
Abstract
Background:
Despite recent guideline recommendations on managing acute upper gastrointestinal bleeding (AUGIB), mortality rates have not substantially improved over the years.
Objectives:
We aimed to understand real-life pre-endoscopic assessment and management practices in AUGIB.
Design:
We conducted an international online survey from April to November 2023.
Methods:
Key domains captured respondents’ demographics and clinical practice location, definitions of hemodynamic instability, and pre-endoscopic assessment. We provided descriptive proportions of responses. Secondary analyses explored differences in responses based on years of clinical experience.
Results:
Among the 533 clinicians who completed the survey, 47.1% reported using a triage system for AUGIB, and only 60.4% applied risk stratification scores at the time of presentation. Normal saline and balanced crystalloid fluids were almost equally preferred for initial fluid resuscitation. Hemodynamically unstable patients were typically managed in emergency departments and/or intensive care units. Over 85% of respondents followed a restrictive blood transfusion strategy in stable patients, but this dropped to 50.3% in hemodynamically unstable cases. Among respondents, 34.3% did not routinely use prokinetics, and 27.6% avoided their use, even in cases of severe bleeding or suspected gastric emptying disorders. The majority (87.1%) prescribed proton pump inhibitors before endoscopy. For suspected variceal bleeding, 83.7% reported using vasoactive agents, and 74.3% reported administering prophylactic antibiotics. Younger clinicians were more likely to follow recent guidelines than those with over 15 years of clinical experience.
Conclusion:
We found considerable variation in the pre-endoscopic management of individuals with AUGIB. Overall adherence to international guidelines was inconsistent, which may have implications for patient outcomes.
Keywords
Introduction
Acute upper gastrointestinal bleeding (AUGIB) is a frequent and potentially life-threatening condition that requires prompt recognition and management. It represents a common cause of hospitalization, posing a significant burden to healthcare systems worldwide. 1 Patients experiencing significant blood loss can present with associated hemodynamic instability, which is a common complication and presentation of AUGIB. 2 Its occurrence is linked to adverse outcomes, including increased mortality rates, higher risk of rebleeding, need for pre-hospital blood transfusions, and adverse events associated with sedation.3–5
Despite major advancements in medical and endoscopic therapeutic options, mortality rates have not shown a substantial decline. 6 Factors such as patient demographics and comorbidities likely prevent the decrease in mortality. 7 Patients presenting with AUGIB are increasingly older, with significant comorbidities including cardiac, vascular, and renal disease, and use of antiplatelet or anticoagulant drugs is common. Moreover, although updated guidelines for managing AUGIB are regularly being published, adherence to expert recommendations appears to be moderate to low, even in tertiary care centers.8,9 Adequate pre-endoscopic management of AUGIB is critical for optimizing patient outcomes and survival, but variation in practice amongst clinicians within this domain is unclear.
This study is an international online survey evaluating clinical practices in the assessment and pre-endoscopic management of individuals presenting with suspected AUGIB. This provides an opportunity to gain insights into areas where guideline recommendations are limited. Moreover, identifying heterogeneity in practice patterns may highlight areas that require more consistent, high-quality care, with opportunities for standardizing care to improve patient outcomes. We aim to report on current clinical practices in the management of patients with suspected AUGIB before endoscopy and to compare these patterns based on years of clinical experience.
Methods
Study design
This study was an international, cross-sectional, online survey conducted following the recommendations of the Checklist for Reporting of Survey Studies (CROSS) guidelines 10 (Table S1). The survey was distributed between April and November 2023, employing a two-phase prospective data collection process.
Participants
The population of interest was comprised of physicians actively managing patients with AUGIB, including emergency medicine physicians, gastroenterologists, surgeons, anesthesiologists, and intensivists. We included clinicians with varying levels of clinical experience, spanning from trainees to specialists with over 20 years of clinical expertise.
Survey development
The questionnaire used in this study was developed by the study team specifically for this research and did not include any copyrighted or previously published tools requiring permission. A review of clinical practice guidelines on AUGIB management was performed. Additionally, content validity was ensured through an independent review by a panel consisting of 12 international experts. A pilot phase was then conducted, including 20 physicians, whose feedback was used to refine the final version of the survey.
Questionnaire contents
The survey included 33 questions, organized into four sections (Supplemental File 2). The first section was related to demographic data and levels of clinical experience, while the second section focused on the criteria used to define hemodynamic instability. The third section evaluated pre-endoscopic assessment and management patterns. In the last section, we addressed optimal timeframes for performing upper endoscopy in patients presenting with AUGIB. 9 This paper reports the results from the first three sections.
Distribution and data management
The survey was first distributed in person in April 2023 during the European Society of Gastrointestinal Endoscopy (ESGE) Days conference in Dublin, Ireland, where a QR code to the survey was displayed during the conference. Email invitations were sent to national and international gastrointestinal societies to seek endorsement of the survey. Official endorsements were received from the Hungarian Society of Gastroenterology, the French Society of Gastroenterology, the French Society of Endoscopy (SFED), the Spanish Society of Gastrointestinal Endoscopy (SEED), the Romanian Society of Gastroenterology, the Czech Gastroenterology Society, the Inter-American Society of Digestive Endoscopy (SIED), and the Association of Scientific-Medical Societies of Chile. The survey was also distributed through Endoaula, a virtual endoscopy academy with over 2000 endoscopists from Spain and Latin America, as well as the co-authors distributed it among their networks. It was also disseminated during the United European Gastroenterology Week in Copenhagen, Denmark, in November 2023.
Data were collected and managed through the Research Electronic Data Capture (REDCap) platform.11,12 Each participant’s response was de-identified to ensure anonymity and confidentiality. Only complete survey answers were included in the final analysis.
Statistical analysis
The primary analysis comprised a descriptive evaluation of individual survey responses. Descriptive statistics were presented as proportions, as they involved categorical data. Secondary analyses explored differences in survey responses based on years of clinical experience. For comparison between categorical variables, Chi-square tests were performed. 13 The null hypothesis assumed no variability in practice patterns between groups of various levels of clinical expertise. A p-value of less than 0.05 was used to indicate statistical significance.
Results
This article reports results derived from a broader international survey project assessing various aspects of AUGIB management. Data related to endoscopy timing based on hemodynamic status have been previously reported in a separate publication. 9 The present study focuses specifically on pre-endoscopic evaluation and management practices, which have not been previously published.
Demographic data
Out of 867 participants, 533 (61.4%) completed the survey. The majority of responses originated from eight countries: France contributed 21.2% of respondents, followed by Spain (9.9%), Hungary (9%), the United Kingdom (8.8%), Denmark (6.4%), India (4.7%), Argentina (4.5%), and Romania (4.5%). For the detailed distribution of responses by country, see Table S2.
Gastroenterologists represented the majority of respondents (83.7%). More than half of the participants worked in university-affiliated hospitals (54.6%) and treated over 100 hospitalized AUGIB patients annually (67.7%). Regarding clinical experience, 55.7% of participants reported less than 10 years of clinical practice, 21.3% had 11–20 years, and 22.8% had over 20 years of clinical experience (Table 1).
Demographic data of survey respondents (n = 533).

AUGIB, acute upper gastrointestinal bleeding; ICU, intensive care unit.
The demographic characteristics of the study participants have been previously partly described in the companion publication focusing on endoscopy timing, 9 as both reports are derived from the same international survey dataset.
Practice location
Regarding clinical practice settings, 83.1% of respondents had access to 24-h emergency endoscopy, including weekends. Emergency interventional radiology was available to only 55.3% of respondents. Surgery was available in 96.8% of hospitals. Notably, 29.1% of hospitals lacked specific internal protocols or guidelines for the initial assessment of AUGIB patients (Table 2).
Information regarding the clinical practice location of survey respondents relevant to AUGIB patient management.
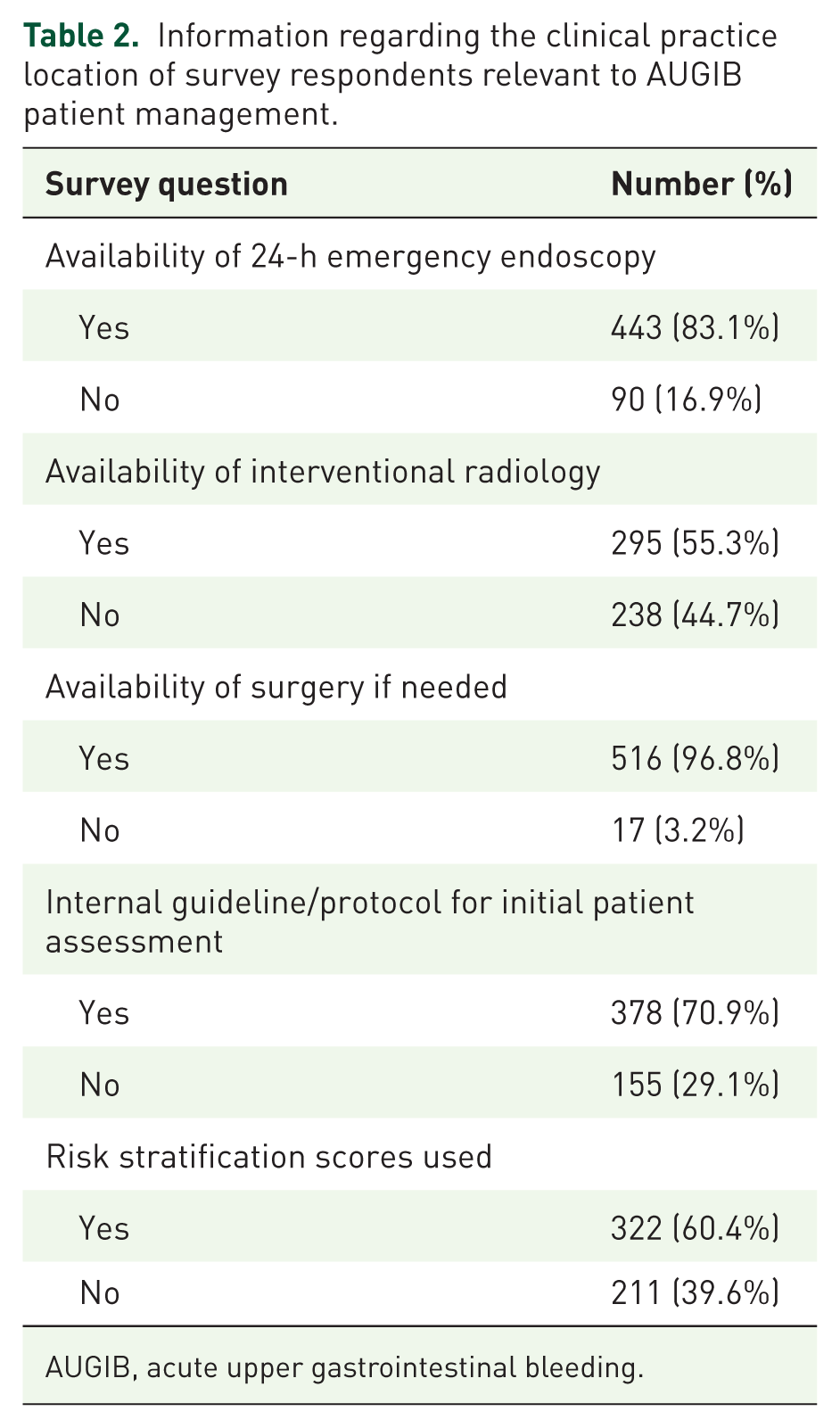
AUGIB, acute upper gastrointestinal bleeding.
Risk stratification and assessment
Triage systems comprise operational frameworks used in emergency settings to determine the urgency of care and allocation of resources. Less than half of the responders (47.1%) reported using a triage system at the time of presentation in patients with AUGIB. Of those, 49.8% were uncertain about which specific triage systems were used at their clinical practice location.
Regarding the initial assessment and management of hemodynamically unstable patients with AUGIB took place, most respondents reported that this occurred in the emergency medicine department (61.7%) and/or the intensive care/high-dependency unit (50.7%).
Only 60.4% of participating physicians used risk stratification scores to assess patients at the time of presentation, with the Glasgow-Blatchford score (GBS) being the most commonly used (72.7%). Details regarding risk stratification and pre-endoscopic assessment of patients presenting with AUGIB are summarized in Table S3.
Fluid resuscitation
In total, 90.1% of respondents reported that they ensure patients arrive at endoscopy with a peripheral cannula most or all of the time. For initial fluid resuscitation in AUGIB, 0.9% saline solution and/or balanced crystalloid fluids, such as lactated Ringer’s, were almost equally preferred (40.9% and 39.6%, respectively). In comparison, 16.5% of responders stated that either crystalloid is an acceptable option (Figure S1).
The preferred rate of fluid resuscitation varied, with 40.2% of physicians stating it depended on the patient’s hemodynamic status. Overall, 30.4% adhered to a conventional fluid resuscitation strategy, aiming to maintain a systolic blood pressure (BP) of around 90 mmHg. In comparison, 22.3% adjusted the rate of fluids based on the suspected etiology of the source of bleeding (Figure S2).
Regarding circulatory aims during resuscitation in hypotensive patients with suspected AUGIB, the most frequently selected targets were maintaining systolic BP >90 mmHg (30.8% of respondents) and >100 mmHg (30%). Achieving a mean arterial pressure of >60 mmHg was chosen by 13.1%, while normalizing the patient’s systolic BP to their habitual level was selected by 7.1%. There was statistically significant variability in the primary circulatory targets across levels of clinical experience (p < 0.001). Less experienced clinicians (<10 years of clinical experience) tended to focus more on achieving systolic BP >90 mmHg and mean arterial pressure >60 mmHg. In contrast, more experienced physicians (>10 years of clinical experience) demonstrated a broader range of preferences, with a notable inclination toward targeting systolic BPs >100 and/or >90 mmHg. For a more detailed presentation of survey responses in this section, see Table 3.
Responses addressing fluid resuscitation strategies in patients presenting with AUGIB.
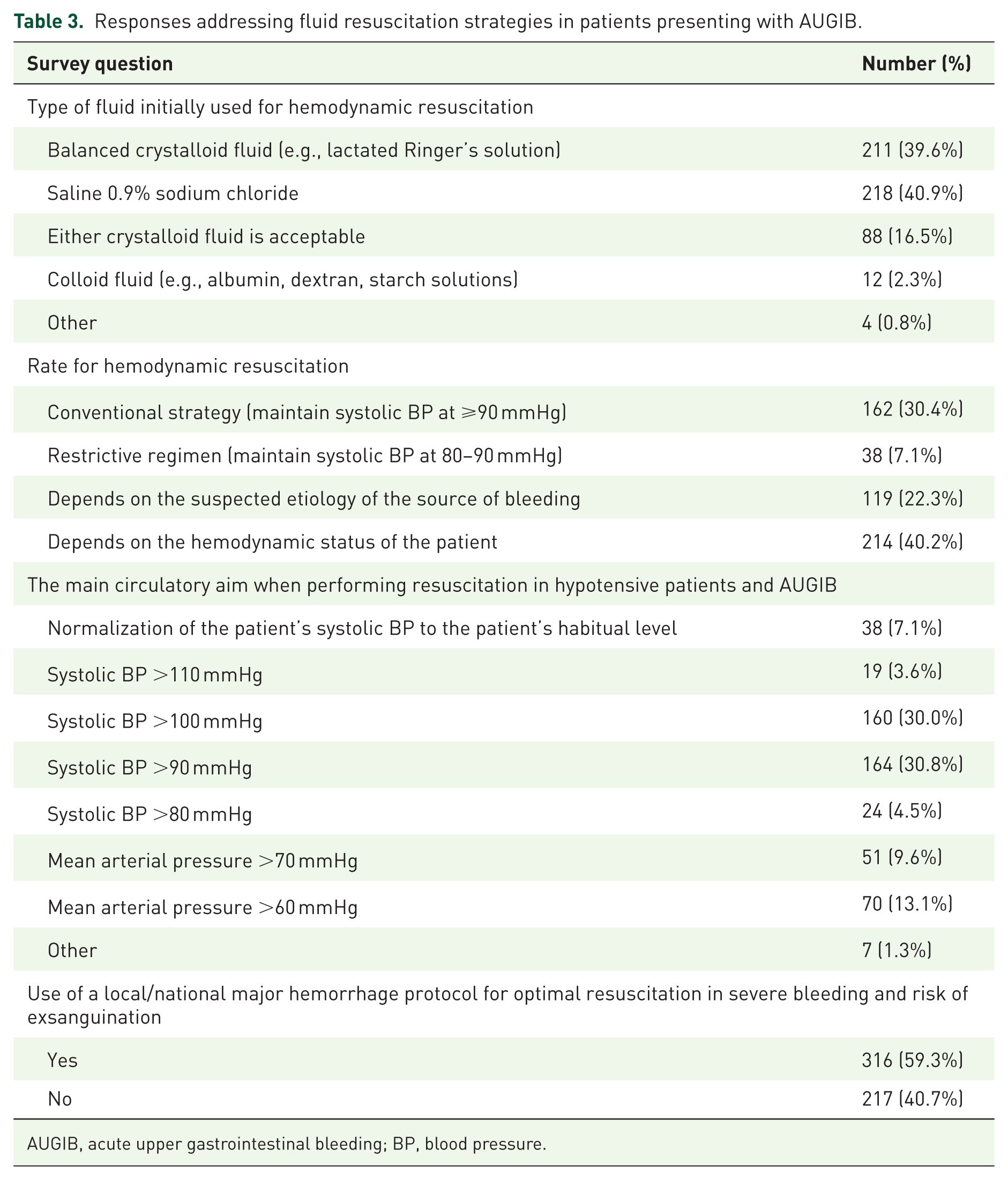
AUGIB, acute upper gastrointestinal bleeding; BP, blood pressure.
Blood transfusion strategies
For patients with severe bleeding and suspected risk of exsanguination (namely those presenting with hypotension and ongoing hematemesis or melena), only 59.3% of respondents reported following local or national major hemorrhage protocols to ensure optimal resuscitation.
When inquired about following a restrictive blood transfusion strategy, defined as a hemoglobin threshold of ⩽7–8 g/dL prompting blood transfusions, answers varied based on the hemodynamic status of patients. In hemodynamically stable cases, most respondents (85.9%) adhered to a restrictive approach to blood transfusions most or all of the time. In hemodynamically unstable patients, only 50.9% of participants followed a restrictive blood transfusion strategy (Figure 1).
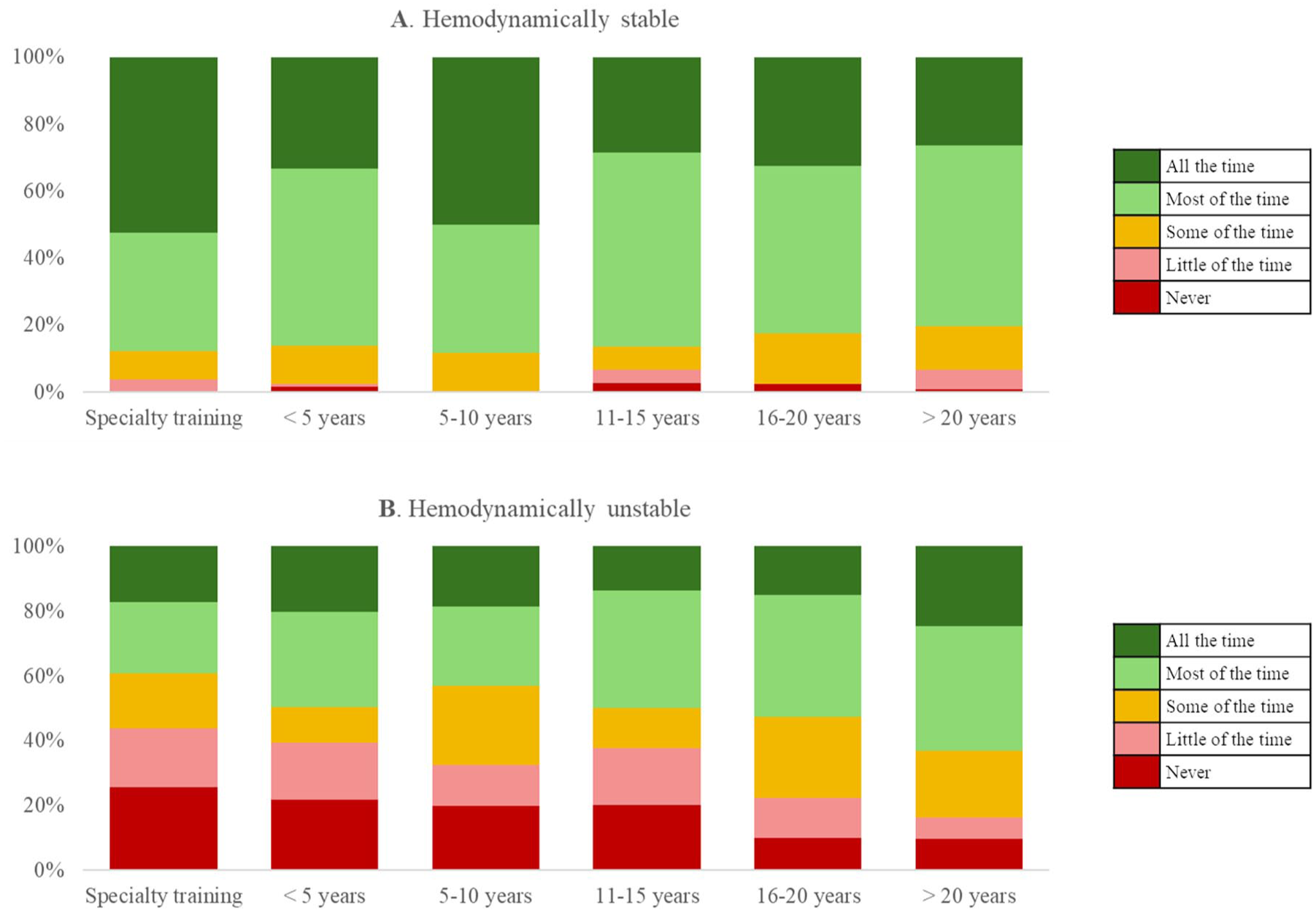
Survey responses stratified by years of clinical experience, assessing adherence to a restrictive blood transfusion strategy in (a) hemodynamically stable patients, (b) hemodynamically unstable patients.
Pre-endoscopy medications
A total of 34.3% of respondents reported not routinely using prokinetics before endoscopy in AUGIB patients (never or little of the time). Moreover, 27.6% reported not commonly using them even in cases involving severe bleeding or known gastric emptying disorders. Proton pump inhibitors (PPIs) were administered before performing upper gastrointestinal endoscopy in all or most cases by most respondents (87.1%). For suspected variceal bleeding, 83.7% of physicians used vasoactive agents in all or most cases (Figure S3).
The majority of respondents reported giving antibiotics before endoscopy in all or most cases of suspected variceal hemorrhage (74.3%). There was statistically significant variability in the use of antibiotics for suspected variceal bleeding by clinicians’ experience level (p < 0.001). Junior doctors (<10 years of clinical experience) were significantly more likely to use antibiotics consistently, with the majority reporting use most or all of the time. In contrast, more senior clinicians (>10 years of experience) demonstrated more varied practices, with a higher proportion reporting using pre-endoscopy antibiotics only a little of the time or never (Figure S4).
The detailed responses to questions included in this subsection are shown in Table 4.
Detailed responses regarding the pre-endoscopic use of medications in managing AUGIB.
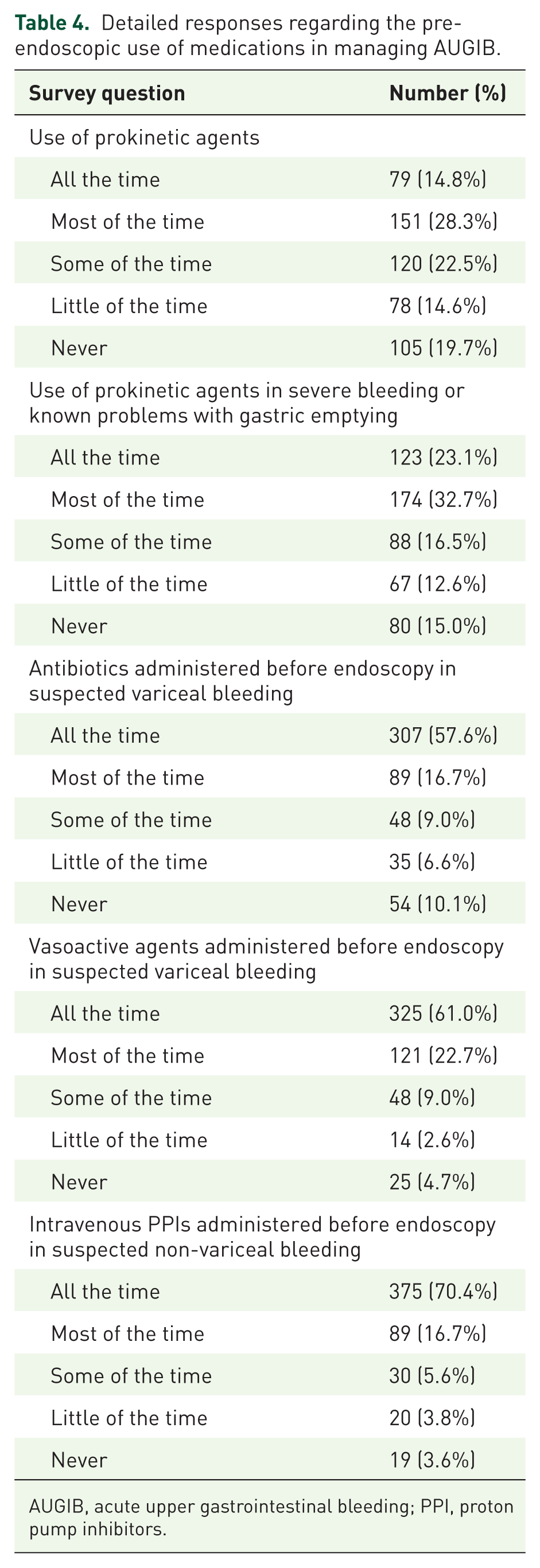
AUGIB, acute upper gastrointestinal bleeding; PPI, proton pump inhibitors.
Sedation and oro-tracheal intubation
Endoscopy is typically performed under moderate sedation in almost half (46%) of patients presenting with AUGIB, with oro-tracheal intubation under general anesthesia being less common (22.9%; Figure 2).

Survey responses addressing the frequency of performing upper gastrointestinal endoscopy under (A) sedation and (B) oro-tracheal intubation.
Discussion
This international survey provides an assessment of current clinical practices in the evaluation and pre-endoscopic management of patients with suspected AUGIB. Despite the availability of regularly updated guidelines, our findings revealed significant variability in practice patterns, particularly in patient triage and risk stratification, fluid resuscitation and blood transfusion strategies, and pre-endoscopy pharmacological interventions.
In our survey, almost all hospitals reported access to surgery, while emergency interventional radiology was available in only about half of the centers. This finding is notable, given that surgery is typically regarded as reserved for cases in which both endoscopic and radiological interventions have failed in the management of AUGIB. The broader availability of surgery compared with interventional radiology reflects resource differences across hospitals, with surgical teams often more universally available than dedicated radiology services. This discrepancy underscores substantial heterogeneity in treatment availability across centers, with important implications for patient outcomes.
One significant challenge in the initial assessment of AUGIB patients is the lack of a standardized definition of hemodynamic instability. A recent systematic review of the literature performed by our study group found that hemodynamic instability is commonly defined using basic parameters such as systolic BP <100 mmHg and/or heart rate >100 beats/min 2 ; however, broader definitions may also incorporate clinical features such as syncope, orthostatic hypotension, or signs of organ hypoperfusion. This heterogeneity was further reflected by the findings of this survey, where physicians reported varying criteria to define instability, ranging from isolated vital sign abnormalities to more complex clinical evaluations. This variability may have significant clinical implications, as the presence of hemodynamic instability directly influences therapeutic management decisions, including the rate of resuscitation, level of care (ward vs high-dependency or intensive care unit), and timing of endoscopy.
Three scoring systems have been primarily studied for pre-endoscopic risk stratification: the GBS, the Rockall score, and AIMS65.14–16 Data suggest that the GBS is superior in identifying low-risk patients who can be safely discharged and managed with outpatient endoscopy, potentially reducing the need for hospital admission and in-hospital endoscopy, and thereby reducing resource utilization.17–19 Both the ESGE and the American College of Gastroenterology advocate for its use in stratifying patients with AUGIB.20,21 Despite this, real-world adherence remains limited, with only 40% of respondents reporting routine use of risk scores at presentation, raising concerns about their feasibility in high-volume clinical settings. As an interesting future direction, a machine learning model was found to outperform these conventional risk scores. Trained on a large international cohort comprised of AUGIB patients, the model demonstrated superior accuracy in predicting blood transfusion needs, hemostatic intervention, and mortality, aiding in the identification of very-low-risk patients.22,23 The integration of such models, automatically calculated from electronic health records, could facilitate broader adoption of risk stratification in clinical practice.
Recent comparative studies suggest that the performance of pre-endoscopic risk stratification tools may vary according to the bleeding source. In non-variceal bleeding, AIMS65, GBS, and Rockall score showed good predictive accuracy for mortality, the need for blood transfusion, and endoscopic intervention, whereas in variceal bleeding, AIMS65 demonstrated superior predictive performance. However, all three scoring systems showed limited ability to reliably predict rebleeding 24 and no single scoring system consistently outperformed others across all outcomes.24,25 Furthermore, recent real-world studies highlighted that the implementation of risk prediction models in clinical practice remains challenging due to moderate predictive accuracy, heterogeneity in patient populations, and differences in healthcare settings and available resources. 26
For initial fluid resuscitation, current European guidelines recommend crystalloid solutions in cases presenting with hemodynamic instability. 20 Most physicians participating in our survey adhered to these recommendations, with over 85% favoring 0.9% saline solution and/or balanced crystalloid solutions, such as lactated Ringer’s. However, a significant challenge in clinical practice lies in the marked variability in the definition of hemodynamic instability. Previous studies examining its prevalence in patients with gastrointestinal bleeding have also highlighted this heterogeneity. 2 While some authors define hemodynamic instability as systolic BP below 100 mmHg and/or a heart rate above 100 bpm, others include additional criteria, such as syncope, orthostatic changes, or evidence of organ hypoperfusion. 9 This lack of consensus represents a critical issue, particularly as the guidelines themselves do not clearly specify the criteria for defining hemodynamic instability.
This observed variability is further reflected in fluid resuscitation strategies. While some tailor their approach to patients’ hemodynamic status or adjust fluid administration rates based on suspected bleeding etiology (variceal vs non-variceal), others adhere to more standardized fluid resuscitation protocols, such as maintaining a systolic BP of at least 90 mmHg. These findings highlight the ongoing debate regarding fluid resuscitation approaches, with this current knowledge gap being underscored even by the most recent ESGE guidelines on AUGIB. 20
Physicians’ approach to blood transfusions represents another critical issue. Restrictive transfusion protocols (blood transfusions prompted by a hemoglobin level below 7 g/dL) were found to reduce the overall all-cause mortality and rebleeding risk without affecting the likelihood of ischemic events.27,28 However, in patients with cardiovascular comorbidities or associated hemodynamic instability, further research is still needed to assess the safety of this approach. A more individualized transfusion framework with higher thresholds is recommended for this high-risk cardiovascular patient population by both European and American guidelines.20,21 Our survey highlighted the implementation of this personalized approach in clinical practice. While over 85% of respondents reported usually adhering to a restrictive blood transfusion protocol, only 50% of respondents employed the same strategy in patients with significant cardiovascular disease or hemodynamic instability. This observation is consistent with the fact that patients with severe hemodynamic instability were rarely included in pivotal trials evaluating restrictive transfusion strategies, highlighting the need for cautious extrapolation in this subgroup.
Regarding the use of pre-endoscopy prokinetic agents, guidelines recommend a 250 mg erythromycin infusion before endoscopy, as it may decrease the need for a second-look endoscopic evaluation and shorten hospitalization.21,29 European guidelines recommend its use only in cases exhibiting clinically severe or ongoing AUGIB. 20 Our survey found that over a third of clinicians do not routinely administer prokinetics before endoscopy, and more than a quarter avoid them even in cases of severe bleeding or documented gastric emptying disorders. Contributing factors to this significant variability in real-world clinical practices may include varying availability of erythromycin, fear of its potential serious side effects (e.g., prolonged QT interval), and perhaps a lack of perceived benefit. The risk-benefit profile of erythromycin use currently remains uncertain, given the insufficient conclusive evidence. 30
The ESGE Guideline recommends pre-endoscopic administration of PPIs in patients presenting with suspected non-variceal AUGIB, as it may help downstage endoscopic stigmata and thereby reduce the need for endoscopic hemostasis. 20 A recent Cochrane systematic review and meta-analysis assessing the utility of initiating parenteral PPI therapy in this patient population before endoscopy did not observe a reduction in mortality, recurrent bleeding, need for surgical intervention, length of hospital stay, or transfusion requirements. 31 Based on this, the American Guidelines have not found sufficient evidence to recommend routine pre-endoscopy PPI use. 21 Our survey found that, in current clinical practice, 90% of surveyed physicians frequently recommend the use of pre-endoscopic PPIs. This finding may reflect that most respondents were from Europe (66.6%).
Antibiotic prophylaxis with ceftriaxone for up to 5 days, as well as administration of vasoactive drugs (e.g., terlipressin, somatostatin, or octreotide) continued for 2–5 days, is recommended in patients with advanced cirrhosis in the setting of AUGIB by the American Association for the Study of Liver Disease (AASLD), Baveno VII Guidelines, and ESGE guidelines.32–34 Initiation of both therapies is strongly encouraged soon after patient presentation as part of the pre-endoscopic management. While 83.7% of physicians who answered our survey reported using vasoactive agents and 74.3% administered antibiotics before endoscopy in all or most cases, this still leaves a considerable proportion, up to one-quarter, who do not consistently follow these evidence-based guideline recommendations. This is particularly concerning given that vasoactive drugs and antibiotic prophylaxis have been shown to significantly lower the risk of acute all-cause mortality, improve bleeding control, and shorten hospital stay.35,36
Real-world data highlight the importance of patient characteristics and clinical context in influencing AUGIB outcomes. Older adults commonly present with features associated with greater healthcare resource utilization and worse outcomes, including higher comorbidity burden and more frequent use of antithrombotic treatment.37–39 These findings strongly suggest that outcomes can be influenced not only by endoscopy timing but also by early stabilization and appropriate initial care, given patient-specific factors. In this context, the variability in pre-endoscopic management observed in our study may have important implications, especially in high-risk populations.
Less than half of respondents reported routinely using sedation during endoscopy for AUGIB. Evidence from a recent propensity score-matched study suggests that sedation may reduce procedure time without increasing adverse event rates. 40 Oro-tracheal intubation under general anesthesia was even less commonly employed, with only approximately 23% of participants reporting its routine use. Currently, ESGE guidelines recommend prophylactic endotracheal intubation only in selected patients, such as those with ongoing hematemesis, agitation, or encephalopathy with impaired airway protection. 20 This recommendation is in line with results from observational data, which suggest that routine prophylactic intubation in severe AUGIB may be associated with increased risks of pneumonia, longer hospital stay, higher costs, and mortality compared with endoscopy performed without intubation.41,42
In a companion analysis from the same international survey focusing on endoscopy timing in patients presenting with AUGIB, we also found that clinicians tend to perform earlier endoscopy with increasing hemodynamic instability. Experienced clinicians in high-volume, university centers are more likely to favor early intervention, particularly in unstable patients. 9 These findings complement the present study, which highlights significant variability in pre-endoscopic management practices. Together, these results suggest that although clinicians recognize the need for urgent intervention in unstable patients, significant heterogeneity remains in the initial assessment and optimization prior to endoscopy.
While our study provides essential insights into common clinical practice patterns in the management of patients presenting with AUGIB, it is subject to certain limitations. The survey primarily included participants from European countries, with over 20% from France, and more than half of the respondents were affiliated with university-based hospitals. Consequently, the findings may primarily reflect European clinical practice patterns rather than global management of AUGIB, limiting generalizability to other areas. Regional differences in healthcare systems, access to endoscopy, availability of interventional radiology, and implementation of clinical guidelines may contribute to the important variability in practice. All these aspects may influence decisions regarding pre-endoscopic management and timing of interventions; therefore, caution is warranted when extrapolating these findings to non-European settings. Moreover, the recruitment strategy, which relied on dissemination through gastroenterology conferences, professional networks, and endoscopy-focused platforms, may have introduced selection bias. The study population was predominantly composed of gastroenterologists and clinicians working in university-affiliated or high-volume centers, potentially underrepresenting emergency physicians, intensivists, and clinicians practicing in non-academic settings who are also involved in the management of AUGIB. This selection bias may have influenced the observed practice patterns, as clinicians with a specific interest in endoscopy and those working in tertiary centers may be more likely to follow guideline-based care and have greater access to resources. In contrast, practice patterns in non-academic or resource-limited settings may differ substantially, potentially limiting the generalizability of our findings. Given our distribution strategy, the total number of clinicians who received the survey invitation is not known, so the response rate could not be calculated. This limits the ability to assess potential non-response bias, as physicians who chose to participate may differ from those who did not respond. Additionally, self-reported questionnaires are inherently prone to response bias, influenced by factors such as a tendency to align responses with perceived expectations rather than actual clinical practices, question wording, and recall errors.
Our findings highlight significant variability in the management of AUGIB, thus emphasizing the need for standardized protocols. Inconsistent application of triage systems and risk stratification scores may delay the implementation of appropriate interventions and increase resource utilization. These results also underscore the need to reinforce evidence-based practices, such as restrictive blood transfusion strategies and appropriate fluid resuscitation, to optimize clinical decision-making. Improving adherence to international evidence-based guidelines through continuous education and systematic implementation strategies could lead to more effective and standardized pre-endoscopic care.43–45 Emerging prediction models, scores, and machine learning-based approaches may improve risk stratification in the future; however, these tools still require broader external validation and assessment of their clinical applicability in the management of patients with AUGIB.
Conclusion
This international survey revealed notable variability in the approach to pre-endoscopic assessment and management of patients presenting with AUGIB. Overall adherence to international guidelines was inconsistent, which may have implications for patient outcomes.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261455285 – Supplemental material for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey
Supplemental material, sj-docx-1-tag-10.1177_17562848261455285 for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey by Mahmoud Obeidat, Diana-Elena Floria, Brigitta Teutsch, Zsolt Abonyi-Tóth, Stig B. Laursen, Marine Camus, Franck Verdonk, áron Vincze, Zsolt Bognár, Vasile Drug, Keith Siau, Ian M. Gralnek, Péter Hegyi and Bálint Erőss in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848261455285 – Supplemental material for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey
Supplemental material, sj-docx-2-tag-10.1177_17562848261455285 for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey by Mahmoud Obeidat, Diana-Elena Floria, Brigitta Teutsch, Zsolt Abonyi-Tóth, Stig B. Laursen, Marine Camus, Franck Verdonk, áron Vincze, Zsolt Bognár, Vasile Drug, Keith Siau, Ian M. Gralnek, Péter Hegyi and Bálint Erőss in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tiff-3-tag-10.1177_17562848261455285 – Supplemental material for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey
Supplemental material, sj-tiff-3-tag-10.1177_17562848261455285 for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey by Mahmoud Obeidat, Diana-Elena Floria, Brigitta Teutsch, Zsolt Abonyi-Tóth, Stig B. Laursen, Marine Camus, Franck Verdonk, áron Vincze, Zsolt Bognár, Vasile Drug, Keith Siau, Ian M. Gralnek, Péter Hegyi and Bálint Erőss in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tiff-4-tag-10.1177_17562848261455285 – Supplemental material for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey
Supplemental material, sj-tiff-4-tag-10.1177_17562848261455285 for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey by Mahmoud Obeidat, Diana-Elena Floria, Brigitta Teutsch, Zsolt Abonyi-Tóth, Stig B. Laursen, Marine Camus, Franck Verdonk, áron Vincze, Zsolt Bognár, Vasile Drug, Keith Siau, Ian M. Gralnek, Péter Hegyi and Bálint Erőss in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tiff-5-tag-10.1177_17562848261455285 – Supplemental material for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey
Supplemental material, sj-tiff-5-tag-10.1177_17562848261455285 for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey by Mahmoud Obeidat, Diana-Elena Floria, Brigitta Teutsch, Zsolt Abonyi-Tóth, Stig B. Laursen, Marine Camus, Franck Verdonk, áron Vincze, Zsolt Bognár, Vasile Drug, Keith Siau, Ian M. Gralnek, Péter Hegyi and Bálint Erőss in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-tiff-6-tag-10.1177_17562848261455285 – Supplemental material for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey
Supplemental material, sj-tiff-6-tag-10.1177_17562848261455285 for Clinical practice patterns in the pre-endoscopic management of individuals presenting with acute upper gastrointestinal bleeding: results of an international survey by Mahmoud Obeidat, Diana-Elena Floria, Brigitta Teutsch, Zsolt Abonyi-Tóth, Stig B. Laursen, Marine Camus, Franck Verdonk, áron Vincze, Zsolt Bognár, Vasile Drug, Keith Siau, Ian M. Gralnek, Péter Hegyi and Bálint Erőss in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We sincerely thank Szonja Anna Kovács, the REDCap administrator at Semmelweis University, for her assistance in facilitating the survey administration. We also extend our appreciation to Joaquin Rodríguez Sánchez for helping distribute the survey through Endoaula, a virtual endoscopy academy, and to Rodrigo Mansilla Vivar for his efforts in distributing the survey in South America.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.