
Abstract
Inflammatory bowel diseases (IBD) are increasing worldwide, requiring multidisciplinary care and coordinated research infrastructures. Leveraging Israel’s integrated healthcare system with IBD centers of specific and complementary research expertise, a national collaborative consortium was established: the Israeli IBD Research Nucleus (IIRN). In this narrative article, we review a decade of IIRN structure, scientific outputs, and lessons learned. The IIRN included five tertiary academic IBD referral centers across Israel, with expertise in epidemiology, mucosal immunology, diet and microbiome, imaging, and psychosocial care. We summarized the IIRN key activities, findings, and contributions across these domains. Publications (2015–2025) were identified using a structured bibliometric approach and included studies aligned with core research programs of the IIRN. This collaborative consortium has been supported since its inauguration by the Leona M. and Harry B. Helmsley Charitable Trust, providing funding, advice, and partnership. The IIRN provided significant contributions in several domains. It established a population-based nationwide registry (epi-IIRN) that integrates data from the four national health maintenance organizations, enabling studies of disease prevalence, course, comorbidities, and treatment patterns. Prospective cohorts of patients with Crohn’s disease provided longitudinal insights linking multidisciplinary programs, Mediterranean diet and lifestyle, and psychosocial interventions with patient-reported outcomes, inflammatory markers, and microbiome features. Integrating imaging, video-capsule endoscopy, and biomarker assessment informed monitoring strategies and treat-to-target concepts. Exploratory translational work in microbiome, transcriptomics, and therapeutic drug monitoring refined insights regarding treatment response and sequencing. Artificial intelligence applications explored image and report interpretation to predict Crohn’s disease. The IIRN experience illustrates how coordinated national collaborations can leverage epidemiology, prospective cohorts, translational research, and multidisciplinary care programs. This experience highlights both the opportunities and challenges of shared research infrastructure and may inform similar collaborative efforts in other healthcare settings.
Plain language summary
Inflammatory bowel diseases (IBD) are complex inflammatory disorders with increasing global prevalence. To address disease complexity, while focusing on patients and human-derived biomaterials to improve research and care, we established a national-level partnership: the Israeli IBD Research Nucleus (IIRN). The IIRN includes five large academic tertiary referral IBD centers in Israel. Each center contributes their own expertise (for example: population health, immunology, diet and the gut bacteria, medical imaging, and mental health support). Here we reviewed IIRN activities, key achievements and impact. We also evaluated all scientific papers published from 2015 to 2025 that either used IIRN shared resources or focused on main IIRN research areas. The IIRN has been supported since it began by the Leona M. and Harry B. Helmsley Charitable Trust, which provided funding support and partnership. Key activities included building a nationwide registry; following well-described groups of patients over time to study links between patient-related factors; creating shared tools and standards for tests used in IBD care (including imaging and biological measurements); and implementing early work in artificial intelligence. Overall, the IIRN produced multiple scientific papers which were cited frequently. Our 10-year experience suggests that long-term teamwork and collaboration can produce meaningful results that single centers cannot achieve, and it can help translate research into better care. The IIRN model may be useful for other countries or disease areas that need strong collaboration to improve outcomes.
Introduction
The care of patients with inflammatory bowel diseases (IBD) has become increasingly complex. With rising prevalence worldwide 1 and the emerging treatment and monitoring options, there is a need for multidisciplinary teams (MDT) to manage the disease and advance meaningful research infrastructures that can integrate epidemiology, clinical studies, and translational research. These changes require more than co-authorships or cross-referrals of patients, but rather a true collaboration as a joint infrastructure.
Israel’s unique environment presents a special opportunity to pursue that goal. Large numbers of ethnically diverse patients with IBD residing at geographically accessible distances, integrated health management organizations (HMOs), a paperless centralized electronic medical record (EMR) system, and a high publication rate per capita 2 have cultivated the path to create such collaboration. The Israeli IBD Research Nucleus (IIRN) was founded in 2014, aiming to create a functioning consortium that will provide meaningful output and represent unique Israeli aspects that could be further generalized. The collective endeavor established a cross-disciplinary shared effort, informed research methodologies, and most importantly, established the perception that sharing data, ideas, and practices makes the participating partners grow stronger and achieve higher accomplishments.
In this paper, we aim to distill over a decade of experiences, insights, outputs, and contributions. We audit the impact of the IIRN through shared values, flagship scientific advancements, and bibliometrics, alongside faced challenges and future directions.
IIRN structure and operational approach
The IIRN unites five tertiary academic IBD referral centers: Rabin Medical Center (RMC), Sheba Medical Center, Shaare Zedek Medical Center (SZMC), Soroka Medical Center (SMC), and Rambam Healthcare Campus (RHCC). These centers span across northern, central, and southern Israel. All centers are affiliated with a medical faculty, including Tel Aviv University (Rabin and Sheba Medical Centers), Hebrew University of Jerusalem (SZMC), Ben-Gurion University (SMC), and the Technion (RHCC). This national spread allows for diverse patient populations, representing Jewish, Arab, Druze, and Bedouin.
The principal investigators from each center form the steering committee and convene periodically to set priorities and discuss cross-site projects. The consortium is led by an administrative and scientific central board that coordinates data sharing and collaboration. Each IIRN center keeps its independent research and expertise, while receiving insights and advice from other IIRN collaborators and aligning its projects in coordination with other centers’ studies.
Periodic steering committee meetings with scientific interactions were conducted several times a year on an ad hoc basis. Extended meetings with external international advisors were held annually to guide the projects’ direction.
This work was made possible by the generous support of The Leona M. And Harry B. Helmsley Charitable Trust. The Helmsley Charitable Trust enabled the establishment of the IIRN unique structure, as well as the specific centers’ projects. Throughout the years, each IIRN center leveraged scientific and financial support to achieve further scientific collaboration and further financial support.
Review methods
We conducted a narrative, consortium-authored review of scientific advancements, translational findings, and patient-related programs. A pre-defined inclusion criterion included studies arising from IIRN-associated infrastructure or multicenter collaborations in the core IIRN research domains. These were synthesized into a conjoint report demonstrating how projects from the different centers merged and evolved throughout the years. We profiled past and present IIRN members to illustrate the disciplines that accounted for the diversity of our collaboration. We note key challenges, failures, and lessons.
To enumerate the number of peer-reviewed publications written as part of the IIRN work throughout the years, we performed a structured bibliometric search using the Scopus database (Elsevier). Two complementary search strategies were applied: (1) Core IIRN publications—we queried studies explicitly affiliated with the IIRN and authored by the predefined core investigators, representing the five participating centers; (2) IIRN-related collaborative outputs—we conducted a broader search of IBD-related publications authored by the same group of investigators between 2015 and 2025, using title/abstract keywords of IIRN domains and author identifiers. Articles were screened and classified as IIRN-related if they reflected multicenter collaboration, use of IIRN infrastructure, or were conceptually derived from IIRN cohorts and research programs. Full queries are provided in the Supplemental Methods.
Results
Throughout the years, the IIRN evolved into a coordinated national-level network linking five academic tertiary IBD centers and multiple interconnecting research domains. The novelty of the IIRN stems from focusing on one disease from pathogenesis to clinical practice, including patient-level, biological studies, and “supra patient” with epidemiology-related studies, adopting an approach of harmonizing core variables and outcomes over uniformity of a sole study focus. The consortium’s flagship domains and exemplary studies are summarized in Table 1.
Flagship studies of the IIRN.
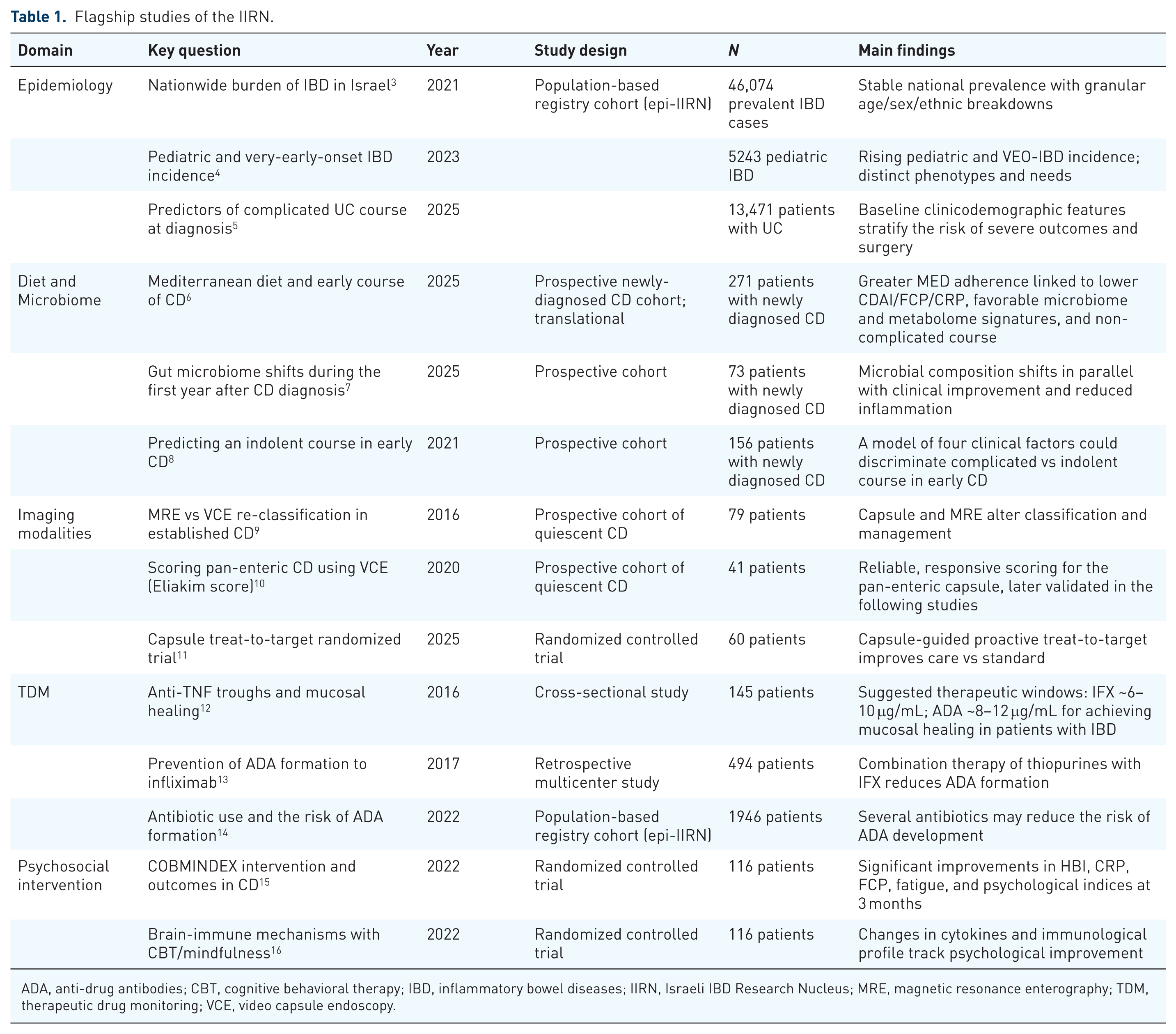
ADA, anti-drug antibodies; CBT, cognitive behavioral therapy; IBD, inflammatory bowel diseases; IIRN, Israeli IBD Research Nucleus; MRE, magnetic resonance enterography; TDM, therapeutic drug monitoring; VCE, video capsule endoscopy.
The following studies are examples presenting the variety of levels and types of evidence.
A nationwide epidemiological data backbone
The epidemiological group of the IIRN (epi-IIRN), Israel’s nationwide IBD cohort, leverages a unique healthcare data infrastructure, in which each resident has a personal ID that connects the four national payers’ HMOs EMRs, thereby covering 98% of the population. This infrastructure enables a population-based, unselected sampling to support research across epidemiology, management, imaging, outcomes, and risk prediction; Israel’s demographics, including Jewish and Arab communities alongside immigrants, create a unique setting to parse genetics, environment, and acculturation. Epi-IIRN’s signal achievement that laid foundation to subsequent scientific research was the uniting of all four national HMOs into a single, population-scale de-identified database and providing a highly accurate algorithm to identify IBD, based on validation and curation by all IIRN centers.
The epi-IIRN platform yielded key studies that demonstrated how IBD prevalence has nearly doubled since 2005, with Crohn’s disease (CD) surpassing ulcerative colitis (UC), alongside heterogeneous trends across age groups and populations. 3 Findings suggest an epidemiologic transition influenced by environmental and socioeconomic factors, 17 with rising pediatric incidence. 4 Risk stratification reflects genetic susceptibility, early-life exposures, and socioeconomic context,18,19 while longitudinal data suggest preclinical disease signals years before diagnosis. 20 Patients with IBD also exhibit increased risk for autoimmune comorbidities.21–23 We illustrated how treatment patterns have shifted toward earlier biologic use with more selective immunomodulator strategies,24–27 yet found that some disease complications remain despite therapeutic advances,28,29 and identified key predictors of worse outcomes.30–33 Collaboration between adult and pediatric gastroenterologists enabled representation of pediatric populations with age-spanning analyses.
Prospective cohorts with granular multi-level data
A key feature of the IIRN is the recruitment of patients with well-defined phenotypes and longitudinal follow-up at prespecified time points, enabling comprehensive multi-level assessment of clinical data, inflammatory, and exploratory markers. This approach has resulted in several medium-sized, center-specific cohorts, with complementary recruitment strategies and limited overlap. Examples include an inception cohort of patients with newly diagnosed CD demonstrating short- and long-term clinical outcomes, microbial shifts, effects of dietary patterns, and the importance of multidisciplinary care in a real world setting6–8; a cohort of patients with CD in remission defining remission depths and suggesting therapeutic interventions to mitigate risk of flare11,34–36; a cohort of patients initiating therapy with anti-TNF with prospective therapeutic drug monitoring (TDM)13,37–40; and a cohort of patients with mild-to-moderate CD demonstrating factors associated with a higher psychosocial burden, and the effects of a mindfulness-based cognitive behavioral interventions to modify CD outcomes.15,16,41–43
Each of these cohorts had a main clinical plan and follow-up term, and its biomarker analyses enabled the addition of mechanistic insights spanning a whole spectrum of CD: from diagnosis, to flare, to remission. Collectively, these complementary cohorts aimed to capture the longitudinal journey of patients with CD.
Empowering MDT approach
The care for patients with IBD extends beyond the gastroenterologist, a notion shared and promoted by IIRN centers, advancing the MDT approach that spans adult and pediatric gastroenterology, colorectal surgery, dermatology, obstetrics/gynecology, pediatrics, IBD nursing, dietetics, and psychosocial care. Emerging real-world evidence from other cohorts has also highlighted the importance of metabolic comorbidities in IBD, including associations between type 2 diabetes and worse outcomes in CD, further reinforcing the need for broader systemic and MDT assessment of the metabolic intake and status of patients with IBD. 44 Concordantly, several studies conducted by the IIRN suggested that coordinated MDT care is associated with improved clinical outcomes, including reduced readmissions 45 and improved short-term outcomes in newly diagnosed CD. 46 Joint clinics, including IBD-Derma, 47 pregnancy, 48 and transition programs, 49 provided structured frameworks for addressing the patient’s journey across various stages of their disease. Diet-related research and implementation within the IIRN have been distributed across centers, a step that established nutrition as a scalable MDT-anchored therapeutic domain. Additional MDT interventions, such as psychological therapies and physical exercise, have demonstrated a shift in the microbial taxa among patients with CD. 43
MDT integration also enabled prospective evaluation of modifiable factors, particularly diet and psychosocial interventions. Patients with early CD who adhered to the Mediterranean diet had a more favorable outcome, with lower inflammatory markers, less dysbiotic microbiome, and changes in fecal metabolites. 6 These findings align with growing international evidence supporting diet as a key modifiable component of IBD management, and in conjunction with microbiome-directed approaches. 50
Guiding diagnosis, prognostication, and remission using novel imaging
One of the key challenges in IBD is selecting appropriate tools for diagnosis, disease monitoring, and assessment of remission. Several IIRN studies addressed the role of different imaging modalities in these settings. Comparative work between video-capsule endoscopy (VCE) and magnetic resonance enterography9,51–53 suggested that VCE may provide higher sensitivity in detecting proximal small-bowel disease, with potential prognostic impact. A validated VCE score was suggested, and the prognostic value of a non-passed patency capsule was highlighted.34,36 These observations were subsequently integrated into an IIRN collaborative randomized trial, the CURE-CD trial, in which a VCE-guided treat-to-target was superior to continued standard care in the prevention of clinical relapse over 24 months. 11 These studies prompted the addition of CD monitoring as an indication for VCE reimbursement by all HMOs.
IIRN studies supported the feasibility of gastroenterologist-performed IUS 54 and further explored practical strategies for disease monitoring and prognostication. 55 Subsequent collaborative efforts contributed to international recommendations regarding IUS response criteria and operator competency.56,57
Overall, these advances turned various tests into shared SOPs and actionable targets in the IIRN centers, implemented in real-world care and national-level decisions.
Biologic therapy: Mechanisms, immunogenicity, and biomarkers
TDM and immunogenicity were other major domains within the IIRN.12,58–60 Specifically, we assessed the formation of anti-drug antibodies (ADA) to anti-TNF agents, mechanistic clues based on mucosal and peripheral blood drug levels and ADA, ways for their modification,13,37–40 and drug levels and ADA relation to disease outcomes and prediction of early response to treatment.39,61,62 Harnessing the epidemiological power of the epi-IIRN, we translated laboratory findings regarding the influence of antibiotics on ADA formation into a clinical trial, demonstrating how different antibiotics might be related to ADA formation.14,63 These studies shed light on our understanding of biologic therapies’ mechanisms and supported the integration of TDM and drug dosing as a part of common clinical practice.
Holistic approach and the psychosocial burden of IBD
As part of the IIRN comprehensive assessment and MDT-guided intervention in IBD, particularly CD, the role of psychosocial factors in disease activity and quality of life was explored. The contribution of stress, life experiences, and social support to disease burden was highlighted showing that adverse life events and family dynamics were associated with higher psychological distress and poorer quality of life,64,65 whereas perceived social support was associated with lower psychological distress and lower disease activity. 66 These findings align with broader, international evidence that has demonstrated a substantial psychiatric burden among patients with IBD, further supporting the integration of psychological assessment into routine IBD care. 67
To this end, we examined disease-specific coping mechanisms, somatization, and their relationship to disease severity to further support integration of psychological assessment and intervention into routine management.68,69 More recent international perspectives expanded this by highlighting the importance of IBD-related trauma, suggesting that disease course and complications may themselves become important contributors to long-term psychological burden. 70 Reflection of these processes was demonstrated in several epi-IIRN-based studies reporting substantial burden of depression and anxiety disorders in pediatric-onset IBD and their modifying factors, 71 as well as fatigue in adults. 72 In a multicenter, randomized controlled trial, we evaluated a structured cognitive-behavioral and mindfulness-based intervention with daily exercise (COBMINDEX) in patients with active CD. 15 The intervention was associated with improvement in quality of life and patient-reported outcomes,16,42 as well as changes in selected microbiome features. 43
Taken together, proactive screening and structured management of psychological burden, as well as incorporation of mental health experts in the IBD MDT, are important implications of IIRN output.
Stepping into the future with artificial intelligence and deep learning
Over time, the IIRN was expanded to include emerging conceptual domains, including artificial intelligence and machine learning. Specifically, predictive models using longitudinal clinical and laboratory data for detecting patients with CD pre-diagnosis20,73 were applied in the epi-IIRN database, and prompt-learning and natural language processing were used to structure radiology reports.74–76 Deep learning models were also applied for the detection of small-bowel ulcers on VCE, demonstrating the potential to shorten reading time, with grading of ulcer severity and the detection of strictures.77–79 The integrated work pipeline of the IIRN that spans across these varied topics is illustrated in Figure 1.
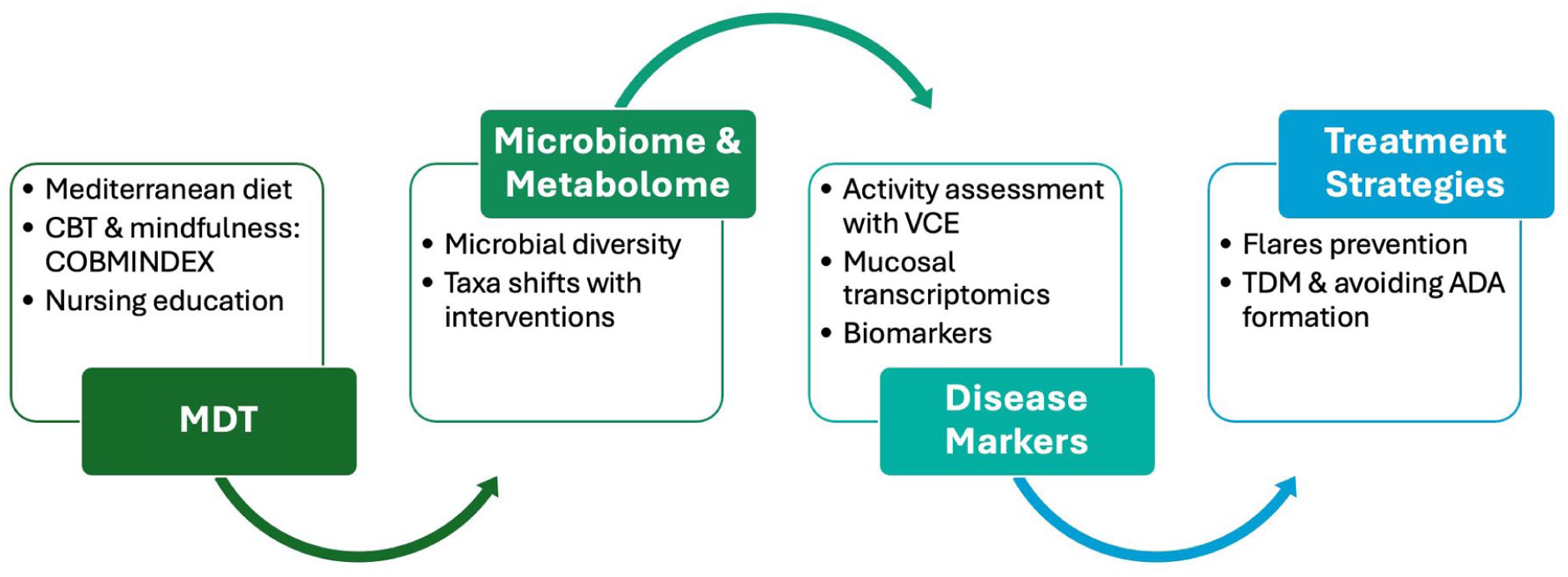
Pipeline work of the IIRN.
The footprint of collaboration: Measuring the IIRN impact
The IIRN spans five centers, but its contribution relies on the people who have contributed to its founding and ongoing works over the years. This network includes physicians across different disciplines, basic and translational scientists, nurses, dietitians, social workers and psychologists, bioinformaticians, and research coordinators. Annual scientific meetings were held 1–2 yearly, enabling discussion of projects, sharing ideas, preliminary findings, and feedback. Scientific output was reflected in multiple publications, with 90 documents as core IIRN outputs between 2015 and 2025 and 2169 citations (Figure 2). IIRN-related collaborative or infrastructure-based studies included 165 publications with 4281 citations.
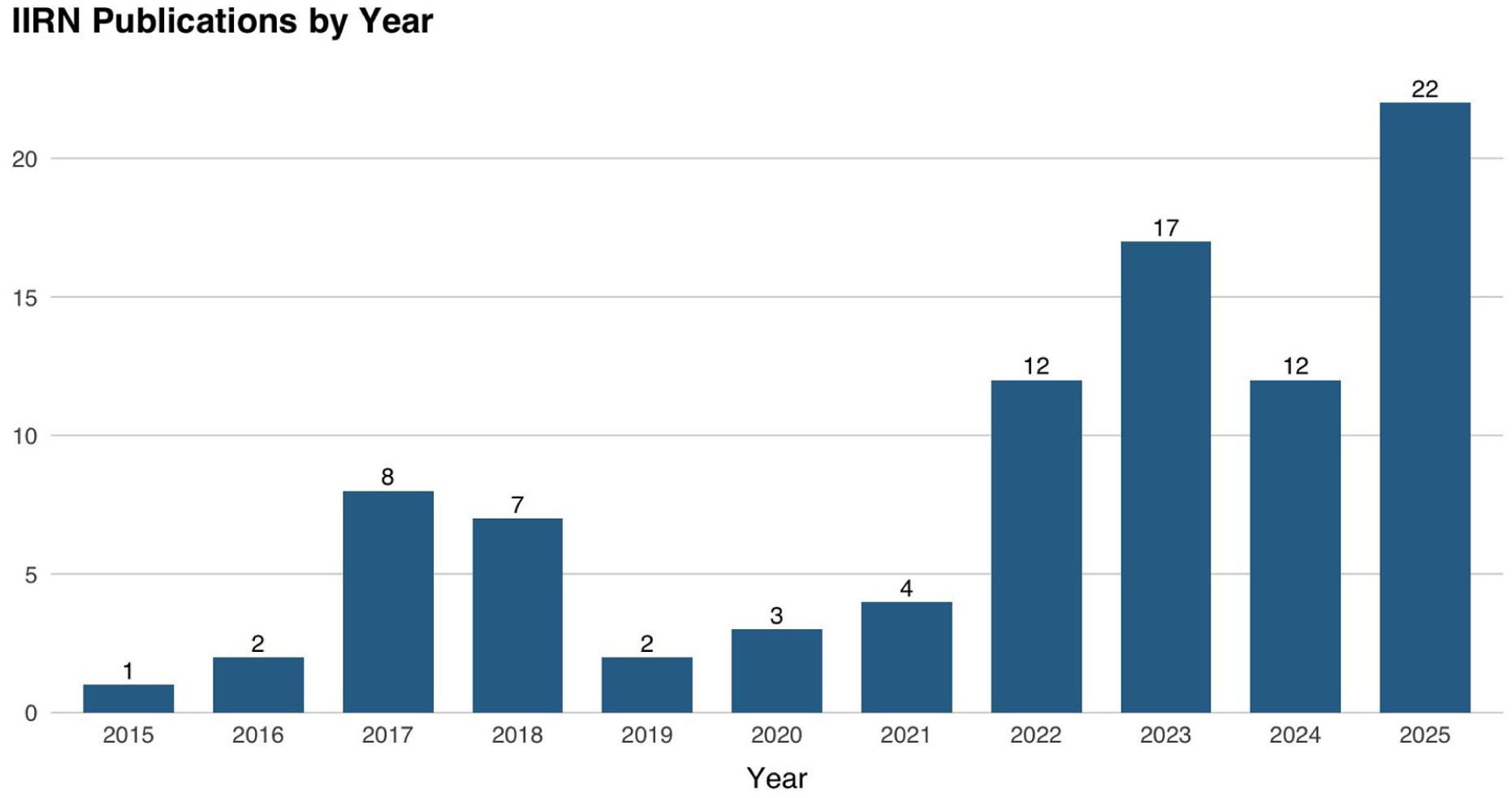
Annual number of peer-reviewed publications arising from IIRN work.
Overcoming limitations, challenges, and lessons learned
Coordinating a national consortium of leading centers over a decade posed several challenges. Early on, moving beyond ad hoc collaboration toward true co-design required building trust, shared priorities, and aligned research and care pathways. Data sharing represented a major constraint, given institutional interests, data-protection policies, and alongside regulatory barriers for establishing multicenter and national cohorts such as the epi-IIRN. The IIRN approach to such challenges was to preserve each center’s unique cohorts and platforms, enabling scientific insights, while fostering interaction cross-referral, validation, and mutual contribution. This comes at a cost of limited harmonization in outcome measures and exploratory assessments across heterogeneous cohorts.
These challenges were addressed through transparent governance, a steering committee with decision-making authority, and targeted, data-sharing pipelines activated when indicated scientifically. Sustained coordination efforts ultimately strengthened the scalability and translational impact of IIRN outputs. Facing and overcoming these challenges enabled our joint effort to produce tangible achievements and to look forward, not without its own lessons. We believe that these challenges may be encountered in similar efforts to bridge over different centers while attempting to conduct comprehensive research, which will focus on a complex disease such as IBD. We therefore summarize our main approaches and lessons for each domain in Table 2.
Main lessons from the IIRN experience in developing a national IBD research network.
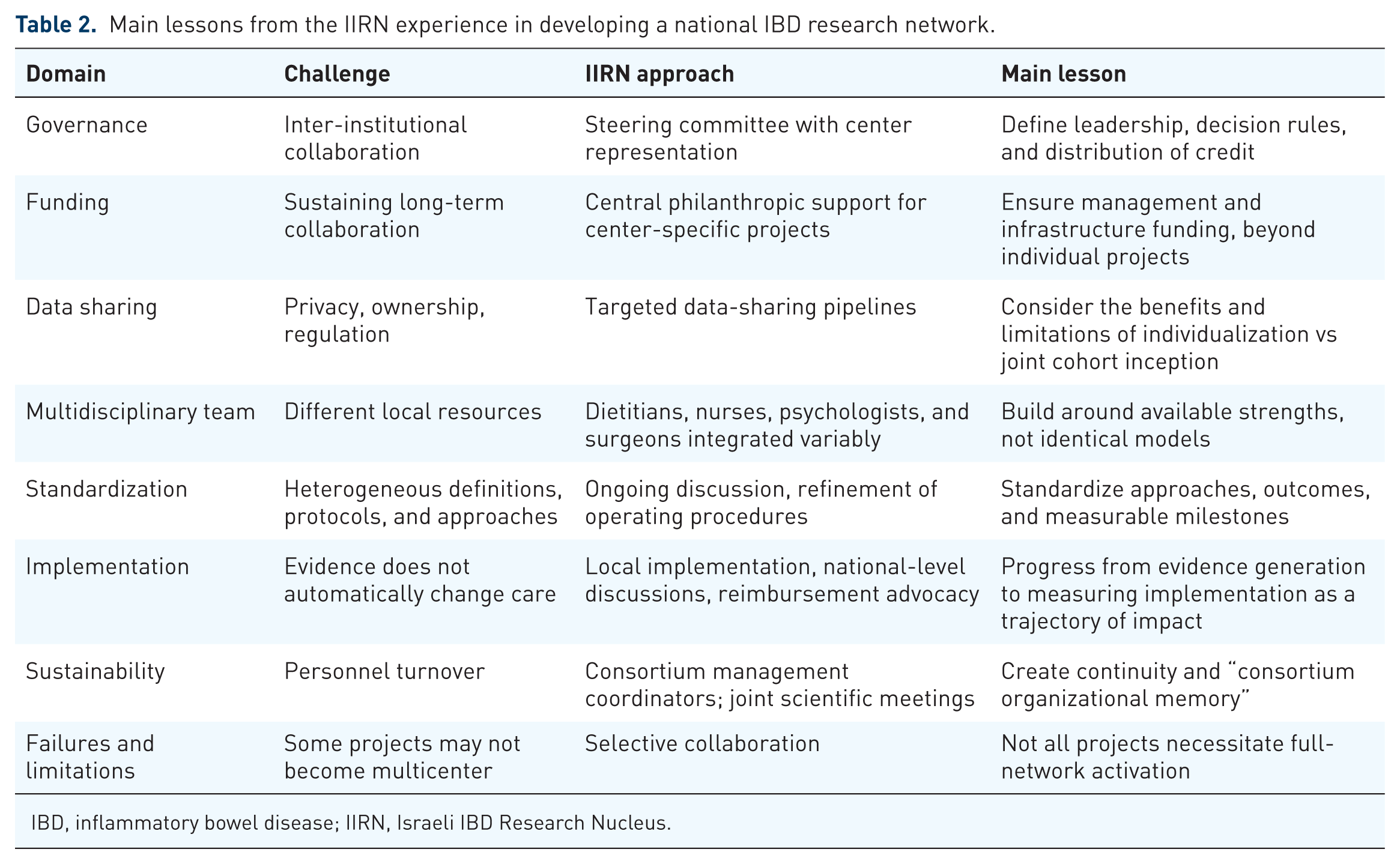
IBD, inflammatory bowel disease; IIRN, Israeli IBD Research Nucleus.
Discussion
This review summarized the experience of the IIRN, a national-level IBD collaborative effort, during over a decade. The IIRN has some distinct features when compared to other national-level organizations: it was established as a collaborative consortium of IBD centers, with the aim of forming a whole that will be greater than the sum of its parts; selection of centers was based on those who had recognized clinical and research expertise in the field. Furthermore, we aimed to include centers that would have complementary, rather than overlapping, expertise and skills.
Several other national-level IBD research networks have made remarkable contributions to the field, each with unique advantages. The Swiss IBD Cohort Study is a prospective cohort with a rich national biobank. The UK IBD BioResource has recruited nearly 50,000 genotyped, recallable patients across over 90 hospitals in an open-access platform. In Canada, the CCC-GEM Project made landmark contributions by tracking healthy first-degree relatives of CD patients to identify pre-diagnostic microbial and environmental risk factors. In the United States, IBD Qorus benchmarks quality of care across gastroenterology practices nationally. In Sweden, the SWIBREG registry links patient-level data to national health records, resulting in multiple nationwide studies. The Danish national registries have enabled landmark population-based studies, and the multinational NORDTREAT inception cohort prospectively examines novel biomarkers across Sweden, Denmark, and Norway. In Germany, the Kompetenznetz Darmerkrankungen unites more than 700 members across academic centers through the German IBD Study Group. The Belgian BIRD group has delivered landmark contributions to IBD genetics and translational biomarker science. The GETAID has pioneered investigator-initiated clinical trials and prospective cohorts across French academic IBD centers, and has demonstrated the power of focused sub-networks through the REMIND group, whose prospective multicenter studies have made seminal contributions to the management of postoperative CD.
Each of these initiatives has substantially advanced IBD science, and their contributions are internationally recognized. The IIRN was conceived to address a complementary set of needs: rather than building depth in a single domain, it sought to create an integrative end-to-end ecosystem by pairing centers with complementary expertise so that population-level signals could be interrogated mechanistically in prospective cohorts, and MDT program observations validated at the national level. Israel’s universal HMO-based healthcare system offered a unique infrastructure to make this vertical integration across the full disease trajectory possible.
Over a decade after its establishment, the consortium transformed ad hoc co-authorship to an infrastructure of intricate collaborations, taking advantage of local expertise and magnifying its effect by providing insights, cross-referrals, specific inter-center analyses, and feedback for further studies. The clinical and scientific notions reported were implemented in daily practices and disseminated through manuscripts, presentations, and new collaborations.
The scientific output comprehensively spanned the journey of a patient with IBD, specifically CD, addressing various layers contributing to pathogenesis and manifestations. Epidemiological, population-level risk factors and predictors; imaging and biomarker studies translating “depth of remission” into practical targets; diet as a modifiable therapy and the microbiome as its mechanistic readout; immunogenicity and TDM applied to biologic treatment and its modifiers and mechanisms; and implementing a diverse MDT with specific programs delivered for patients all across centers. The unique cohorts recruited and followed span different stages in the journey of a patient with CD, providing clinical evidence and exploratory biomarkers and notions. Beyond the clinical and scientific insights, several IIRN initiatives informed clinical practice patterns and organizational structures, thereby contributing to a broader national impact. Specifically, adopting the MDT approach across centers was implemented gradually in all centers, associated with earlier specialty triage, holistic care, and improved strategies. IBD nurses, dietitians, and psychosocial care are now integral to most Israeli IBD centers. Importantly, national-level policy changes and initiatives followed, such as formalizing MDT member positions and including evaluation, such as VCE and TDM measures in reimbursed procedures. While the direct impact of these activities is difficult to quantify, they highlight the potential role of coordinated national network in shaping healthcare delivery beyond individual institutions.
All these fields represent major contributions the IIRN team members led throughout the years, for which they have been internationally recognized. The consortium collaboration manifested a workflow from idea, through protocols and measurements, to implementation of new findings, with hundreds of peer-reviewed outputs. The body of work generated within the IIRN spans a wide range of evidence types, from population-based epidemiologic studies and randomized trials, through translational and biomarker studies of hypothesis-generating nature, to early proof-of-concept works requiring prospective validation.
As with all collaborations, there are limits—which we have faced collectively. Promoting data sharing while protecting each center’s own interests, aligning different perspectives and opinions, and creating a true and honest alliance may not come easily. Yet we responded to these challenges with open discussion, resource pooling and allocation, pre-specified rules and systems, and targeted sharing for high-value, high-impact studies. CD was somewhat overrepresented compared to UC in most centers, which can be in part due to every center’s uncoordinated individual focus in the field of IBD and the high prevalence of CD in the pediatric population. As this review was written by active members of the consortium, it is inherently subject to self-assessment bias; efforts were made to mitigate this by applying predefined inclusion criteria and categorizing studies by flagship domains; however, independent external validation of impact remains limited.
Looking into the next decade, we have yet to answer questions to continue exploring. While we recruited national cohorts, standardized endpoints, trained MDT members, and enabled immense biologic and statistical infrastructure, the next step is to ensure the chain proceeds while expanding its impact. We hope to continue and explore diagnosis, surveillance, prognostication, and management methods; conduct real-world trials on specific interventions; advocate for equity and reach in the care of patients with IBD across the nation; and incorporate innovative, novel technologies in our health systems and research methods.
The success of the IIRN stems not only from isolated outputs and meaningful publications but also from reciprocal and shared approaches. Our record over the last decade shows that coordinated, multidisciplinary effort delivers insights and improvements that no single group could achieve on its own. Taken together, the IIRN experience should be interpreted as a descriptive account of a national collaborative model, highlighting contributions and lessons learned. Sustaining and expanding our reach, we continue to work as a collaborative team to deliver better care for people living with IBD.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261463603 – Supplemental material for The Israeli IBD Research Nucleus: collaborative advancements in Israeli IBD research
Supplemental material, sj-docx-1-tag-10.1177_17562848261463603 for The Israeli IBD Research Nucleus: collaborative advancements in Israeli IBD research by Iris Dotan, Shomron Ben-Horin, Doron Schwartz, Haggai Bar-Yoseph, Maya Fischman, Shai S. Shen-Orr, Yehuda Chowers, Shmuel Odes, Rami Eliakim and Dan Turner in Therapeutic Advances in Gastroenterology
Footnotes
Acknowledgements
We would like to thank Prof. Maria Abreu, Prof. Matthieu Allez, Prof. Jonathan Braun, and Prof. Stefan Schreiber for scientific input, insights, and feedback as scientific advisors for the IIRN throughout the years.
Author note
On behalf of the IIRN Researchers: RMC—Irit Avni Biron, Hagar Banai, Jacob Ollech, Tali Fischler Sharar, Lihi Godny, Revital Barkan, Shelly Shakhman, Sarine Elial Fatal, Tamar Pfeffer Gik, Keren Rabinowitz, Sarit Cohen Kedar, Kawsar Kaboub, Hanan Abu-Taha, Uri Gophna, Leah Reshef, Maor Pauker, Adi Friedberg, and Tanir Ben-Yishai. Sheba—Bella Ungar, Yael Haberman, Adi Lahat, Dan Carter, Michal Amitai, Ophir Ukashi, Limor Selinger, Adi Talan-Asher, Orit Picard, Ella Fudim, Miri Yavzori, Sandra Neuman, Gilat Efroni, Tzipi Braun, Nina Levhar, Amnon Amir, Tal Engel, Mai Tzur, Ahmad Albshesh, Asaf Levertovsky, Eyal Klang, and Doron Yablecovitch. Soroka—Ganit Goren, Orly Sarid, Vered Slonim-Nevo, Alon Monsonego, Anna Nemirovsky, Karny Ilan, Michal Grinberg, Dan Greenberg, Ruslan Sergienko, Dan Vilenchik, Michael Friger, Shirley Regev, Hillel Vardi, Oz Seadia, Maya Cordova, Shaked Sharvit-Daham, Naama Amir, Ariel Weiner, Oshrit Tamano, Elena Chernin, Karny Ilan, Livnat Lerner, Avihu Pereg, and Terri Singer. RHCC—Sigal Pressman, Shiran Gerassy, Alexandra Blatt, Yuri Gorelik, Roni Weisshof, Matti Waterman, Neta Milman, Timothy Cooper, and Elina Starosvetsky. SZMC—Ohad Atia, Chagit Friss, Adi Mendelovich, Adi Toker, Gili Kurtzer-Gilad, Rona Lujan, Menachem Skolnik, Elad Sinai, and Itamar Koren.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.