
Abstract
Background:
The incidence of inflammatory bowel disease (IBD) is rising across Southeast Asia, yet real-world data on clinical phenotypes, treatment strategies, and outcomes in tuberculosis (TB)-endemic, resource-constrained settings remain scarce.
Objectives:
To characterize disease phenotypes, treatment utilization, and 1-year outcomes in a Vietnamese inception cohort of newly diagnosed IBD patients in a tuberculosis-endemic, resource-constrained setting.
Design:
Single-center, hybrid retrospective–prospective inception cohort study.
Methods:
Consecutive adults diagnosed with Crohn’s disease (CD) or ulcerative colitis (UC) at a tertiary referral center in Ho Chi Minh City, Vietnam, between June 2019 and June 2024. A Baseline Cohort (N = 126) was analyzed for phenotypic characterization. Patients completing ⩾12 months of follow-up comprised the Outcome Cohort (N = 66) for assessment of treatment patterns and clinical, biochemical, and endoscopic outcomes. Treatment followed an accelerated step-up strategy with originator anti-tumor necrosis factor (TNF) agents (infliximab/adalimumab) after mandatory TB screening.
Results:
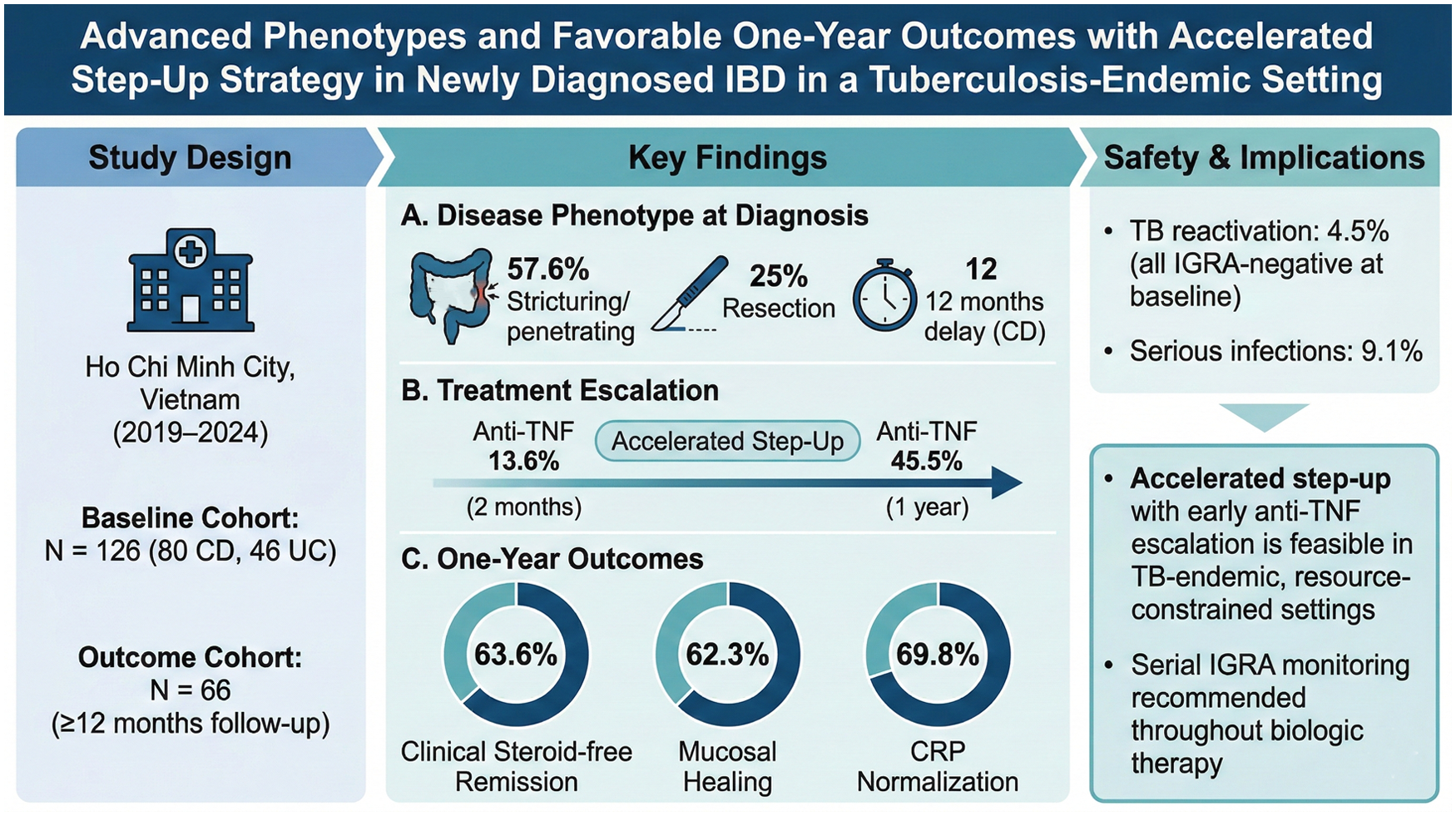
Among 126 patients (80 CD, 46 UC), CD was characterized by substantial diagnostic delay (median 12 months), with 57.6% presenting stricturing or penetrating behavior and 25.0% having undergone intestinal resection before IBD confirmation. Extensive colitis (E3) predominated among UC patients (63.0%), and 78.3% had moderate-to-severe disease. Anti-TNF utilization increased from 13.6% within the first 2 months after diagnosis to 45.5% at 1 year. In the Outcome Cohort (N = 66), steroid-free clinical remission was achieved in 63.6%, and mucosal healing was documented in 62.3% of endoscopically evaluated patients. Serious infections occurred in 9.1%, with TB reactivation in 4.5%.
Conclusion:
IBD in Vietnam presents with diagnostic delays, complicated phenotypes, and high surgical rates at initial presentation. Despite these challenges, an accelerated step-up strategy with early anti-TNF escalation was associated with favorable 1-year steroid-free remission and mucosal healing rates. These findings suggest that treat-to-target care with early biologic escalation may be feasible in selected patients in TB-endemic, resource-constrained settings, provided that structured TB monitoring is implemented.
Plain language summary
Inflammatory bowel disease (IBD) is becoming more common in Southeast Asia, including Vietnam. However, diagnosing it is difficult because its symptoms are very similar to intestinal tuberculosis (TB), a common infection in the region. Because of this confusion, patients often suffer for a long time—sometimes up to a year—before finding out they have IBD. By the time they are properly diagnosed, their disease is often severe, and some even require surgery before receiving the correct diagnosis. In this study, we looked at 126 adults newly diagnosed with IBD at a major hospital in Vietnam. We wanted to see if treating them quickly with strong, advanced medications (known as biologics) would be safe and effective. We found that this treatment approach was associated with encouraging one-year outcomes. After one year of treatment, about 64% of the patients felt completely well without needing to take steroid medications. Furthermore, tests showed that the inside of the intestines had healed completely in 62% of the patients. However, because these strong medications can lower the body’s immune defenses, we carefully tested everyone for TB before starting treatment. Even with negative initial TB tests, 4.5% of patients still developed TB later. This highlights that ongoing monitoring for tuberculosis may be important throughout the course of biologic treatment, rather than relying solely on a single test before starting therapy.
Keywords
Introduction
Inflammatory bowel disease (IBD), comprising Crohn’s disease (CD) and ulcerative colitis (UC), was traditionally considered a condition predominantly affecting Western populations. However, the epidemiology of IBD has shifted dramatically in recent decades, evolving into a global disease with rapidly rising incidence in newly industrialized Asian countries. 1 In Southeast Asia, although prevalence remains lower than in the West, the incidence is rising rapidly, mirroring urbanization and dietary westernization in the region. 2 Despite this emerging burden, prospective data on the clinical characteristics, treatment patterns, and outcomes of IBD patients in Southeast Asia—particularly Vietnam—remain scarce. Most existing studies are cross-sectional or retrospective, leaving a significant knowledge gap regarding the natural history and disease trajectory in this population.3–5
Diagnosis and management of IBD in tropical, TB-endemic regions like Vietnam present unique challenges. Vietnam remains among the 30 high TB-burden countries globally, with an estimated incidence of 100–299 cases per 100,000 population in 2024. 6 This high background prevalence of TB profoundly complicates IBD management, as the clinical presentation of CD frequently overlaps with intestinal tuberculosis (ITB), creating a diagnostic dilemma that leads to delays and misdiagnosis.7,8 Consequently, patients often present with advanced disease phenotypes, including stricturing or penetrating behavior, at the time of definitive diagnosis. In a recent Vietnamese multicenter study, stricturing and penetrating phenotypes were observed in 25.0% and 28.1% of newly diagnosed CD patients, respectively. 3 Understanding the baseline characteristics of these newly diagnosed patients is crucial for tailoring appropriate management strategies and preventing early complications.
Over the past decade, the therapeutic paradigm of IBD has shifted toward a treat-to-target approach, emphasizing early control of inflammation and objective targets such as mucosal healing.9,10 The introduction of biologic agents has transformed patient care by improving rates of mucosal healing, steroid-free remission, and long-term outcomes.11,12 While international guidelines advocate for early and effective intervention to alter the disease course,13,14 real-world data on the implementation of these strategies in Vietnam and comparable Southeast Asian countries are limited. In particular, whether an accelerated step-up strategy with early biologic escalation can achieve favorable mucosal healing rates in a TB-endemic, resource-constrained setting has not been established.
To address these knowledge gaps, we conducted a single-center, hybrid retrospective–prospective cohort study of adults newly diagnosed with IBD at a tertiary referral hospital in Vietnam. Our objectives were threefold: (1) to characterize the baseline clinical phenotypes of this inception cohort; (2) to delineate treatment patterns with a focus on biologic utilization over the first 12 months; and (3) to evaluate 1-year clinical, biochemical, and endoscopic outcomes under an accelerated step-up strategy.
Methods
Study design and context
We conducted a single-center, hybrid retrospective–prospective inception cohort study at the IBD Unit, University Medical Center Ho Chi Minh City, a tertiary referral hospital in Vietnam. The study period spanned 5 years, from June 2019 to June 2024. The hybrid retrospective–prospective design was adopted to maximize cohort size while maintaining inception cohort principles. The retrospective arm captured patients diagnosed during the early establishment of our IBD unit (June 2019–May 2023), while the prospective arm enabled standardized data collection (June 2023–June 2024). The study protocol was approved by the Institutional Review Board of the University of Medicine and Pharmacy at Ho Chi Minh City (approval number: 711/HDDD-DHYD, dated May 15, 2023). Written informed consent was obtained from all prospectively enrolled patients, while a waiver of consent was granted for the retrospective chart review. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 15 The completed STROBE checklist is provided as Supplemental Material.
Study population and data collection
The study population comprised adult patients (aged ⩾18 years) with a newly confirmed diagnosis of IBD established according to the European Crohn’s and Colitis Organisation (ECCO) criteria. 16 Diagnosis was based on a comprehensive integration of clinical evaluation, endoscopy, histology, radiology, and biochemical investigations. Given the high background prevalence of TB, a comprehensive screening—including clinical evaluation, routine chest radiography, Interferon-Gamma Release Assay (IGRA), and tissue polymerase chain reaction (PCR)—was performed to rigorously exclude ITB. To ensure a homogeneous inception cohort, we excluded patients with IBD-unclassified, isolated perianal disease without luminal involvement, or those who had received IBD-specific treatment prior to referral.
Eligible patients were stratified into two analytical groups: a Baseline Cohort, consisting of all newly diagnosed patients for the assessment of initial characteristics and disease phenotype; and an Outcome Cohort, comprising patients who completed at least 12 months of follow-up to evaluate treatment effectiveness and 1-year outcomes.
Data acquisition was standardized across both arms. Prospectively recruited patients were assessed using a standardized case report form; retrospective data were abstracted from medical records using a predefined extraction template. All data were consolidated into a secure, de-identified database.
Definitions
Baseline characteristics were classified according to standard international systems. For UC, disease extent was defined using the Montreal classification as proctitis (E1), left-sided colitis (E2), or extensive colitis (E3). 16 Clinical disease activity was assessed based on the Truelove and Witts criteria, while endoscopic activity was graded using the Mayo Endoscopic Subscore.16,17 For CD, baseline phenotypes were characterized according to the Montreal classification, including location (ileal (L1), colonic (L2), ileocolonic (L3), and upper gastrointestinal modifier (L4)) and disease behavior (non-stricturing non-penetrating (B1), stricturing (B2), penetrating (B3)).16,17 Perianal disease, defined as the presence of fistulae, abscesses, or anal ulcers, was recorded as a modifier (p). 17 Clinical activity for CD was quantified using the Crohn’s Disease Activity Index (CDAI).16,17 In this study, “advanced phenotypes” was used as an operational descriptor for complicated CD phenotypes and extensive UC. Complicated CD phenotypes were defined as stricturing (B2) or penetrating (B3) behavior according to the Montreal classification, while extensive UC was defined as E3 disease.
Given the high prevalence of TB in Vietnam, a standardized screening protocol was implemented prior to initiation of immunomodulators or biologic therapy. Screening for latent tuberculosis infection (LTBI) included a chest radiograph and an IGRA.17,18 Patients diagnosed with LTBI (defined as a positive IGRA without clinical or radiographic evidence of active TB) received prophylactic treatment with isoniazid (300 mg/day) for 9 months.17,18 Biologic therapy was typically initiated after at least 4 weeks of adequate prophylactic treatment, in accordance with Asian consensus guidelines.17,18
Therapeutic strategy
Therapeutic management followed international guidelines, with treatment tiers categorized hierarchically in ascending order of potency: 5-aminosalicylates (5-ASA), systemic corticosteroids, immunomodulators (azathioprine or 6-mercaptopurine), and anti-TNF agents. 4 In this cohort, the biologic agents administered were exclusively originator anti-TNF agents (infliximab and adalimumab). No patients received biosimilars or non-anti-TNF biologics (such as vedolizumab or ustekinumab) during the study period. The overall therapeutic framework remained consistent throughout the study period (2019–2024). No major protocol changes were implemented; however, the threshold for early biologic escalation progressively lowered over time in line with evolving international evidence supporting earlier intervention in high-risk patients.
In this study, an accelerated step-up strategy was defined as the initiation of conventional therapy (5-ASA, corticosteroids, or immunomodulators) at diagnosis, with early escalation to anti-TNF agents within the first 2–6 months. Escalation to anti-TNF was triggered by inadequate clinical response (persistence or worsening of symptoms despite optimized conventional therapy), objective evidence of ongoing inflammation (elevated C-reactive protein (CRP) >5 mg/L or fecal calprotectin >250 µg/g), or endoscopic disease activity at scheduled reassessment. While there was no rigid protocol mandating escalation at a fixed time point, decision-making followed standardized reassessment intervals (every 2–3 months) and was guided by a treat-to-target framework applied consistently by the IBD team throughout the study period. This approach differs from the conventional step-up strategy, in which biologic escalation typically occurs only after prolonged failure of multiple conventional agents, and from a top-down strategy, in which biologics are initiated as first-line therapy. Patients were routinely reassessed at 2–3 month intervals during the first year, with clinical evaluation, biochemical monitoring (CRP and fecal calprotectin), and endoscopic re-evaluation typically performed at 6–12 months post-diagnosis or earlier if clinically indicated.
To characterize the treatment trajectory, medication exposure was summarized using two hierarchical variables: (1) Highest Initial Therapy, defined as the most potent medication tier administered within the first 2 months post-diagnosis; and (2) Highest One-Year Therapy, defined as the most potent medication tier required during the 12-month follow-up period. 4 For each patient, only the highest tier reached within the specified timeframe was recorded.
Outcomes were evaluated at 12 months post-diagnosis using clinical, biochemical, and endoscopic criteria. Clinical response was defined as a decrease in CDAI of ⩾70 points from baseline for CD, and a reduction of at least 50% in the frequency of loose and bloody stools compared to baseline for UC. 17 Clinical remission was defined as a CDAI <150 points for CD, and for UC, as the normalization of bowel habit (stool frequency ⩽3 times/day) combined with the absence of bloody stool. 17 Steroid-free clinical remission was defined as the achievement of clinical remission without the use of corticosteroids for at least 4 weeks prior to the assessment.
Objective markers of disease control included biochemical and endoscopic outcomes. Normalization of CRP was defined as a serum CRP level <5 mg/L, while normalization of fecal calprotectin was defined as a level <150 µg/g. 9 Endoscopic remission (mucosal healing) was strictly defined as the complete absence of mucosal ulceration for CD and a Mayo Endoscopic Score of 0 for UC. 9
Adverse outcomes and safety endpoints included IBD-related hospitalizations, TB reactivation, and the need for IBD-related surgery (intestinal resection for CD or colectomy for UC). Serious infections were defined as any infection requiring hospitalization and administration of intravenous antibiotics. 3
Statistical analysis
Statistical analyses were performed using IBM SPSS version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as medians with interquartile ranges (IQR) due to non-normal distribution, while categorical variables were presented as frequencies and percentages. Comparisons between groups (Outcome Cohort vs excluded patients; retrospective vs prospective arms) were performed using the Mann–Whitney U test for continuous variables and the Chi-square test or Fisher’s exact test for categorical variables. To assess the representativeness of the Outcome Cohort relative to the Baseline Cohort, standardized mean differences (SMDs) were calculated; an SMD <0.10 was considered negligible, and <0.25 was considered small. Missing data were not imputed; analyses were conducted on available cases with denominators explicitly reported for each outcome measure. Sensitivity analyses bracketing best-case and worst-case scenarios were performed for outcomes with notable missing data (mucosal healing). Given the descriptive nature of this study and the limited Outcome Cohort size (N = 66), multivariable analyses adjusting for confounders were not performed; observed outcomes should be interpreted as descriptive associations rather than causal estimates. All statistical tests were two-sided, and a p-value of <0.05 was considered statistically significant. No adjustment for multiple comparisons was applied given the exploratory nature of the analyses.
Results
Patient enrollment and cohort assembly
During the study period, 126 patients with newly diagnosed IBD were included in the baseline analysis (Baseline Cohort), comprising 80 (63.5%) patients with CD and 46 (36.5%) patients with UC (Figure 1). Of these, 66 patients (41 CD and 25 UC) completed at least 12 months of follow-up and were included in the Outcome Cohort. Among the 60 patients excluded from outcome analysis, 47 (78.3%) had not yet reached the 12-month time point at the data cutoff (administrative censoring), and 13 (21.7%) were lost to follow-up (LTFU). The primary reasons for LTFU were: patient discontinuation (n = 5, 38.5%), transfer to a local hospital closer to home (n = 4, 30.8%), financial constraints (n = 3, 23.1%), and relocation (n = 1, 7.7%). Outcome ascertainment was attempted in all 13 LTFU patients via telephone contact and review of subsequent hospital records. Nine patients were successfully contacted: seven were clinically stable or in remission, whereas two remained symptomatic. Four patients could not be reached. No deaths were recorded during the study period among either the outcome cohort or the patients excluded from outcome analysis.
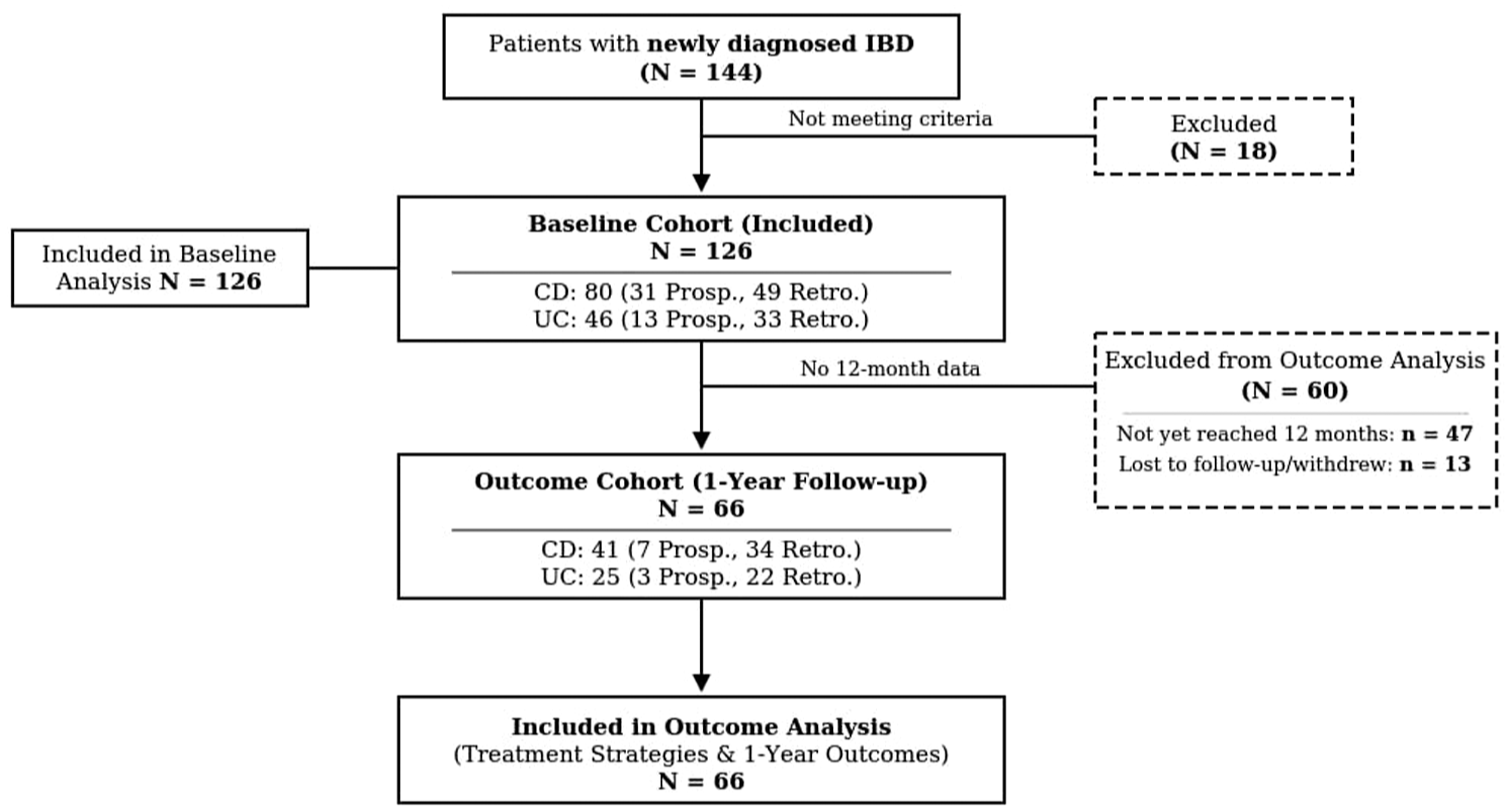
Study flowchart showing patient enrollment and cohort assembly. A total of 144 patients with newly diagnosed IBD were screened; 18 were excluded for not meeting inclusion criteria. The remaining 126 patients comprised the Baseline Cohort for phenotypic characterization. Of these, 66 patients who completed at least 12 months of follow-up were included in the Outcome Cohort for treatment and outcome analysis. Among the 60 patients excluded from the outcome analysis, 47 had not yet reached the 12-month time point (administrative censoring), and 13 were lost to follow-up or withdrew.
Baseline characteristics and disease phenotype
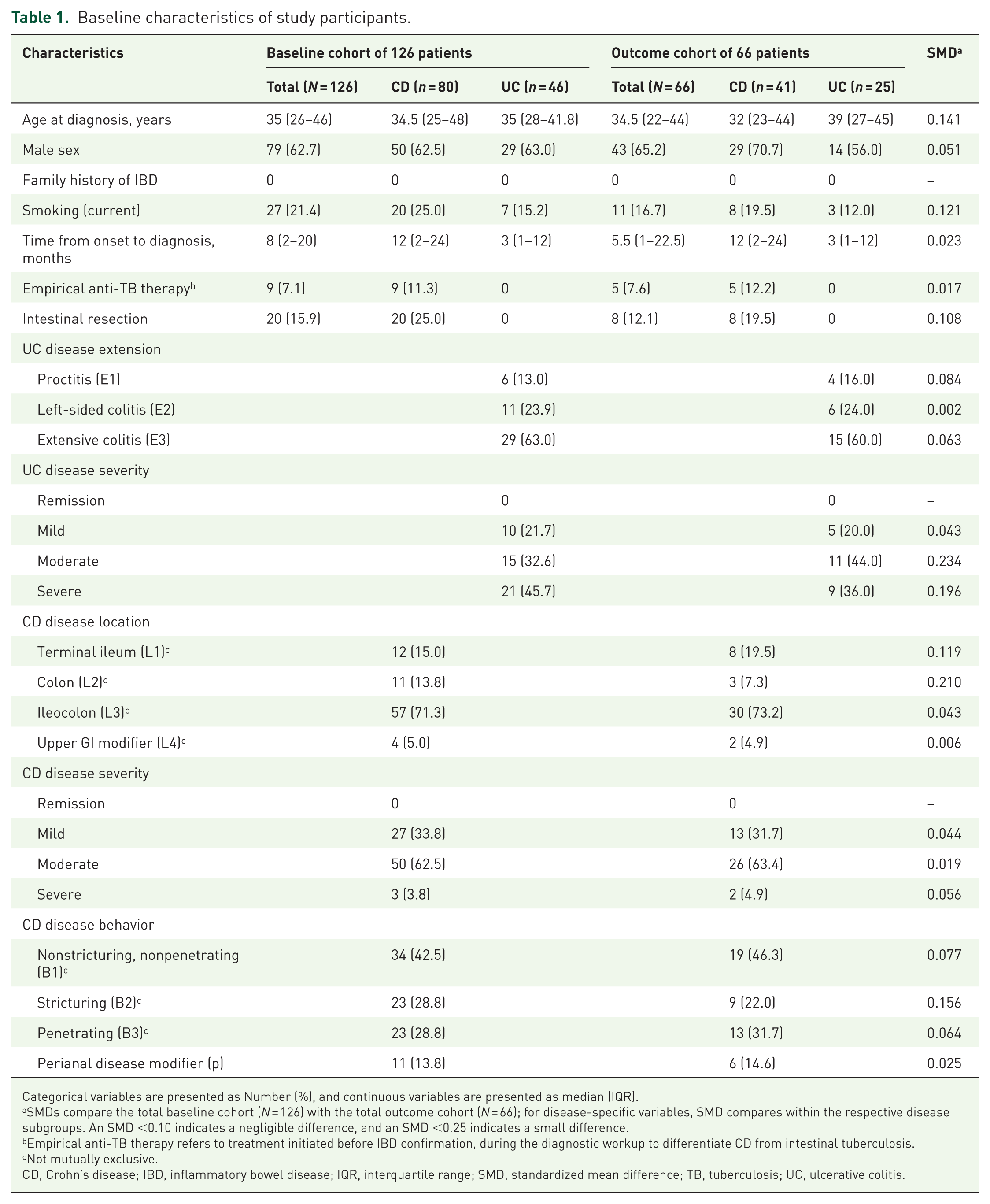
The baseline demographic and clinical characteristics of the study population are summarized in Table 1. The median age at diagnosis was 35 years (IQR 26–46), with a male predominance (62.7%) and no reported family history of IBD. The median time from onset to diagnosis was 8 months (IQR 2–20), which was considerably longer in patients with CD (12 months) compared to UC (3 months). Notably, 11.3% (9/80) of patients in the baseline CD cohort received empirical anti-TB therapy prior to the confirmation of IBD, whereas no patients with UC received this treatment.
Baseline characteristics of study participants.
Categorical variables are presented as Number (%), and continuous variables are presented as median (IQR).
SMDs compare the total baseline cohort (N = 126) with the total outcome cohort (N = 66); for disease-specific variables, SMD compares within the respective disease subgroups. An SMD <0.10 indicates a negligible difference, and an SMD <0.25 indicates a small difference.
Empirical anti-TB therapy refers to treatment initiated before IBD confirmation, during the diagnostic workup to differentiate CD from intestinal tuberculosis.
Not mutually exclusive.
CD, Crohn’s disease; IBD, inflammatory bowel disease; IQR, interquartile range; SMD, standardized mean difference; TB, tuberculosis; UC, ulcerative colitis.
In the CD cohort, ileocolonic involvement (L3) was most common (71.3%), and complicated behavior was frequent, with stricturing (B2) and penetrating (B3) phenotypes each accounting for 28.8% of cases; perianal disease was present in 13.8% of patients. Overall, 66.3% of CD patients had moderate-to-severe disease activity at diagnosis, and 25.0% had already undergone intestinal resection prior to referral.
In the UC cohort, extensive colitis (E3) was the dominant phenotype, observed in 63.0% of patients. The disease burden was significant at presentation, with 78.3% of patients exhibiting moderate-to-severe disease activity, including 45.7% classified as severe.
The SMDs between the baseline cohort and the outcome cohort were small across all measured variables (all SMDs <0.25; Table 1), with the majority showing negligible differences (SMDs <0.10). Additionally, no statistically significant differences were observed when directly comparing the outcome cohort with the 60 patients excluded due to insufficient follow-up (all p > 0.05; Table S1). Baseline characteristics were also broadly comparable between the retrospective (n = 82) and prospective (n = 44) arms, except for time from symptom onset to diagnosis, which likely reflected ascertainment heterogeneity inherent to the hybrid retrospective–prospective design (Table S2). Follow-up completeness differed by design, with a higher proportion of retrospective patients reaching the 12-month assessment (70.7% vs 18.2%, p < 0.001), reflecting administrative censoring in the prospective cohort. Loss to follow-up occurred only in the retrospective arm (15.9%). Together, these findings support the representativeness of the Outcome Cohort and suggest no substantial baseline imbalance between the retrospective and prospective arms.
Treatment patterns in the outcome cohort
Table 2 details the highest tier of medication utilized within 2 months and 1 year after diagnosis. In the first 2 months post-diagnosis, immunomodulators were the predominant highest-tier therapy for CD (51.2%), while oral mesalamine was the most frequently used agent for UC (44.0%). Notably, anti-TNF agents were initiated early in 13.6% of the total population.
Highest treatment tier within 2 months and at 12 months after diagnosis in the outcome cohort.
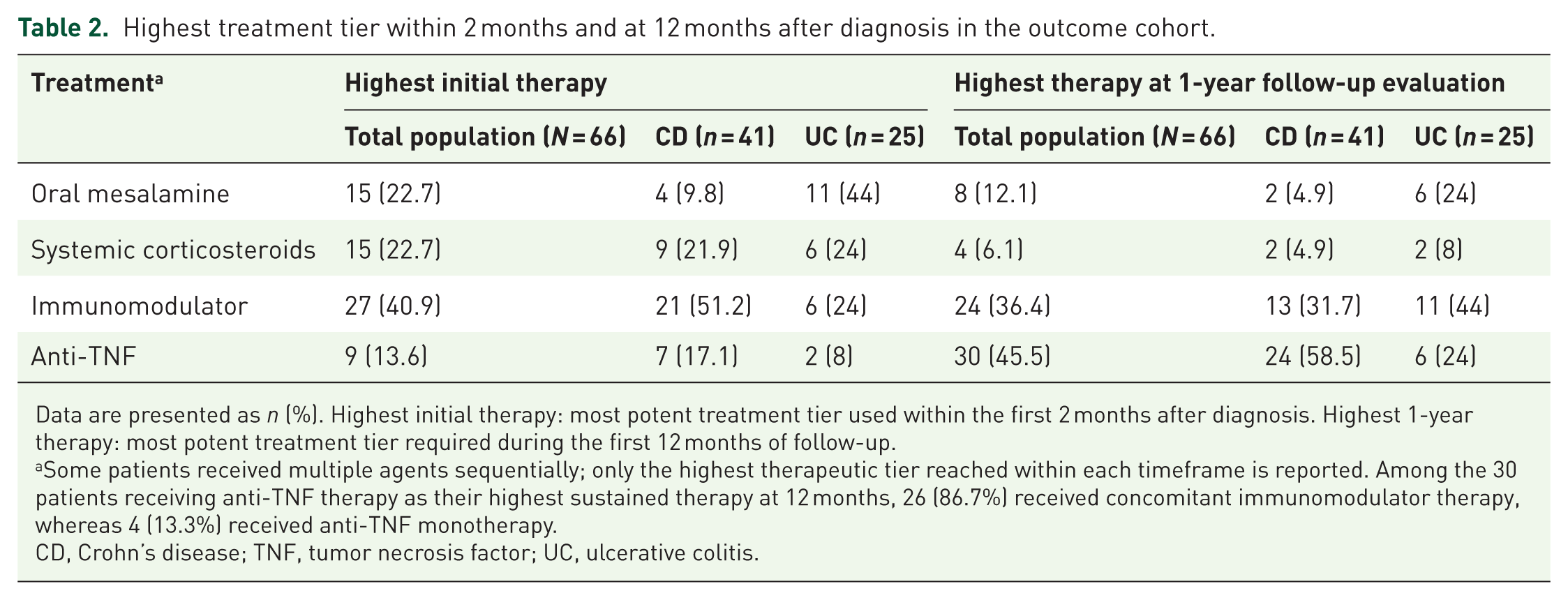
Data are presented as n (%). Highest initial therapy: most potent treatment tier used within the first 2 months after diagnosis. Highest 1-year therapy: most potent treatment tier required during the first 12 months of follow-up.
Some patients received multiple agents sequentially; only the highest therapeutic tier reached within each timeframe is reported. Among the 30 patients receiving anti-TNF therapy as their highest sustained therapy at 12 months, 26 (86.7%) received concomitant immunomodulator therapy, whereas 4 (13.3%) received anti-TNF monotherapy.
CD, Crohn’s disease; TNF, tumor necrosis factor; UC, ulcerative colitis.
At the 12-month follow-up, a significant therapeutic shift was observed, characterized by an escalation in biologic utilization and a concurrent reduction in corticosteroid and 5-ASA reliance. The proportion of patients receiving anti-TNF agents as the highest therapeutic tier increased markedly to 45.5% of the total cohort. This trend was particularly pronounced in CD, where 58.5% of patients were maintained on anti-TNF therapy. Conversely, the use of systemic corticosteroids as the primary maintenance therapy declined substantially to 6.1%, and the use of oral mesalamine decreased from 22.7% at baseline to 12.1% at 1 year.
In the Outcome Cohort, the median time from diagnosis to first anti-TNF dose was 3.0 months (IQR 1.0–6.0). Cumulatively, anti-TNF therapy had been initiated by 2, 3, 6, and 12 months after diagnosis in 9 (13.6%), 16 (24.2%), 21 (31.8%), and 30 patients (45.5%), respectively. All patients who received anti-TNF as their highest initial therapy within 2 months had received at least a brief course of conventional therapy (5-ASA and/or corticosteroids) before biologic initiation; none received anti-TNF as true first-line (top-down) therapy. Among patients receiving anti-TNF therapy at the 12-month assessment (N = 30, Table 2), 26 (86.7%) received concomitant immunomodulator therapy with azathioprine or 6-mercaptopurine, whereas 4 (13.3%) received anti-TNF monotherapy.
One-year outcomes
The clinical, biochemical, and endoscopic outcomes at 1 year post-diagnosis are detailed in Table 3. Overall, clinical remission was achieved in 52 out of 66 patients (78.8%), with rates of 75.6% (31/41) for CD and 84.0% (21/25) for UC. Steroid-free clinical remission was attained in 63.6% (42/66) of the cohort (58.5% CD, 72.0% UC), indicating successful corticosteroid tapering in the majority of responders.
Clinical outcomes at 1 year after diagnosis of the outcome cohort.

Data are presented as number/total assessed (%). Denominators vary because of missing data. Clinical remission was defined as CDAI <150 for Crohn’s disease and normalization of bowel habit with absence of bloody stool for UC. Steroid-free clinical remission was defined as clinical remission without corticosteroid use for ⩾4 weeks. Mucosal healing was defined as complete absence of mucosal ulceration for Crohn’s disease and Mayo Endoscopic Score of 0 for UC. Mucosal healing was assessed among the 53 patients (80.3%) who underwent endoscopic re-evaluation at 12 months. Sensitivity analysis bounds: 50.0% (worst-case) to 69.7% (best-case).
CDAI, Crohn’s disease activity index; CRP, C-reactive protein; IBD, inflammatory bowel disease; UC, ulcerative colitis.
Regarding objective markers of inflammation, CRP normalization (<5 mg/L) was achieved in 69.8% (44/63) of patients, while fecal calprotectin normalization (<150 µg/g) was observed in 61.1% (33/54) of evaluated cases. Furthermore, among the 53 patients who underwent endoscopic re-evaluation, mucosal healing was documented in 62.3% (33/53). This included 62.5% of the CD cohort and 61.9% of the UC cohort. Of note, endoscopic evaluation was not available for 13 of 66 patients (19.7%) at the 12-month time point, and CRP and fecal calprotectin data were missing in 4.5% and 18.2% of cases, respectively.
Endoscopic re-evaluation was performed in 53 of 66 patients (80.3%) in the Outcome Cohort. Endoscopy was protocolized at 6–12 months post-diagnosis as part of the treat-to-target strategy and was not solely symptom-driven. The 13 patients (19.7%) who did not undergo follow-up endoscopy were classified by reason: 6 (46.2%) had clinical remission with deferral by the treating clinician or patient, 4 (30.8%) cited financial constraints, and 3 (23.1%) declined endoscopy because they felt well. Endoscopic scores were assessed by the treating gastroenterologist; central review was not performed. In a sensitivity analysis examining the impact of missing endoscopy data, the mucosal healing rate ranged from 50.0% (33/66, assuming all missing patients had active disease) to 69.7% (46/66, assuming all missing patients had achieved mucosal healing), bracketing the per-protocol estimate of 62.3% (33/53).
TB reactivation occurred in 3 of 66 patients (4.5%) in the Outcome Cohort: 2 receiving infliximab and 1 receiving adalimumab. Notably, all three patients had negative baseline IGRA results and unremarkable chest radiography, thus not meeting criteria for isoniazid prophylaxis. TB manifested as cutaneous, pulmonary, and pleural disease at 23, 16, and 14 months post-anti-TNF initiation in three respective patients (two with CD, one with UC). Two cases were on combination anti-TNF + immunomodulator therapy at the time of diagnosis; the remaining patient was on anti-TNF monotherapy. Repeat IGRA testing was not performed at the time of TB diagnosis in any of the cases due to (i) per institutional protocol following ECCO recommendations, 18 IGRA re-screening is scheduled at annual intervals rather than at symptom presentation, and (ii) financial constraints precluding ad hoc IGRA in our resource-limited setting; chest radiography was used instead. IGRA conversion status at TB diagnosis, therefore, cannot be determined. Upon diagnosis, anti-TNF therapy was immediately discontinued, and all patients successfully completed standard anti-tubercular treatment. Rather than resuming anti-TNF agents, the two patients with CD were subsequently switched to ustekinumab, and the patient with UC was switched to tofacitinib; all three are currently clinically stable (Table S3). The small number of TB reactivation cases precludes a formal comparison between infliximab and adalimumab.
Serious infections (excluding TB reactivation) were reported in 6 of 66 patients (9.1%). In the UC cohort, one patient developed a lung abscess and one had septicemia. In the CD cohort, serious infections included septic arthritis of the knee (n = 1), septicemia (n = 1), and febrile neutropenia with bloodstream infection (n = 2). No infection-related mortality occurred. IBD-related surgery was required in two patients (3.0%), both with CD (4.9%), and no colectomies were performed in the UC group during the 1-year follow-up.
Discussion
This inception cohort study provides a contemporary profile of newly diagnosed IBD in Vietnam. While a recent Vietnamese multicenter retrospective study described the clinical course of IBD patients in comparison with a Korean cohort, 3 the present study extends these findings in several important respects. First, we employed an inception cohort design with systematic enrollment of consecutively diagnosed patients, reducing the selection bias inherent to retrospective case series. Second, all patients underwent protocolized TB screening with IGRA prior to immunosuppressive or biologic therapy, enabling a systematic assessment of TB-related safety outcomes. Third, mucosal healing was evaluated as a primary objective endpoint, consistent with current treat-to-target recommendations. 8 Finally, we specifically characterized and evaluated an accelerated step-up therapeutic strategy, providing real-world evidence on the feasibility of early biologic escalation in a TB-endemic, resource-constrained setting. Newly diagnosed patients frequently presented with advanced and complicated disease, yet a treat-to-target strategy incorporating early escalation to biologic therapy was associated with high rates of steroid-free clinical remission and mucosal healing at 1 year. Overall, 63.6% of patients attained steroid-free clinical remission, and 62.3% achieved mucosal healing, outcomes that appear broadly comparable to contemporary international cohorts despite the resource-constrained setting.
Phenotype and diagnostic delay
In this cohort, complicated CD behavior was frequent: stricturing (B2) and penetrating (B3) phenotypes together accounted for 57.6% of cases, and 25.0% of CD patients had already undergone intestinal resection before referral. Similarly, the burden of UC was substantial, with 63% presenting with extensive colitis and 45.7% classified as having severe disease. These figures are consistent with recent data from four Vietnamese tertiary centers, which reported similarly high rates of complicated CD and severe UC, 3 but contrast with Western inception cohorts where uncomplicated inflammatory CD (B1) accounts for about 74% of cases at diagnosis. 19 Additionally, none of our patients reported a family history of IBD, reinforcing the hypothesis that environmental factors associated with rapid urbanization may play a more dominant role than genetics in our population. 1
The high rates of complications and prior surgery in CD may be partly attributed to diagnostic delay, given that the median time from symptom onset to diagnosis in this study was 12 months. This paradox of “prior resection” in newly diagnosed patients reflects a specific challenge in our setting. Many patients underwent emergency surgery for complications like perforation or obstruction at lower-level hospitals before referral and definitive IBD confirmation. This underscores the critical impact of diagnostic delay, where disease progression necessitates surgical intervention even before the initiation of medical therapy. For a quarter of CD patients, the therapeutic window for medical management had closed before diagnosis was established—underscoring the urgent need for improved IBD awareness and earlier referral pathways.
The diagnostic delay is multifactorial. Historically, IBD was considered rare in Vietnam, leading to a low index of suspicion among primary care physicians. Initial symptoms are frequently misattributed to common tropical infections or hemorrhoids, resulting in repeated courses of antibiotics or self-medication before a referral is initiated. Furthermore, the challenge of distinguishing CD from infectious mimics, particularly ITB, contributes to this delay. Differentiating CD from ITB remains a significant challenge in TB-endemic regions. In Asian countries, 17.9% of CD patients are initially misdiagnosed as ITB. 20
The diagnostic pathway in TB-endemic regions is frequently complicated by the need to exclude infectious etiologies, often necessitating empirical anti-TB therapy before immunosuppression can be considered. Consistent with Asian consensus guidelines, which allow for a therapeutic trial of anti-TB therapy when differentiation is difficult, 21 11.3% of our baseline CD cohort received empirical anti-TB treatment before IBD confirmation. While clinically necessary, this approach is not without consequence. Evidence from India suggests that empirical anti-TB therapy in patients with CD is associated with an increased risk of complications and need for surgery. 22 Two strategies may mitigate this: first, IBD education programs targeting community healthcare workers to reduce diagnostic delay; and second, strict adherence to the recommended 8–12-week limit for empirical anti-TB trials, with prompt re-evaluation thereafter. 21 In our cohort, patients undergoing empirical anti-TB therapy were strictly monitored and re-evaluated after 8–12 weeks. The definitive diagnosis of CD was subsequently confirmed based on the lack of clinical or endoscopic response to anti-TB agents, negative results on repeated microbiological tests (including tissue culture and PCR), and persistent or progressive lesions characteristic of IBD on repeat endoscopy. Furthermore, the accuracy of the final diagnosis was corroborated by the favorable response to subsequent IBD-specific therapies in all these cases.
Treatment strategy
Our treatment data illustrate how an accelerated step-up approach can be applied in a middle-income, TB-endemic setting. Anti-TNF agents were used as the highest initial therapy in 13.6% of patients within the first 2 months, increasing to 45.5% overall and 58.5% among CD patients by 12 months. This utilization is higher than that reported in earlier Asian inception cohorts. 4 This likely reflects the substantial burden of complicated disease in our population, including the high prevalence of stricturing/penetrating behavior and prior intestinal resection. For these high-risk patients, particularly those with prior surgeries, the early introduction of biologics, reflected in a median time-to-anti-TNF of 3.0 months (IQR 1.0–6.0), aligns with international recommendations to effectively prevent postoperative recurrence. 23
The most notable shift occurred during follow-up. By the 1-year mark, biologic use had increased more than threefold to 45.5% overall, and to 58.5% for CD patients. This trend reflects the adoption of an “accelerated step-up” strategy. Although Western guidelines increasingly support a top-down approach for selected high-risk patients,13,14 economic constraints in Vietnam and comparable Asian countries often necessitate starting with conventional therapies. 24 Asian consensus guidelines, however, endorse an accelerated step-up approach as a pragmatic alternative. 25 Our data suggest that while a “step-up” approach was technically followed, the severity of disease at presentation necessitates rapid escalation to biologics. This observation is consistent with recent Asian data showing increasing biologic utilization 24 and with previous data from our center suggesting that early biologic introduction improves outcomes. 3 Our treatment strategy also aligns with recent international guidance: the AGA 2024–2025 Living Guidelines and ECCO 2024 recommendations support early use of advanced therapies in moderate-to-severe IBD rather than thiopurine monotherapy.13,14,26 In this context, the rapid escalation observed in our cohort (median time-to-anti-TNF 3.0 months; 45.5% of the Outcome Cohort on anti-TNF by 12 months) reflects a pragmatic convergence between international recommendations and real-world constraints in Vietnam.
Outcomes and safety
Despite advanced disease at presentation, accelerated step-up therapy resulted in encouraging short-term outcomes. Overall, 78.8% of patients in the Outcome Cohort achieved clinical remission and 62.3% achieved mucosal healing at 1 year. These mucosal healing rates are comparable to previous Vietnamese multicenter data. 3 Biochemical control was also achieved in most evaluable patients, with CRP normalization in 69.8% and fecal calprotectin normalization in 61.1%. Taken together, these findings suggest that timely therapeutic escalation within a structured management framework may be associated with outcomes broadly comparable to international cohorts, even in resource-constrained settings.
Regarding safety, TB reactivation occurred in 4.5% of our cohort (3/66), a rate consistent with previous Vietnamese data (7.1%), 3 and within the range reported in East Asian IBD populations receiving anti-TNF therapy. 27 A critical finding was that all three cases had negative baseline IGRA results, yet developed TB 14–23 months after biologic initiation. This observation carries several important clinical implications. First, a single negative IGRA at baseline may not reliably exclude the risk of TB reactivation during anti-TNF therapy in high-endemic settings. This likely reflects the limited sensitivity of IGRA for detecting LTBI in populations with high background exposure, where intermittent or low-level Mycobacterium TB exposure may not elicit a measurable interferon-gamma response at the time of testing. Consequently, none of the three patients met criteria for isoniazid prophylaxis, and baseline chest radiography was unremarkable, leaving no clinical indicator to flag their subsequent risk. Second, the relatively prolonged interval between biologic initiation and TB diagnosis (14–23 months) suggests that these events may represent either de novo infection acquired during immunosuppression or reactivation of latent infection that was undetectable by baseline screening. This temporal pattern indicates that the risk of TB is not confined to the early post-initiation period but extends throughout the duration of anti-TNF therapy. Third, the diversity of TB presentations in our cohort—cutaneous, pulmonary, and pleural—underscores that reactivation may manifest at extrapulmonary sites, necessitating a high index of clinical suspicion that extends beyond routine chest radiography surveillance.
These findings are consistent with the ECCO recommendation for annual re-screening with IGRA and chest radiography in patients receiving anti-TNF therapy in intermediate-to-high TB incidence areas. 17 While our data do not directly evaluate the efficacy of serial IGRA testing—as systematic re-screening was not performed in this cohort, and indeed repeat IGRA was not feasible at the time of TB diagnosis in any of our three cases due to resource constraints—the observation that all three reactivation cases had negative baseline IGRA supports the rationale for longitudinal TB surveillance beyond a single pre-treatment assessment. However, real-world implementation of this longitudinal surveillance remains distinctly suboptimal; recent Indian data revealed that annual latent TB screening was performed in only 27.2% of patients receiving advanced therapies for over a year.28,29 Our findings suggest that treat-to-target strategies and biologic therapy can be effectively implemented even in resource-constrained and TB-endemic settings when supported by structured screening and close monitoring. Based on indirect evidence from our findings and expert opinion, we suggest that in settings with TB incidence exceeding 150 per 100,000 population, structured TB surveillance (combining annual IGRA where feasible and chest radiography) may be considered as part of routine biologic monitoring protocols, although the optimal screening strategy remains to be defined in prospective studies.
Limitations
The study has several limitations. First, it was conducted at a single tertiary referral center and is therefore prone to referral bias toward more severe and complex cases, which may limit generalizability to community settings. Second, the hybrid design incorporates a retrospective component, introducing the possibility of incomplete records and information bias despite the use of standardized extraction procedures. Our hybrid retrospective–prospective design imposes inherent limitations on harmonization of certain variables across arms. Notably, the time from symptom onset to diagnosis appeared shorter in the retrospective arm (median 5 vs 14 months in prospective). On review, this difference reflects ascertainment heterogeneity: in retrospective abstraction, this duration was often captured from clinical notes describing only the duration of the presenting episode (e.g., “diarrhea for 2 weeks before admission”), while the prospective protocol systematically queried the entire history of pre-diagnostic symptoms. The implausibly short retrospective intervals (31.7% recorded as ⩽1 month) corroborate this interpretation. We therefore caution that this specific variable should not be interpreted as an epidemiologic finding. All primary outcome variables (treatment receipt, mucosal healing, TB reactivation, surgery) were measured uniformly across both arms using objective criteria and are not subject to this ascertainment limitation. Third, the Outcome Cohort was relatively small (N = 66) and followed for only 12 months, which restricts subgroup analyses, limits statistical power for CD-versus-UC comparisons, and prevents assessment of long-term durability of response. Of the 60 patients excluded, 47 had not yet reached the 12-month time point (administrative censoring) and 13 were LTFU; importantly, baseline characteristics did not differ significantly between the outcome cohort and excluded patients (Table S1), arguing against major selection bias. Fourth, endoscopic evaluation was not available for 19.7% of the outcome cohort at 12 months, and CRP and calprotectin data were incomplete. If patients with missing endoscopy were more likely to have active disease, the observed mucosal healing rate of 62.3% may represent an overestimate. These missing data reflect real-world constraints inherent to this setting. Fifth, the study period partially overlapped with the COVID-19 pandemic (2020–2021), during which intermittent public health restrictions in Vietnam affected outpatient access and may have delayed scheduled follow-up visits for some patients. However, as a tertiary referral center with a dedicated IBD unit, continuity of biologic infusions and essential monitoring was maintained throughout the pandemic period, and no patients in the outcome cohort experienced treatment interruptions directly attributable to pandemic-related restrictions, although some follow-up appointments were rescheduled. Finally, the absence of a comparator group precludes causal inference regarding the effectiveness of the accelerated step-up strategy; the observed outcomes should be interpreted as descriptive rather than attributable to a specific intervention.
Conclusion
IBD in Vietnam is characterized by advanced phenotypes, substantial diagnostic delays, and high rates of pre-diagnostic surgery, driven largely by low disease awareness and the diagnostic overlap with ITB. An accelerated step-up strategy incorporating early anti-TNF escalation was associated with favorable 1-year outcomes, including steroid-free clinical remission in 63.6% and mucosal healing in 62.3% of patients. However, TB reactivation occurred in 4.5% of patients despite negative baseline IGRA screening, demonstrating that a single pre-treatment assessment may be insufficient in high-endemic settings and suggesting that protocolized, repeated TB surveillance throughout the course of biologic therapy may be important.
These findings may be relevant to clinicians managing IBD not only in Southeast Asia but also in other regions sharing similar epidemiological characteristics and resource constraints. Future efforts should prioritize shortening the diagnostic interval through targeted physician and public education, expanding access to biologic therapies, and integrating longitudinal TB monitoring strategies into routine biologic treatment protocols in endemic settings.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261455281 – Supplemental material for Advanced phenotypes and favorable 1-year outcomes with accelerated step-up strategy in newly diagnosed inflammatory bowel disease in a tuberculosis-endemic, resource-constrained setting
Supplemental material, sj-docx-1-tag-10.1177_17562848261455281 for Advanced phenotypes and favorable 1-year outcomes with accelerated step-up strategy in newly diagnosed inflammatory bowel disease in a tuberculosis-endemic, resource-constrained setting by Trung Hoang Dinh, Luan Minh Dang, Chuong Dinh Nguyen, Diem Thi-Ngoc Vo, Tien Manh Huynh, Thong Duy Vo, Hoang Huu Bui and Duc Trong Quach in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848261455281 – Supplemental material for Advanced phenotypes and favorable 1-year outcomes with accelerated step-up strategy in newly diagnosed inflammatory bowel disease in a tuberculosis-endemic, resource-constrained setting
Supplemental material, sj-docx-2-tag-10.1177_17562848261455281 for Advanced phenotypes and favorable 1-year outcomes with accelerated step-up strategy in newly diagnosed inflammatory bowel disease in a tuberculosis-endemic, resource-constrained setting by Trung Hoang Dinh, Luan Minh Dang, Chuong Dinh Nguyen, Diem Thi-Ngoc Vo, Tien Manh Huynh, Thong Duy Vo, Hoang Huu Bui and Duc Trong Quach in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-3-tag-10.1177_17562848261455281 – Supplemental material for Advanced phenotypes and favorable 1-year outcomes with accelerated step-up strategy in newly diagnosed inflammatory bowel disease in a tuberculosis-endemic, resource-constrained setting
Supplemental material, sj-docx-3-tag-10.1177_17562848261455281 for Advanced phenotypes and favorable 1-year outcomes with accelerated step-up strategy in newly diagnosed inflammatory bowel disease in a tuberculosis-endemic, resource-constrained setting by Trung Hoang Dinh, Luan Minh Dang, Chuong Dinh Nguyen, Diem Thi-Ngoc Vo, Tien Manh Huynh, Thong Duy Vo, Hoang Huu Bui and Duc Trong Quach in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-4-tag-10.1177_17562848261455281 – Supplemental material for Advanced phenotypes and favorable 1-year outcomes with accelerated step-up strategy in newly diagnosed inflammatory bowel disease in a tuberculosis-endemic, resource-constrained setting
Supplemental material, sj-docx-4-tag-10.1177_17562848261455281 for Advanced phenotypes and favorable 1-year outcomes with accelerated step-up strategy in newly diagnosed inflammatory bowel disease in a tuberculosis-endemic, resource-constrained setting by Trung Hoang Dinh, Luan Minh Dang, Chuong Dinh Nguyen, Diem Thi-Ngoc Vo, Tien Manh Huynh, Thong Duy Vo, Hoang Huu Bui and Duc Trong Quach in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors acknowledge the use of Gemini 3.1 Pro (Google) for English language editing assistance, and its integrated Nano Banana model for support in designing the visual abstract. All underlying concepts, data interpretation, and scientific ideas are strictly those of the authors. The authors take full responsibility for the final content, originality, and accuracy of the manuscript. No funding was received for the use of these tools.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.