
Abstract
Although immune checkpoint inhibitors have revolutionized oncologic therapy, they are frequently associated with a wide spectrum of immune-related adverse events, most notably immune-mediated colitis (ImC). For cases of moderate-to-severe colitis, treatment typically involves corticosteroids with escalation to biologic agents such as infliximab or vedolizumab when necessary. However, treatment-refractory cases remain a major clinical challenge. We report the case of a 52-year-old woman with triple-negative breast cancer who developed severe ImC after pembrolizumab therapy. Despite high-dose corticosteroids and infliximab, her condition remained refractory. Initiation of upadacitinib, a selective Janus kinase 1 (JAK1) inhibitor, led to rapid clinical improvement and complete endoscopic remission of the colitis. This report highlights the therapeutic potential of upadacitinib against ImC, while also analysing the possible twofold role of JAK1-inhibitors in enhancing antitumour therapy efficacy and limiting the potential immune-related adverse events.
Keywords
Introduction
Treatment with immune checkpoint inhibitors (ICI) has become a cornerstone in the management of certain types of malignancies. Agents targeting programmed cell death protein 1 (PD-1), programmed death-ligand 1 (PD-L1), and cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4) have demonstrated significant antitumour efficacy by enhancing T-cell-related immune responses. However, such clinical benefits are accompanied by a growing incidence of immune-related adverse events (irAEs), which increases even more with the combination of two ICIs. 1 IrAEs may eventually involve any organ system, occasionally affecting more than one simultaneously, requiring thorough clinical and laboratory monitoring. The most frequent systemic toxicities include skin manifestations, gastrointestinal (GI) tract inflammation, pulmonary involvement and endocrine gland dysfunction. 2 Immune-mediated colitis (ImC) represents the most prevalent and significant GI irAE, presenting with a wide spectrum of endoscopic and even histopathological features.
Current European and American consensus recommendations initially suggest management with systemic corticosteroids, and in cases of inadequate response, escalation to biologic agents, such as infliximab (IFX) or vedolizumab.3,4 In cases where patients fail to respond to biologic agents, alternative therapeutic strategies, often adapted from the management of inflammatory bowel diseases (IBD), have been considered. Agents such as ustekinumab and tofacitinib have demonstrated encouraging outcomes; however, the available evidence remains limited to individual case reports. 4 Herein, we describe a novel case of severe, treatment-refractory immune-mediated colitis that achieved complete clinical remission following the initiation of upadacitinib, a selective Janus kinase 1 (JAK1) inhibitor. The case report was prepared in accordance with the CARE guidelines: Consensus-based Clinical Case Reporting Guideline Development (Supplemental Material). 5
Case presentation
We report the case of a 52-year-old woman with no significant past medical history who was diagnosed with triple-negative breast cancer and subsequently developed severe ImC following treatment with ICI.
The patient initially received oncologic care at an external institution, where she was diagnosed with triple-negative breast cancer (T2N1M0). She was then started on neoadjuvant therapy with pembrolizumab, an anti–PD-1 ICI, administered at a dose of 200 mg every 3 weeks, in combination with weekly paclitaxel and carboplatin, prior to a planned lumpectomy. After the third dose, she developed severe diarrhoea, with up to 15 bowel movements per day along with diffuse cramping abdominal pain. Diarrhoea initially presented as watery stools and later progressed to bloody, mucus-containing stools. She remained afebrile throughout. She presented to the emergency department, where abdominal computed tomography (CT) showed findings consistent with colitis extending to the left colonic flexure. She was subsequently admitted to the oncology ward. Microbiological analysis of stool samples was negative, and faecal calprotectin levels were elevated (3490 μg/g). Additional laboratory investigations, including thyroid and pancreatic function tests, revealed no evidence of other immune-related organ involvement. Colonoscopy revealed left-sided colitis extending to the splenic flexure, with endoscopic inflammation equivalent to an Ulcerative Colitis Endoscopic Index of Severity (UCEIS) score of 4 (Figure 1). Histopathological analysis of the biopsy specimens taken disclosed signs of active inflammation consistent with ImC (Figure 2). Initial treatment included intravenous (IV) fluid resuscitation and corticosteroid therapy, with methylprednisolone at 1 mg/kg body weight (BW)/day, and treatment with pembrolizumab was discontinued. As her symptoms improved, treatment was scaled down to oral prednisolone after 3 days, and the patient was discharged. However, due to clinical worsening during corticosteroid tapering, the patient was readmitted 1 week after discharge. A follow-up sigmoidoscopy demonstrated persistent active inflammation of the left colon, leading to reintroduction of IV methylprednisolone at 1 mg/kg BW/day. Because of the patient’s lack of clinical response to steroids, infliximab was subsequently initiated at a dose of 5 mg/kg. As a result of significant weight loss and poor oral intake, the patient’s nutritional status was supported with parenteral nutrition. Despite administration of a second IFX dose at an escalated dose of 10 mg/kg 5 days after the initial infusion, the patient showed no significant clinical improvement. A follow-up abdominal CT scan excluded colitis-related complications and demonstrated persistent active colitis without progression in extent (Figure 3). Owing to the refractory nature of her condition, she was referred to our tertiary centre specializing in the management of IBD.
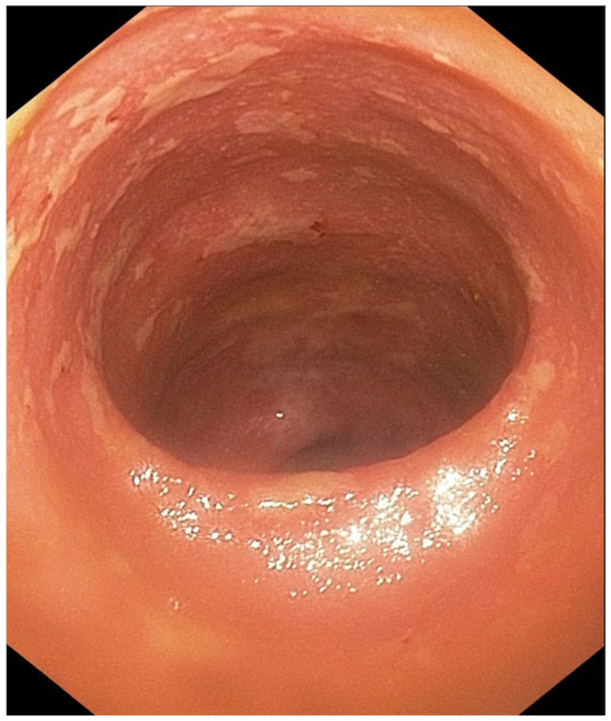
Endoscopy image prior initiation of JAK1-inhibitor therapy, demonstrating features consistent with inflammation, including erythema, friability with contact-induced bleeding, and oedematous mucosa, with absence of the vascular pattern, and round ulcerations, approximately 1 cm in diameter, covered by a fibrinous exudate. Given the endoscopic resemblance to Ulcerative colitis and the absence of a distinct endoscopic scoring system for ImC, the features were classified as 4 points according to the Ulcerative Colitis Endoscopic Index of Severity.
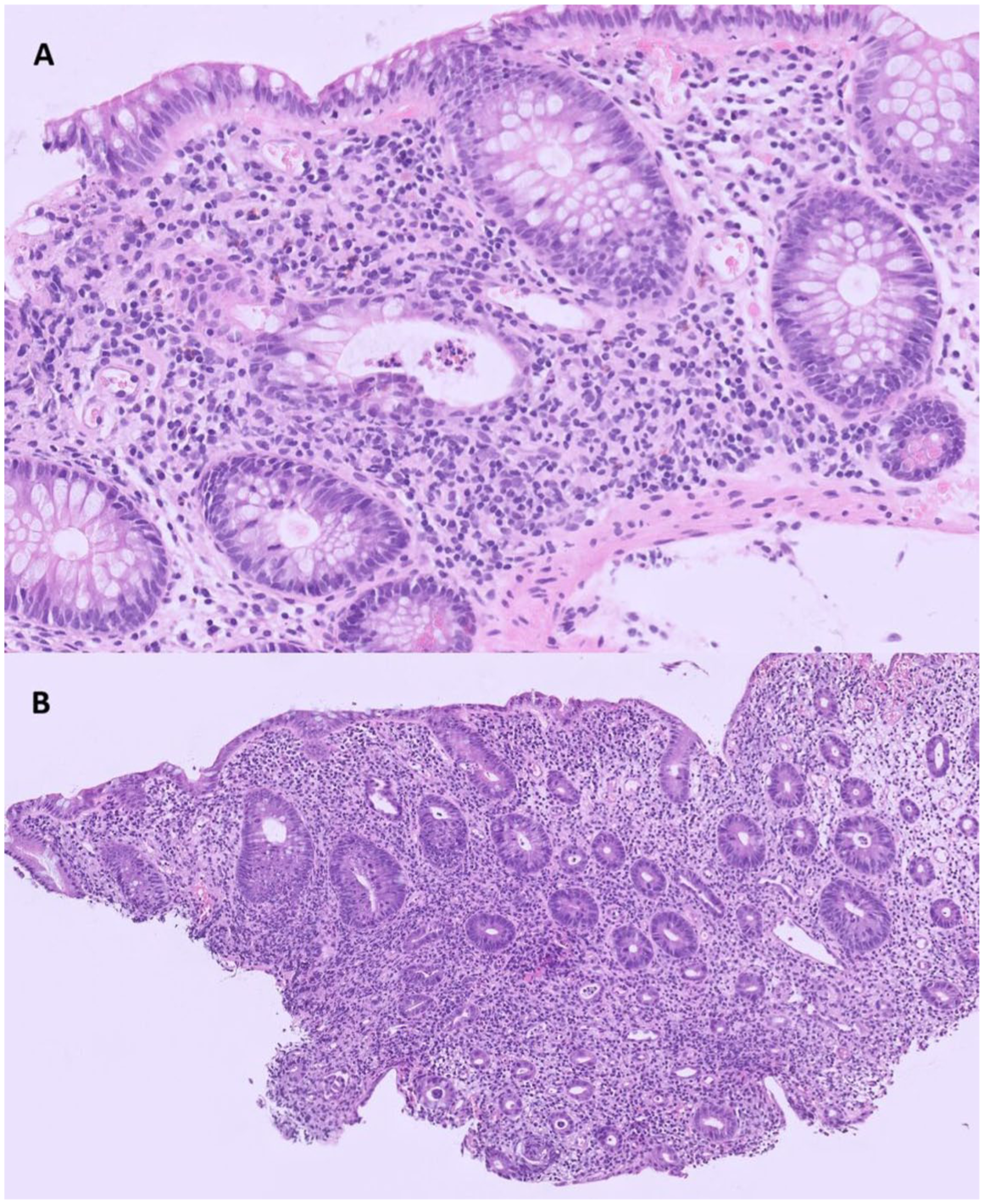
Histopathological images in hematoxylin and eosin (H&E) stain revealed infiltration of crypts, crypt abscess formation and a mild mononuclear cell infiltration of the surrounding lamina propria (a). Additionally, there was marked plasma cell infiltration of the lamina propria, along with neutrophilic epithelial infiltration, cryptitis, with overall preservation of crypt architecture and the presence of multiple small-sized attenuated, and atrophic crypts (b). No granulomas were identified. H&E, (a) 20×, (b) 10×.
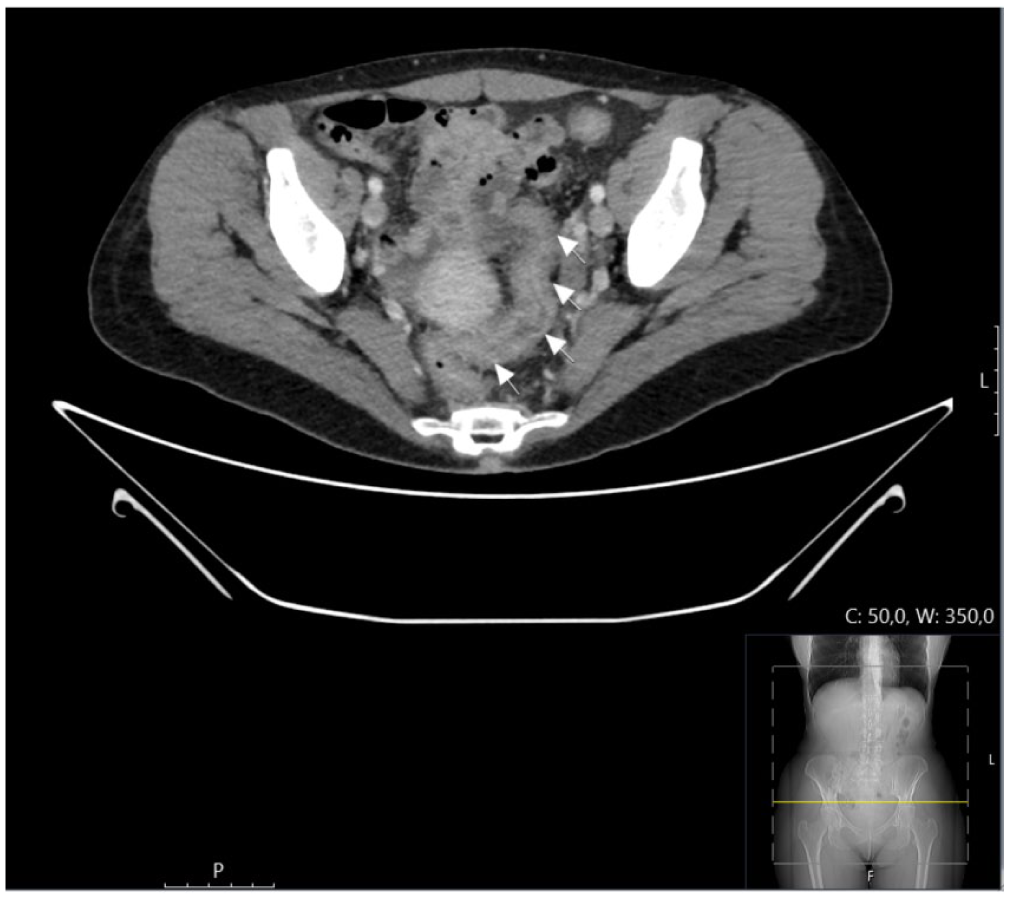
Abdominal computed tomography revealed findings consistent with active proctocolitis, including bowel wall thickening of the rectum, sigmoid colon, and descending colon (arrows), with mild adjacent fat stranding. There were no signs of bowel perforation, abscess formation, or pneumatosis. A small amount of free intraperitoneal fluid was noted.
Comprehensive laboratory investigations, including repeat faecal microbiology, were negative. Repeat sigmoidoscopy with biopsies showed ongoing mucosal inflammation extending to the left flexure, with a UCEIS score of 4, consistent with a lack of endoscopic improvement. Serological testing was positive for both IgM and IgG antibodies against cytomegalovirus (CMV). Re-evaluation of the most recent endoscopic biopsy specimens by specialized gastrointestinal pathologists demonstrated inflammatory changes related to ImC, with only a single CMV-positive cell identified on immunohistochemical staining. No evidence of extraintestinal CMV organ involvement was detected in the laboratory work-up. The findings were interpreted as CMV reactivation secondary to immunosuppression, rather than a primary CMV colitis.
Oral upadacitinib was initiated at a daily dose of 45 mg, 2 weeks after the first IFX infusion. To reduce thromboembolic risk in the setting of active colitis, malignancy and JAK-inhibitor therapy, the patient received prophylactic low-molecular-weight heparin, dalteparin 5000 IU subcutaneously once daily, until discharge. Given the patient’s cumulative exposure to immunosuppressive agents, prophylactic antiviral therapy with ganciclovir was administered. The patient had a rapid clinical response to the JAK1-inhibitor and was discharged within 1 week. Follow-up sigmoidoscopy 2 weeks after initiation of therapy revealed only post-inflammatory findings in the left colon. After the patient completed an 8-week course of upadacitinib 45 mg daily, followed by a maintenance dose of 15 mg daily for an additional 8 weeks, a repeat endoscopy performed before treatment completion showed complete mucosal healing with no signs of active inflammation (Figure 4). The medication was discontinued, and the patient remains in complete remission, without the need for maintenance therapy after approximately 1 year of follow-up (Figure 5). She continues regular follow-up with the oncology department at our hospital and received adjuvant local radiotherapy for breast cancer after achieving remission from ImC.
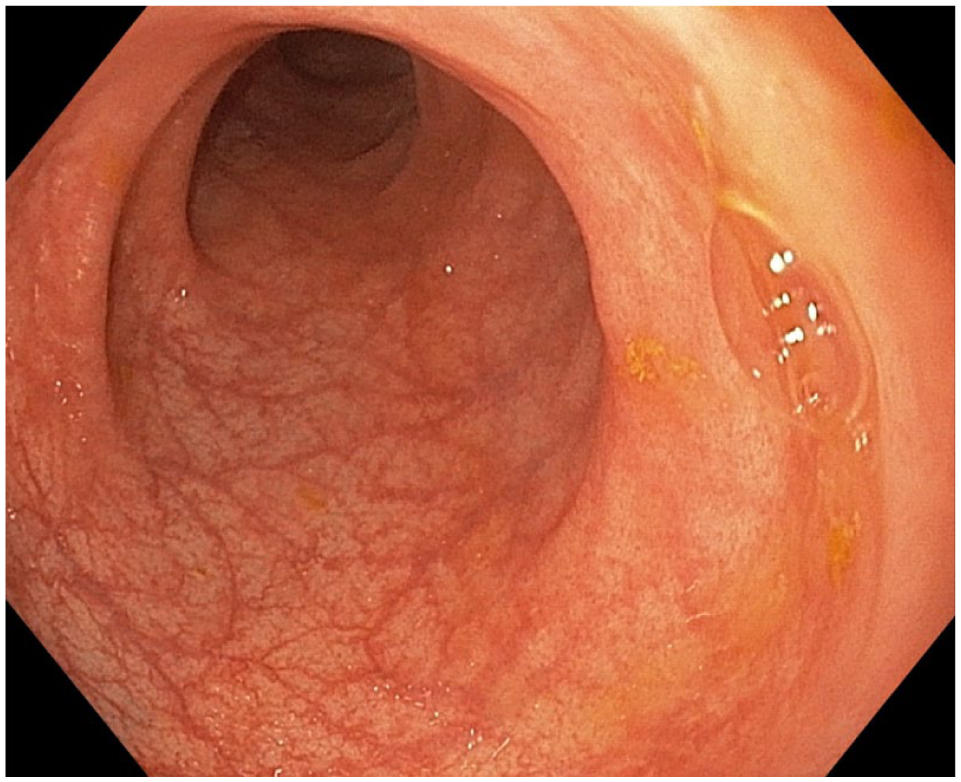
Endoscopy image following 16 weeks of JAK1-inhibitor therapy, demonstrating complete healing with restoration of normal colonic mucosa.
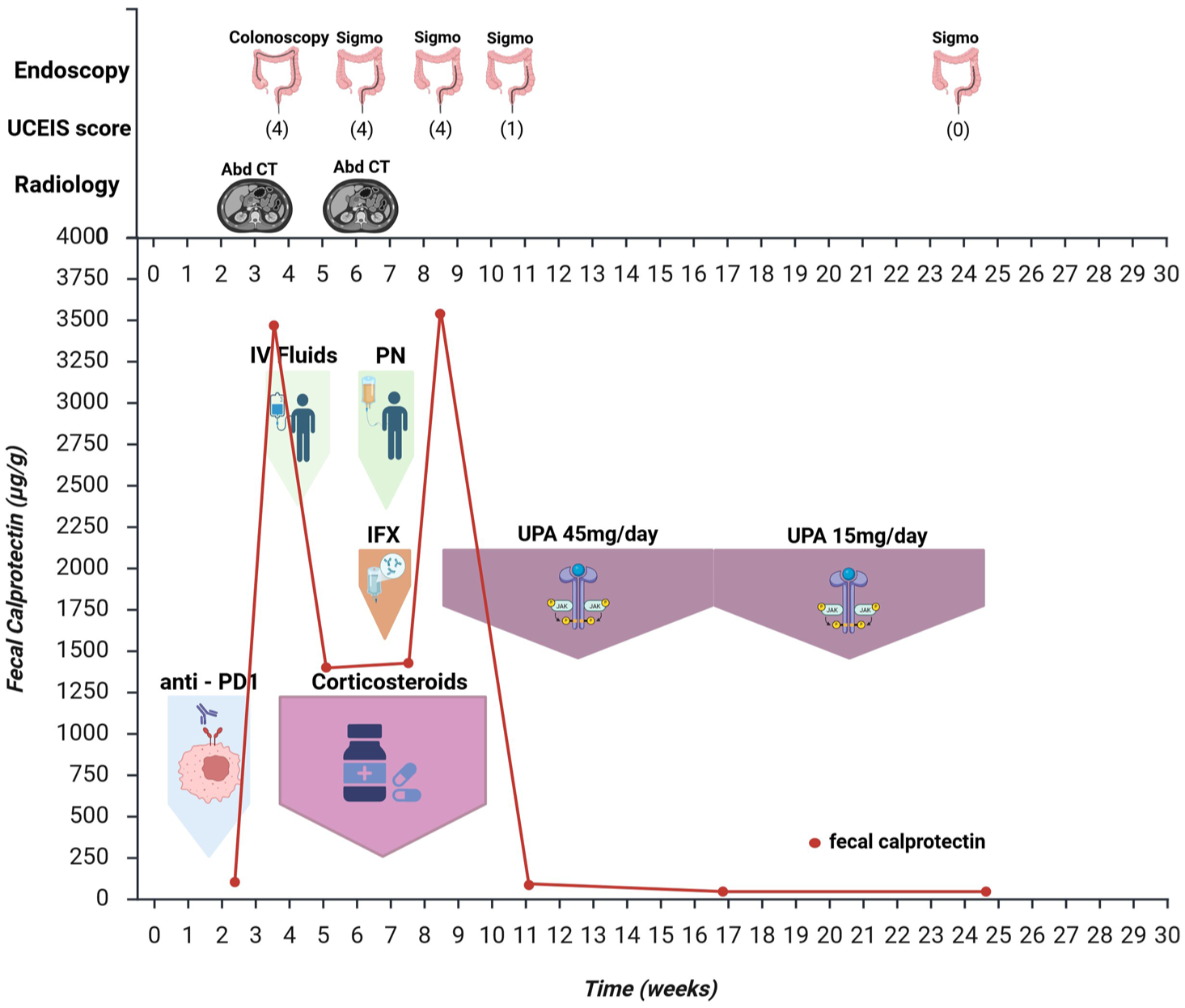
Chronological overview of examinations and clinical management.
Discussion
In this study, we report a case of severe ImC that was successfully treated with upadacitinib following failure to achieve remission with high-dose corticosteroids and infliximab. Data regarding the use of JAK inhibitors for ImC remains limited, primarily case series involving tofacitinib. There is currently only one other published case describing the successful induction of remission with upadacitinib in a patient with ImC refractory to biologics. 6
Although the exact pathophysiologic mechanisms underlying the inflammatory cascade triggered by ICI therapy have not been fully elucidated, ImC appears to share several molecular inflammatory pathways with IBD-type inflammation. This overlap likely explains the similar clinical presentation, endoscopic appearance and histopathological features between the two entities, 7 and thus similar therapeutic approaches for inducing remission are usually employed. 8
Both European and American oncology societies have issued treatment recommendations to support clinicians in managing this adverse event.3,9 These consensuses, however, are solely based on retrospective data, highlighting the need for high-quality prospective studies to support the establishment of standardized, evidence-based therapeutic approaches. In clinical practice, patients presenting with mild symptoms, classified as grade I diarrhoea according to the Common Terminology Criteria for Adverse Events (CTCAE; Table 1), are typically managed conservatively with dietary modifications, adequate hydration and antidiarrhoeal agents. 10 For moderate-to-severe presentations, current practice involves discontinuation of the ICI agent and initiation of oral corticosteroids. Patients who exhibit persistent symptoms or experience relapse during steroid tapering generally require hospitalization and intravenous corticosteroid therapy. All current recommendations suggest escalation to infliximab in cases that do not demonstrate improvement within 5–7 days of intravenous corticosteroids. 11 Although three doses of infliximab, 5 mg/kg, are usually sufficient to induce remission, there are no prospective data to guide further treatment adjustments in cases of infliximab-refractory disease. Notably, the existing treatment recommendations propose transition to vedolizumab; however, the evidence for this strategy remains limited, consisting primarily of two retrospective case series involving a total of 35 patients. 12 In our case, given the patient’s moderate ImC refractory to IFX, upadacitinib was selected as the next therapeutic step due to the benefit of oral administration and its rapid onset of action, in contrast to vedolizumab, which, according to the literature, can be associated with a slower clinical response. 3 Corticosteroids were quickly switched to oral and tapered over the first 4 weeks of upadacitinib therapy. Following consultation with the Infectious Diseases department, the patient also received oral ganciclovir alongside upadacitinib as prophylaxis due to the high immunosuppressive load. Colonic biopsies revealed only a single CMV-positive cell, and laboratory work-up revealed no other organ involvement, indicating low-level reactivation. Although a potential contribution cannot be entirely excluded, that low CMV burden was considered unlikely to induce primary colitis and likely played only a minimal role to the refractory nature of the ImC to IFX.
Severity grading of diarrhoea and colitis according to CTCAE.
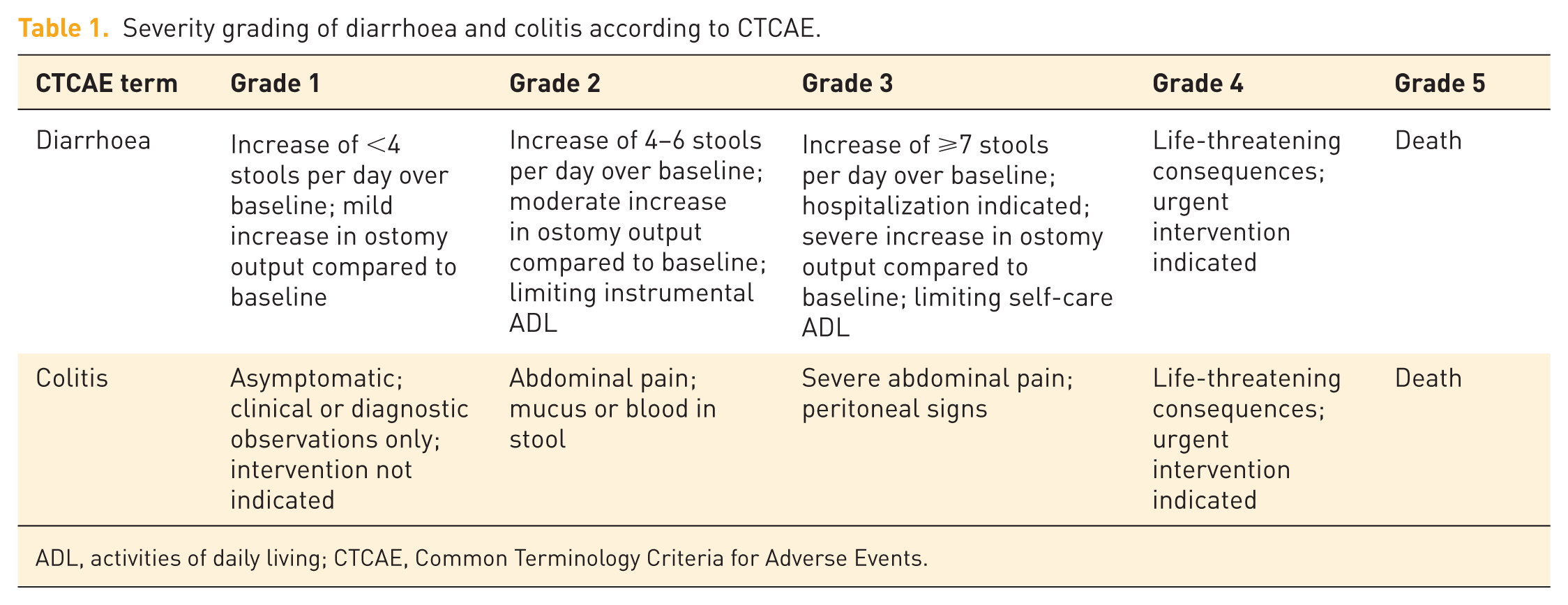
ADL, activities of daily living; CTCAE, Common Terminology Criteria for Adverse Events.
To date, no standardized treatment duration protocols exist, and current recommendations suggest that therapy should be individualized based on clinical, laboratory, endoscopic and histological data. 3 For patients receiving IFX or vedolizumab, infusions of standard doses at weeks 0, 2 and 6 are often sufficient, but in some cases treatment extension may be required depending on symptom burden and endoscopic findings.9,11 In our case, and in the absence of current recommendations, an 8-week course of high-dose upadacitinib was selected in line with strategies used in IBD patients for the induction of remission, followed by an additional 8 weeks at a lower dose. In parallel, the patient was closely monitored with clinical assessment, laboratory work-up, faecal calprotectin and endoscopy to detect any potential relapse. Although this approach was considered as safe and rational to achieve the best clinical outcome, further prospective studies and clinical trials are needed to better define the optimal duration of small molecules in patients with ImC.
Several pathogenic mechanisms of ImC have been proposed, including T-cell hyperactivation, intestinal microbiome dysregulation, increased secretion of pro-inflammatory cytokines and impaired epithelial barrier integrity. PD-1 receptor blockade interferes with the physiological regulation of immune responses, resulting in T-cell activation and subsequent impairment of mucosal immune tolerance. Overactivated CD8+ and CD4+ T lymphocytes contribute to the production of TNF-α, IFN-γ, IL-17, IL-6 and other pro-inflammatory cytokines, which are key mediators of the inflammatory cascade. 13 Excessive IFN-γ expression has been linked to JAK-STAT pathway upregulation and induction of intestinal epithelial cell apoptosis, followed by epithelial barrier disruption and microbial antigen translocation, mediating inflammatory activity. 14
A deeper understanding of the role of the JAK/STAT signalling pathway in the inflammatory response of ImC could provide critical insights for optimizing future therapeutic strategies. Notably, activation of the IL-6/JAK1 axis has been shown to promote the stabilization of PD-L1 expression in cancer cells. Thus, inhibition of JAK1 kinase activity may cause tumour cells to be more vulnerable to immunosurveillance, while suppression of IL-6 secretion could not only decrease the frequency of irAEs but also extend the clinical benefit of immunotherapy. 15 Given that upadacitinib selectively inhibits JAK1-dependent inflammatory mediators such as IL-6 and IFN-γ, both in vitro and in vivo, it may serve as a potential therapeutic strategy to manage immune-mediated toxicities arising from ICI treatment, such as ImC. 16
Of particular interest, data from two independent clinical trials indicate that combined administration of JAK inhibitors and ICIs could serve as a promising treatment for patients with specific types of cancers. Mathew et al., 17 in a phase 2 clinical trial including patients with metastatic non-small cell lung cancer, reported that the combination of an anti-PD1 agent with delayed induction of a JAK1-inhibitor resulted in increased antitumour response. Furthermore, Zak et al., 18 in a phase 1/2 clinical trial demonstrated that the combined administration of an anti-PD1 agent and a JAK1/2-inhibitor enhanced clinical efficacy in patients with Hodgkin lymphoma who had previously failed to respond to ICI monotherapy. They also reported a lower incidence of adverse events, and no patients discontinued treatment because of drug toxicity. Although the combined sample of patients receiving combined ICI and JAK-inhibitor therapy in these studies was small, and the populations did not specifically target patients with ImC, no GI irAEs were reported. This raises the question of whether JAK inhibitors might have a protective effect in this context; however, data from larger populations in phase III trials are needed to explore this possibility. JAK1-inhibitors have demonstrated an overall favourable safety profile across several autoimmune and haematological disorders compared with less selective JAK inhibitors. However, physicians should be aware of potential adverse events associated with JAK-1 inhibitor therapy, including viral and opportunistic infections, neutropenia and hepatotoxicity. 19 Thromboembolic events are particularly pertinent in patients with additional prothrombotic conditions such as colitis and cancer. 20 Future studies should define the thromboembolic risk in this patient population with multiple risk factors, as well as clarify the optimal dosing and treatment duration in patients with ImC.
In summary, this case report illustrates that treatment with upadacitinib can induce remission in ImC, highlighting the therapeutic potential of this JAK1-inhibitor. Emerging evidence further suggests that JAK1 inhibitors can also enhance antitumour responses, in combination with ICI, while reducing treatment-related toxicities. These promising results underscore the need for future prospective studies to evaluate the clinical utility of JAK1-inhibitors in ImC management and their potential integration into future standardized treatment guidelines.
Supplemental Material
sj-pdf-1-tag-10.1177_17562848261458694 – Supplemental material for Upadacitinib for anti-TNFα refractory immune checkpoint inhibitor–induced colitis: a case report
Supplemental material, sj-pdf-1-tag-10.1177_17562848261458694 for Upadacitinib for anti-TNFα refractory immune checkpoint inhibitor–induced colitis: a case report by Grigorios Petrousis, Charlotte R. H. Hedin, Stephan L. Haas, Hans Strid, Francesca Bresso and Katarina Bilén in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
The authors sincerely thank the patient for providing informed consent for the publication of this work. The patient’s generous cooperation was essential to the completion of this manuscript. We also express our sincere gratitude to our colleague Alexandros Arvanitis, Consultant Pathologist at Unilabs, Stockholm, for his valuable contribution in providing detailed histopathological images and descriptions, which significantly improved the quality of this manuscript. ![]() was created with the assistance of BioRender.com. In the course of preparing this manuscript, ChatGPT-4 was used to assist with language refinement and to enhance the clarity of the text. All content was subsequently carefully reviewed, revised and approved by the authors, who assume full responsibility for the accuracy and integrity of the final manuscript.
was created with the assistance of BioRender.com. In the course of preparing this manuscript, ChatGPT-4 was used to assist with language refinement and to enhance the clarity of the text. All content was subsequently carefully reviewed, revised and approved by the authors, who assume full responsibility for the accuracy and integrity of the final manuscript.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.