
Abstract
Background:
Acid exposure time (AET) yields inconclusive results in 10%–15% of patients undergoing 24-h ambulatory pH-impedance monitoring (multichannel intraluminal impedance-pH, MII-pH) for suspected gastroesophageal reflux disease (GERD), delaying diagnosis and appropriate management. The pHoenix score (pHx-s) was developed to reduce this diagnostic uncertainty. Its performance in Latin American populations remains uncharacterized.
Design:
Net reclassification index (NRI) analysis based on a retrospective cohort.
Methods:
A cohort of symptomatic adults who underwent high-resolution manometry, MII-pH, and upper endoscopy at Hospital Universitario San Ignacio, Bogotá (Colombia) was included. pHx-s was calculated as (upright AET × 0.991) + (supine AET × 1.286) and classified as normal (<7.06), borderline (7.06–8.45), or pathological (>8.45). Diagnostic performance and area under the receiver operating curve (AUC) were calculated. DeMeester score (>14.7) served as the reference standard. NRI analysis is presented independently for patients with and without confirmed GERD.
Results:
292 patients were included in the analysis (Median 61 years, 71.2% female, 79.1% with hiatal hernia (HH)). The AUC of pHx-s was 0.98 (0.963–0.992). At the lower threshold (7.06), sensitivity was 95.7% and specificity 99.1%; at the upper (⩾8.45), sensitivity 89.8%, and specificity 100%. pHx-s reduced inconclusive results from 13.0% (using exclusively AET criteria) to 4.1% (−68.5%, p < 0.001). Among inconclusive AET cases, pHx-s reassigned 55.3% as pathological and 18.4% as normal, with an overall NR improvement of 14.6%.
Conclusion:
In this Latin American cohort with a high prevalence of HH, pHx-s substantially reduced inconclusive GERD diagnoses and demonstrated excellent performance compared with the DeMeester score. These findings support the use of the pHx-s in diverse clinical settings.
Plain language summary
Diagnosing gastroesophageal reflux disease (GERD) can be difficult because the standard test gives unclear results in some patients. The pHoenix score is a newer tool designed to reduce this uncertainty. In this study, we evaluated the pHoenix score in 292 adults from Colombia who underwent testing for GERD. The score showed excellent accuracy and reduced unclear results from 13% to 4.1%. It also helped reclassify many patients whose initial test results were inconclusive. These findings suggest that the pHoenix score may help doctors diagnose GERD more clearly and guide treatment more effectively. Further studies in other populations are needed.
Keywords
Introduction
Gastroesophageal reflux disease (GERD) is a common condition 1 with the modern definition requiring objective evidence of pathological reflux in the presence of clinically relevant symptoms, as defined in the Lyon Consensus 2.0. 2 Up to 70% of symptomatic patients have a normal esophageal mucosa at endoscopy, which makes 24-h multichannel intraluminal impedance-pH (MII-pH) monitoring essential for establishing a definitive diagnosis. Among the parameters derived from this consensus, acid exposure time (AET) remains the central metric: values above 6% confirm GERD, values below 4% effectively exclude it, and values between these two thresholds yield inconclusive results. 2 These inconclusive results are obtained in approximately 10%–15% of patients undergoing ambulatory monitoring. They delay appropriate management, expose patients to prolonged empirical treatment, and complicate candidacy assessment for antireflux surgery.
Historically, the DeMeester score, 3 a composite index integrating six individual pH-metric parameters, has been accepted as a reference standard for GERD diagnosis, 4 as it performs well in identifying patients who need anti-reflux management and predicts outcomes, 5 however, its components do not have equal reproducibility or diagnostic value, with total AET considered the most reproducible parameter. 6 Moreover, it has not been incorporated into the Lyon Consensus 2.0 due to the complexity of its calculation and failure to model the disease as a continuum. While AET alone is simpler and closely associated with therapeutic response to proton pump inhibitors (PPI) and antireflux surgical outcomes, 2 it omits the contribution of supine acid exposure, a parameter that is independently associated with mucosal injury severity.7,8
The pHoenix score (pHx-s) was developed to overcome these limitations by combining the clinical robustness of the DeMeester score with the operational simplicity of AET, while also taking positional acid exposure into account. Calculated as (upright AET × 0.991) + (supine AET × 1.286), the score assigns greater importance to supine reflux burden and introduces a borderline category that accommodates diagnostic uncertainty rather than imposing binary classification. In its original derivation cohort using wireless Bravo pH capsule monitoring, 9 the pHx-s significantly reduced the proportion of the initial inconclusive cases and demonstrated excellent discriminative ability (area under the receiver operating curve (AUC) 0.957) when compared with the DeMeester score as the reference standard. At a threshold of 7.06, the pHx-s had a sensitivity (SE) of 94.4% and a specificity (SP) of 79.2%, whereas at an 8.45 cutoff, the SE was 87% and the SP was 95.8%. Subsequent validation using conventional 24-h catheter-based pH monitoring yielded comparable performance (AUC 0.996) with a 57.1% relative reduction in inconclusive diagnoses. 10
Despite these consistent findings, the available validation data are derived exclusively from North American and European populations. To date, no study has examined the performance of the pHx-s in a Latin American cohort, despite the fact that this is a setting with potentially distinct epidemiological characteristics. This study aimed to compare the results of two physiologic metrics, the pHx-s and the DeMeester score (assumed as the reference standard), in a consecutive cohort of symptomatic adults with suspected GERD in Latin America, and to determine whether the pHx-s can correctly reassign patients with inconclusive results according to AET.
Methods
Study design and population
We conducted an NRI analysis based on a retrospective cohort of symptomatic patients with suspected GERD, who presented to the Gastrointestinal Physiology department at Hospital Universitario San Ignacio in Bogotá (Colombia) between January 2022 and December 2025. Patients over 18 years of age with either typical or atypical GERD symptoms, who had discontinued PPI therapy and undergone high-resolution manometry (HRM), MII-pH, and an upper endoscopy within no more than 6 months apart, were included. Those with incomplete studies due to technical failure or data omission, a history of upper esophagogastric surgery, or use of medications that alter esophageal motility (metoclopramide, anticholinergics, opioids) were excluded. The protocol was approved by the Ethics Committee of the Pontificia Universidad Javeriana (FM-CIE-0135-26). The report conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 11
Clinical data
Patients were identified through the institutional procedure registry and subsequently verified by review of medical records. Following the Chicago Consensus, HRM was performed after a minimum fast of 6 h, using a solid-state catheter with 36 circumferential sensors (Medtronic, Duluth, GA, USA). 12 The pH-metry was performed using a Versaflex Z® catheter placed 5 cm above the proximal margin of the lower esophageal sphincter, after discontinuation of PPIs, H2 antagonists, antacids, and prokinetics for at least 7 days. Tracings were then analyzed using Reflux Reader Software v6.1.1.11. The Los Angeles (LA) classification was systematically applied during endoscopy for the characterization of erosive esophagitis. 13 Hiatal hernia (HH) was evaluated in HRM during the resting phase, measuring the distance from the lower esophageal sphincter to the diaphragmatic crura.
Statistical analysis
Sampling was consecutive, selecting all the patients who met the inclusion criteria in the study period. Continuous variables were assessed for normality using the Shapiro–Wilk test and were described as mean ± standard deviation or median with interquartile range (IQR), as appropriate. Categorical variables were expressed as absolute frequencies and percentages and were compared using the Chi-square test or Fisher’s exact test, as appropriate.
Sensitivity, specificity, predictive values, and area under the receiver operating characteristic (ROC) curve of the pHx-s were calculated using DMS as the reference standard. In order to assess the extent to which the diagnosis of GERD is correctly or incorrectly reassigned, the net reclassification index (NRI) 14 was used based on a category-based approach compared with AET. First, the entire sample was stratified into positive (>6%), inconclusive, or negative (<4%) categories according to AET, separating groups with confirmed or excluded diagnoses according to our reference standard (DeMeester score >14.7 or ⩽14.7, respectively) for the analysis. Within each group, the percentage of patients correctly or incorrectly reassigned by the pHx-s was assessed. Categories for pHx-s considered the lower (7.06) and upper (8.45) thresholds described in the original study. 9 Changes in classification were reported independently: event NRI (confirmed diagnosis of GERD) and non-event NRI (exclusion of GERD). The difference between the proportions of inconclusive cases obtained by both methods were analyzed using a Z test for comparison of proportions. Subgroup analysis of NRI in patients with HH >2 cm was performed. A p-value <0.05 was considered statistically significant. All analyses were performed using STATA version 16.1 (StataCorp, College Station, TX, USA).
Results
Of 1552 HRM studies reviewed in this study period, 1237 were excluded since MII-pH or complementary upper endoscopy data were unavailable in the pre-specified 6-month time window, and 23 for a history of esophagogastric surgery (Figure 1). A cohort of 292 patients was analyzed (median age 61, IQR 50–68.5 years; 71.2% female). HH was present in 79.1% of patients, and conclusive endoscopic findings of GERD were present in 7.5%, 1.7%, and 4.8% according to the LA grade B, C, and D esophagitis classification, respectively. Barrett’s esophagus and peptic stenosis were identified in 2.4% and 1.7% of patients, respectively. Regarding pH monitoring metrics, median AET was 5.9% (IQR 1.9–13.7), upright AET 6.15% (IQR 2.05–13.85), supine AET 1.4% (IQR 0–12.35), DeMeester score 22.7 (IQR 8.3–50.2), pHx-s 11.21 (IQR 3.17–27.84), and the median of total reflux episodes was 66.5 (IQR 36.5–117; Table 1).
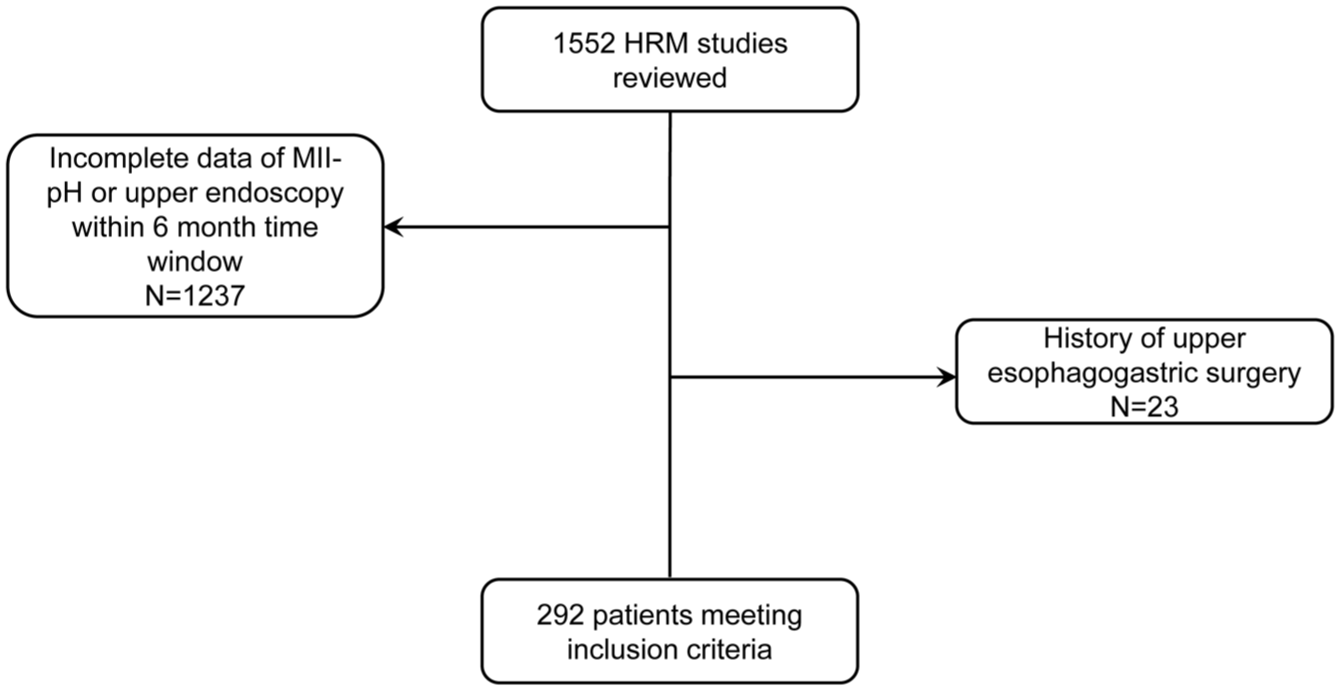
Flow diagram of the included patients.
Clinical characteristics, as well as endoscopic, manometric, and pH monitoring findings of the included patients.
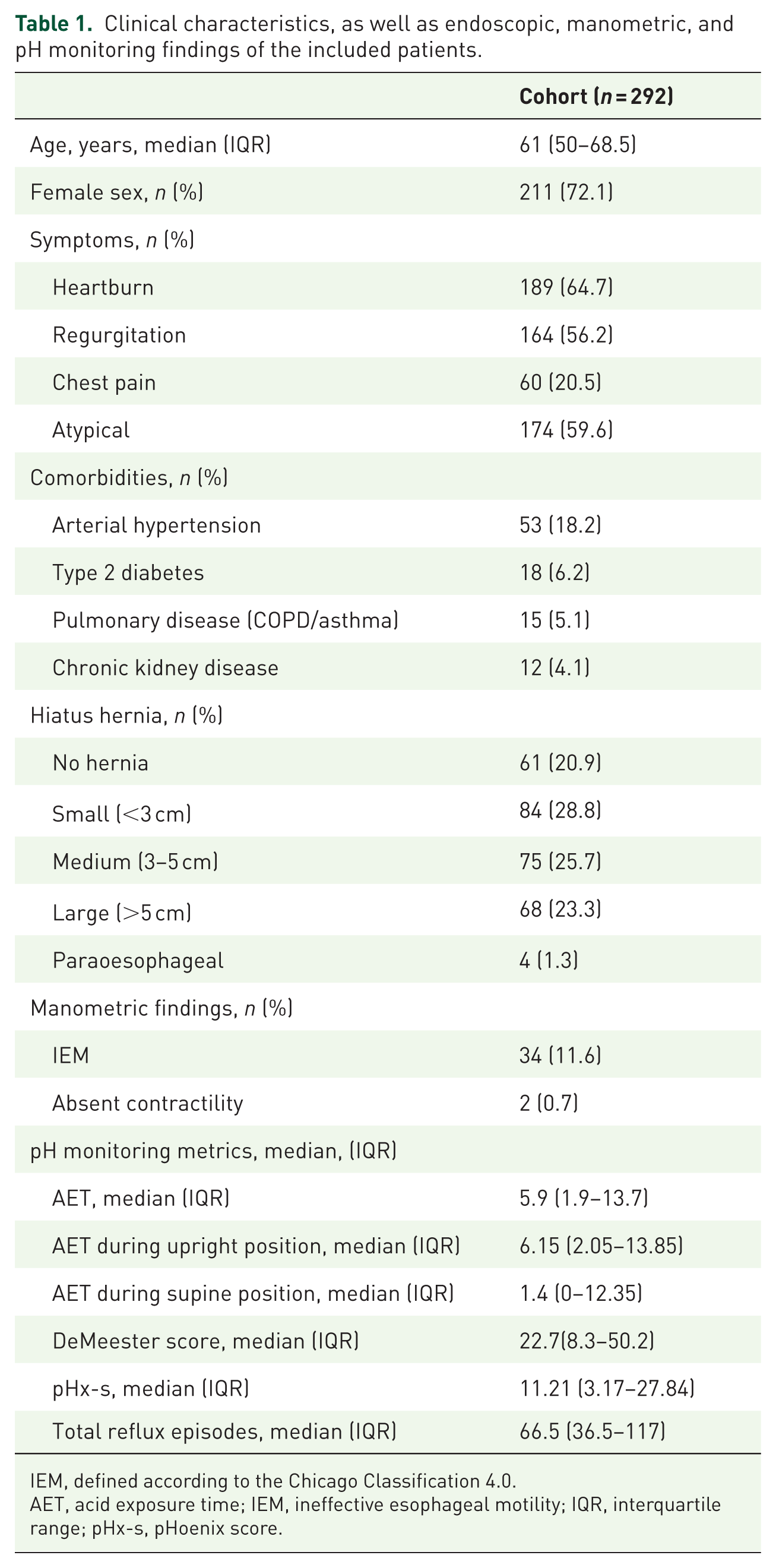
IEM, defined according to the Chicago Classification 4.0.
AET, acid exposure time; IEM, ineffective esophageal motility; IQR, interquartile range; pHx-s, pHoenix score.
Performance of pHx-s against the DeMeester score
The diagnostic performance of the pHx-s is presented in Supplemental Table 1. At the lower threshold (7.06), the score showed a sensitivity of 95.7% and a specificity of 99.1%. Using the upper threshold of ⩾8.45, the sensitivity was 89.8% and the specificity 100%, with a negative likelihood ratio (LR−) of 0.10. The discriminative ability of the pHx-s was excellent (Figure 2), with an AUC of 0.973 (CI 0.955–0.990) using the DeMeester score as the reference standard.
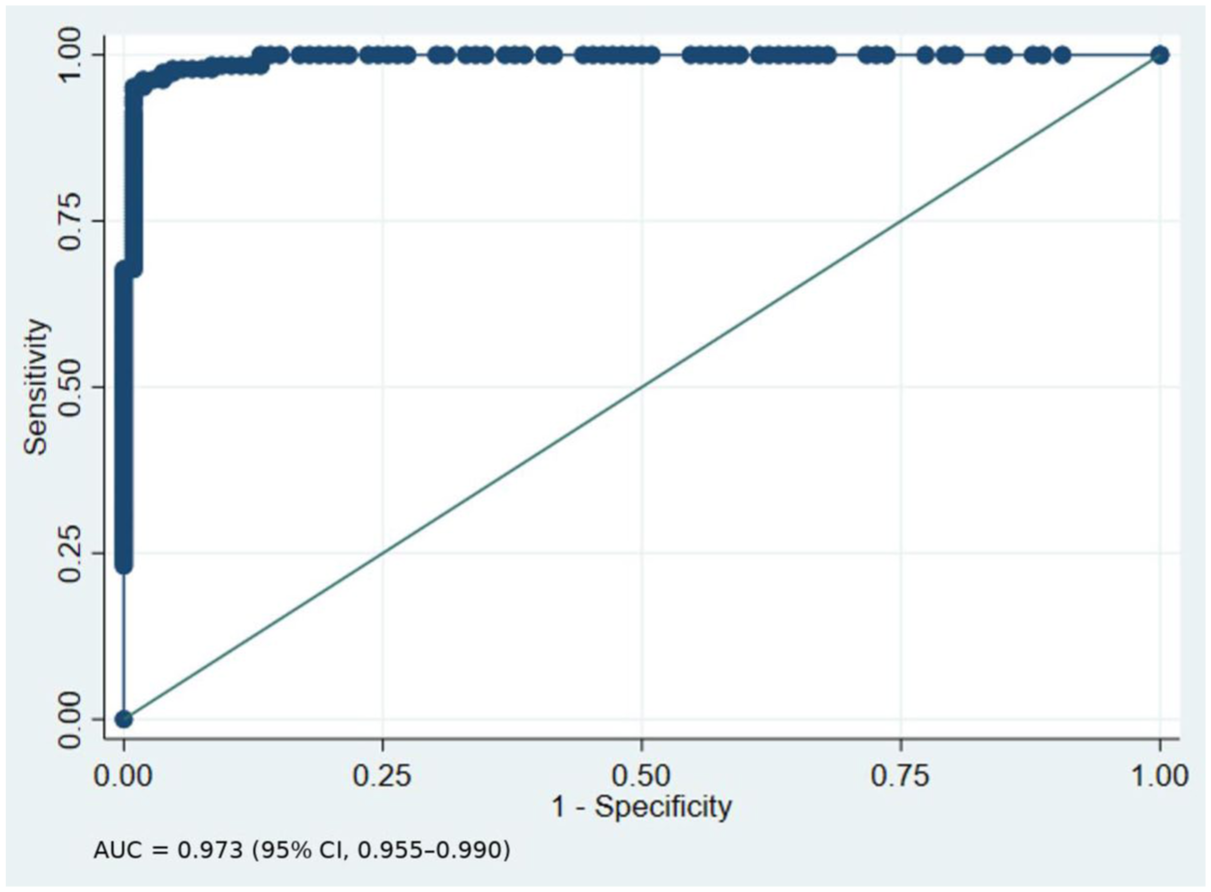
Performance analysis of the Phoenix score using the area under the receiver operating curve.
NRI analysis
According to AET, 111 patients (38.0%) had normal (<4%), 38 (13.0%) inconclusive (4%–6%), and 143 (49.0%) pathological values (>6%). When classified by the pHx-s, 112 patients (38.4%) were categorized as normal (<7.06), 12 (4.1%) borderline (7.06–8.45), and 168 (57.5%) pathological (>8.45). The pHx-s reduced the proportion of inconclusive studies, decreasing the rate from 13.0% using AET alone to 4.1% (p < 0.001), representing a relative reduction of 68.5% in inconclusive diagnostic results. Among patients with inconclusive AET (4%–6%), the pHx-s reassigned 21 patients (55.3%) as pathological, 7 patients (18.4%) as normal, while 10 patients (26.3%) remained in the borderline category (Table 2).
Concordance between AET and pHx-s.
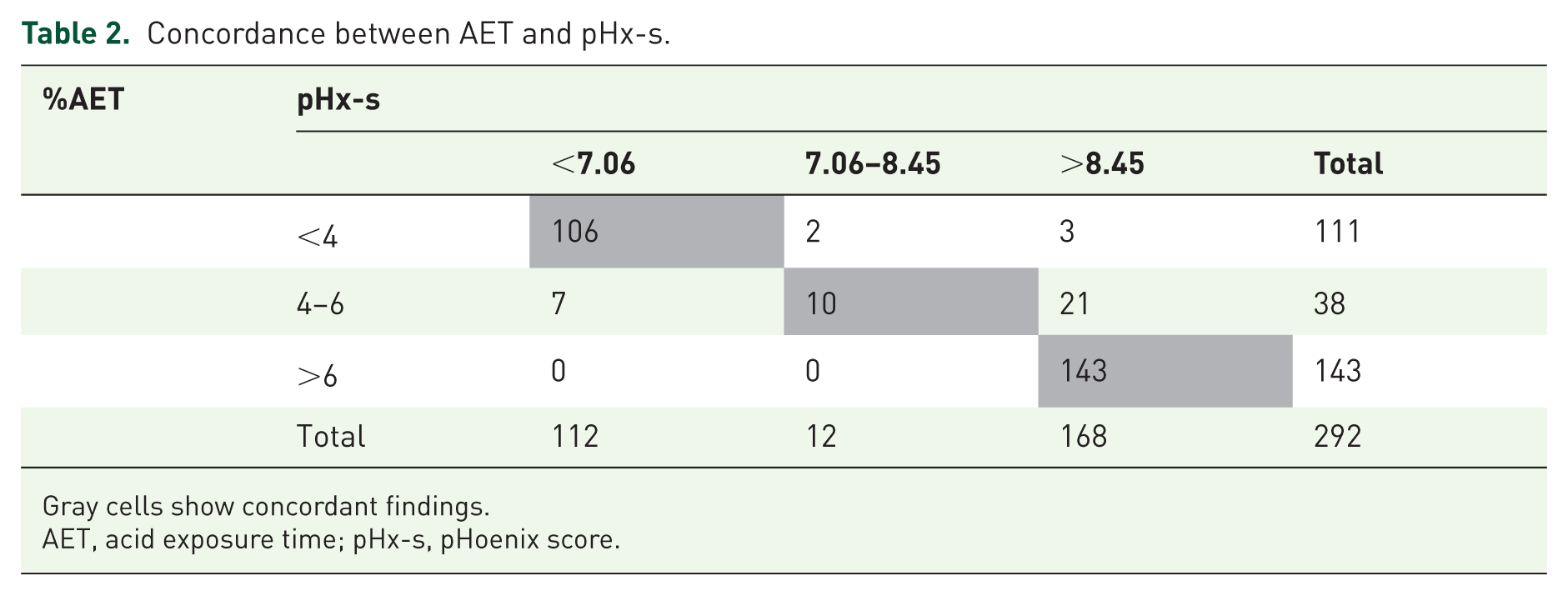
Gray cells show concordant findings.
AET, acid exposure time; pHx-s, pHoenix score.
Using the DeMeester score as the reference standard, 186 patients (63.7%) had GERD and 106 patients (36.3%) did not. In patients without GERD, all patients (102 out of 102 patients) with AET <4% were correctly classified as normal by the pHx-s. In the inconclusive AET subgroup, 3 out of 4 were reassigned as normal ((a) in Table 3). In the GERD group, the pHx-s classified all 143 patients with AET >6% as pathological. Among patients with inconclusive AET, 21 of 34 patients were reassigned as pathological, 9 remained borderline, and 4 were classified as normal. Lastly, pHx-s correctly reassigned five out of nine patients with AET<4% ((b) in Table 3).
NRI of AET with pHx-s, using DeMeester as reference standard.
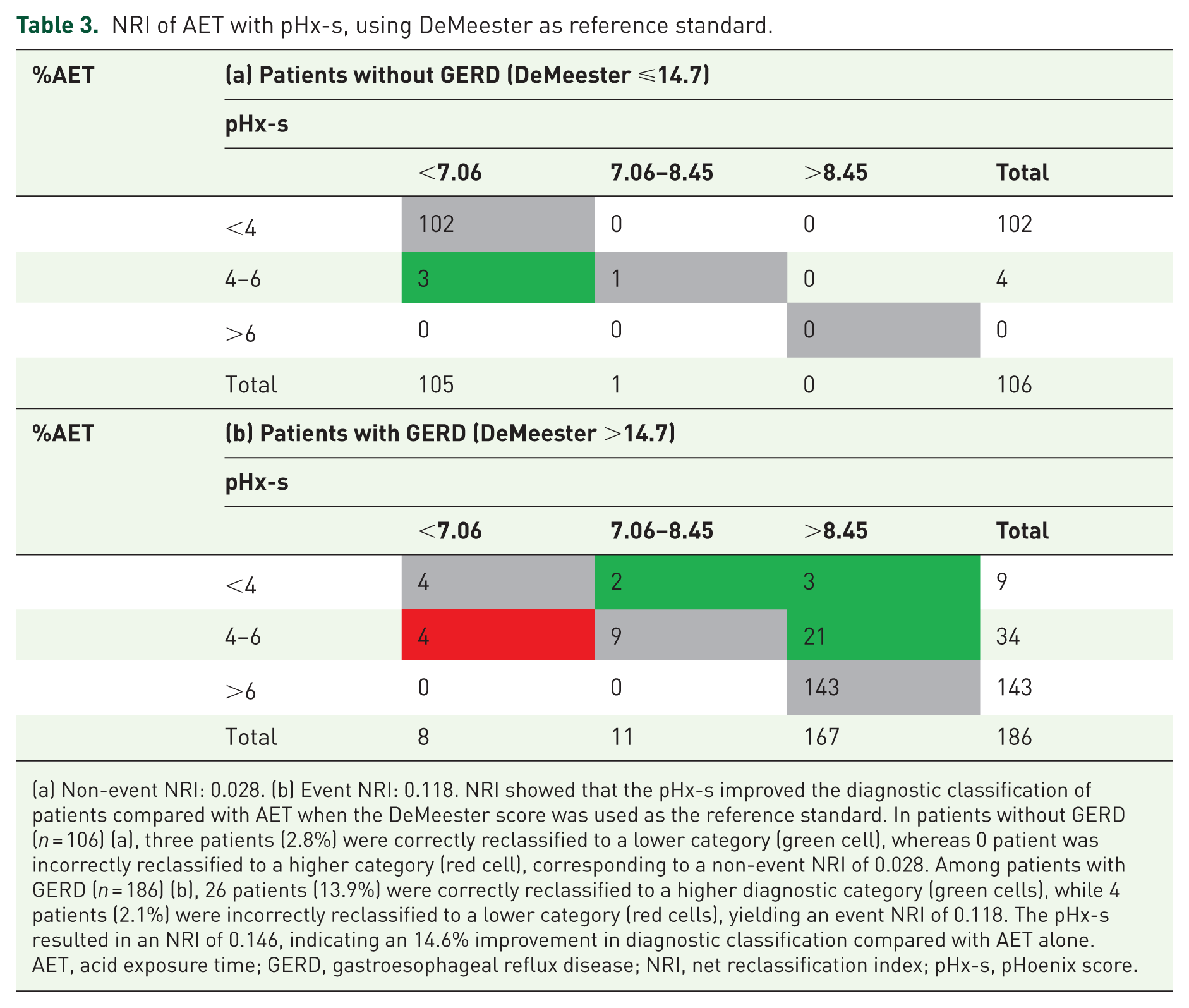
(a) Non-event NRI: 0.028. (b) Event NRI: 0.118. NRI showed that the pHx-s improved the diagnostic classification of patients compared with AET when the DeMeester score was used as the reference standard. In patients without GERD (n = 106) (a), three patients (2.8%) were correctly reclassified to a lower category (green cell), whereas 0 patient was incorrectly reclassified to a higher category (red cell), corresponding to a non-event NRI of 0.028. Among patients with GERD (n = 186) (b), 26 patients (13.9%) were correctly reclassified to a higher diagnostic category (green cells), while 4 patients (2.1%) were incorrectly reclassified to a lower category (red cells), yielding an event NRI of 0.118. The pHx-s resulted in an NRI of 0.146, indicating an 14.6% improvement in diagnostic classification compared with AET alone.
AET, acid exposure time; GERD, gastroesophageal reflux disease; NRI, net reclassification index; pHx-s, pHoenix score.
NRI showed that the pHx-s improved the diagnostic classification of patients compared with AET when the DeMeester score was used as the reference standard, yielding an event NRI of 0.118 and a non-event NRI of 0.028. Overall, the pHx-s resulted in an NRI of 0.146, indicating an 14.6% improvement in diagnostic classification compared with AET alone (Table 3).
In patients without GERD (DeMeester ⩽14.7), pHx-s failed to correctly classify 1 case, whereas in patients with GERD (DeMeester >14.7), PHx-s failed to correctly classify 19 cases. Their characteristics are described in Supplemental Table 2.
Subgroup analysis of NRI in patients with HH >2 cm
In the subgroup of patients with HH >2 cm, the pHx-s demonstrated excellent diagnostic performance, with an AUC of 0.969 (95% CI 0.933–0.989). At the lower threshold (⩾7.06), sensitivity was 97.3% and specificity 96.6%, while at the higher threshold (⩾8.45), sensitivity was 93.8% and specificity 96.7%. Net reclassification analysis showed an overall NRI of 0.094, with a non-event NRI of 0.033 (Supplemental Table 3(A)) and an event NRI of 0.061 (Supplemental Table 3(B)).
Discussion
In this study, we not only found that the pHx-s had excellent diagnostic accuracy, but we also demonstrated that, compared with AET alone, the pHx-s can reduce the number of inconclusive studies and correctly reassign them. Furthermore, the 69% relative reduction in inconclusive studies and the 14.6% total net reclassification improvement support its use. Our finding aligns with the 57.1% overall reduction in inconclusive AETs in the original 24-h pH monitoring validation cohort. 10 An Italian cohort also found a 59.4% relative decrease in borderline diagnoses. 15
The high prevalence of HH in our study is a unique characteristic compared to the previously described cohorts, as this adds novel information for the utility of the pHx-s in this particular subgroup. These findings are consistent with the original pHx-s derivation study, 9 in which patients with borderline AET reassigned as pathological by pHx-s showed a higher prevalence of HH >2 cm and Barrett’s esophagus, supporting the hypothesis that pHx-s may effectively capture EGJ integrity and GERD burden beyond AET alone. In our subgroup analysis restricted to patients with HH >2 cm, the pHx-s maintained excellent diagnostic performance, AUC 0.969 (95% CI 0.933–0.989), with high sensitivity and specificity across thresholds. However, the magnitude of reclassification improvement was attenuated compared with the overall cohort (NRI 0.094 vs 0.146), suggesting that while the direction of effect remains consistent, the incremental value of pHx-s over AET may be reduced in patients with more advanced anatomical disruption. This finding is physiologically plausible, as in the presence of significant EGJ impairment, acid exposure metrics alone may already capture most of the reflux burden, thereby limiting the additional discriminatory contribution of composite scores. 16
Among the 20 patients with discordant pHoenix and DeMeester classifications (Supplemental Table 2), most cases corresponded to patients with a positive DeMeester score in whom the pHx-s did not classify GERD as pathological. When these cases were reviewed according to their AET and pHx-s categories, several physiologic patterns became apparent. The first group, highlighted in orange, included patients with a positive DeMeester score but both AET and pHx-s in the inconclusive range. These patients had borderline total AET, predominantly upright acid exposure, and minimal or absent supine reflux, suggesting that the DeMeester score may have been driven by recurrent or prolonged upright acid events, while the pHx-s appropriately maintained them in a borderline category rather than classifying them as definitively pathological.
The second group, highlighted in blue, included patients with positive DeMeester scores and inconclusive AET, but negative pHx-s. These cases also showed borderline total AET, low supine acid exposure, and variable MNBI values, suggesting that the lower pHx-s classification may be explained by the limited contribution of supine reflux to the overall acid burden. In this setting, the pHx-s may be less likely to classify GERD as pathological when reflux is predominantly upright and does not reach the weighted threshold.
The third group, highlighted in purple, consisted of patients with a positive DeMeester score, a negative AET, and an inconclusive pHx-s. These cases may represent an intermediate phenotype, in which total AET remains below the pathological threshold but some degree of reflux burden, particularly positional or prolonged reflux, still increases the pHx-s into the borderline range.
The fourth group, highlighted in gray, included patients with a positive DeMeester score but both negative AET and negative pHx-s. In these cases, most objective metrics did not support pathological reflux burden, suggesting that the discordance may reflect limitations of the DeMeester score as a composite reference standard rather than true failure of the pHx-s. However, the presence of low MNBI in some patients suggests that chronic reflux-related mucosal impairment may still be present despite non-pathological acid exposure thresholds.
Since AET, DeMeester, and pHx-s are all derived from acid metrics, their correlation in most of the GERD spectrum is not surprising. Thus, the principal limitation of this study probably lies in the use of the DeMeester score as a reference standard since other novel scores, such as Lyon and Milan, lack validation in the Latin American population. Nevertheless, using the DeMeester score as a reference standard allows direct comparison with the developmental and validation cohorts. Another limitation is the large number of patients excluded due to the lack of concurrent endoscopy and pH monitoring. However, this approach ensures a more comprehensive assessment of the true diagnosis of reflux when interpreting physiological patterns.
Finally, some authors have argued that the NRI may not be a reliable metric, as it overlooks the varying severity of different types of misclassification errors—each of which can have distinct clinical implications for patients. 17 In our analysis, we report both correct and incorrect reassignments among GERD and non-GERD patients according to the DeMeester score as a reference standard, facilitating interpretation by allowing recognition of the specific consequences associated with each type of error in both groups. The ability to reduce the proportion of inconclusive diagnoses carries implications that extend well beyond diagnostic accuracy. Patients with borderline AET often spend months or even years in an uncertain diagnostic state, continuing empirical PPI therapy without objective confirmation of disease, a situation that is frustrating for patients and costly for health systems alike. Early objective diagnosis has been estimated to save up to $1197–$6303 per patient over a 10-year period by avoiding unnecessary PPI use. 18
Conclusion
pHx-s is a useful novel metric that can reduce the proportion of inconclusive GERD cases and correctly reassign them. Further studies using a more comprehensive reference standard are needed to strengthen the implications of its use in clinical practice.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261463424 – Supplemental material for Does the pHoenix score reduce the inconclusive GERD diagnosis: a net reclassification index analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848261463424 for Does the pHoenix score reduce the inconclusive GERD diagnosis: a net reclassification index analysis by Raúl A. Cañadas, Freddy A. Ávila, Albis C. Hani, Juan P. García, Carlos A. Rivera, Oscar M. Muñoz and Juan S. Hernández in Therapeutic Advances in Gastroenterology
Supplemental Material
sj-docx-2-tag-10.1177_17562848261463424 – Supplemental material for Does the pHoenix score reduce the inconclusive GERD diagnosis: a net reclassification index analysis
Supplemental material, sj-docx-2-tag-10.1177_17562848261463424 for Does the pHoenix score reduce the inconclusive GERD diagnosis: a net reclassification index analysis by Raúl A. Cañadas, Freddy A. Ávila, Albis C. Hani, Juan P. García, Carlos A. Rivera, Oscar M. Muñoz and Juan S. Hernández in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.