
Abstract
Background:
Helicobacter pylori (H. pylori) infection and its related diseases constitute a significant global public health issue, and the growing antibiotic resistance of H. pylori poses a serious challenge.
Objectives:
Consequently, the search for sensitive, safe, economical, and readily available therapeutic drugs has become a core challenge in contemporary research.
Design:
This systematic review and meta-analysis of randomized controlled trials and observational studies followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (2020).
Data sources and methods:
This study conducted a thorough and systematic literature review of PubMed, Web of Science, EMBASE, China National Knowledge Infrastructure, Chinese Scientific Journal Database, and Wanfang Data up to October 16, 2025, using keywords such as minocycline and H. pylori. The included studies were assessed for risk of bias, and meta-analyses were conducted using Review Manager 5.3 and Stata/MP 14.0 to estimate the pooled effect sizes. Risk ratios (RR) were used for statistical analysis, and the corresponding 95% confidence intervals (CI) were calculated.
Results:
Minocycline exhibits pharmacokinetic characteristics including high absorption, strong lipophilicity, tissue permeability, and a prolonged half-life. Beyond its antibacterial effects, it also possesses non-antimicrobial activities such as anti-inflammatory, immunomodulatory, antioxidant, and anti-apoptotic properties. Eighteen studies from six countries indicate that H. pylori is sensitive to minocycline. This study included 33 clinical trials that evaluated minocycline-containing eradication regimens for H. pylori infection. Based on pairwise meta-analysis, both the intention-to-treat (ITT; RR = 1.04, 95% CI: 0.99–1.08, p = 0.15) and per-protocol (PP; RR = 1.04, 95% CI: 1.00–1.08, p = 0.06) analyses showed no significant difference in H. pylori eradication rates between the minocycline-containing eradication regimen and the control group; however, the overall incidence of adverse reactions was significantly lower (RR = 0.85, 95% CI: 0.78–0.92, p < 0.05), while compliance rate was comparable to that of the control group (RR = 1.01, 95% CI: 1.00–1.03, p = 0.15). Based on meta-analysis of proportions, the ITT analysis indicated the H. pylori eradication rate was 83% (95% CI: 79%–87%), while the PP analysis showed an eradication rate of 88% (95% CI: 83%–92%), an adverse reaction incidence of 29% (95% CI: 23%–36%), and compliance rates of 94% (95% CI: 91%–96%). The analysis revealed that minocycline-containing regimens exhibited favorable efficacy, safety, and patient compliance.
Conclusion:
Minocycline may be considered a viable antibiotic option for the eradication of H. pylori. Further multicenter, large-scale, high-quality clinical studies are still required to validate this conclusion.
Trial registration:
The review was not registered in PROSPERO, we will do so in future studies.
Introduction
Helicobacter pylori (H. pylori) can colonize human gastric mucosal tissue, and infection rates remained as high as 43.1% between 2011 and 2022 in China. 1 H. pylori infection is correlated with diseases such as peptic ulcers, functional dyspepsia, and chronic gastritis, and is a significant risk factor for gastric cancer. Eradicating H. pylori reduces gastric cancer risk, playing a crucial role in alleviating the burden of H. pylori-related diseases. 2 Furthermore, H. pylori infection is positively correlated with multiple extra-gastroduodenal diseases. 3 As an infectious disease, H. pylori can spread between individuals. Therefore, in the absence of contraindications, all infected individuals should undergo eradication therapy. 4
The Maastricht VI/Florence Consensus Report recommends routine drug susceptibility testing. However, treatment strategies guided by susceptibility testing remain underutilized in clinical practice. In the absence of individualized susceptibility testing, clinicians must base decisions on antibiotic resistance prevalence in the target population, current local cure rates, or specific treatment regimens. 3 A meta-analysis encompassing 351 studies revealed an upward trend in primary resistance rates for clarithromycin, metronidazole, and levofloxacin between 1990 and 2022. Recent resistance rate data from the Asia-Pacific region show clarithromycin at 30%, metronidazole at 61%, and levofloxacin at 35%. 5 The escalating antibiotic resistance rates have complicated H. pylori treatment. 6 Consequently, the quest for therapeutic agents that are sensitive, safe, affordable, and accessible has emerged as a significant challenge in contemporary research.
Minocycline is a broad-spectrum tetracycline antibiotic effective against a wide range of bacterial infections. Consequently, it is commonly employed in clinical settings to treat acne vulgaris and certain sexually transmitted diseases. 7 However, minocycline also demonstrates several biological activities that are independent of its antibacterial properties, including anti-inflammatory, immunomodulatory, antioxidant, and anti-apoptotic effects. 8
The rising prevalence of antibiotic resistance has brought minocycline into focus due to its low resistance rate. Minocycline-based regimens for H. pylori eradication has revealed their exceptional efficacy, safety, and compliance. 9 This study aims to conduct an extensive literature review and analysis, exploring pharmacokinetics, mechanisms of action, resistance status, and clinical efficacy of minocycline to offer insights into clinical practice and future investigations.
Pharmacokinetic characteristics
Absorption
Minocycline achieves nearly complete oral absorption (95%–100%), mainly in the gastric, duodenal, and jejunal segments of the digestive tract. Its peak plasma concentration occurs 2–3 h after oral administration, reaching 2–6 mg/L at conventional doses of 100–300 mg. 10 Food has little impact on its absorption, allowing administration independent of meals. However, co-administration with dairy products reduces absorption by 6%, while milk and iron supplements decrease absorption by 27% and 77%, respectively.11,12 Furthermore, the antibacterial activity of minocycline against H. pylori is minimally affected by pH. In 2025, Li et al. reported that although the minimum inhibitory concentration (MIC) of minocycline increased only slightly for most H. pylori isolates when pH dropped from 7.3 to 6.0, the overall impact of pH was not significant. Overall, the effect of pH on the MIC of minocycline resembles that of amoxicillin. 13 At the standard dose (100 mg twice daily), the steady-state peak plasma concentration of minocycline ranges from approximately 1.6 to 6 mg/L, meeting the therapeutic concentration requirements for H. pylori eradication. 11
Distribution
Minocycline, in comparison to other tetracycline antibiotics such as doxycycline, demonstrates increased lipophilicity and enhanced tissue permeability. With an initial 200 mg dose followed by 100 mg twice daily for a 2- to 7-day course, minocycline achieves an average concentration of 0.97 μg/mL in gastric tissue, with a tissue/blood ratio of 2.26 in the stomach. The tissue/serum ratios in bile, liver, and gallbladder are 38, 12, and 6.5, respectively, indicating its efficient diffusion in the gastrointestinal tract. 14 Vallé et al. observed minocycline concentrations in intestinal contents to be 6–39 times higher than in plasma. With a human serum protein binding rate of 76%, minocycline’s superior lipophilicity and lower binding rate contribute to its favorable tissue penetration. 15
Metabolism and excretion
Minocycline undergoes biotransformation in the liver, resulting in the formation of three microbiologically inactive metabolites that are excreted in urine and feces. Unchanged minocycline accounts for 8%–12% of the administered dose in urine, corresponding to a renal clearance of 0.54 L/h. The parent compound is excreted in feces at 20%–35% of the administered dose, while the remainder is eliminated as metabolites via urine or feces. 11 The elimination half-life of minocycline ranges from 15 to 23 h, substantially longer than that of first-generation tetracycline antibiotics. 8 This prolonged half-life results in minimal fluctuations in steady-state plasma concentrations, facilitating the sustained maintenance of effective concentrations at the gastric mucosal target site. Consequently, this pharmacokinetic profile reduces the necessity for frequent dosing, thereby justifying the twice-daily dosing regimen in clinical practice and enhancing patient compliance.
Mechanisms of action
Antibacterial effect
Minocycline shares a similar antibacterial mechanism with other tetracycline antibiotics. 16 Minocycline primarily penetrates bacteria through outer membrane protein channels and exerts its antibacterial effect by targeting the aminoacyl-tRNA binding site on the bacterial 30S ribosomal subunit. It blocks the binding of aminoacyl-tRNA, inhibits peptide chain elongation, and ultimately inhibits bacterial protein synthesis. 9
Non-antibacterial effects
Multiple studies have indicated that minocycline exhibits anti-inflammatory, immunomodulatory, antioxidant, and anti-apoptotic properties. Its potential mechanisms include: (i) Inhibition of key enzyme activity. Elevated levels of inducible nitric oxide synthase (iNOS) were observed in biopsy specimens from patients with CagA H. pylori-infected gastritis. 17 Amin et al. 18 demonstrated that minocycline suppresses NOS mRNA expression, resulting in reduced protein expression and diminished NOS activity. H. pylori lipopolysaccharide modulates gastric mucin synthesis through an extracellular signal-regulated kinase-dependent cytosolic phospholipase A2 (PLA2) activation pathway. 19 Minocycline can inhibit PLA2 by interacting with its substrates, potentially serving as an effective adjunctive therapy for inflammatory diseases associated with PLA2-mediated pathogenic mechanisms. 20 (ii) Inhibition of caspase-3 activation. H. pylori infection activates IL-18, ICE, and caspase-3, thereby stimulating Th1 responses and exacerbating mucosal damage. 21 Minocycline inhibits caspase-3 mRNA upregulation and reduces iNOS activity. 22 (iii) Upregulation of Bcl-2 expression. H. pylori infection reduces GES-1 cell viability, increases cell mortality, inhibits cell migration, elevates apoptosis rates, increases Bax expression, and downregulates Bcl-2 expression. 23 Minocycline demonstrates anti-apoptotic effects by reducing Bax expression levels and upregulating Bcl-2 expression levels. 24 (iv) Reduction of p38 MAPK phosphorylation. In H. pylori-infected GES-1 cells, the p38 MAPK pathway is activated, 25 and minocycline can inhibit p38 MAPK activation. 26
Resistance to minocycline
Eighteen studies from six countries indicate that H. pylori strains exhibit sensitivity to minocycline (Table 1). Specifically, seven studies were conducted in Japan, seven in China, and one each in Belgium, Greece, Cameroon, and Mongolia.
Resistance status of Helicobacter pylori to minocycline.

MIC50, minimum inhibitory concentration 50; MIC90, minimum inhibitory concentration 90; NA, not available.
Japan
In 1994, Igari et al. investigated the inhibitory activity of minocycline toward 50 clinically isolated strains. The study revealed potent activity of minocycline against 50 strains of H. pylori, with MIC50 and MIC90 values of 0.063 and 0.25 μg/mL, respectively. 28 In 1997, Irie et al. conducted a comparative study on the susceptibility of 24 H. pylori strains to multiple antibiotics. The findings showed that minocycline displayed antibacterial activity inferior only to clarithromycin and amoxicillin, with an MIC range of 0.125–2 μg/mL. 29 Similarly, Okabe et al. 30 obtained comparable results through the agar dilution method, with MIC values ranging from 0.2 to 1.56 μg/mL in 10 H. pylori strains. Ikezawa et al. 32 isolated H. pylori strains from untreated patients and determined the MIC of each antimicrobial agent, revealing no instances of minocycline resistance. In 2005, Fujimura et al. 33 assessed MIC values for antibiotics against H. pylori in Japanese pediatric patients, demonstrating that all 51 strains were susceptible to minocycline, with MIC50 and MIC90 values of 0.016 and 0.094 μg/mL, respectively. In 2006, Murakami et al. studied the antibacterial activity of minocycline against H. pylori. MIC50 and MIC90 values were 0.20 and 0.39 μg/mL, comparable to other antimicrobial agents. 34 In 2009, Horiki et al. recruited 3521 treatment-naïve H. pylori patients confirmed by microaerophilic culture. Using the Kirby-Bauer disk diffusion method for antibiotic susceptibility testing, they found an overall primary resistance rate of 0.06% (2/3521) to minocycline. 35 Since 1994, numerous studies using the agar dilution method in Japan have consistently confirmed that local strains of H. pylori are highly susceptible to minocycline; indeed, resistance levels in the region have remained low since then.
China
In 2015, Chinese researchers Bai et al. employed the E-test to determine the susceptibility of H. pylori to antimicrobial drugs. The study demonstrated that minocycline could effectively eradicate H. pylori in vitro, with the resistance rate being only 6.6% (12/181). 36 In 2016, Song et al. isolated H. pylori from patients undergoing first-line and rescue therapy and detected antibiotic resistance. The resistance rate to minocycline was 6.9% in first-line and 8.7% in second-line treatment patients. 37 Furthermore, two clinical studies conducted at the same center in treatment-naïve patients with H. pylori infection demonstrated resistance rates of 8.2% (11/134) and 6.7% (9/134) for minocycline, respectively.40,41 In 2023 and 2024, two clinical studies conducted by Huang et al.42,43 in refractory H. pylori-infected patients showed resistance rates of 0.7% (2/288) and 0.6% (1/158) for minocycline, respectively. In 2024, a clinical study using the E-test method to assess H. pylori susceptibility to minocycline reported no resistance to minocycline among 101 clinical H. pylori isolates. Compared to tetracycline, minocycline demonstrated stronger antibacterial activity against H. pylori. 44 Since 2015, China has used the E-test as its primary screening method, with H. pylori resistance rates ranging from 0% to 8.7%, which is higher than in most other regions.
Other countries
In 1988, Glupczynski et al. from Belgium determined the MIC of minocycline in 49 H. pylori strains. The MIC50 value was 0.25 μg/mL, and the MIC90 value was 0.50 μg/mL. 27 In 1999, Mentis et al. 31 conducted a study to evaluate the activity of antibiotics against H. pylori strains isolated from Greek children, finding that all 36 strains were susceptible to minocycline, with MIC ranges between 0.03 and 0.50 μg/mL. In 2019, Kouitcheu Mabeku et al. from Cameroon isolated 140 H. pylori strains from gastric biopsies of dyspeptic patients and analyzed their antimicrobial susceptibility. The research revealed a resistance rate of 0.71% (1/140) to minocycline. 38 In 2020, Azzaya et al. from Mongolia isolated 361 H. pylori strains, determined the MICs of 5 antibiotics through agar dilution, and identified genetic determinants of antibiotic resistance. They identified 1 minocycline-resistant strain among 361 (0.28%) with an MIC of 2 μg/mL, carrying the A928C codon mutation. 39 Studies from Belgium, Greece, Cameroon, and Mongolia have all shown that the rate of minocycline resistance is less than 1%, indicating that strains across these regions remain susceptible to this drug.
Clinical application of eradication regimens containing minocycline
Literature search
This study was undertaken according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (Supplemental Table 1). 45 The review was not registered in PROSPERO, although this would have been desirable. A thorough and systematic literature search was conducted in PubMed, Web of Science, EMBASE, China National Knowledge Infrastructure, Chinese Scientific Journal Database (VIP), and Wanfang Data up to October 16, 2025, using keywords such as minocycline and H. pylori. The detailed search terms are provided in Supplemental Table 2.
Inclusion and exclusion criteria
Inclusion criteria: (i) Population: study participants were adults aged 16 years and older who met the criteria for H. pylori infection; (ii) Intervention and control: Minocycline is added to the H. pylori eradication regimen in the experimental group. No restrictions were applied to the control group; (iii) Availability of detailed information on the eradication regimen, including drug names, dosages, administration frequency, and treatment cycles was required; and (iv) outcomes: reporting results for the intention-to-treat (ITT) and per-protocol (PP) analyses.
Exclusion criteria: (i) reviews, guidelines, expert consensus statements, meta-analyses, conference abstracts, commentaries, case reports, and cell line or animal-only studies; (ii) duplicate studies; (iii) the sample size for each group was less than 20; and (iv) the language of the study was neither English nor Chinese.
Literature filtering and data extraction
Two investigators independently filtered the literature, read the literature to extract the data, and cross-checked the reviewed data. In case of disagreement, two investigators reached agreement through discussion or consultation with a third reviewer. During the literature filtering process, the title and abstract were reviewed first to eliminate unrelated literature; then read the literature and screen again; if there was still uncertain information, contact the authors by email to obtain the original data. The contents of data extraction: (1) The information of the study: author, title, publication time; (2) Baseline characteristics, intervention measures, course of treatment, outcome indicators in the study; (3) Quality evaluation information of included literature.
Risk-of-bias assessments
Two researchers independently assessed the quality of the included studies, cross-checked their findings, and resolved any disagreements by consulting a third reviewer. We used the Cochrane Risk of Bias Tool (ROB2) 46 to assess the risk of bias in randomized controlled trials (RCTs), the Risk of Bias in Non-randomized Interventions tool to assess the risk of bias in non-randomized clinical trials, and the critical appraisal checklists for case series in Appendix 7.3 of the JBI Evidence Synthesis Manual to assess the risk of bias in single-arm studies. The results of risk-of-bias assessments for RCTs and cohort studies were visualized using the Risk-of-bias VISualisation (robvis) tool. 47
Statistical analysis
Meta-analyses of the included studies were performed using Review Manager (version 5.3, The Cochrane Collaboration, Copenhagen, Denmark) and Stata/MP (version 14.0, StataCorp LLC, College Station, TX, USA) to estimate the pooled effect sizes. The outcome measures in this study—H. pylori eradication rates, incidence of adverse reactions, and compliance—were all binary variables; therefore, risk ratios (RR) were used for statistical analysis, and the corresponding 95% confidence intervals (CI) were calculated. Cochrane’s Q and I2 statistics were used to assess statistical heterogeneity between studies; a p-value <0.05 or I2 >50% indicated significant heterogeneity. A fixed-effects model was employed when heterogeneity was not significant, while a random-effects model was used when significant heterogeneity was present. Exploratory subgroup analyses were conducted to further investigate the potential influence of study quality, duration of intervention, and prior eradication status of study participants on heterogeneity. Sensitivity analyses were performed to assess the robustness of the meta-analysis results. Potential publication bias was assessed using funnel plots, Begg’s test, and Egger’s test. The evidence level for the outcome measures was assessed using the grading system of evidence evaluation (GRADE). 48
Results
Literature screening and characteristics
This review included 33 studies (Figure 1), comprising 18 RCTs,13,34,40 –42,49 –61 12 cohort studies,37,43,44,62 –70 and 3 single-arm studies71 –73; full details are provided in Supplemental Table 3. Studies were classified into two groups based on the control group exposure: (1) Comparative studies with a non-minocycline control (n = 17): Studies that included a control group not receiving minocycline. Data from both the minocycline and control groups were extracted, and a pairwise meta-analysis was performed (calculating RR and 95% CI). (2) Studies without a non-minocycline control (n = 16): These included single-arm studies, and multi-arm studies where all treatment arms contained minocycline. Data from the minocycline-containing regimens were extracted, and a meta-analysis of proportions was performed (calculating the pooled rate and 95% CI).
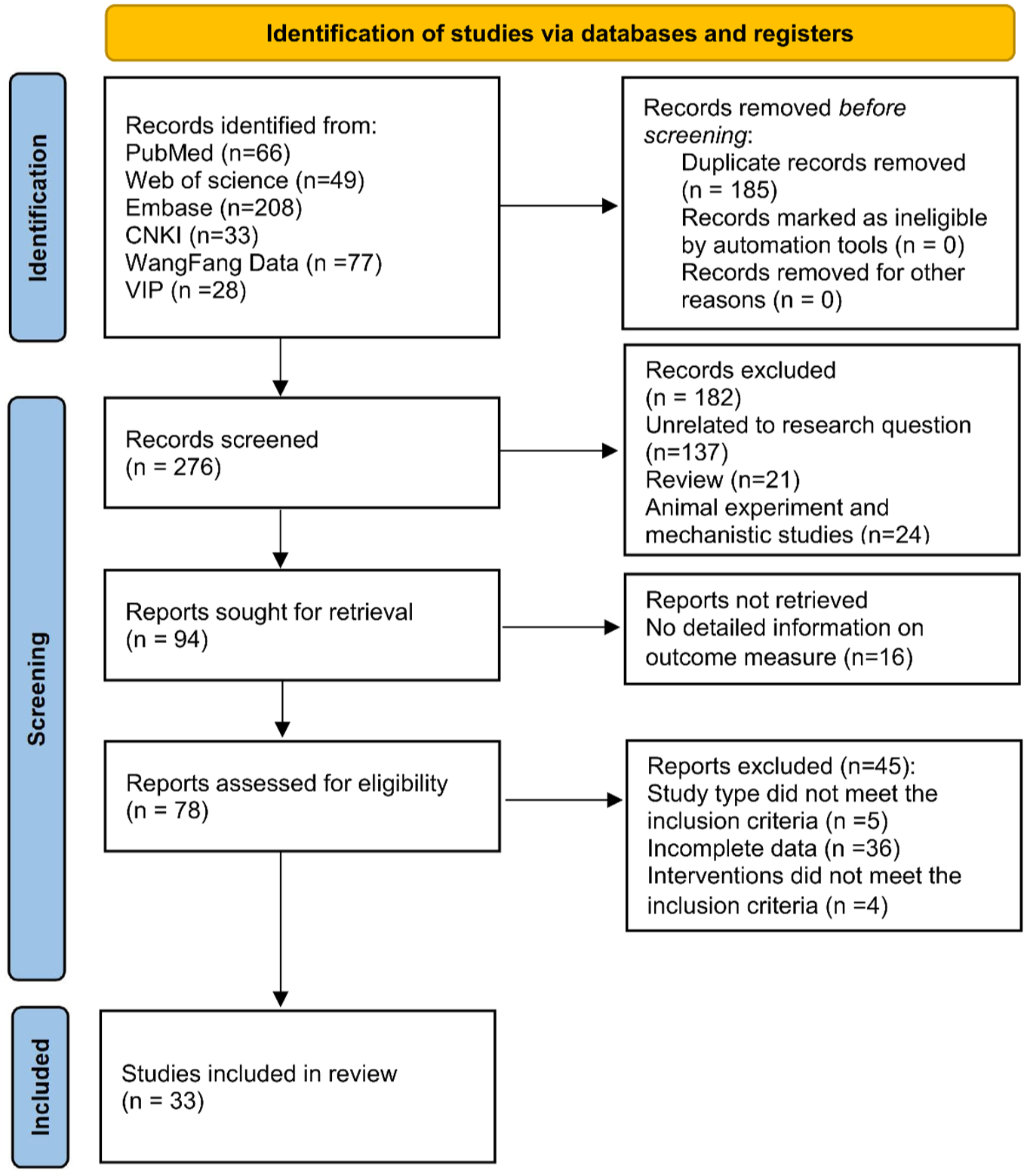
Overview of study selection process.
Risk-of-bias
Of the 18 RCTs included, 3 were identified as having a high risk of bias in the randomization process and were therefore classified as having a high risk of overall bias, while the remaining 15 studies were all assessed as having a low risk of bias (Figure 2(a) and (b)). Of the 12 cohort studies, 2 were classified as having a serious risk of bias, 5 as having a moderate risk, and the remaining 5 as having a low risk (Figure 2(c) and (d)). Of the three single-arm studies, two were assessed as “unclear” under the item “Are subjects enrolled consecutively in the case series?” (Supplemental Table 4). Overall, the quality of the included studies ranged from moderate to high; sources of bias primarily stemmed from the randomization process, confounding factors, and classification of interventions, while data completeness and reporting transparency were generally satisfactory.
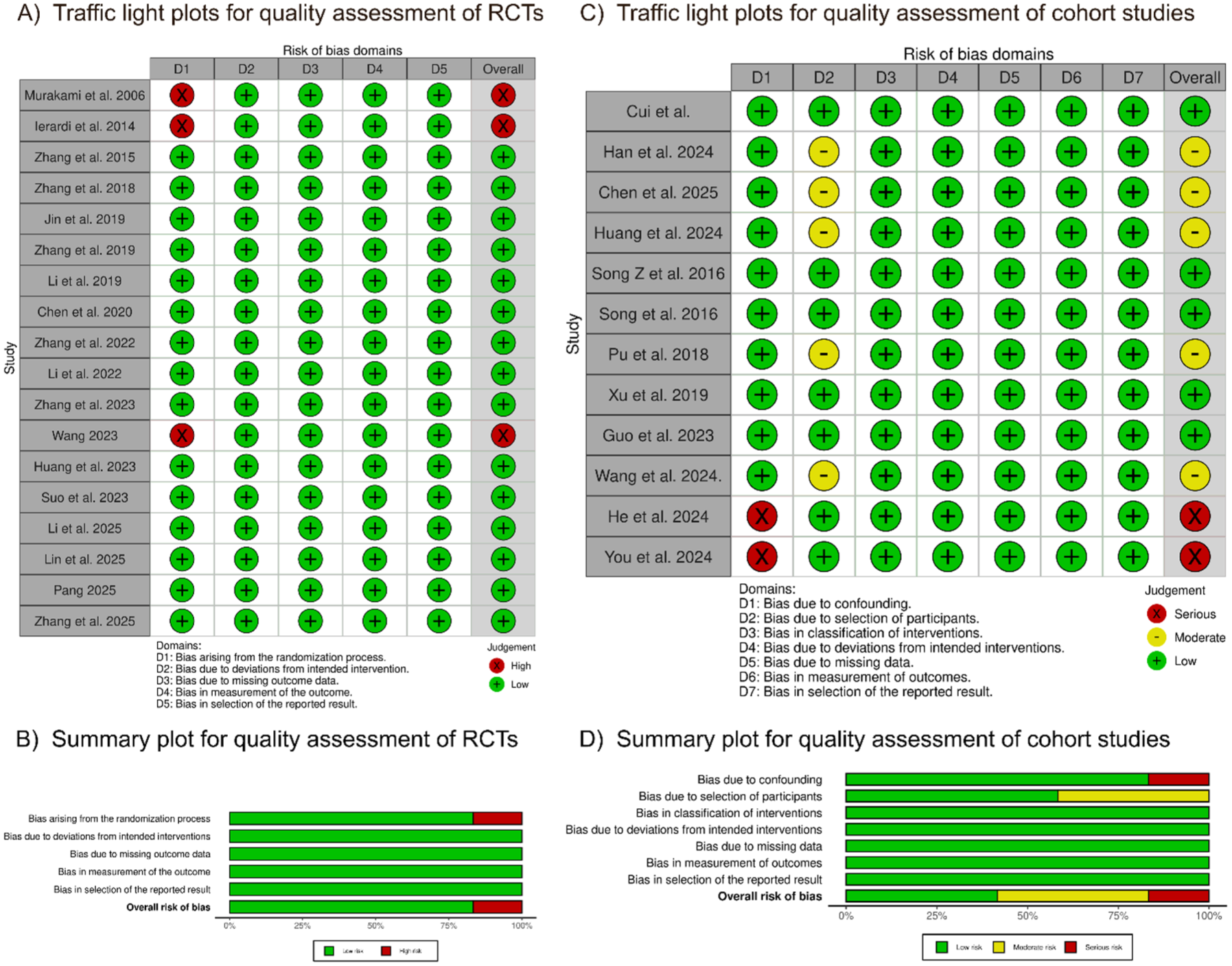
Risk-of-bias. (a) Traffic light plots for quality assessment of RCTs. (b) Summary plot for quality assessment of RCTs. (c) Traffic light plots for quality assessment of cohort studies. (d) Summary plot for quality assessment of cohort studies.
Outcomes
H. pylori eradication rate
A pairwise meta-analysis of 17 studies showed that, in terms of H. pylori eradication rates, both the ITT (RR = 1.04, 95% CI: 0.99–1.08, p = 0.15) and PP (RR = 1.04, 95% CI: 1.00–1.08, p = 0.06) analyses indicated that the minocycline-containing treatment regimen did not differ significantly from the control group, as shown in Figure 3(a) and (b). Both ITT (I2 = 71%, p < 0.05) and PP (I2 = 78%, p < 0.05) analyses indicated significant heterogeneity across the studies; sensitivity analyses failed to identify the source of this heterogeneity, as shown in Figure 4.
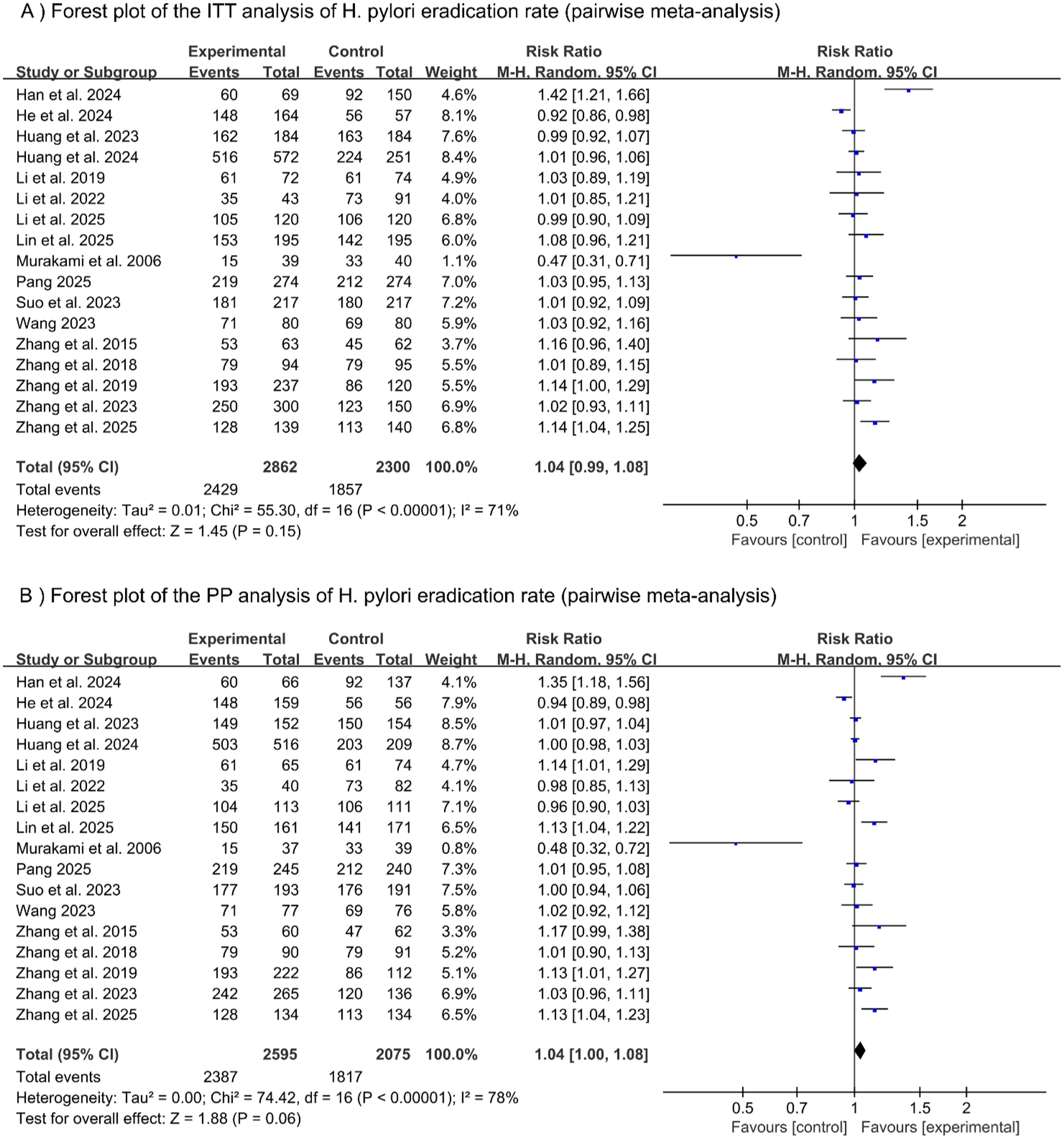
Forest plot of Helicobacter pylori eradication rate (pairwise meta-analysis). (a) Forest plot of the ITT analysis of H. pylori eradication rate (pairwise meta-analysis). (b) Forest plot of the PP analysis of H. pylori eradication rate (pairwise meta-analysis).
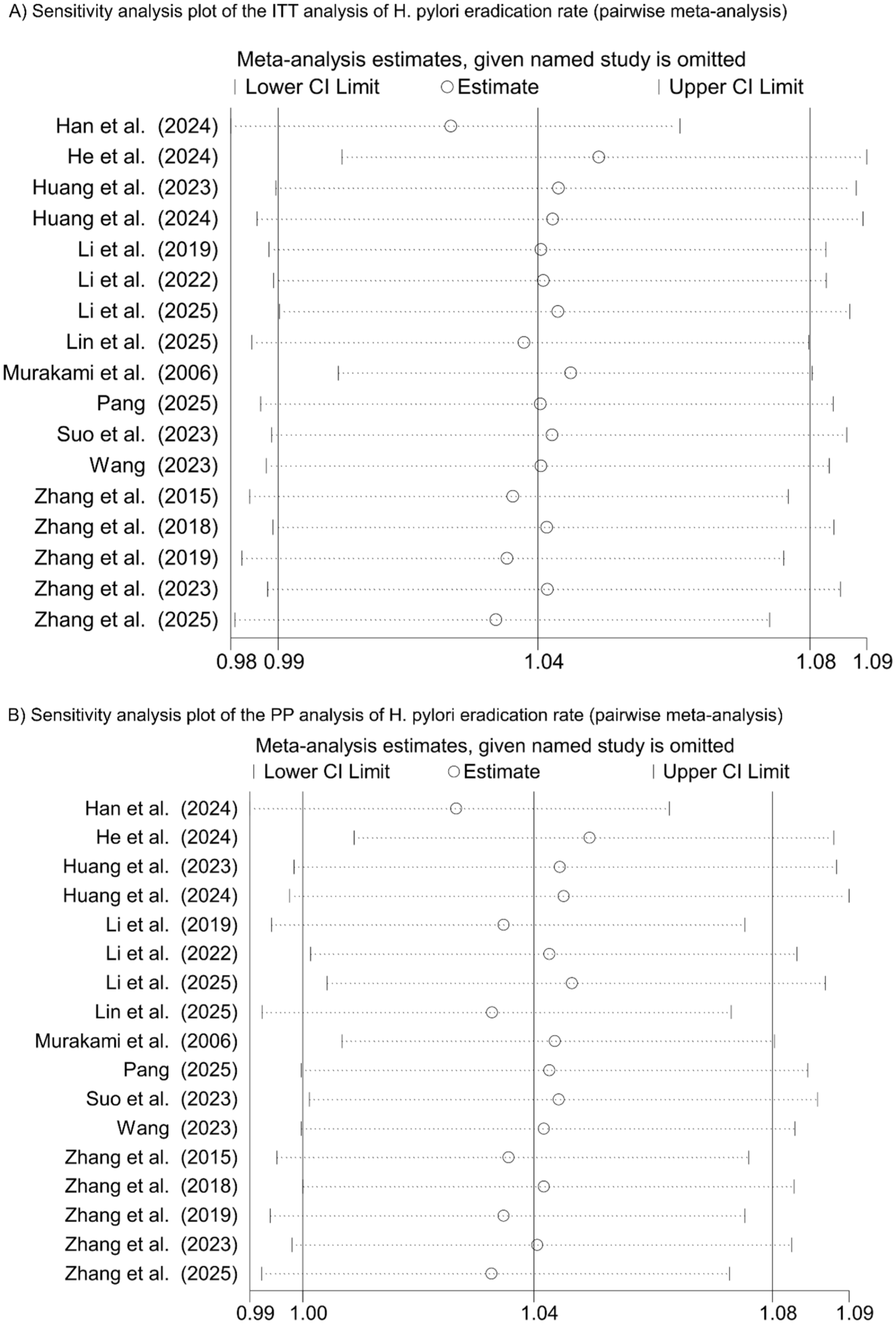
Sensitivity analysis plot of Helicobacter pylori (H. pylori) eradication rate (pairwise meta-analysis). (a) Sensitivity analysis plot of the ITT analysis of H. pylori eradication rate (pairwise meta-analysis). (b) Sensitivity analysis plot of the PP analysis of H. pylori eradication rate (pairwise meta-analysis).
The results of the subgroup analysis stratified by study quality are shown in Supplemental Figures 1 and 2. In the subgroup of studies classified as low risk, the ITT analysis showed no heterogeneity (I2 = 0%, and p = 0.45); whereas the PP analysis revealed substantial heterogeneity between studies (I2 = 62%, p < 0.05). The pooled results indicated that, compared with the control group, both the ITT (RR = 1.04, 95% CI: 1.01–1.07; p = 0.02) and PP (RR = 1.04, 95% CI: 1.01–1.08; p = 0.02) analyses suggested that minocycline-containing regimens showed a statistically significant difference in eradication rates, indicating that the minocycline-containing treatment regimen may play a role in improving eradication efficacy. The results of the subgroup analysis stratified by duration of intervention are shown in Supplemental Figures 3 and 4. Both the ITT (I2 = 85.7%, p < 0.05) analysis and the PP (I2 = 86.1%, p < 0.05) analysis indicated significant heterogeneity between the subgroups, suggesting that the duration of the intervention was one of the factors contributing to this heterogeneity. Results from the subgroups with intervention durations of 14 days (ITT: RR = 1.04, 95% CI: 0.99–1.09, p = 0.10; PP: RR = 1.04, 95% CI: 1.00–1.08, p = 0.07) and 10 days (ITT: RR = 1.06, 95% CI: 0.96–1.16, p = 0.26; PP: RR = 1.09, 95% CI: 0.98–1.21, p = 0.10) both showed no significant difference in eradication rates between the control group and the minocycline-containing treatment regimen; in the subgroup with a 7-day intervention duration, the eradication rate of the minocycline-containing treatment regimen was significantly lower than that of the control group (ITT: RR = 0.47, 95% CI: 0.31–0.71, p < 0.05; PP: RR = 0.48, 95% CI: 0.32–0.72, p < 0.05), but this was based on only one study and was contrary to the findings of other studies. These findings suggest that minocycline-containing eradication regimens should not be limited to 7 days, and durations of at least 10 days may be preferable. The results of the subgroup analysis stratified by the study participants’ prior eradication status are shown in Supplemental Figures 5 and 6. Both the ITT (I2 = 80.7%, p < 0.05) analysis and the PP (I2 = 81.5%, p < 0.05) analysis indicated significant heterogeneity between the subgroups, suggesting that prior eradication status was one of the factors contributing to this heterogeneity. In the subgroups comprising first-line (ITT: RR = 1.05, 95% CI: 0.99–1.12, p = 0.11; PP: RR = 1.04, 95% CI: 0.99–1.10, p = 0.11) and rescue treatment (ITT: RR = 1.01, 95% CI: 0.97–1.05, p = 0.51; PP: RR = 1.03, 95% CI: 0.98–1.09, p = 0.21), the analysis results consistently showed no significant difference in eradication rates between the control group and the minocycline-containing regimen; however, in the “Mixed first-line and rescue treatment” subgroup, the eradication rate of the minocycline-containing regimen was significantly lower than that of the control group (ITT: RR = 0.92, 95% CI: 0.86–0.98, p < 0.05; PP: RR = 0.94, 95% CI: 0.89–0.98, p < 0.05), but this conclusion is based on only one study and contradicts the findings of other studies. These results suggest that a history of previous treatment failure may be a key factor influencing the efficacy of minocycline and contributing to the heterogeneity observed across the included studies.
A meta-analysis of proportions from 16 studies showed that minocycline-containing regimens are indeed effective in eradicating H. pylori. The ITT analysis reported a pooled proportion of 0.83, 95% CI: 0.79–0.87, p < 0.05, with significant heterogeneity between studies (I2 = 84.06%, and p < 0.05), as illustrated in Figure 5(a). The PP analysis reported a pooled proportion of 0.88, 95% CI: 0.83–0.92, p < 0.05, with significant heterogeneity between studies (I2 = 89.81%, and p < 0.05), as illustrated in Figure 5(b). Sensitivity analyses failed to identify the source of this heterogeneity, as illustrated in Figure 5(c) and (d).
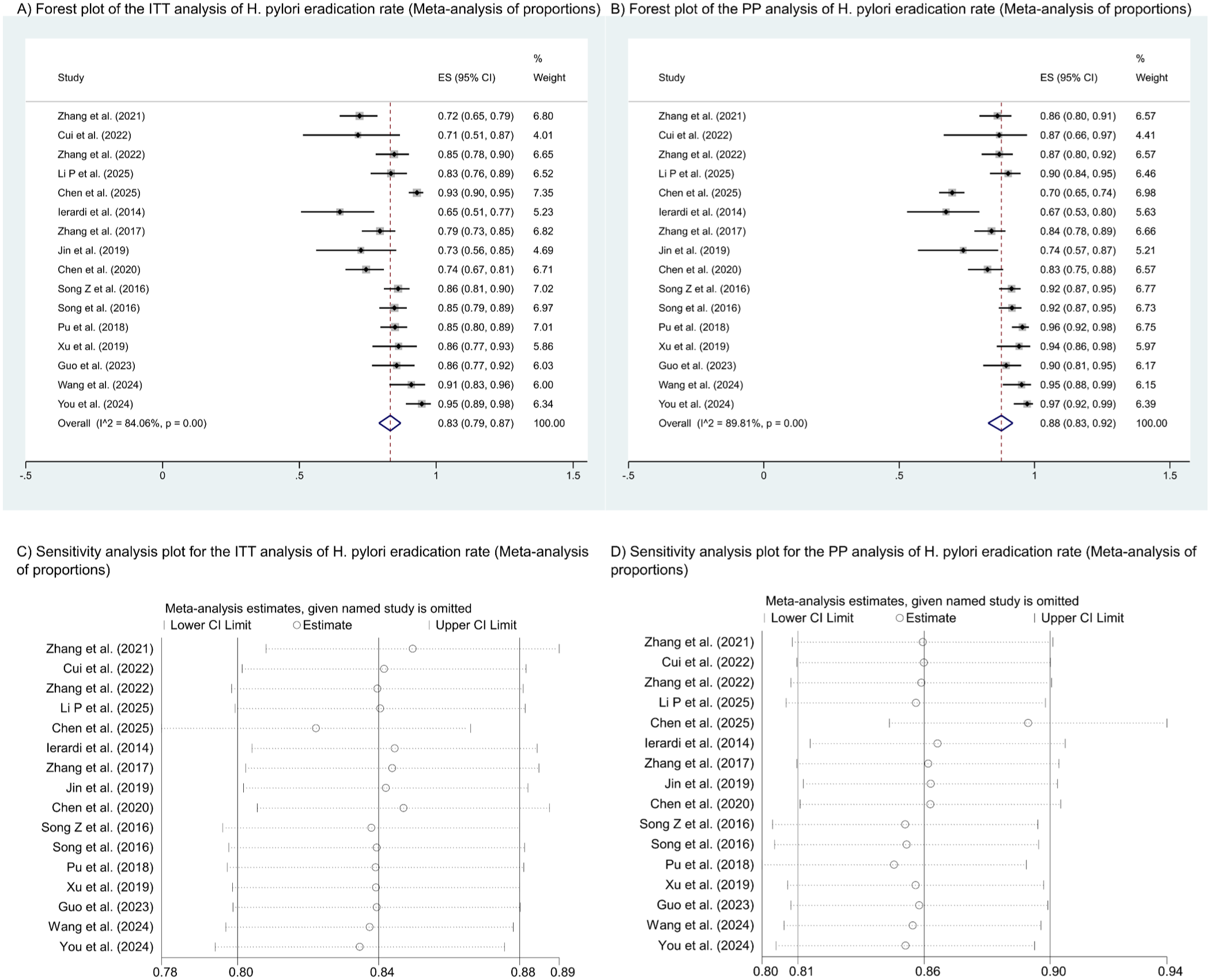
Forest plot and sensitivity analysis plot of Helicobacter pylori (H. pylori) eradication rate (meta-analysis of proportions). (a) Forest plot of the ITT analysis of H. pylori eradication rate (meta-analysis of proportions). (b) Forest plot of the PP analysis of H. pylori eradication rate (meta-analysis of proportions). (c) Sensitivity analysis plot of the ITT analysis of H. pylori eradication rate (meta-analysis of proportions). (d) Sensitivity analysis plot of the PP analysis of H. pylori eradication rate (meta-analysis of proportions).
Incidence of adverse reactions
Of the 5112 participants receiving the minocycline-containing treatment regimen, 1595 (31.2%) reported adverse reactions; common adverse reactions included dizziness (12.77%), nausea (12.75%), abdominal discomfort (7.16%), and diarrhea (6.38%), as shown in Supplemental Table 5.
A pairwise meta-analysis showed that, in terms of the incidence of adverse reactions, minocycline-containing treatment regimens significantly reduced the incidence of adverse reactions compared with the control group (RR = 0.85, 95% CI: 0.78–0.92, p < 0.05), as shown in Supplemental Figure 7. Heterogeneity between studies was low (I2 = 25%, and p = 0.17).
A meta-analysis of proportions from 15 studies showed that the pooled adverse reaction rate for minocycline-containing regimens was 0.29, 95% CI: 0.23–0.36, p < 0.05, as illustrated in Supplemental Figure 8. There was a substantial heterogeneity among the studies (I2 = 91.49%, and p < 0.05); sensitivity analyses failed to identify the source of this heterogeneity, as illustrated in Supplemental Figure 9.
Compliance rate
A pairwise meta-analysis showed that minocycline-containing regimens did not differ significantly from the control group in terms of compliance rate (RR = 1.01, 95% CI: 1.00–1.03, p = 0.15), as illustrated in Supplemental Figure 10. Heterogeneity between studies was low (I2 = 28%, and p = 0.16).
A meta-analysis of proportions from 9 studies showed that minocycline-containing regimens the pooled compliance rate for minocycline-containing regimens was 0.94, 95% CI: 0.91–0.96, p < 0.05, as illustrated in Supplemental Figure 11. There was substantial heterogeneity among the studies (I2 = 70.88%, and p < 0.05); sensitivity analyses failed to identify the source of this heterogeneity, as illustrated in Supplemental Figure 12.
Publication bias and quality of evidence
Funnel plots were constructed to assess publication bias in the H. pylori eradication rates obtained from the two meta-analyses; the funnel plots appeared visually symmetrical (Figure 6(a)–(d)). Furthermore, both the Egger’s test and the Begg’s test indicated that p > 0.05, suggesting no statistically significant evidence of publication bias. The funnel plots showing the incidence of adverse reactions and compliance are presented in Supplemental Figures 13–16. According to the GRADE system, the evidence for H. pylori eradication rates in both the ITT and PP analyses was of low certainty, while the evidence for the incidence of adverse reactions was of high certainty, and the evidence for compliance was of moderate certainty, as illustrated in Supplemental Table 6.
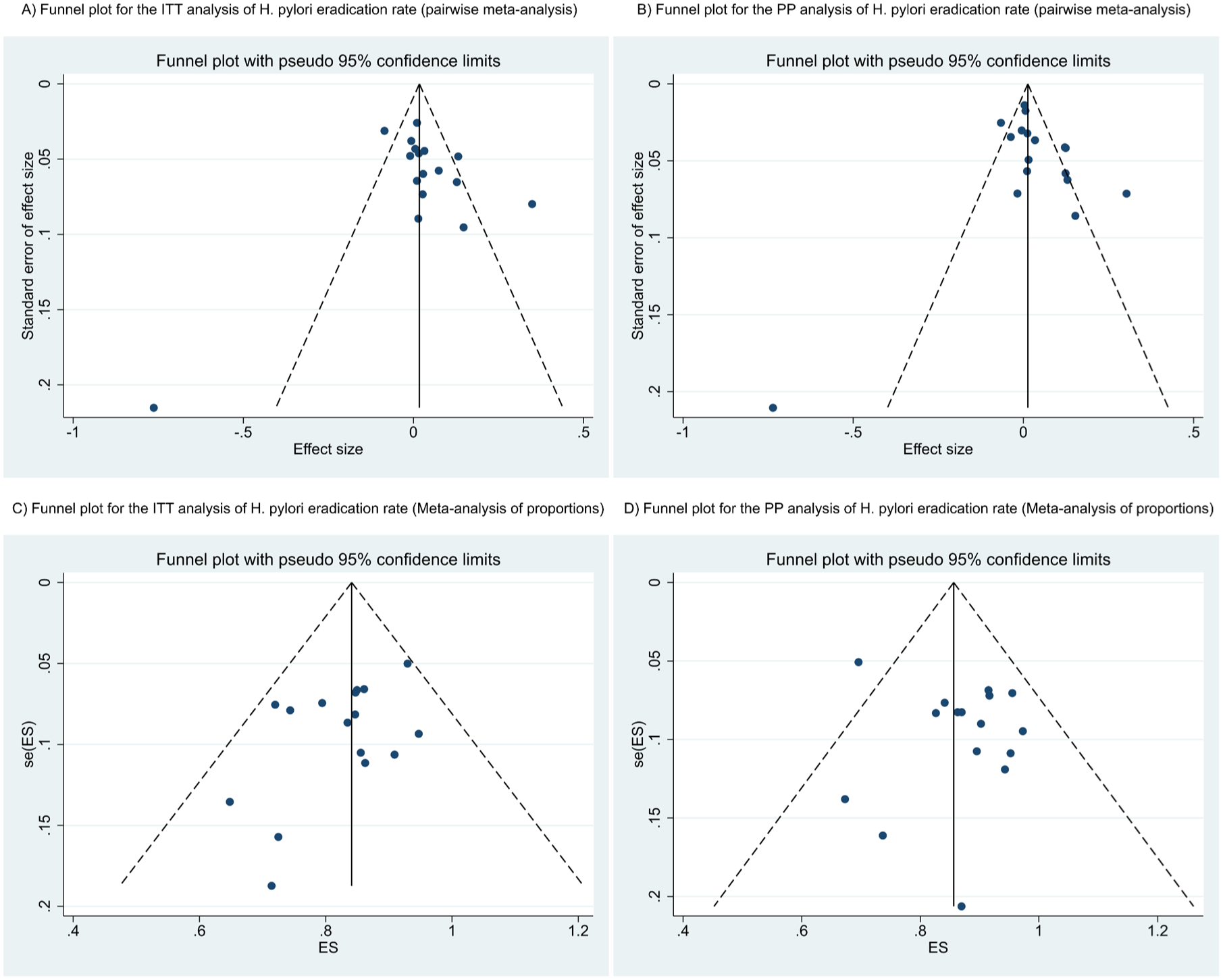
Funnel plot of Helicobacter pylori (H. pylori) eradication rate. (a) Funnel plot for the ITT analysis of H. pylori eradication rate (pairwise meta-analysis). (b) Funnel plot for the PP analysis of H. pylori eradication rate (pairwise meta-analysis). (c) Funnel plot for the ITT analysis of H. pylori eradication rate (meta-analysis of proportions). (d) Funnel plot for the PP analysis of H. pylori eradication rate (meta-analysis of proportions).
Discussion
Resistance to minocycline
The 18 studies reported data on H. pylori resistance to minocycline; however, differences in susceptibility testing methods and resistance breakpoints may affect the comparability of the results. Specifically, seven studies used the E-test,36,37,40 –44 nine employed the agar dilution method,27 –34,39 and two utilized the Kirby-Bauer disc diffusion method.35,38 The E-test combines ease of use with quantitative accuracy; the agar dilution method is a traditional reference method but requires a high degree of standardization; the disc diffusion method has the lowest level of standardization, is most susceptible to laboratory conditions, and does not explicitly report MIC breakpoints, thus limiting direct comparability. Furthermore, resistance breakpoint standards are inconsistent: Chinese studies predominantly use >8 μg/mL36,37,40,41 and >1 μg/mL.42 –44 The observed differences in resistance rates primarily reflect the baseline MIC distribution characteristics of different regions and populations, rather than selection effects arising from the breakpoint standards themselves. Given the aforementioned methodological heterogeneity, this study did not perform a pooled analysis of resistance rates, instead presenting descriptive summaries. Overall, the resistance rate for minocycline remains relatively low compared to other antibiotics. Future studies should standardize antimicrobial susceptibility testing methods and breakpoint criteria, prioritizing the use of E-tests or standardized agar dilution methods to enhance the cross-study comparability of resistance surveillance data.
Clinical application of eradication regimens containing minocycline
This meta-analysis included 33 studies. Based on pairwise meta-analysis, both the ITT and PP analyses showed no significant difference in H. pylori eradication rates between the minocycline-containing eradication regimen and the control group; however, the overall incidence of adverse reactions was significantly lower, while compliance rate was comparable to those of the control group. Based on meta-analysis of proportions, the ITT analysis indicated the H. pylori eradication rate was 83% (95% CI: 79%–87%), while the PP analysis showed eradication rates of 88% (95% CI: 83%–92%), adverse reaction incidence of 29% (95% CI: 23%–36%), and compliance rates of 94% (95% CI: 91%–96%). This suggests that minocycline may serve as an alternative treatment for H. pylori infection, offering an acceptable eradication rate while reducing the incidence of adverse reactions and ensuring good patient compliance.
Application of different minocycline-based eradication regimens
Bismuth quadruple therapy
Among the 33 studies included in this research, 30 utilized bismuth quadruple therapy. The most prevalent combination was bismuth quadruple therapy with minocycline and amoxicillin (13 studies), particularly for patients receiving both first-line and rescue therapies. ITT analysis revealed H. pylori eradication rates between 79.4% 73 and 94.7%, 44 while PP analysis indicated eradication rates spanning 84.1% 73 –97.3%, 44 with adverse reaction rates varying from 5.50% 70 to 51% 64 and patient compliance rates between 82.5% 67 and 99.1%. 44 Amoxicillin demonstrates low and stable resistance rates, which are essential for the treatment of H. pylori infection. However, its use is contraindicated in penicillin-allergic patients, posing challenges for their treatment. Consequently, minocycline-metronidazole quadruple therapy is frequently employed (10 studies), particularly as a first-line treatment for penicillin-allergic patients. ITT analysis showed H. pylori eradication rates ranging from 71.4% 62 to 90.3%, 43 while PP analysis indicated rates from 83.6% 51 to 98.0%. 42 Adverse reaction rates were reported between 34.9% 41 and 55.4%, 42 with patient compliance rates ranging from 88% 42 to 96.5%. 43 The quadruple therapy may also include minocycline in combination with rifabutin, furazolidone, levofloxacin, cefuroxime, clarithromycin, or ornidazole for H. pylori infection. ITT analysis revealed eradication rates from 72.5% 59 to 92.1%, 56 while PP analysis indicated rates between 73.7% 59 and 95.5%. 56 The incidence of adverse reactions ranged from 7.40% 57 to 33.8%, 51 with patient compliance rates at or above 90%. In certain studies, the incidence of adverse reactions associated with minocycline quadruple therapy was notably high, with prevalent symptoms such as nausea and dizziness. Nevertheless, these reactions were typically mild and subsided following the cessation of the medication. Huang et al. 43 employed a quadruple regimen of minocycline 50 mg twice daily, suggesting that this regimen offers higher adherence and a lower incidence of adverse reactions without compromising eradication efficacy; however, as there are currently few relevant studies, further validation is required. The results of this study suggest that regimens containing minocycline significantly reduce the incidence of adverse reactions compared with other regimens. Furthermore, in 2014, Ierardi et al. 57 utilized minocycline in conjunction with tinidazole as a rescue therapy, achieving an eradication rate of 51.9%. This comparatively lower rate may be ascribed to the elevated resistance rate of tinidazole and its prior application in first-line treatment regimens.
Dual therapy
Among the studies included, two employed the dual therapy of vonoprazan and minocycline. In an RCT evaluating dual therapy as first-line treatment, ITT and PP analyses demonstrated eradication rates of 87.5% and 92.0%, respectively, indicating non-inferiority efficacy compared with bismuth quadruple therapy. The incidence of adverse reactions in the vonoprazan and minocycline dual therapy was significantly lower than that in bismuth quadruple therapy (16.7% vs 28.3%), with patient compliance at 94.2%. 13 In a cohort study evaluating the efficacy of dual therapy, 54 patients receiving first-line therapy, 13 patients having failed one treatment regimen, and 21 patients having failed multiple treatment regimens were included. ITT analysis showed H. pylori eradication rates of 90.7%, 84.6%, and 95.2%, respectively, while PP analysis reported rates of 94.2%, 91.7%, and 100%. The overall incidence of adverse events in the dual therapy was 23.0%. The most common adverse reactions were nausea and mild dizziness, which resolved spontaneously without intervention. Patient compliance reached 96.4%. 69 The vonoprazan and minocycline dual therapy demonstrated favorable eradication rates, low incidence of side effects, and excellent compliance, making it a promising new treatment option for both first-line and rescue therapy.
Combined probiotics and Chinese medicine
Among the studies included, three utilized the bismuth quadruple therapy that combined probiotics61,64 or Chinese medicine. 55 In first-line treatment, the quadruple therapy containing minocycline and amoxicillin, along with Saccharomyces boulardii, achieved an eradication rate comparable to that of the quadruple therapy alone, while substantially lowering the incidence of adverse reactions (20.4% vs 51.0%). 64 In rescue therapy, the bismuth quadruple therapy containing minocycline and moxifloxacin combined with Live Combined Bifidobacterium and Lactobacillus Tablets improved H. pylori eradication rates, while reducing the incidence of adverse reactions. 61 One study utilized a bismuth quadruple therapy combining berberine with minocycline. In first-line treatment, this regimen demonstrated comparable H. pylori eradication rates, adverse reaction incidence, and patient compliance to the quadruple therapy containing amoxicillin and clarithromycin. 55
In summary, among minocycline-containing eradication therapies, quadruple therapy is the most frequently employed regimen. Research on dual therapy, along with Chinese medicine and probiotic treatment, remains relatively limited. These therapies demonstrate advantages such as high eradication efficacy, relative safety, and favorable patient compliance.
Strengths and limitations
This study provides a comprehensive review of the pharmacokinetic characteristics, mechanism of action, resistance patterns, and clinical efficacy of minocycline in the treatment of H. pylori infection. To investigate these issues comprehensively and systematically, we included both RCTs and observational studies; however, significant heterogeneity was observed among the studies in the meta-analysis. Gao et al. 74 and Zhou et al. 10 published similar reports in 2023 and 2024, respectively, but those reviews included relatively few studies and did not systematically summarize the resistance profile of minocycline. This study has certain limitations. The included studies comprised both RCTs and observational studies, and the treatment regimens involved either quadruple or dual therapy; the quality of the studies varied considerably, and there was significant heterogeneity between them, thereby lowering the certainty of evidence.
Optimization of treatment strategies and future perspectives
The resistance rate of H. pylori to clarithromycin, metronidazole, and levofloxacin continues to rise. Minocycline has emerged as a viable alternative antibiotic. The studies indicate that H. pylori demonstrates low resistance to minocycline, and eradication therapy incorporating this antibiotic presents advantages. Nonetheless, several aspects require further optimization: (1) Precision in dosage and duration: The standard minocycline regimen for H. pylori eradication is 100 mg administered twice daily for 14 days. One study suggested that a reduced dosage of 50 mg twice daily may achieve effective eradication while minimizing adverse reactions. 43 Future clinical investigations should determine the optimal dosage and duration to ensure both efficacy and safety. (2) Selection of optimal combination antibiotics: Minocycline can currently be combined with various antibiotics for eradication therapy. Future studies should evaluate the advantages, disadvantages, and appropriate contexts for different combinations (e.g., with amoxicillin, metronidazole, rifabutin, furazolidone, etc.). (3) Selection of different eradication regimens: Additional RCTs are needed to compare the benefits, drawbacks, and applicable scenarios of minocycline-containing quadruple therapy with other salvage regimens (e.g., dual therapy, combinations with Chinese medicine or probiotics). (4) Long-term monitoring of trends in H. pylori resistance rates to minocycline: Future research should concentrate on these aspects to comprehensively elucidate the role of minocycline in H. pylori infection.
Conclusion
In summary, as antibiotic resistance in H. pylori becomes increasingly severe, minocycline has emerged as a valuable option for both first-line and rescue therapy. Studies have shown that eradication regimens containing minocycline can maintain optimal H. pylori eradication rates while reducing the incidence of adverse reactions and ensuring high compliance. However, this study has certain limitations, and further multicenter, large-scale, high-quality clinical trials are required to validate its efficacy. Future research should prioritize optimizing dosages and treatment durations, as well as elucidating the comparative advantages and appropriate clinical scenarios for various therapeutic strategies. Minocycline is positioned to play an increasingly pivotal role in addressing the challenges associated with H. pylori eradication.
Supplemental Material
sj-docx-1-tag-10.1177_17562848261464690 – Supplemental material for Minocycline-containing therapy in Helicobacter pylori infection: a systematic review and meta-analysis
Supplemental material, sj-docx-1-tag-10.1177_17562848261464690 for Minocycline-containing therapy in Helicobacter pylori infection: a systematic review and meta-analysis by Zhihua Tian, Yanjiao Zhang, Nan Luo, Xuefei Zhao, Shaoli Wang and Zhen Liu in Therapeutic Advances in Gastroenterology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.