior symptomatic and endoscopic improvement rates. Stricturotomy was associated with a lower need for subsequent surgery (9.5% vs 33.5%) and a reduced risk of perforation compared to balloon dilation. However, a significant drawback of ES was an 8.8% incidence of post-procedural bleeding requiring transfusion.73,74 The study in question presented some methodological imperfections: baseline characteristics indicated a higher rate of pre-procedural anti-TNF-alpha utilization in the ES group versus the EBD group (42.9% vs 25.6%), potentially reflecting a cohort with more severe, refractory disease. Additionally, follow-up periods were markedly disparate: median follow-up was 0.8 years (IQR: 0.1–1.6) for ES and 4.0 years (IQR: 0.8–6.9) for EBD. Nevertheless, after appropriate statistical adjustment, the authors reported no significant difference in surgery-free survival between the cohorts. 73 According to the 2020 guidelines of the Global Interventional Bowel Disease Group, stents can be considered in cases of failed EBD and stricturotomy for the management of strictures. 72 Despite the technical simplicity of stent placement, there is a substantial rate of stent migration (43.9%, with fully covered self-expandable metal stents, in particular) and a complication rate of 15.7%, including perforation in 2.7% of cases75,76 (Table 2).
ES and EBD comparison.
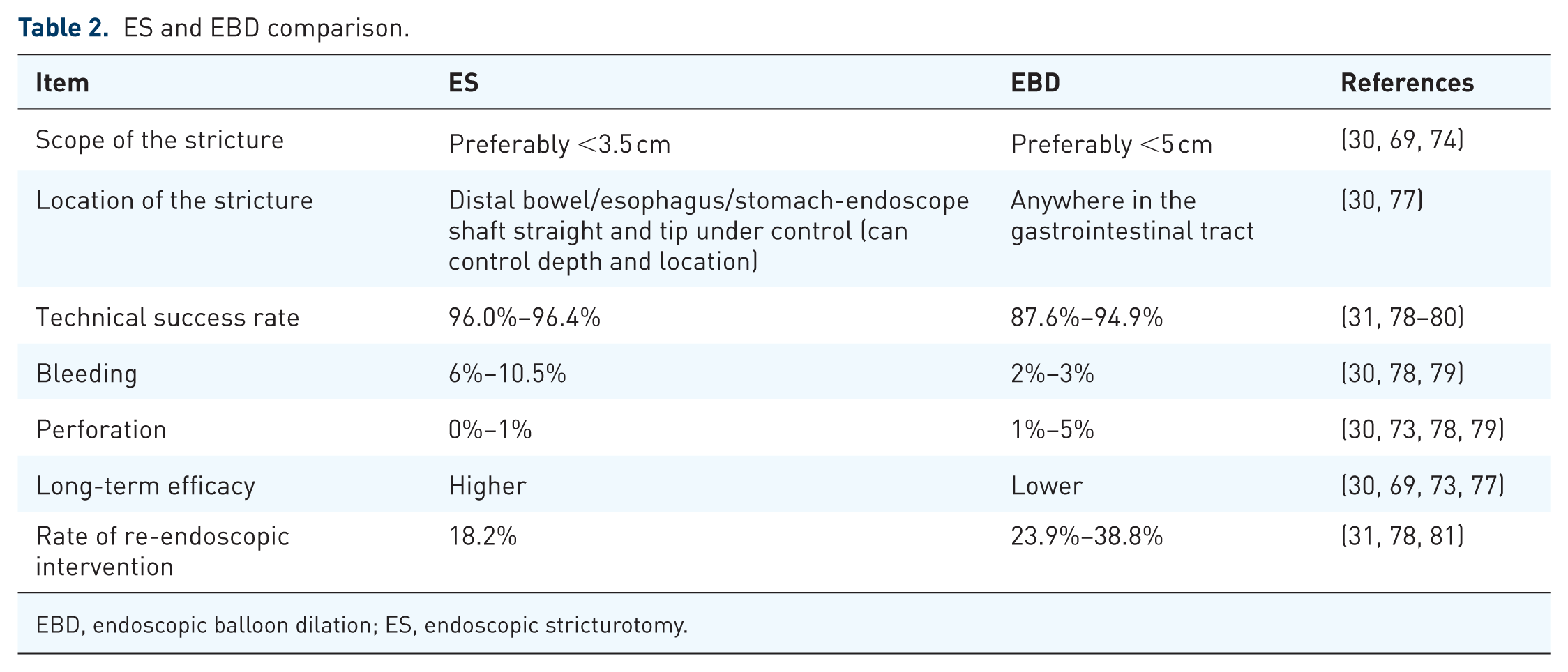
EBD, endoscopic balloon dilation; ES, endoscopic stricturotomy.
Polyps of the small intestine
Small intestinal polyps are found in 90% of patients with PJS and in over 75% of patients with familial adenomatous polyposis (FAP). 14 Other gastrointestinal polyposis syndromes include juvenile polyposis syndrome (JPS) and hamartomatous tumor syndromes associated with PTEN mutations (PHTS). Lesions can also occur sporadically. Polyps in the small intestine most often occur in the duodenum. Although they usually do not give symptoms, they can develop into cancerous lesions, cause bleeding or lead to obstruction and therefore require removal.
According to the ESGE Guideline, the current standard of care is single and DBE, which enables both diagnostic assessment and therapeutic intervention for lesions located deep within the small bowel. These techniques allow effective removal of polyps measuring up to 60–100 mm in diameter, depending on the report. For polyps ⩽10 mm and multiple diminutive lesions, cold snare polypectomy is considered an appropriate therapeutic option, as such small lesions carry a low risk of malignancy. 82
Patient selection for enteroscopic polypectomy is based on the underlying polyposis syndrome, polyp size, and the presence of clinical symptoms. In patients with PJS, intervention is recommended for polyps ⩾15–20 mm due to the high risk of intussusception; in clinical practice, treatment is often considered when at least one polyp ⩾15 mm is identified.83,84 In FAP duodenal adenomas, resection is generally considered for lesions ⩾10 mm. 83 For benign epithelial or subepithelial small bowel tumors confined to the mucosal or submucosal layers, endoscopic treatment is indicated in symptomatic cases or when there is a risk of malignant transformation.
Polypectomy is particularly important in FAP syndrome, where the risk of malignant transformation is very high.82,85,86 Also in PJS, some polyps may show features of precancerous or even cancerous lesions. 87 Removal of these lesions aims to significantly reduce the risk of malignant tumors in the future. Although polyps caused by JPS are benign, people diagnosed with JPS are at higher risk of developing certain types of cancer, including small bowel cancer. These polyps can also cause significant gastrointestinal bleeding. While many polyps in PHTS are benign hamartomas, some may demonstrate neoplastic potential; therefore, strict endoscopic surveillance is required.
Outcomes of DAE demonstrate high technical success and a significant reduction in complications requiring emergency intervention. DAE enables safe removal of lesions located deep within the small bowel without the need for laparotomy. In patients with PJS, removal of hamartomatous polyps of the small intestine (present in 60%–90% of patients) reduces the risk of intussusception, obstruction, and bleeding. 83 In FAP, endoscopic treatment of advanced duodenal polyposis has been shown to lower Spigelman scores, reflecting a reduction in polyp burden and dysplasia. 83
Enteroscopy should be preferred over surgical treatment whenever it allows avoidance of repeated bowel resections and the development of short bowel syndrome, particularly in patients with PJS requiring multiple interventions. 84 Each laparotomy increases the risk of adhesions, which may complicate future procedures. 87
Foreign body removal
Over 80% of ingested foreign bodies pass spontaneously without the need for medical intervention. 88 Patient selection for enteroscopic removal is primarily based on the presence of small bowel impaction and clinical symptoms. When a foreign body becomes retained in the small bowel, enteroscopy enables minimally invasive retrieval. The most common foreign bodies include retained endoscopic capsules, bezoars, needles, coins, gastric bands, dental prostheses, parasites, and migrated stents.14,89 The ESGE recommends performing balloon enteroscopy for such indications as an alternative to surgery if the patient does not have an acute intestinal obstruction. 21 After several unsuccessful endoscopic attempts at foreign body removal, or in the case of clinical deterioration, surgical intervention may be required. 90
Reported outcomes of balloon-assisted enteroscopy for foreign body removal vary across studies. In a multicenter Korean study including 34 patients undergoing single- or double-balloon enteroscopy, the overall success rate was 50%. Two patients experienced procedure-related complications (perforation and pancreatitis), which resolved with conservative treatment. 91 The complication profile of enteroscopic retrieval appears generally favorable, with low rates of serious adverse events. Notably, 52.9% of retained foreign bodies were endoscopic capsules. Symptomatic patients—presenting with abdominal pain, nausea, vomiting, or bloating—accounted for 58.8% of cases and demonstrated a higher likelihood of successful endoscopic retrieval compared with asymptomatic individuals. 91 In contrast, among nine patients without symptoms in whom retrieval failed, four experienced spontaneous passage of the foreign body, suggesting that watchful waiting may be an appropriate strategy in selected asymptomatic cases. 91
Higher success rates have also been reported. A study by Nakamura et al. 92 analyzed 22 cases of foreign bodies in the small bowel among 1280 patients undergoing DBE. Foreign bodies included endoscopic capsules, artificial teeth, medical tubes, worms, press-through packets of medicine, and intestinal stones. The oral route and snare forceps were most commonly used. The removal success rate reached 86.3%, with no reported complications.
ESGE recommends clinical observation for asymptomatic patients who have swallowed blunt, small objects (excluding batteries and magnets), and for asymptomatic patients who have swallowed drug packets, with weekly X-rays if progression is not observed. 93 Urgent endoscopic (within 24 h) or surgical intervention is indicated for sharp and pointed objects, magnets, batteries, and large or long objects in the small bowel, as well as in cases of failed conservative management or when signs of perforation or bowel obstruction develop.
ERCP in surgically altered anatomy
With enteroscope, one may perform endoscopic retrograde cholangiopancreatography (ERCP) in patients after surgical procedures such as Roux-en-Y total gastrectomy, Roux-en-Y gastric bypass, pancreatoduodenectomy (Whipple surgery), Roux-en-Y hepato-jejunostomy, and Billroth II partial gastrectomy (second-choice test).10,21 ERCP is the gold standard for diagnosing and treating biliary tract pathologies, including stones and benign or malignant strictures. 94
In patients with surgically altered anatomy, standard duodenoscopes often fail to reach the biliary tree. In these scenarios, an enteroscope enables deep intubation of the small bowel, allowing access to the native papilla or biliopancreatoenteric anastomosis to perform essential cholangiopancreatography and subsequent therapeutic interventions. 95
The clinical necessity for these advanced techniques is increasing due to the growing incidence of bariatric surgery and improved survival rates among patients following surgical resections for upper gastrointestinal cancers. 94
Specific surgical procedures that profoundly alter the anatomy and hinder standard ERCP include Roux-en-Y gastric bypass (a bariatric procedure indicated for the management of severe obesity), Billroth II reconstruction ( often performed following a distal gastrectomy for gastric cancer or severe peptic ulcer disease), pancreaticoduodenectomy (Whipple procedure) (indicated for the radical resection of pancreatic, duodenal, or distal bile duct malignancies) and hepaticojejunostomy and choledochojejunostomy (reconstructions performed for benign biliary strictures, severe bile duct injuries, or malignant biliary obstructions).94,95
When standard endoscopic access fails, the endoscopic ultrasound rendezvous (EUS-RV) technique serves as a valuable rescue strategy. This method involves the EUS-guided puncture of an intrahepatic bile duct to pass a guidewire through the anastomosis, which is subsequently retrieved by an enteroscope to successfully complete the ERCP.
Successful intervention relies intrinsically on tailoring endoscope selection to the specific surgical reconstruction. 96
For short-limb anatomies, such as Billroth II or short Roux-en-Y reconstructions, forward-viewing pediatric colonoscopes typically afford sufficient access, effectively precluding the need for BAE.96,97
Conversely, long-limb configurations—including Roux-en-Y gastric bypass, post-Whipple reconstructions, and hepaticojejunostomies—exceed the working length of conventional endoscopes and necessitate deep small-bowel intubation.96,98
In these complex cases, DAE serves as the gold standard. DAE is a generic term that describes any endoscopic technique for small bowel examination involving assisted progression, utilizing specialized mechanisms like single-balloon or double-balloon overtubes. 94 DAE overcomes the mechanical constraints of standard scopes, providing unparalleled deep enteral access and achieving high technical success rates for ERCP across complex surgically reconstructed bowel. 21 However, because specialized DAE technology is available in very few medical centers, clinical practice often necessitates focusing on typical enteroscopes and maximizing their standard capabilities in ERCP. 95
Patients with IBD, such as UC or Crohn’s disease, face a significantly elevated risk of developing PSC. 94 These specific PSC-related complications often manifest as severe, progressive fibroinflammatory biliary strictures, or ultimately cholangiocarcinoma, creating a critical clinical indication for enteroscopy-assisted ERCP to achieve urgent tissue diagnosis and life-saving biliary drainage. 95
Although the balloon enteroscope provides unparalleled deep enteral access, its protracted length and narrow working channel preclude the passage of conventional delivery systems for self-expandable metal stents. To bypass this mechanical constraint, a modified deployment strategy is utilized. Initially, the enteroscope is advanced to the stricture, facilitating the placement of a guidewire across the stenotic segment. The enteroscope is then entirely withdrawn while maintaining the position of both the guidewire and the inflated overtube. This allows for the over-the-wire deployment of a large-caliber enteral stent directly through the wider overtube lumen to traverse the stricture. Ultimately, this advanced technique enables effective therapeutic stenting within deep, surgically reconstructed bowel, thereby circumventing the morbidity associated with high-risk revisional laparotomies. 99
Safety of enteroscopy
It is worth highlighting that enteroscopy is a high-safety procedure, where the risk of complications ranges from 0.4% to 5.5% for both double-balloon and single-balloon enteroscopy. 100 No significant differences in the safety of the two examination techniques have been found. The possible complications include perforation, pancreatitis, bleeding, aspiration pneumonia, intussusception, paralytic ileus, and intestinal necrosis. 100 As presented in Table 3, the incidence of specific complications such as bleeding, bowel perforation, and pancreatitis remains low, not exceeding 2.9% for the most serious adverse events. A higher risk of complications, such as bleeding and perforation, is a concern with therapeutic interventions. 11 Older patients are more likely than younger ones to suffer from side effects related to sedation itself, which occur in 17% of all interventions. 11 Therefore, in elderly patients, it is advisable to use the lowest cumulative dose of sedation drugs possible. 100 Geriatric patients are also at higher risk of aspiration and hypoxia during enteroscopy. 100 Nevertheless, with appropriately selected cases and taking into account each patient’s individual risk factors, enteroscopy remains a safe procedure with a low incidence of complications (Table 3).
The incidence of specific complications in patients undergoing SBE and DBE.
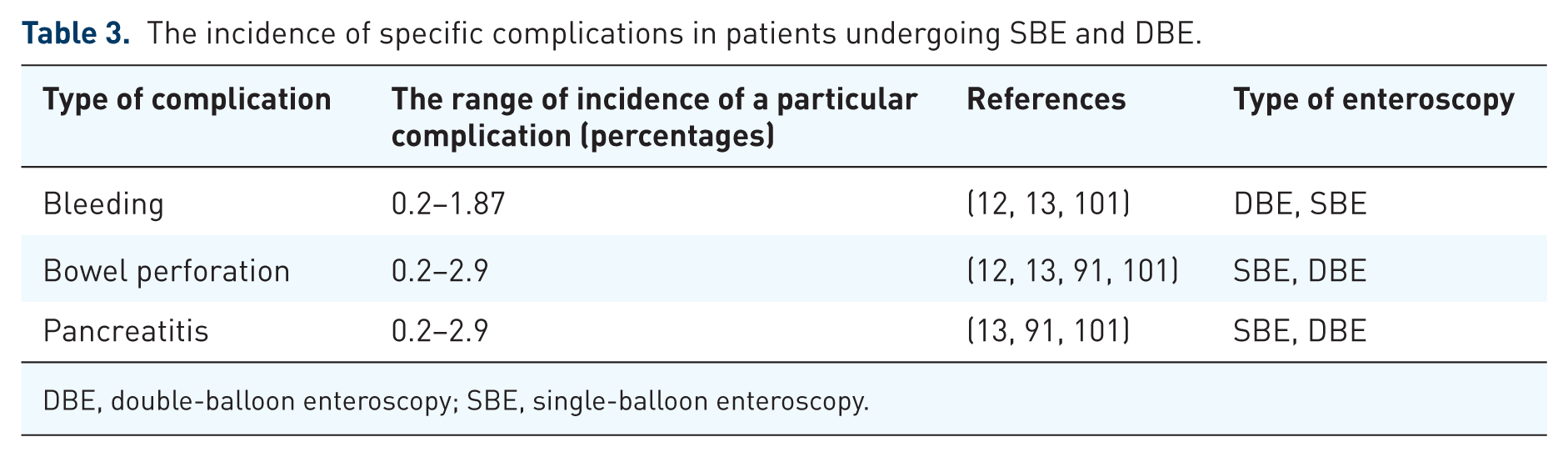
DBE, double-balloon enteroscopy; SBE, single-balloon enteroscopy.
Comparison of enteroscopy and other small bowel imaging
Imaging studies such as ultrasound, CT, and magnetic resonance imaging (MRI) have several advantages over enteroscopy, such as less patient discomfort, reduced risk of bowel perforation, and a non-invasive nature. CT and MRI are used to assess the activity and location of small bowel involvement in Crohn’s disease by evaluating the wall thickness of the intestine and contrast enteric wall enhancement. Ultrasound through the abdominal wall demonstrates lower sensitivity and specificity in assessing the extent of bowel involvement than MRI (70% vs 80%, 81% vs 95%). 102 A diagnosis of Crohn’s disease could be made based on MRE with a sensitivity of 78% and a specificity of 85%. 103 MRE is a targeted examination of gastrointestinal tract, requiring distending bowels with a contrast solution administered either orally or after mid-gut tubing. 104 Both ultrasound and MRI showed greater specificity (92.9%, 94.0%, and 90.2% for US, MRI, and CT, respectively) and sensitivity (73.5%, 70.4%, and 67.4% for US, MRI, and CT, respectively) in assessing IBD involvement of a bowel segment than CT, making them preferred examinations while reducing patient exposure to radiation. 103 Intestinal ultrasound emerges as an accurate monitoring tool measuring CD activity, allowing for even more objective evaluation, regardless of operators’ experience, with the parameter of bowel wall thickness (BWT, considering BWT over 4 mm a pathological finding) demonstrating almost perfect inter-rater agreement and correlation with overall assessment of disease activity.103,105
In one systematic review including 251 patients, capsule endoscopy was evaluated as a diagnostic method with a value comparable to MRE, and even—in the case of involvement of the proximal small bowel—more valuable (odds ratio 2.79; 95% CI: 1.2–6.48; p = 0.02; I2 = 68%). 106 In case of suspected active small bowel gastrointestinal bleeding, DBE should be the procedure of choice. This is supported by the fact that capsule endoscopy, passing through a given segment of the intestine too quickly or having the camera obscured by, for example, food residues, air bubbles, or bile, misses 20%–30% of lesions later visualized in DBE.11,16 Considering the application of this method, the risk of its use in case of strictures or obstructions should be taken into account.
Even after taking into consideration all of these advantages of imaging studies over enteroscopy, it proves superior in sensitivity and specificity, especially in visualizing deeper lesions, over intestinal ultrasound. 107 It’s also superior in the detection of proximal small intestinal lesions, identifying 19 duodenal lesions (9.6%) and 62 upper jejunal lesions (31.3%), compared to just 1 lesion identified by CTE and 4 lesions identified by intestinal ultrasound (p < 0.001).108–110
Enteroscopy, with its coagulation, biopsy, polypectomy, or stricture dilation, has a clear advantage of allowing therapeutic intervention over other small bowel imaging techniques. Enteroscopy demonstrates higher sensitivity and specificity compared to intestinal ultrasound for visualizing deeper lesions within the small bowel wall. Enteroscopic therapy for bleeding, strictures, and polyps primarily reduces the risk of adverse events and complications compared to surgical interventions. MRE and capsule endoscopy are recommended for small-bowel surveillance in PJS. The main limiting factors for wider implementation of these techniques are: the limited number of prospective randomized studies (which does not allow for the strong recommendations and guidelines), high enter point regarding the operator’s experience, fact that it’s a highly time consuming technique, and inaccessibility for the wider population. The use of enteroscopy with the new additional techniques is increasing in the last decades, therefore along with the growing experience and awareness of small bowel diseases, patients’ prognosis may improve in the near future.
Discussion
The management of small-bowel pathology has undergone a paradigm shift in the span of the last 20 years. Our article highlights this transition from a “reactive” diagnostic approach to a “proactive” interventional one, driven largely by the refinement of VCE and DAE techniques.
A recurring theme emerging across the literature is the complementary relationship between VCE and DAE. VCE has been established as the preferred initial diagnostic tool (due to its non-invasive nature and high negative predictive value). However, as supported by ESGE Guidelines (2023), the role of DAE has also expanded: it is no longer merely a “follow-up” to an abnormal capsule study; in cases of high clinical suspicion (such as suspected Crohn’s strictures or complicated CD), the “DAE-first” or “MRE-guided” approach is increasingly supported to allow for immediate tissue acquisition and interventional therapy.
One of the most striking developments within the interventional enteroscopy is the evolution of CD management—while early 2010s data focused on the safety of EBD, the most recent references from 2024 to 2025 signal the rise of ES. This technique, which offers a more durable solution for complex strictures than traditional dilation, represents a significant move toward bowel-sparing strategies, potentially delaying or even eliminating the need for surgical resection in a subset of patients.
While this review’s focus is on endoscopy, the data reinforce that endoscopy does not exist in a vacuum. MRE and intestinal ultrasound have become indispensable for assessing the extent of IBD involvement of a bowel segment. The ability of MRE to detect extra-mural disease (abscesses, fistulae) can provide a safety roadmap for the endoscopist, identifying which strictures are safe to dilate and which require a surgical rather than endoscopic approach.
Despite the increased complexity of procedures like stricturotomy and large-scale polypectomy, the safety profile of small-bowel endoscopy remains high. This is likely due to better training and the emergence of highly specialized centers performing a high volume of these procedures. However, the literature warns of the “sedation gap”—the need for specialized anesthetic support during long DAE procedures, especially in elderly populations where procedural time directly correlates with complication risk. As such, a concern for the growing discrepancies in access to quality healthcare emerges—with smaller rural health facilities potentially lacking the support needed to obtain highly specialized training, equipment, and anesthetic support.
In conclusion, the small bowel is no longer the “dark continent” of the gastrointestinal tract. Between 2001 and 2025, the field has moved beyond simple visualization. We have entered an era of interventional enteroscopy, where the endoscopist can treat bleeding, dilate or cut strictures, and remove complex polyps deep within the small intestine. Future research should focus on the long-term durability of stricturotomy versus surgery and the integration of artificial intelligence in capsule endoscopy to further refine the diagnostic accuracy of these life-changing tools and bridge the gap between demand and supply for highly specialized professionals.