
Abstract
Background:
Biologics and small-molecule therapies are widely used for ulcerative colitis (UC), but their comparative effectiveness in anti-tumor necrosis factor (TNF)-exposed patients is unclear.
Objectives:
To compare the effectiveness and safety of vedolizumab, ustekinumab, and tofacitinib in anti-TNF-experienced patients with UC.
Design:
Multicenter retrospective observational cohort study.
Methods:
A multicenter retrospective cohort of anti-TNF-experienced UC patients treated with vedolizumab (n = 260), tofacitinib (n = 149), or ustekinumab (n = 193) was analyzed. Partial Mayo Score (pMayo), endoscopic remission, and biomarker response were assessed at baseline, 12, 24, and 52 weeks, respectively. Inverse Probability of Treatment Weighting (IPTW) was applied to balance baseline characteristics, and longitudinal changes were analyzed using repeated-measures general linear models with post hoc corrections.
Results:
After IPTW adjustment, at week 52, clinical remission was highest with tofacitinib compared with ustekinumab (p < 0.001) and vedolizumab (p = 0.002). Steroid-free clinical remission showed a similar pattern (tofacitinib vs ustekinumab: p = 0.006; tofacitinib vs vedolizumab: p < 0.001). No significant differences in biochemical remission were found across groups at week 52 (p = 0.931). Endoscopic remission favored vedolizumab over ustekinumab and tofacitinib (p < 0.001). Subgroup analyses revealed superior tofacitinib performance in extensive colitis and in patients with ⩾2 prior biologic classes (vs vedolizumab: p = 0.089; vs ustekinumab: p < 0.001). Adverse events were infrequent and similar across groups.
Conclusion:
In anti-TNF-experienced UC patients, tofacitinib was associated with higher long-term clinical and steroid-free remission rates, ustekinumab showed intermediate effectiveness with a favorable safety profile, while vedolizumab was associated with higher endoscopic remission. These findings may help inform individualized, outcome-oriented treatment strategies, but they should be interpreted with caution and confirmed in prospective head-to-head studies.
Introduction
Ulcerative colitis (UC) is one of the two main phenotypes of inflammatory bowel diseases (IBD), a group of chronic, relapsing-remitting, immune-mediated disorders of the gastrointestinal tract. 1 In recent years, the treatment landscape for UC has evolved with the introduction of several novel biotechnological therapies targeting new specific inflammatory pathways implicated in the disease pathogenesis.2–4 The classes of biologic therapies currently recommended for moderate-to-severe UC include anti-tumor necrosis factor (TNF) agents (i.e., infliximab, adalimumab, and golimumab), anti-integrin antibodies, interleukin-12/23 inhibitors (IL-12/23), and, more recently, Janus kinase (JAK) inhibitors and sphingosine-1-phosphate receptor modulators.2,5–8 The advent of novel therapies has raised important questions regarding their comparative effectiveness and optimal sequencing of treatment. This issue is particularly relevant in anti-TNF-experienced patients, in whom treatment selection after anti-TNF failure remains a frequent and clinically challenging scenario. In this setting, several advanced therapies are available, but direct comparative data are still limited, making real-world (RW) comparative evidence especially important for guiding treatment positioning and sequencing.
Vedolizumab, a humanized α4β7 integrin monoclonal antibody, ustekinumab, an IL-12/23 inhibitor, and tofacitinib, a pan-JAK inhibitor, have each demonstrated efficacy in induction and maintenance therapy in the pivotal GEMINI 1, UNIFI, and OCTAVE trials, respectively.9–13 Their effectiveness has also been confirmed in recent large RW studies.14–16 However, head-to-head trials comparing these agents in patients with moderately to severely active UC are lacking. As a result, comparative efficacy has largely been explored through indirect analyses, such as network meta-analyses (NMAs).17–22 In addition, the few RW comparative studies available have been limited by small sample sizes. 23
Therefore, the aim of our study was to compare vedolizumab, ustekinumab, and tofacitinib in patients with UC who had failed or were intolerant to anti-TNF therapy, with the goal of providing evidence to inform treatment positioning within the therapeutic algorithm for UC.
Patients and methods
Study design and setting
In this multicenter retrospective observational study conducted in Italy, the medical records of patients with UC were retrospectively reviewed from 2019 to 2024 at multiple specialized gastroenterology and IBD care centers participating in the Italian Network for Inflammatory Bowel Diseases, to identify and extract variables of interest. Data were collected anonymously, with no possibility of tracing information back to individual patients. The study focused on anti-TNF-experienced patients who initiated treatment with vedolizumab, ustekinumab, and tofacitinib during this period, with available data at baseline and at 12, 24, and 52 weeks post-treatment initiation. Variables collected included demographic information (e.g., birth-assigned sex, age, smoking status), medical history (comorbidities, age at UC diagnosis, previous treatments undertaken), and clinical variables such as the partial Mayo score (pMayo), a non-invasive index including stool frequency, rectal bleeding, and physician’s global assessment, with a total score ranging from 0 to 9, 24 fecal calprotectin, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and endoscopy data.
This study adhered to the Declaration of Helsinki (1975) and the Italian Medicines Agency’s determination of March 20, 2008. Ethical approval was not required due to its retrospective, observational, and anonymized design. All data were strictly anonymized, analyzed in aggregate form, and could not be traced back to individual patients. The manuscript was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 25
Inclusion and exclusion criteria
Eligible participants were adults with a confirmed diagnosis of UC who did not respond or were intolerant to anti-TNF agents and had been prescribed a biologic or small-molecule therapy according to current guidelines. 6 Patients with uncertain diagnosis or undergoing differential diagnosis for other conditions (e.g., ischemic, infectious, or radiation colitis; microscopic or indeterminate colitis; or suspected Crohn’s disease) were excluded. Exclusion criteria included severe conditions such as fulminant colitis, acute severe UC, toxic megacolon, major colonic surgery (e.g., subtotal or total colectomy, proctocolectomy), and patients diagnosed with cancer within 6 months of baseline. In addition, patients whose baseline demographic or clinical characteristics could not be clearly determined were excluded to ensure accurate analysis of sex and other variables as potential confounders.
Treatment
Vedolizumab was administered at 300 mg intravenously at weeks 0, 2, and 6 (induction scheme), followed by 300 mg every 8 weeks (maintenance scheme). Ustekinumab was administered as a single intravenous infusion based on the patient’s body weight, namely 260 mg (⩽55 kg), 390 mg (55–85 kg), or 520 mg (>85 kg), followed by a subcutaneous injection of 90 mg after 8 weeks (induction scheme). Maintenance dosing consisted of 90 mg subcutaneously every 8 weeks. Tofacitinib was administered orally at 10 mg twice daily for 8 weeks (induction scheme), followed by 5 mg twice daily as maintenance.
Study outcomes
The primary aim was to evaluate intertreatment differences, comparing outcomes across the three treatments (VDZ, UST, and TOFA).
The primary endpoints were as follows:
- to assess the effectiveness of each drug in achieving clinical remission, defined as a pMayo ⩽1, 26 and steroid-free clinical remission at 12, 24, and 52 weeks from baseline. Steroid-free clinical remission was defined as clinical remission in the absence of systemic or low-absorbable corticosteroid use at the corresponding study visit.
- to assess the safety of each drug, assessed by recording adverse events in accordance with WHO classification criteria. 27
Secondary endpoints included the following:
- Sustained clinical remission and sustained clinical response, defined as the persistence of remission from 24 to 52 weeks, according to the criteria previously described.
- Biochemical remission at 12, 24, and 52 weeks, defined as fecal calprotectin level less than 250 μg/g and CRP <5 mg/L.
- Endoscopic remission at 52 weeks was defined as a Mayo endoscopic score <2.11,26
Statistical methods
All statistical analyses were conducted using SPSS Statistics (version 27.1; IBM Corp., Armonk, New York, USA). Continuous variables were reported as medians with interquartile ranges (IQRs) and compared using the Kruskal–Wallis test for non-parametric distributions. Categorical variables were presented as counts and percentages and analyzed using the Chi-square test or Fisher’s exact test, as appropriate.
Longitudinal changes in clinical and biochemical outcomes were assessed using a repeated-measures general linear model (GLM), with therapy type as the between-subject factor and timepoints as the within-subject factor. Mauchly’s test was used to evaluate the assumption of sphericity, with Greenhouse–Geisser corrections applied when necessary. Pairwise comparisons were adjusted for multiple testing using the least significant difference correction.
To account for baseline confounders and improve comparability between treatment groups, Inverse Probability of Treatment Weighting (IPTW) was applied using propensity scores estimated via a multinomial logistic regression model. Covariates included age at diagnosis, sex, smoking status, disease duration, prior therapies, UC extension, pMayo, inflammatory markers (ESR, CRP, fecal calprotectin), and comorbidities. Moreover, prior biologic exposure was defined as the number of distinct biologic classes previously used before index treatment (e.g., anti-TNF, anti-integrin, anti-IL-12/23), rather than the number of individual molecules within the same class.
Covariate balance before and after weighting was assessed using standardized mean differences (SMD), with SMD <0.10 indicating adequate balance. To enhance model stability and minimize the impact of extreme values, IPTW weights were truncated at the 1st and 99th percentiles, and patients with extreme weights were excluded to prevent bias and ensure the validity of the weighted estimates.
IPTW-adjusted analyses included repeated measures ANOVA (RM-ANOVA) for longitudinal pMayo score changes, generalized linear models (GLMs) to assess treatment response predictors, and pairwise therapy comparisons with Bonferroni and Games-Howell corrections, as appropriate. Sensitivity analyses included propensity score matching (PSM) and inverse probability of censoring weighting (IPCW) to evaluate the robustness of findings. Multivariate analyses were conducted using Wilks’ Lambda test to assess the global effect of time and its interaction with therapy type. Effect sizes were reported as partial eta squared (η2). For between-group comparisons at each timepoint, Bonferroni-adjusted post hoc tests were applied.
A two-sided p-value <0.05 was considered statistically significant for all analyses. Missing data were addressed using multiple imputation to mitigate potential bias and preserve statistical power. Prior to imputation, the structure of the missingness was assessed, and an arbitrary (non-monotonic) missing data pattern was identified, with missing values scattered across several variables rather than following a monotonic dropout or phase-wise structure. Variables with more than 50% missing observations were not imputed and were excluded from subsequent analyses to maintain analytic robustness. The imputation model assumed data were missing at random and included baseline variables showing imbalance across treatment groups, together with clinically relevant concomitant medications, namely age at study inclusion, age at diagnosis, smoking status, medical comorbidities, mesalamine use, corticosteroid use, previous biologic class exposure, infliximab exposure, golimumab exposure, baseline pMayo score, fecal calprotectin, and disease severity. Outcome variables were not included in the imputation model. A total of five imputed datasets were generated and analyzed, and the results were combined using Rubin’s rules. All analyses adhered to the STROBE guidelines for observational studies. 25
Results
Baseline characteristics
A total of 602 anti-TNF-experienced patients with UC were included in this analysis: 260 received Vedolizumab, 149 received tofacitinib, and 193 received ustekinumab. Overall, missingness was low, and no variable or outcome included in the analyses had more than 5% missing data. Figure 1 summarizes the study flowchart. Significant baseline differences were observed between the treatment groups, as shown in Table 1. Patients in the tofacitinib group were younger at both diagnosis and study inclusion. Medical comorbidities were more common in the Ustekinumab group.
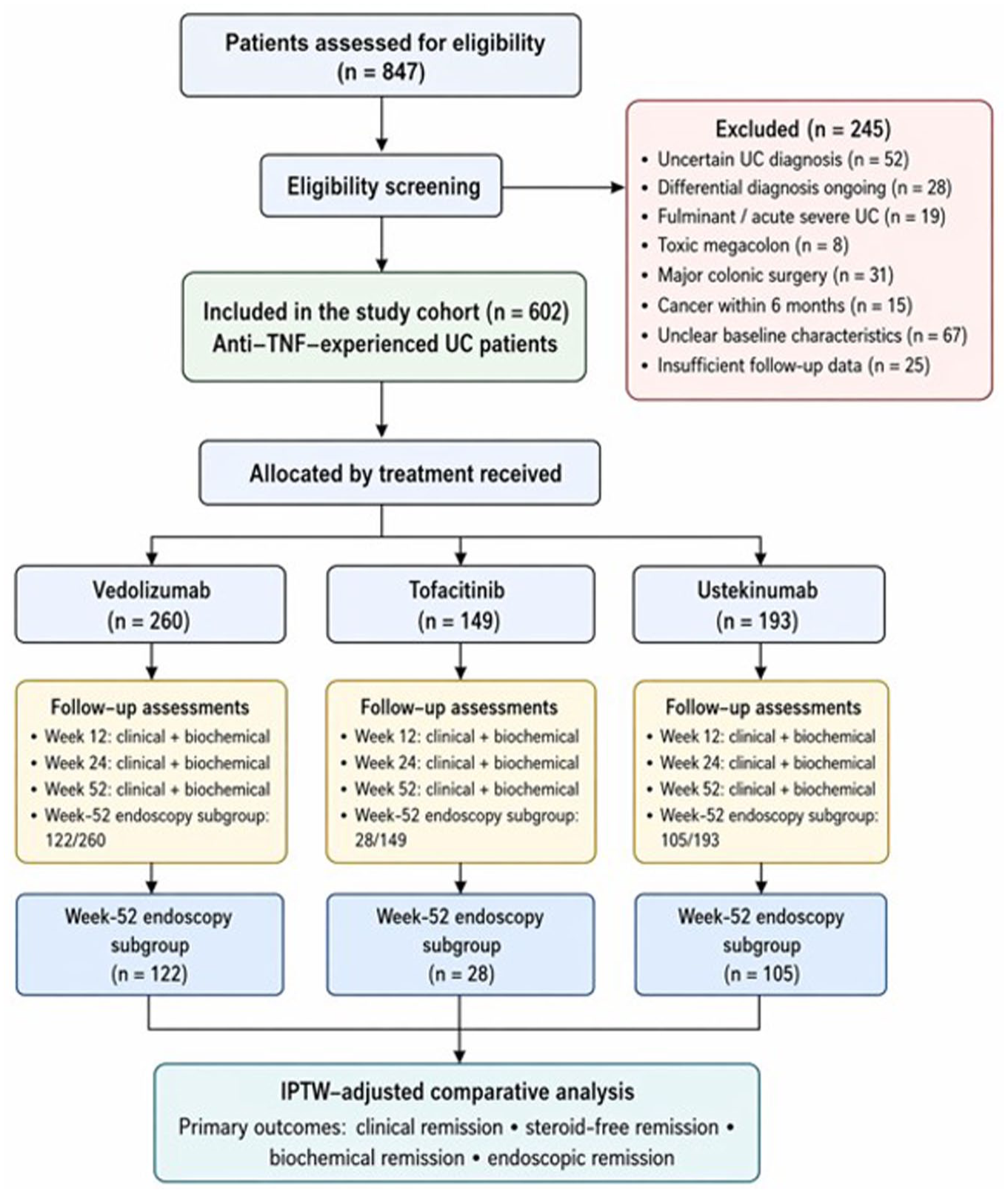
Flowchart of the study.
Baseline characteristics of the study population by treatment group (before IPTW).
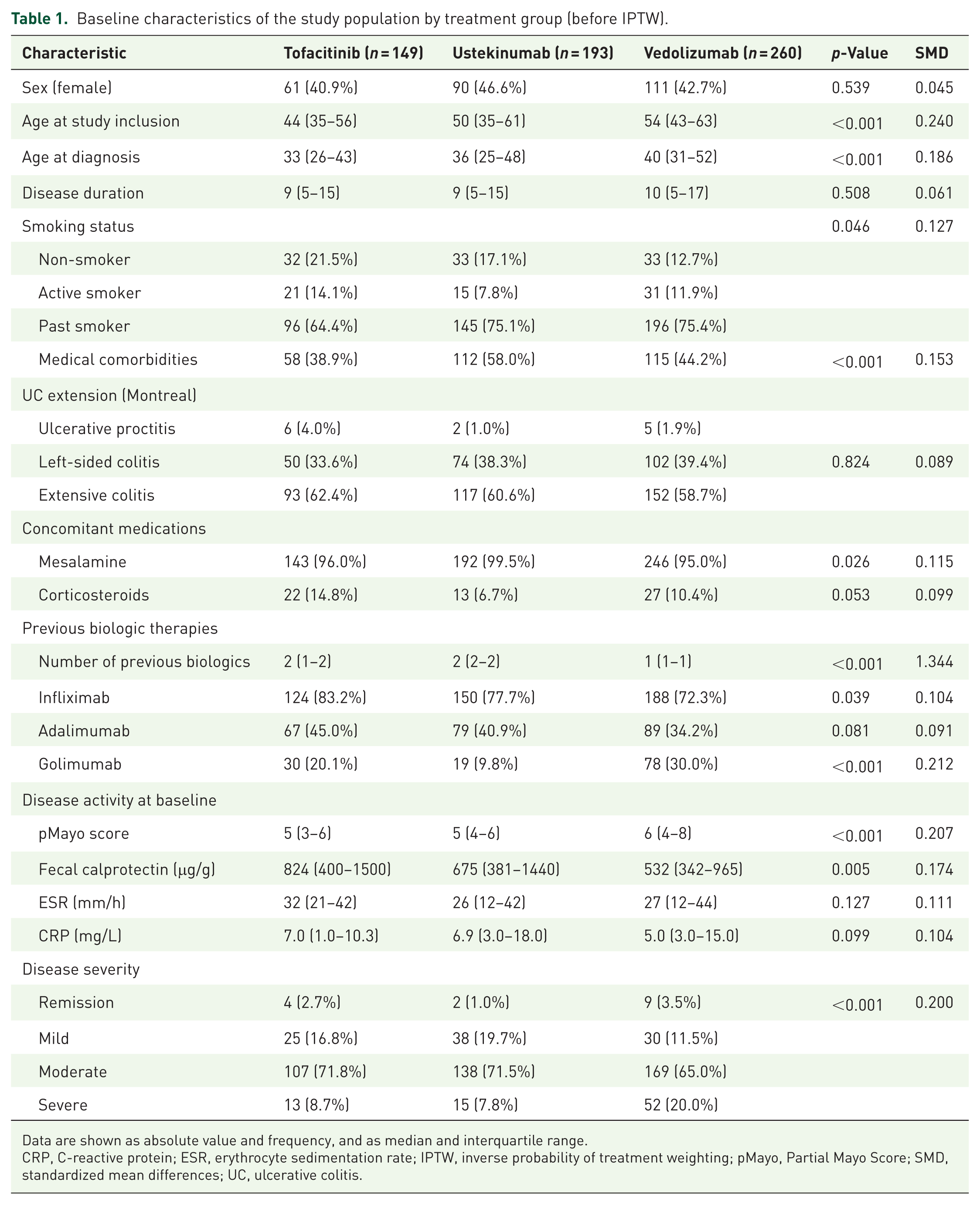
Data are shown as absolute value and frequency, and as median and interquartile range.
CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; IPTW, inverse probability of treatment weighting; pMayo, Partial Mayo Score; SMD, standardized mean differences; UC, ulcerative colitis.
A gradient of prior treatment exposure was observed, with ustekinumab patients having received the highest number of previous biologic classes (2, IQR 2–2), compared to tofacitinib (2, IQR 1–2) and vedolizumab (1, IQR 1–1). Disease activity at baseline, as measured by the pMayo score, was higher in the vedolizumab group, which also had the largest proportion of patients with severe disease, compared to the other groups.
Given these significant baseline differences, IPTW was applied to balance covariates for subsequent comparative analyses. After IPTW adjustment, no statistically significant differences emerged among the different therapies in all variables analyzed. The corticosteroid use showed modest numerical differences between treatment arms, including a numerically higher rate in the vedolizumab group after IPTW adjustment without reaching statistical significance.
Outcome data
After applying IPTW to balance baseline characteristics, we assessed various remission outcomes across the three treatment groups. Table 3 and Figure 2 present the IPTW-adjusted remission rates with 95% confidence intervals (CIs) at each timepoint for clinical remission, steroid-free remission, biochemical remission, and endoscopic remission (Tables 2 and 3).

IPTW-adjusted remission outcomes by treatment group over time. Bar plots showing IPTW-adjusted proportions of patients achieving clinical remission, steroid-free clinical remission, biochemical remission, and endoscopic remission with tofacitinib, ustekinumab, and vedolizumab. Clinical, steroid-free clinical, and biochemical remission are shown at weeks 12, 24, and 52; endoscopic remission is shown at week 52 only. Error bars represent 95% confidence intervals. Clinical remission was defined as pMayo score ⩽1; steroid-free clinical remission as clinical remission in the absence of systemic corticosteroid use at the corresponding study visit; biochemical remission as fecal calprotectin <250 μg/g and CRP <5 mg/L; and endoscopic remission as Mayo endoscopic score <2.
Baseline characteristics of the study population by treatment group (after IPTW).
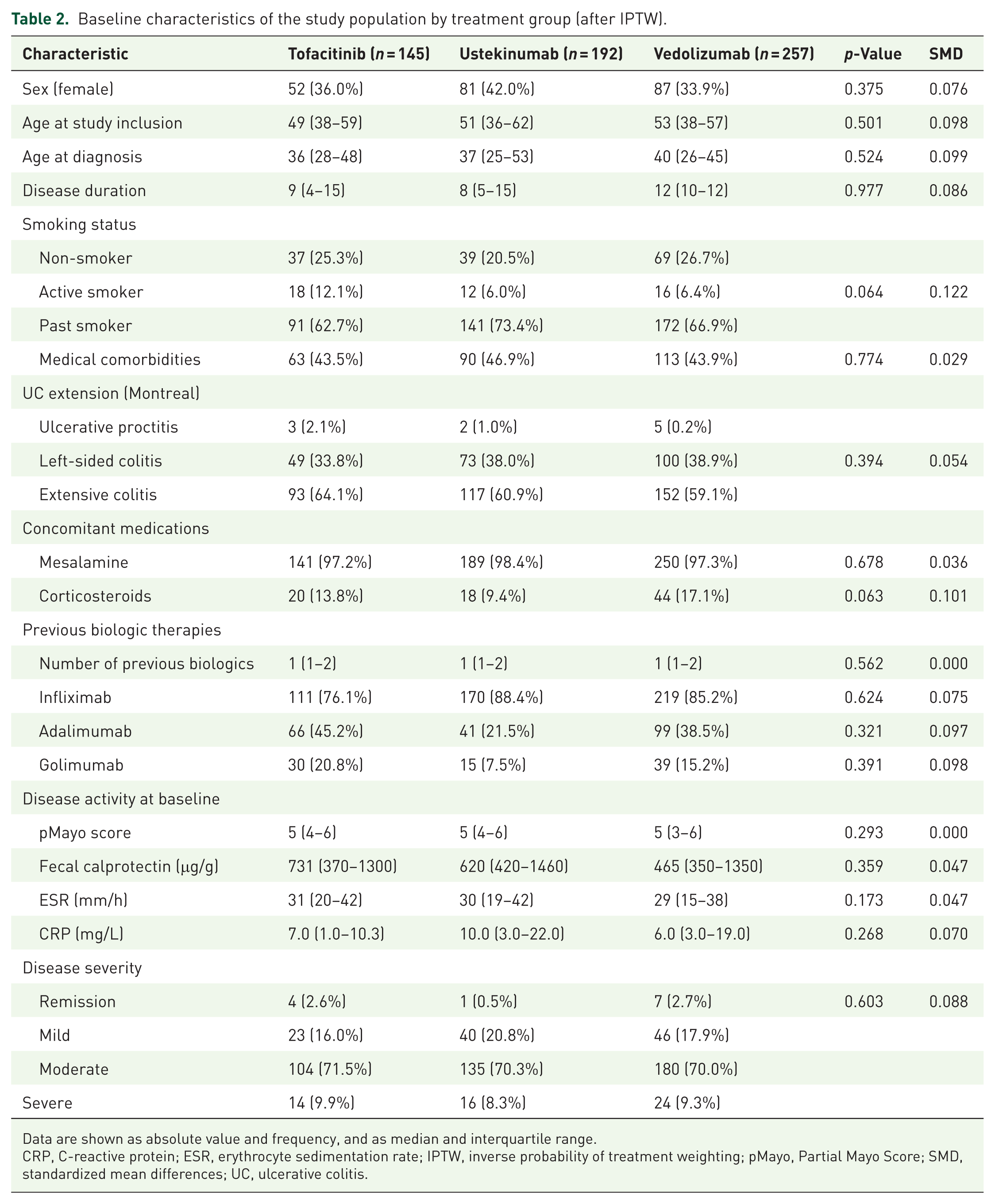
Data are shown as absolute value and frequency, and as median and interquartile range.
CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; IPTW, inverse probability of treatment weighting; pMayo, Partial Mayo Score; SMD, standardized mean differences; UC, ulcerative colitis.
IPTW-adjusted remission rates by treatment group and timepoint.

Data are presented as n; percentage with 95% confidence intervals in parentheses.
IPTW, inverse probability of treatment weighting.
Clinical remission
At 12 weeks, clinical remission rates were comparable across treatment groups, with vedolizumab achieving 29.6% (95% CI: 10.1–57.9), tofacitinib 24.5% (95% CI: 17.4–33.0), and ustekinumab 26.9% (95% CI: 18.8–36.4; p = 0.941). At 24 weeks, all groups showed improvement, with vedolizumab achieving 34.4% (95% CI: 13.0–62.5), tofacitinib 33.6% (95% CI: 25.4–42.5), and ustekinumab 36.3% (95% CI: 27.2–46.3; p = 0.985). At 52 weeks, significant differences emerged between treatment groups, with tofacitinib achieving the highest rate at 55.0% (95% CI: 45.9–63.9), followed by ustekinumab at 41.0% (95% CI: 31.5–51.0; p < 0.001 compared to tofacitinib) and vedolizumab at 37.9% (95% CI: 15.3–65.7; p = 0.002 compared to tofacitinib).
Steroid-free clinical remission
At 12 weeks, steroid-free clinical remission was achieved at modest rates across all groups, with tofacitinib at 21.4% (95% CI: 14.6–29.5), vedolizumab at 26.1% (95% CI: 8.1–54.3), and ustekinumab at 20.9% (95% CI: 13.7–29.9; p = 0.907). At 24 weeks, vedolizumab achieved 31.6% (95% CI: 11.3–59.8), ustekinumab 36.1% (95% CI: 27.0–46.0), and tofacitinib 29.1% (95% CI: 21.4–37.9; p = 0.909). At 52 weeks, significant differences were observed between treatment groups with tofacitinib achieving 53.0% (95% CI: 43.9–61.9), vedolizumab 20.8% (95% CI: 5.4–48.6; p < 0.001 compared to tofacitinib), and ustekinumab 41.0% (95% CI: 31.5–51.0; p = 0.006 compared to vedolizumab).
Biochemical remission
At 12 weeks, biochemical remission rates were similar among all treatment groups, with vedolizumab achieving 45.9% (95% CI: 21.0–72.6), ustekinumab 25.6% (95% CI: 17.6–3.0), and tofacitinib 36.3% (95% CI: 27.9–45.3; p = 0.931). At 24 weeks, tofacitinib achieved 39.0% (95% CI: 30.4–48.1), vedolizumab 45.4% (95% CI: 20.6–72.2), and ustekinumab 36.8% (95% CI: 27.6–47.8; p = 0.837). At 52 weeks, tofacitinib achieved 56.9% (95% CI: 47.7–65.7), vedolizumab 57.3% (95% CI: 30.1–81.3), and ustekinumab 56.3% (95% CI: 46.3–66.0).
Endoscopic remission
Endoscopic assessment at week 52 was available in 255 patients overall, including 28/149 (18.8%) treated with tofacitinib, 105/193 (54.4%) treated with ustekinumab, and 122/260 (46.9%) treated with vedolizumab.
At 52 weeks, endoscopic remission differed significantly between treatment groups, with tofacitinib achieving 21.4% (95% CI: 9.5–38.9), ustekinumab 19.0% (95% CI: 12.4–27.3), and vedolizumab 27.9% (95% CI: 20.5–36.3; p < 0.001 compared to ustekinumab).
Time-to-event analysis for clinical remission
IPTW-adjusted time-to-event analysis was conducted to assess the probability of achieving clinical remission over time. Supplemental Table 1 presents the results of the Cox proportional hazards model and cumulative incidence of clinical remission by treatment group.
The cumulative probability of achieving clinical remission over the 52-week follow-up period was significantly different between treatment groups. Compared to vedolizumab, tofacitinib was associated with a significantly higher probability of achieving remission (hazard ratio (HR) = 1.40, 95% CI: 1.08–1.83, p = 0.012), while ustekinumab was associated with a similar probability of achieving clinical remission as vedolizumab (HR = 1.16, 95% CI: 0.89–1.50, p = 0.271).
Figure 3 shows the probability of achieving clinical remission during the follow-up period.
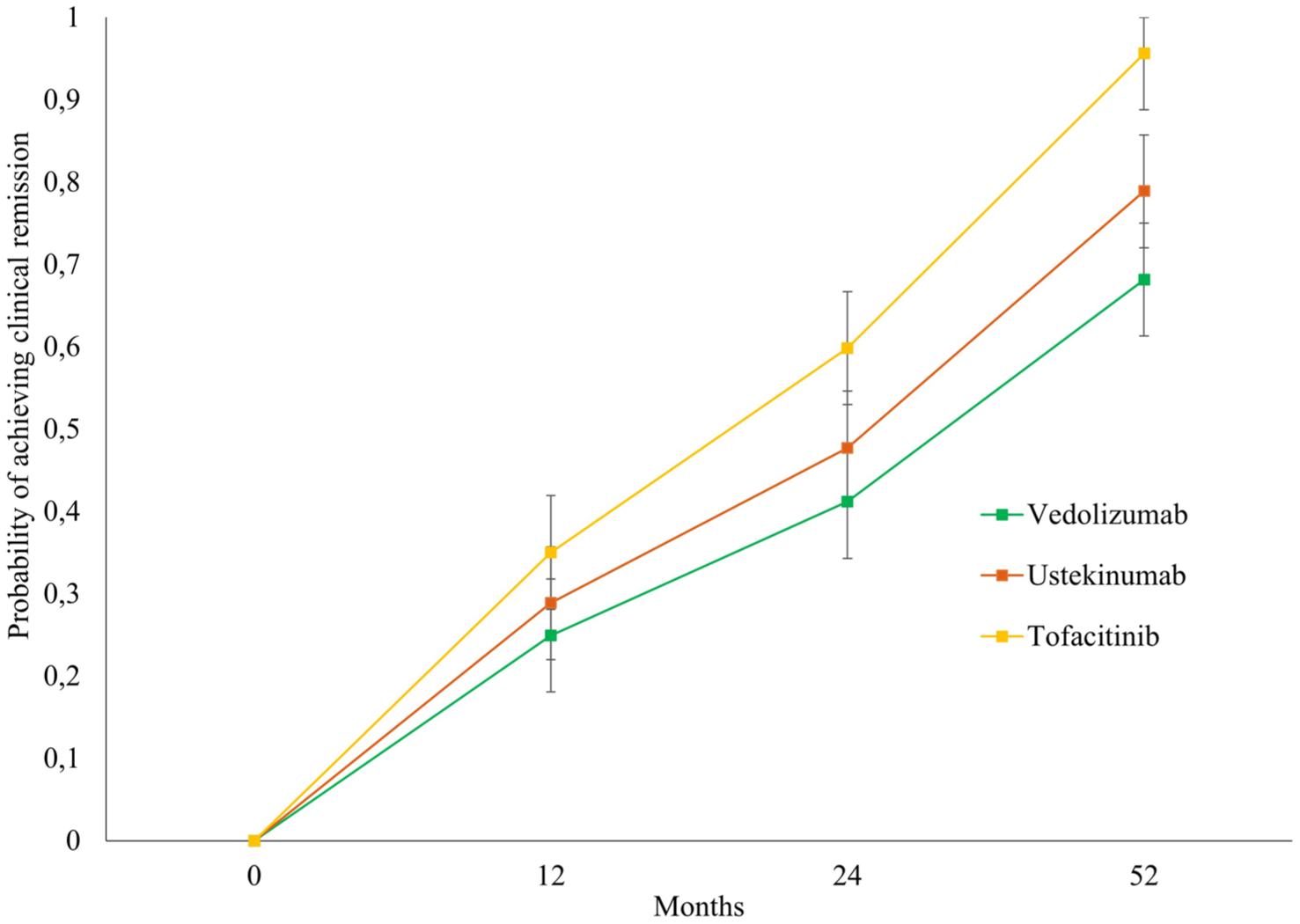
IPTW-adjusted cumulative probability of clinical remission over 52 weeks. Line plot showing the IPTW-adjusted cumulative probability of achieving clinical remission over the 52-week follow-up period in patients treated with tofacitinib, ustekinumab, or vedolizumab. Error bars represent 95% confidence intervals.
Composite endpoints
IPTW-adjusted analyses of composite endpoints provide a broader assessment of treatment efficacy at week 52. Combined clinical and biochemical remission was achieved in 33.5% (95% CI: 25.3–42.4) with tofacitinib, 26.6% (95% CI: 18.6–36.1) with ustekinumab, and 32.1% (95% CI: 11.6–60.3) with vedolizumab (p = 0.897). The proportion of patients achieving sustained clinical remission from 24 to 52 weeks was similar between all treated groups, with tofacitinib achieving 25.8% (95% CI: 18.4–34.3), Ustekinumab achieving 23.2% (95% CI: 15.6–32.3), and vedolizumab achieving 30.8% (95% CI: 18.6–36.1) with p = 0.849.
Subgroup analyses
Clinical remission at week 52 varied by disease extension and prior biologic exposure (Supplemental Table 2). Among patients with extensive colitis, clinical remission rates were 29.6%, 58.8%, and 36.3% for vedolizumab, tofacitinib, and ustekinumab, respectively. In patients with >2 prior biologics, tofacitinib showed the highest rate of clinical remission at 52 weeks (59.3%) compared to vedolizumab (33.4%; p = 0.089) and ustekinumab (31.4%; p < 0.001).
Safety outcomes
Supplemental Table 3 presents safety outcomes across the three treatment groups. Adverse events were reported in up to 6% of patients, with no significant differences: higher prevalence in the tofacitinib (6.94%) and lower in the ustekinumab (2.07%) groups. Serious adverse events occurred in 0.76% of vedolizumab patients and 2.01% of tofacitinib patients, with none reported in the ustekinumab group.
Discussion
The optimal positioning of current drugs in treatment algorithms after anti-TNF failure remains undefined, making it essential to compare available agents to identify the best sequencing strategy. In the absence of prospective head-to-head trials in UC, indirect comparisons are the only option. 28 This multicenter retrospective study included a large cohort of UC patients previously exposed to anti-TNF therapy who were refractory and/or intolerant, and subsequently treated with vedolizumab, ustekinumab, or tofacitinib.
At baseline, the significant differences between the three groups were observed, and to address these imbalances, we applied a weighted IPTW approach to balance covariates for comparative analyses. After IPTW adjustment, baseline characteristics across treatment groups were more balanced, allowing a more comparable assessment of outcomes between vedolizumab, ustekinumab, and tofacitinib in anti-TNF-experienced UC patients. However, because IPTW accounts only for measured covariates, residual confounding by indication cannot be excluded, and the observed between-group differences should be interpreted as associations rather than as causal treatment effects. 29
With respect to clinical outcomes, rates of both clinical remission and steroid-free clinical remission at 12 and 24 weeks were comparable across therapies, suggesting similar short-term effectiveness. At 52 weeks, however, significant differences emerged: tofacitinib achieved the highest rates of sustained remission, followed by ustekinumab, while vedolizumab showed lower long-term outcomes. Given the IPTW balancing, these results suggest superior durability of clinical response with JAK inhibition, with ustekinumab occupying an intermediate position. Nevertheless, the wide CIs observed for vedolizumab—likely due to smaller sample size—indicate uncertainty and call for cautious interpretation.
For biochemical remission, the three therapies showed largely similar rates, particularly at 52 weeks, where results converged across groups. This apparent alignment may reflect some differences in the sensitivity of clinical versus biochemical endpoints or a temporal asynchrony between symptom improvement and biomarker normalization. 30 Thus, while all agents appear comparably effective in reducing systemic or fecal markers of inflammation, they diverge in terms of sustained symptomatic control.
Regarding endoscopic remission, assessed in a subgroup of 255 patients at 52 weeks, vedolizumab achieved significantly higher rates than ustekinumab, while tofacitinib displayed intermediate results. This finding contrasts with the superiority of tofacitinib for clinical outcomes and may be explained by several factors. The gut-selective mechanism of vedolizumab (α4β7 blockade) could promote deeper mucosal healing, while clinical endpoints are influenced by extra-inflammatory symptoms.31,32 Moreover, subgroup analyses may attenuate the effect of IPTW balancing, and patient selection for endoscopy may introduce bias. These discrepancies highlight the complexity of interpreting multidimensional treatment outcomes in UC.
Overall, several meta-analyses have investigated the setting of anti-TNF-experienced UC, comparing various drugs.5,17,18,33–35 However, most of these analyses are based on RCT data, and it is well recognized that RCT populations often do not fully reflect RW patients due to differences in demographics, clinical characteristics, and concurrent management.5,17,18,33–35 Restricting the analysis to the three drugs in this study, tofacitinib appears to achieve higher remission rates at 8 weeks; vedolizumab catches up at 24–48 weeks, while ustekinumab tends to have lower efficacy.5,17,18,33–35
Compared with other RW studies, in a recent retrospective cohort study including UC patients previously exposed to a TNFi, after one-to-one PSM, Kochhar et al. 36 reported that ustekinumab might be the preferred second-line therapy over tofacitinib and vedolizumab, particularly regarding the risk of a composite outcome of intravenous steroids or colectomy within 2 years. By contrast, in our study, ustekinumab showed intermediate long-term efficacy, with higher clinical remission rates than vedolizumab but lower than tofacitinib. Notably, vedolizumab achieved superior endoscopic remission compared to ustekinumab, suggesting a potential advantage for mucosal healing. These results differ from Kochhar et al., who reported better outcomes with ustekinumab, likely reflecting differences in populations, endpoints, and methodology. Overall, our findings indicate that tofacitinib provides the most durable clinical benefit, ustekinumab maintains intermediate effectiveness, and vedolizumab may be favored when mucosal healing is prioritized. 37
Regarding vedolizumab, our findings align with other real-world studies,14,38,39 showing that clinical remission and steroid-free remission were time-dependent. This supports the clinical practice of maintaining vedolizumab therapy for at least 6 months before considering alternative treatments in patients who lack an early response but have objective markers of disease activity. 14 Notably, our clinical remission rates at week 52 were worse than those recorded in the GEMINI 2 trial, 40 likely reflecting differences in patient characteristics—particularly that nearly half of GEMINI participants were bio-naïve, whereas our cohort had longer disease duration. More strikingly, at 12 weeks, both clinical remission rates and steroid-free remission were comparable to those of the other two drugs, particularly tofacitinib. This contrasts with some other RW studies and NMAs of RCTs.21,34,41 In a recently published IG-IBD multicenter study comparing the effectiveness of vedolizumab and tofacitinib in a cohort of UC patients with anti-TNF failure, tofacitinib showed greater efficacy in inducing corticosteroid-free clinical remission at week 8. 42 A possible explanation could be the time of disease activity evaluation (8 vs 12 weeks): evaluation at 12 weeks instead of 8 would give vedolizumab more time to demonstrate effectiveness. Finally, in our cohort, we observed the greater effectiveness of tofacitinib in the medium-long term. Interestingly, at week 52, not only there were more than half of the patients treated with tofacitinib in clinical remission, but all of them were also in steroid-free remission. It is worth noting that our findings do not fully align with some other RW experiences.43,44 For instance, a large observational study reported lower treatment persistence with tofacitinib compared to vedolizumab in anti-TNF-experienced UC patients. 43 Similarly, in the IG-IBD cohort, both drugs appeared equally effective and safe during maintenance. 42 To note, the discrepancy observed in the vedolizumab group between clinical remission and steroid-free clinical remission at week 52 should be interpreted cautiously. Although corticosteroid use was not significantly different after IPTW, it remained numerically higher in the vedolizumab group than in the other treatment arms, which may have influenced the steroid-free endpoint.
The subgroup analysis provides further insight into potential treatment heterogeneity. In extensive colitis, remission was higher with tofacitinib (58.8%) than with ustekinumab (36.3%) and vedolizumab (29.6%). In left-sided colitis, vedolizumab achieved the highest remission rate (71.0%), followed by tofacitinib (50.9%) and ustekinumab (48.9%). Considering prior biologic class exposure, patients with >2 previous biologic classes achieved higher remission rates with tofacitinib (59.3%) compared to vedolizumab (33.4%) and ustekinumab (31.5%), while in those with 1–2 biologic classes, tofacitinib was numerically higher (52.1%) than ustekinumab (47.1%) and vedolizumab (42.2%). Findings for ulcerative proctitis (tofacitinib 34.1%, n = 2; 0% with vedolizumab and ustekinumab) should be interpreted with caution due to the very small sample size. Taken together, these exploratory analyses suggest that both disease extent and treatment history may influence relative treatment performance, reinforcing the importance of a personalized, target-oriented approach.45,46
With respect to safety outcomes, adverse events were reported in a small proportion of patients across all three treatment groups, with no statistically significant differences. The highest overall prevalence was observed in the tofacitinib group (6.9%), while the lowest was in the ustekinumab group (2.1%). Serious adverse events were infrequent, occurring in 0.8% of vedolizumab-treated patients and 2.0% of those on tofacitinib, with none reported in the ustekinumab group. These results are consistent with the safety profiles described in pivotal RCTs and long-term extension studies, which have generally shown low rates of severe complications with these agents.5,17,18,33–35
Overall, the effectiveness of these three treatments once again underscores the need for a personalized approach, which takes into account various aspects related to the patient and the pathology, including the presence of extraintestinal manifestations, the patient’s comorbidities, the speed of action of the drug, and its safety profile, and there is no single approach.
A strength of the present study is the inclusion of a multicenter RW cohort and the use of standardized clinical scores to evaluate disease activity. However, the size of the individual treatment arms was more limited, particularly in subgroup analyses. Strict criteria to define remission and clinical response enhance the results obtained. On the other hand, there are also limitations, including its retrospective design, in addition to the lack of some data for certain variables (e.g., endoscopic parameters), reflecting the RW nature of the dataset. Despite IPTW adjustment, residual confounding from unmeasured or incompletely captured variables cannot be excluded. In particular, factors such as the type of prior anti-TNF failure, steroid dependence, extraintestinal disease burden, and dose optimization/escalation may have influenced both treatment selection and subsequent outcomes. Therefore, the comparative results of this retrospective study should be interpreted with caution. In addition, detailed data on the reason for anti-TNF discontinuation were not uniformly available in this retrospective dataset. Moreover, prior treatment exposure was categorized by biologic class rather than by individual molecules within the same class, which may limit the interpretation of treatment sequencing. In addition, endoscopic remission was assessed only in the subgroup of patients who underwent follow-up endoscopy at week 52. Since the decision to perform endoscopy in RW practice may have been influenced by the patient’s clinical course during follow-up, this analysis may be affected by selection bias and reduced statistical power. IPCW was not applied specifically to address this potential bias in the endoscopic subgroup analysis; therefore, these findings should be interpreted with caution. Furthermore, detailed data on steroid dependence, baseline steroid dose, and tapering strategy were not uniformly available in this retrospective dataset. Moreover, after IPTW, baseline corticosteroid use remained numerically higher in the vedolizumab group than in the other treatment arms. These factors may have influenced the steroid-free remission endpoint, particularly the lower week-52 rate observed with vedolizumab, and, therefore, this finding should be interpreted with caution. Detailed data on steroid dependence and steroid-refractory disease were not uniformly available and therefore could not be incorporated into the IPTW model. No further balancing procedure or additional post-IPTW covariate adjustment was applied, and this may have influenced the comparative estimates. Finally, the wide CIs for some estimates highlight statistical uncertainty.
In conclusion, in this multicenter retrospective cohort of anti-TNF-experienced UC patients, tofacitinib was associated with higher long-term clinical and steroid-free remission rates; ustekinumab showed intermediate effectiveness with a favorable safety profile; and vedolizumab was associated with higher endoscopic remission. These findings may help inform individualized, outcome-oriented treatment strategies, but they should be interpreted in light of the potential for residual confounding and require confirmation in prospective head-to-head studies.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261455563 – Supplemental material for An inverse probability of treatment weighted comparison between vedolizumab, ustekinumab, and tofacitinib in anti-TNF-experienced ulcerative colitis patients
Supplemental material, sj-docx-1-tag-10.1177_17562848261455563 for An inverse probability of treatment weighted comparison between vedolizumab, ustekinumab, and tofacitinib in anti-TNF-experienced ulcerative colitis patients by Antonio Tursi, Andrea Pasta, Walter Elisei, Brigida Barberio, Luisa Bertin, Giammarco Mocci, Giovanni Maconi, Antonietta Gerarda Gravina, Raffaele Pellegrino, Giorgia Bodini, Alfredo Papa and Edoardo Vincenzo Savarino in Therapeutic Advances in Gastroenterology
Footnotes
Author note
Collaborators: Italian Network for Inflammatory Bowel Diseases (IN-IBD)—Davide G. Ribaldone: IBD Unit, A.O.U. Citta della Salute e della Scienza,” Torino, Italy; Antonio Ferronato: UOSD di Endoscopia Digestiva, ULSS7 Pedemontana, Ospedale di Santorso, Santorso (VI), Italy; Greta Lorenzon and Fabiana Zingone: UOC di Gastroenterologia, Dipartimento di Scienze Chirurgiche, Oncologiche e Gastroenterologiche, Università di Padova, Azienda Ospedaliero-Universitaria “Sant’Antonio,” Padova, Italy; Davide Checchin: UOC di Gastroenterologia, Ospedale “S Giovanni e Paolo,” Mestre-Venezia, Italy; Carla Felice: UOC di Medicina Interna, Ospedale Universitario “Ca’ Foncello,” Treviso, Italy; Giovanni Cataletti: UOC di Gastroenterologia, A.O. “L. Sacco,” Milano, Italy; Giorgia Bodini: UOC di Gastroenterologia, Dipartimento di Medicina Interna, IRCCS Ospedale “San Martino” Hospital, Università di Genova, Genova, Italy; Giovanni Aragona and Patrizia Perazzo: UOC di Gastroenterologia, Ospedale “Guglielmo da Saliceto,” Piacenza, Italy; Federica Gaiani and Stefano Kayali: UOC di Gastroenterologia ed Endoscopia Digestiva, Dipartimento di Medicina e Chirurgia, Ospedale Maggiore, Università di Parma, Parma, Italy; Fabio Cortellini: UOC di Gastroenterologia ed Endoscopia Digestiva, Ospedale “Infermi,” Rimini, Italy; Francesco Costa: UOC di Gastroenterologia, Azienda Ospedaliero-Universitaria Pisana, Pisa, Italy; Lorenzo Bertani: UOC di Gastroenterologia, Ospedale “Felice Lotti,” Azienda USL Toscana Nord Ovest, Pontedera (PI), Italy; Antonella Scarcelli and Mariaelena Serio: UOC di Gastroenterologia, Ospedale “San Salvatore,” Pesaro, Italy; Emanuele Bendia and Laura Bolognini: UOC di Gastroenterologia, Endoscopia Digestiva e Malattia infiammatorie Croniche Intestinali, Ospedale “Torrette,” Ancona, Italy; Simona Piergallini: UOC di Gastroenterologia, IBD Unit, Ospedale “A. Murri,” Fermo, Italy; Francesca Maria Onidi, Giorgia Orrù, and Paolo Usai Satta: UOC di Gastroenterologia, Azienda Ospedaliera di Rilievo Nazionale “Brotzu,” Cagliari, Italy; Giorgia Orrù: Department of Medical Sciences and Public Health, University of Cagliari, Cagliari, Italy; Raffaele Colucci and Francesco Bachetti: UOSD di Endoscopia Digestiva, Ospedale “San Matteo degli Infermi,” Spoleto (PG), Italy; Gabrio Bassotti and Elisabetta Antonelli: Sezione di Gastroenterologia ed Epatologia, Dipartimento di Medicina, Ospedale “Santa Maria della Misericordia”, Perugia, Italy; Costantino Zampaletta, Giulia Rocco, and Carlotta Sacchi: UOC di Gastroenterologia, Ospedale “Belcolle,” Viterbo, Italy; Franco Scaldaferri and Daniele Napolitano: UOC di Medicina Interna e Gastroenterologia, Dipartimento di Scienze Mediche e Chirurgiche, IRCCS Fondazione “Policlinico Gemelli, Università Cattolica del Sacro Cuore, Roma, Italy; Roberto Faggiani, Rita Monterubbianesi, and Michela Di Fonzo: UOC di Gastroenterologia ed Endoscopia Digestiva, A.O. “S. Camillo-Forlanini,” Roma, Italy; Cristiano Pagnini, Maria Giovanna Graziani, and Maria Carla Di Paolo: UOC di Gastroenterologia ed Endoscopia Digestiva, A.O. “S. Giovanni-Addolorata,” Roma, Italy; Roberta Pica, Maddalena Zippi, Andrea Cocco, and Claudio Cassieri: UOC di Gastroenterologia ed Endoscopia Digestiva, Ospedale “S. Pertini,” Roma, Italy; Roberto Lorenzetti: UOC di Gastroenterologia, Ospedale Territoriale “Nuovo Regina Margherita,” Roma, Italy; Gian Marco Giorgetti and Valeria Clemente: UOSD di Endoscopia Digestiva Nutrizionale, Ospedale “S. Eugenio,” Roma, Italy; Patrizio Scarozza, Girolamo Bevevino, Giulia Zerboni, and Federico Iacopini: UOC di Gastroenterologia ed Endoscopia Digestiva, “Ospedale dei Castelli,” Ariccia (Roma), Italy; Giacomo Forti: UOSD di Endoscopia Digestiva, Ospedale “S. Maria Goretti,” Latina, Italy; Laurino Grossi: UOC di Gastroenterologia, Ospedale “Spirito Santo,” Università “G d’Annunzio,” Pescara, Italy; Serafina Fiorella: UOSD di Gastroenterologia ed Endoscopia Digestiva, Ospedale “P. Pio,” Vasto (CH), Italy; Giovanni Lombardi and Marta Patturelli: UOC di Gastroenterologia, Azienda Ospedaliera di Rilievo Nazionale “Antonio Cardarelli,” Napoli, Italy; Giuliana Vespere, Silvia Sedda, and Leonardo De Luca: UOC di Gastroenterologia, “Ospedale del Mare” ASL NA1 Centro, Napoli, Italy; Caterina Mucherino, Elvira D’Antonio, and Laura Montesano: UOC di Gastroenterologia, Azienda Ospedaliera “S. Anna e S. Sebastiano,” Caserta, Italy; Pietro Capone and Guido Daniele Villani: UOC di Gastroenterologia ed Endoscopia Digestiva, Ospedale “T. Maresca,” Torre del Greco (NA), Italy; Antonio Cuomo and Laura Donnarumma: UOSD di Gastroenterologia, Ospedale “Umberto I,” Nocera Inferiore (SA), Italy; Nicola Della Valle: UOC di Gastroenterologia, A.O. “Ospedali Riuniti,” Foggia, Italy; Giuseppe Pranzo: UOS di Endoscopia Digestiva, Ospedale “Valle D’Itria,” Martina Franca (TA), Italy; Paolo Tonti and Viviana Neve: UOSD di Gastroenterologia ed Endoscopia Digestiva, Ospedale “A. Perrino,” Brindisi, Italy; Libera Fanigliulo: UOC di Gastroenterologia, A.O. “S.S. Annunziata,” Taranto, Italy; Leonardo Allegretta, Alessia Immacolata Cazzato, and Stefano Scorza: UOC di Gastroenterologia ed Endoscopia Digestiva, Ospedale “Santa Caterina Novella,” Galatina (LE), Italy; Manuela Marzo: UOC di Gastroenterologia ed Endoscopia Digestiva, Ospedale “Veris-Delli Ponti,” Scorrano (LE), Italy; Ileana Luppino: UOC di Gastroenterologia ed Endoscopia Digestiva, Ospedale “Annunziata,” Cosenza, Italy; Francesco Luzza and Rocco Spagnuolo: Dipartimento di Scienze Mediche, UOC di Fisiopatologia Digestiva, Azienda Ospedaliera “Mater Domini,” Università di Catanzaro, Catanzaro, Italy; Stefano Rodinò and Ladislava Sebkova: UOC di Gastroenterologia, A.O. “Ciaccio-Pugliese,” Catanzaro, Italy; Antonio De Medici: Servizio di Gastroenterologia Territoriale, AST Catanzaro, Catanzaro Lido, Italy; Domenico Catarella, Dario D’Agostino, and Elisabetta Di Bartolo: UOC di Gastroenterologia, ARNAS “Garibaldi,” Catania, Italy.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.