
Abstract
Background:
A clinically significant proportion of patients experience early neurological deterioration (END) despite receiving dual antiplatelet therapy (DAPT) for acute ischemic stroke. It is crucial to identify this specific population for risk stratification and targeted intervention.
Objectives:
To identify predictors for END after DAPT in acute ischemic stroke.
Design:
We performed a post hoc analysis of the antiplatelet therapy in acute mild to moderate ischemic stroke (ATAMIS) trial.
Methods:
Patients who received DAPT (clopidogrel plus aspirin) in the ATAMIS trial were included, and classified into END and Non-END groups according to whether they experienced END. END was defined as an increase of ⩾2 points within 7 days from baseline on the National Institutes of Health Stroke Scale (NIHSS). Independent predictors were identified using multivariable logistic regression.
Results:
Of the 1,122 patients with acute mild-to-moderate ischemic stroke treated with DAPT, 66 (5.9%) developed END within 7 days. Multivariable analysis identified three independent factors associated with increased END risk: a shorter time from symptom onset to antiplatelet initiation (adjusted odds ratio [aOR] per hour, 0.97; 95% CI, 0.95–0.99; p = 0.01), higher admission systolic blood pressure (aOR per mmHg, 1.01; 95% CI, 1.00–1.02; p = 0.047), and a stroke etiology of either small artery occlusion (aOR, 2.24; 95% CI, 1.29–3.89; p = 0.004) or cardioembolism (aOR, 28.36; 95% CI, 1.23–654.11; p = 0.04).
Conclusion:
Among patients with mild-to-moderate ischemic stroke receiving DAPT, key predictors of END include very early presentation, elevated systolic blood pressure at admission, and a nonlarge artery atherosclerosis etiology (small artery occlusion or cardioembolism). These findings highlight subgroups that may require intensified monitoring or adjunctive therapeutic strategies beyond standard DAPT.
Trial registration:
ClinicalTrials.gov Identifier: NCT02869009.
Plain language summary
A clinically significant proportion of patients experience early neurological deterioration (END) despite receiving dual antiplatelet therapy (DAPT) for acute ischemic stroke. Identifying risk factors for END in this specific population is crucial for risk stratification and targeted intervention. We performed a post hoc analysis of the Antiplatelet Therapy in Acute Mild to Moderate Ischemic Stroke (ATAMIS) trial, focusing on patients who received DAPT (clopidogrel plus aspirin). The primary outcome was END within 7 days, defined as an increase of ⩾2 points from baseline on the National Institutes of Health Stroke Scale (NIHSS). Independent predictors were identified using multivariable logistic regression. Of the 1,122 patients with acute mild-to-moderate ischemic stroke treated with DAPT, 66 (5.9%) developed END within 7 days. Multivariable analysis identified three independent factors associated with increased END risk: a shorter time from symptom onset to antiplatelet initiation (adjusted odds ratio [aOR] per hour, 0.97; 95% CI, 0.95–0.99; p = 0.01), higher admission systolic blood pressure (aOR per mmHg, 1.01; 95% CI, 1.00–1.02; p = 0.047), and a stroke etiology of either small artery occlusion (aOR, 2.24; 95% CI, 1.29–3.89; p = 0.004) or cardioembolism (aOR, 28.36; 95% CI, 1.23–654.11; p = 0.04). Thus, among patients with mild-to-moderate ischemic stroke receiving DAPT, key predictors of END include very early presentation, elevated systolic blood pressure at admission, and a non-large artery atherosclerosis etiology (small artery occlusion or cardioembolism). These findings highlight subgroups that may require intensified monitoring or adjunctive therapeutic strategies beyond standard DAPT.
Introduction
Current guidelines endorse reperfusion therapies as the standard of care for acute ischemic stroke. 1 However, due to stringent time windows and limited access to endovascular centers, the majority of patients are ineligible for these interventions and instead receive antiplatelet treatment. 2 In patients with minor stroke or high-risk transient ischemic attack, landmark trials—CHANCE, POINT, and INSPIRES—established that dual antiplatelet therapy (DAPT) with clopidogrel and aspirin, initiated within 24 to 72 h of symptom onset, significantly reduces early stroke recurrence compared to aspirin alone, particularly in those with large artery atherosclerosis.3–5 Despite this evidence, monotherapy with aspirin remains the guideline-recommended standard for patients with mild-to-moderate deficits, 1 a population nonetheless at substantial risk for early neurological deterioration (END)—a complication strongly linked to poor long-term prognosis.6–8
The Antiplatelet Therapy in Acute Mild to Moderate Ischemic Stroke (ATAMIS) trial provided pivotal evidence, demonstrating that DAPT significantly reduces the incidence of END at 7 days compared to aspirin alone in patients treated within 48 h of symptom onset. 9 Nevertheless, a clinically relevant proportion of patients in ATAMIS and in our prior analysis still experienced END despite receiving DAPT.9,10 Identifying the risk factors for END in this specific population is critical to recognize high-risk individuals, elucidate underlying mechanisms, and inform targeted strategies to mitigate this complication. While prior studies have explored END risk factors in broader stroke cohorts, including those receiving reperfusion therapy,8,11,12 data specifically focusing on patients treated with DAPT are lacking. Furthermore, whether END occurring in the context of DAPT retains its established association with poor functional outcomes remains uncertain.
To address these gaps, we conducted a post hoc analysis of the ATAMIS trial. Our objectives were twofold: first, to identify factors independently associated with END at 7 days in patients receiving DAPT; and second, to evaluate the association between END and 90-day functional outcome in this population.
Methods
This post hoc analysis was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline.
Study design and participants
This was a post hoc analysis of individual patient data from the ATAMIS trial. The ATAMIS trial was a multicenter, open-label, blinded-endpoint, randomized clinical trial that enrolled 3000 patients between December 2016 and August 2022. It evaluated the efficacy of clopidogrel plus aspirin versus aspirin alone in patients with acute mild-to-moderate ischemic stroke (baseline National Institutes of Health Stroke Scale [NIHSS] scores 4–10) within 48 h of symptom onset. 13 The ATAMIS trial was registered with ClinicalTrials.gov (NCT02869009).
Procedure
For the current analysis, we included patients from the modified intention-to-treat population who received DAPT. Patients with incomplete baseline data were excluded. The included cohort was then stratified into two groups based on the occurrence of END during DAPT: the END group and the Non-END group. END was defined as an increase of ⩾2 points in the NIHSS score at 7 days compared to the baseline. 14
The DAPT regimen in ATAMIS consisted of a 300-mg clopidogrel loading dose plus 100 mg of aspirin on Day 1, followed by 75 mg/day clopidogrel and 100 mg/day aspirin from Day 2 to 14, and then either 75 mg/day clopidogrel or 100 mg/day aspirin from Day 15 to 90. 9 Stroke etiology was classified according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria. 15 The NIHSS score was assessed at admission and at 7 days by the same certified assessor at each center. The 90-day modified Rankin Scale (mRS) score was assessed via in-person or telephone interview by trained, certified personnel who were blinded to treatment allocation.
Statistical analysis
Continuous variables are presented as median (interquartile range (IQR)) and categorical variables as frequency (percentage). Group comparisons for baseline characteristics were performed using the Mann-Whitney U test or the Chi-square test, as appropriate.
Associations between potential risk factors and END were analyzed using binary logistic regression. Variables with a p value <0.1 in univariable analysis, along with established risk factors from prior literature (history of hypertension, diabetes, atrial fibrillation, previous transient ischemic attack, baseline NIHSS score, and prior antiplatelet use),12,16 were entered into a multivariable logistic regression model. Results are expressed as odds ratios (ORs) with 95% confidence intervals (CIs). The collinearity will be tested by calculating variance inflation factor (VIF). Furthermore, considering lower proportion of patients with END, we performed inverse probability of treatment weighting as a sensitivity analysis. The propensity scores were estimated using a logistic regression model that included all covariates originally used in the primary multivariable model. The weighted logistic regression analysis was then repeated to estimate the association between these covariates and END.
The association between END and the distribution of 90-day mRS scores was analyzed using an ordinal regression model, adjusted for all risk factors that achieved statistical significance (p < 0.05) in the final multivariable logistic model.
All analyses were considered exploratory. A two-sided p value < 0.05 was considered statistically significant. Analyses were performed using SPSS software (version 26.0; IBM Corp., Armonk, NY, USA).
Results
Study participants
From the ATAMIS trial, 1516 patients were documented as having received DAPT, including those who crossed over from monotherapy. After excluding 394 patients with incomplete baseline data, the final analysis cohort comprised 1122 patients (Figure 1). Among these, 66 patients (5.9%) experienced END within 7 days of DAPT initiation, constituting the END group, while 1056 patients comprised the Non-END group. The baseline characteristics of the total cohort and the two subgroups are detailed in Table 1.
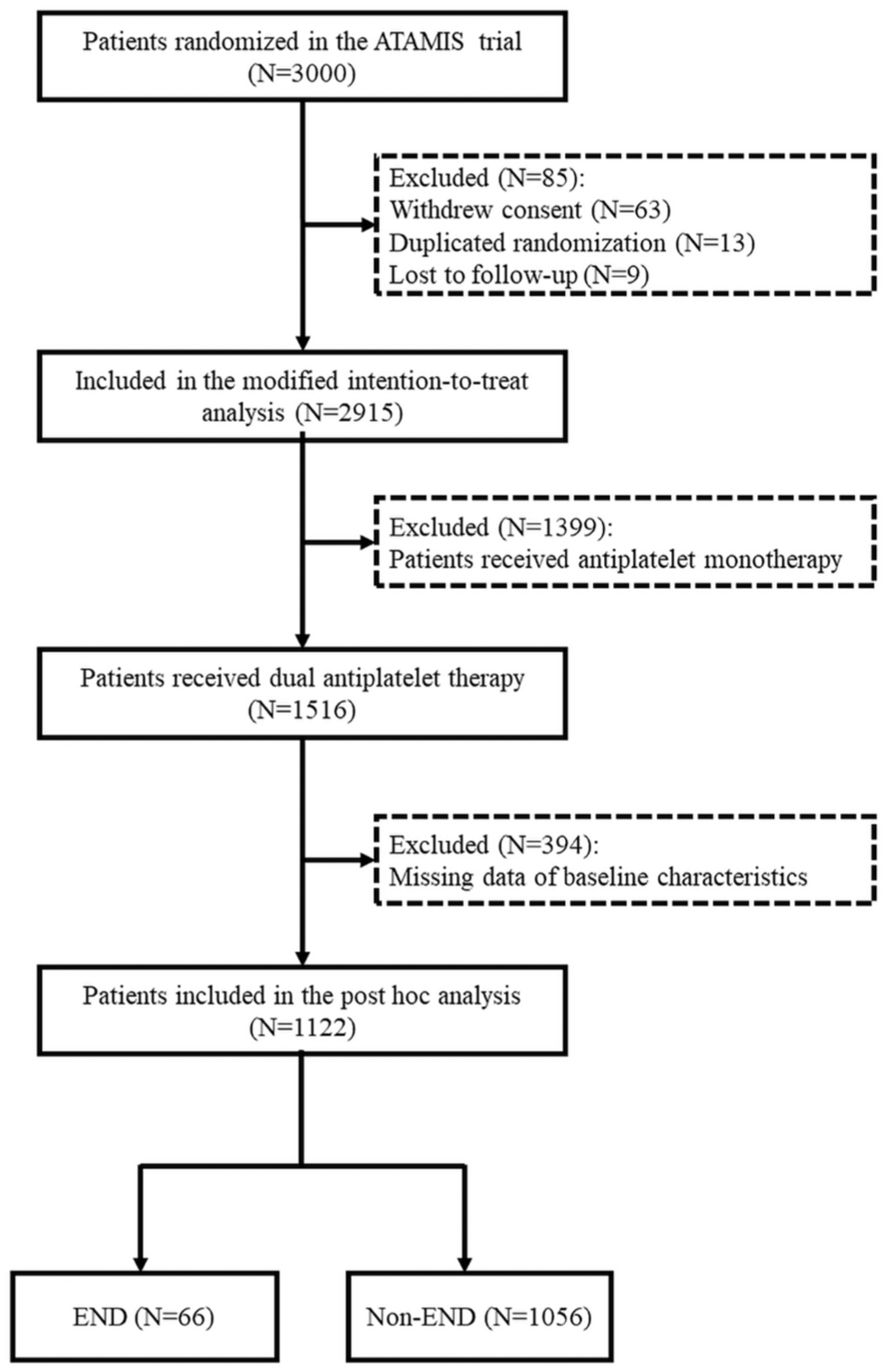
Trial profile.
Baseline characteristic in patients with END and without END.
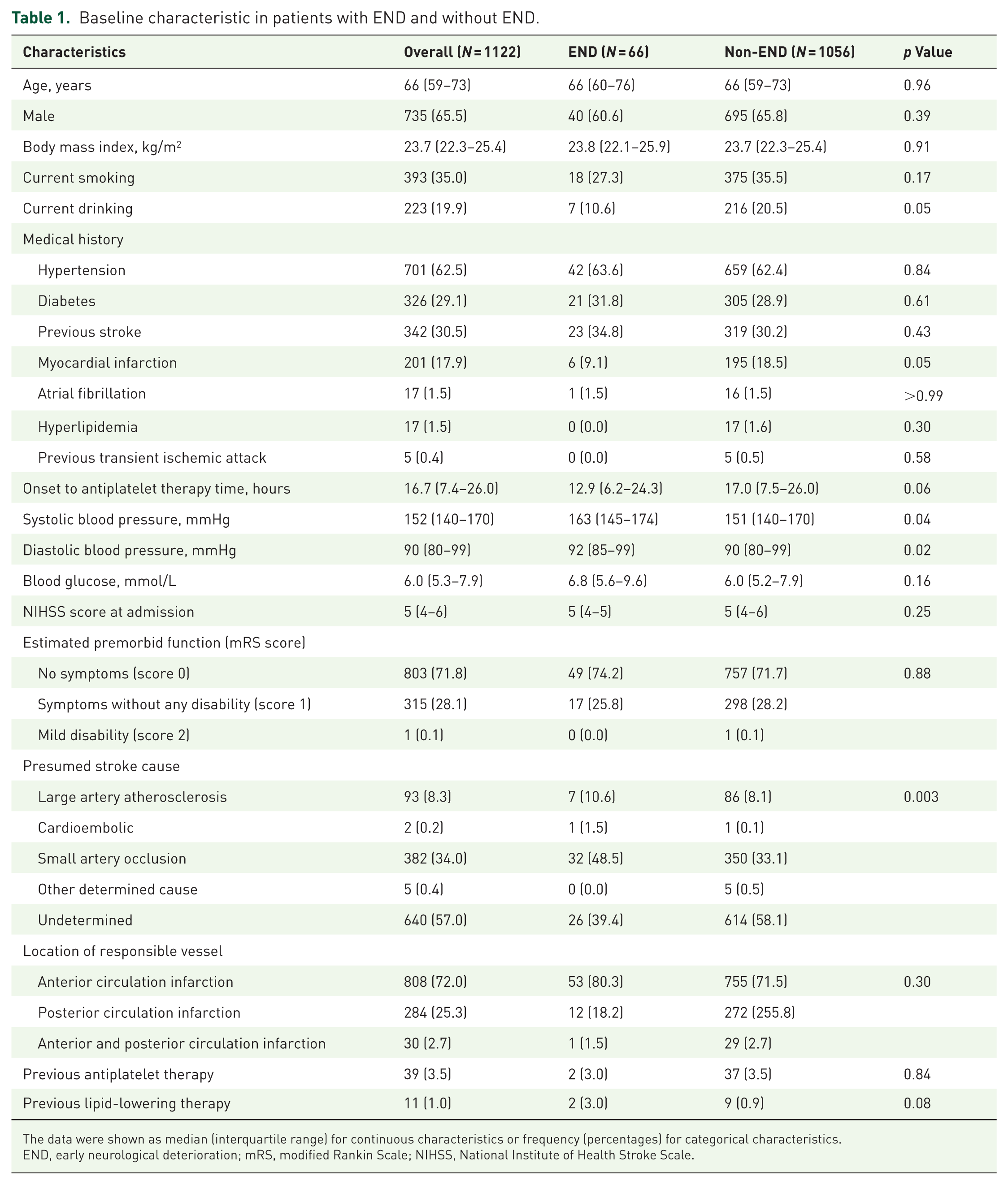
The data were shown as median (interquartile range) for continuous characteristics or frequency (percentages) for categorical characteristics.
END, early neurological deterioration; mRS, modified Rankin Scale; NIHSS, National Institute of Health Stroke Scale.
Risk factors associated with END
Baseline characteristics were compared between the END and Non-END groups. Univariable logistic regression identified several potential risk factors associated with END: current drinking (OR 0.46, 95% CI 0.21–1.02; p = 0.06), history of myocardial infarction (OR 0.44, 95% CI 0.19–1.04; p = 0.06), time from symptom onset to antiplatelet therapy initiation (OR 0.97 per hour, 95% CI 0.95–0.99; p = 0.02), admission systolic blood pressure (OR 1.01 per mmHg, 95% CI 1.00–1.02; p = 0.04), admission blood glucose (OR 1.07, 95% CI 0.99–1.14; P = 0.05), and presumed stroke etiology (OR 0.79, 95% CI 0.66–0.94; p = 0.007) (Table 2).
Univariable analysis (Odds ratio associated with END).
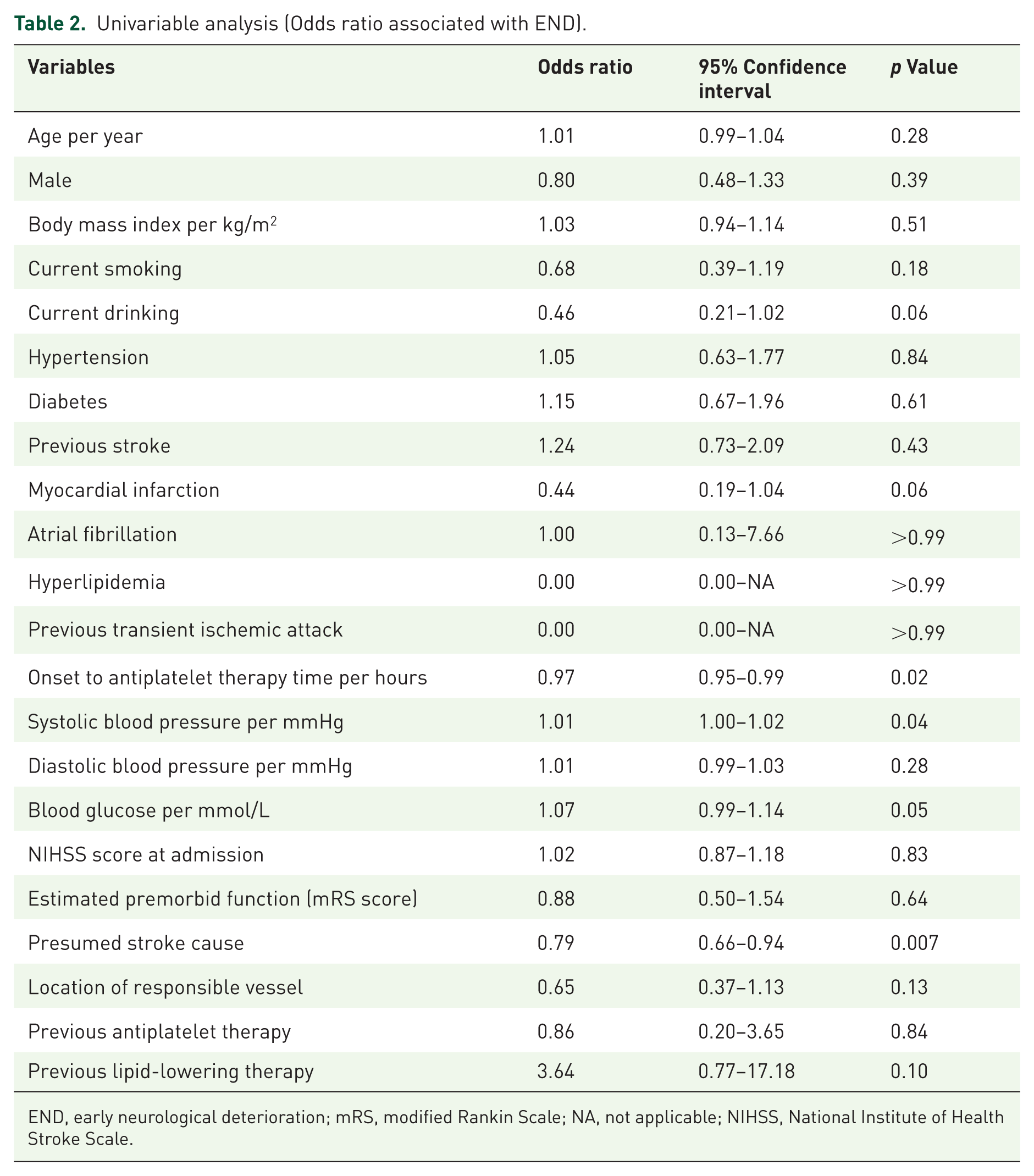
END, early neurological deterioration; mRS, modified Rankin Scale; NA, not applicable; NIHSS, National Institute of Health Stroke Scale.
Multivariable logistic regression, incorporating variables with p < 0.1 in univariable analysis and predefined clinical factors, identified three independent predictors of END in patients receiving DAPT (Table 3): longer time to antiplatelet therapy initiation was associated with a lower risk of END (OR 0.97 per hour, 95% CI 0.95–0.99; p = 0.01), higher admission systolic blood pressure was associated with an increased risk (OR 1.01 per mmHg, 95% CI 1.00–1.02; p = 0.047), and specific stroke etiologies conferred significantly higher risk, with the strongest association observed for cardioembolic stroke (OR 28.36, 95% CI 1.23–654.11; p = 0.04), followed by small artery occlusion (OR 2.24, 95% CI 1.29–3.89; p = 0.004). All VIF values of covariates included in the multivariable logistic regression were < 2, indicating no substantial multicollinearity. The result of sensitivity analysis was consistent with the primary analysis (Table 3).
Multivariable analysis (odds ratio associated with END).
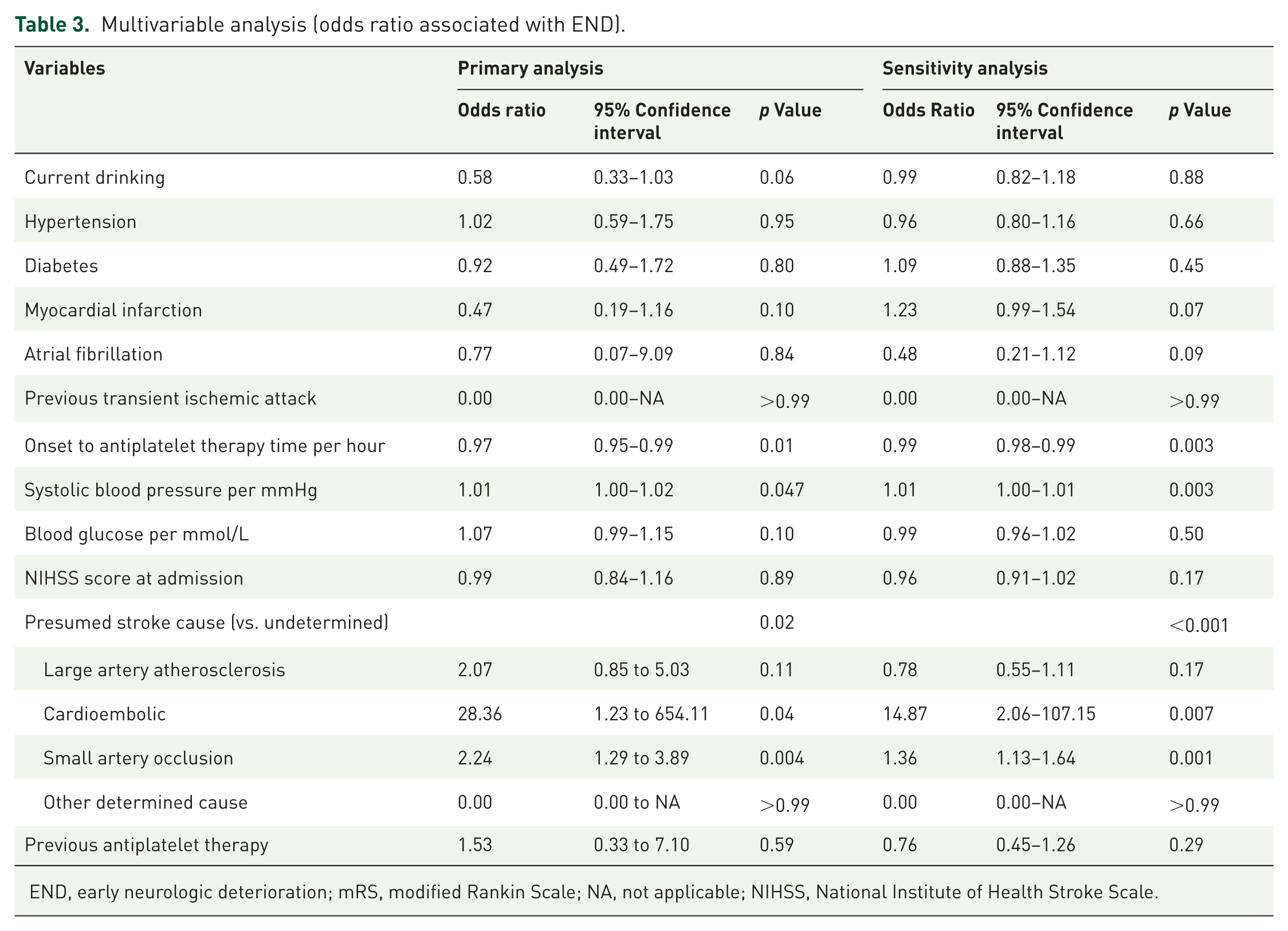
END, early neurologic deterioration; mRS, modified Rankin Scale; NA, not applicable; NIHSS, National Institute of Health Stroke Scale.
Association of END with functional outcome
The distribution of 90-day mRS scores was significantly worse in the END group compared to the Non-END group (Figure 2). Ordinal regression analysis confirmed that experiencing END within 7 days was strongly and independently associated with poorer functional outcome at 90 days (common OR 0.09, 95% CI 0.06–0.15; p < 0.001).
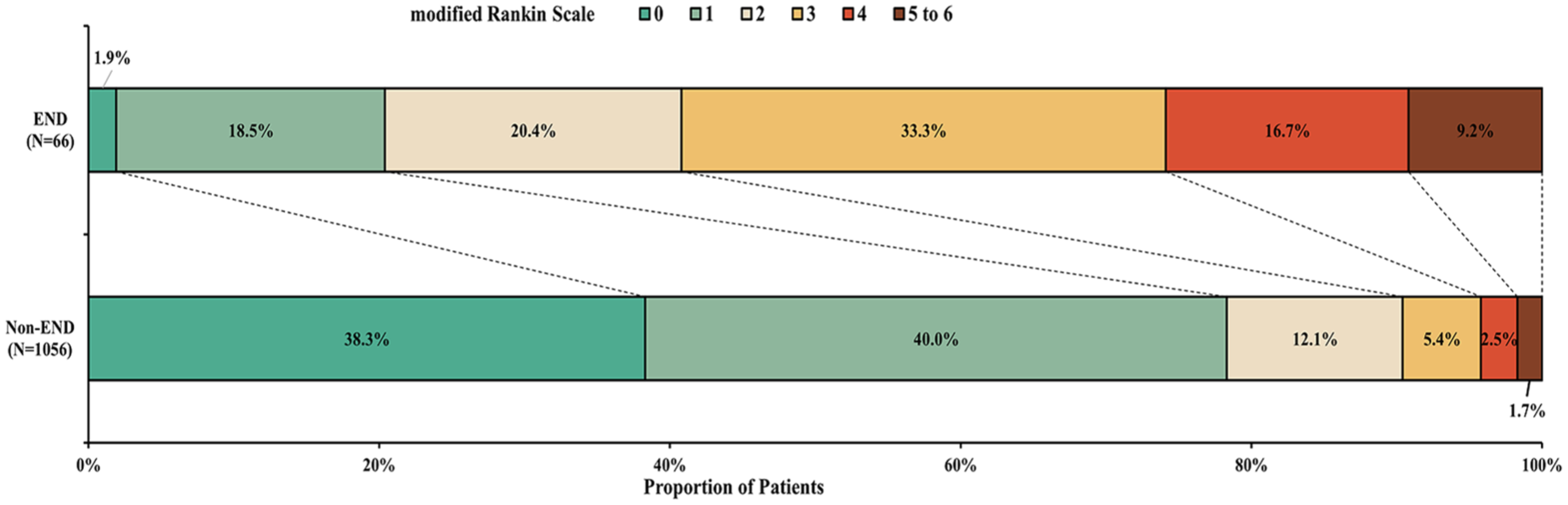
Distribution of modified Rankin Scale Score at 90 days. The raw distribution of scores was shown in patients with END versus without END. Scores ranged from 0 to 6. 0 = no symptoms, 1 = symptoms without clinically significant disability, 2 = slight disability, 3 = moderate disability, 4 = moderately severe disability, 5 = severe disability, and 6 = death. Abbreviations: END indicates early neurological deterioration. A shift measure of function according to the full range of scores on the mRS at 90 days was investigated by ordinal regression analysis, and the chi-square for the likelihood ratio test were 18.1 (p = 0.96). The odds ratio was 0.09 and 95% confidence interval was 0.06 to 0.15 (p < 0.001).
Discussion
In this post hoc analysis of the ATAMIS trial, we found that (1) in patients receiving DAPT for mild-to-moderate ischemic stroke, a shorter time from symptom onset to treatment, higher admission systolic blood pressure, and stroke etiology of cardioembolism or small artery occlusion were independently associated with a higher risk of END within 7 days; and (2) END following DAPT remained strongly associated with poorer 90-day functional outcomes.
END is a well-established predictor of poor prognosis in acute ischemic stroke.7,8,11 In our cohort, the incidence of END was 5.9%, a rate lower than that reported in our previous study of a population with large artery atherosclerosis. 10 This discrepancy may be attributed to the distinct etiologic profile of the present cohort, in which nearly 90% of strokes were classified as small artery occlusion or of undetermined cause, whereas large artery atherosclerosis itself is a known independent risk factor for END. 12 Crucially, despite the administration of DAPT, END remained a potent determinant of poor long-term outcome, reinforcing the imperative to prevent this complication even in patients receiving intensive antiplatelet regimens.
Our analysis provides insights into the profile of patients at heightened risk for END despite DAPT. First, higher admission systolic blood pressure was an independent risk factor, consistent with prior evidence. 17 This may reflect underlying poor cerebral hemodynamic reserve or inadequate collateral circulation, which predisposes the ischemic penumbra to further injury.18,19 Second, contrary to the intuitive expectation, a shorter onset-to-treatment time was associated with a higher risk of END. On the one hand, in the ATAMIS trial, patients who received reperfusion therapies were excluded and the mean time from symptom onset to antiplatelet initiation was about 19 h, which was a sub-acute phase of stroke. END mainly occurred in the earlier phase, during which reperfusion therapies may be effective compared with antiplatelet given that more aggressive infarct expansion in the hyperacute phase were attributed to persistent arterial occlusion.20,21 On the other hand, in this prespecified subgroup analysis of the ATAMIS trial, 22 initiation of DAPT < 24 h after symptom onset was highly effective, whereas later initiation was not. Thus, although shorter time to initiate was associated with higher END, it was still necessary to start DAPT as early as possible. Third, patients with cardioembolic or small artery occlusion etiology were at elevated risk. The efficacy of DAPT is known to be etiology-dependent, with the greatest benefit observed in LAA.23,24 For cardioembolic strokes, anticoagulation is the guideline-recommended therapy for secondary prevention.1,25 The high risk observed in small vessel disease may be related to factors such as hypertension, hyperglycemia, and strategic infarct location, 26 suggesting that optimized risk factor management may be as critical as antiplatelet therapy in this population. Notably, established risk factors like higher baseline NIHSS score or prior antiplatelet use were not significant in our model, possibly due to the overall milder stroke severity and lower prevalence of prior therapy in our cohort, limiting statistical power.
Several limitations merit consideration. First, the relatively low event rate of END constrained the statistical power of our multivariable models as well as introduced risk of overfitting. Second, the absence of serial blood pressure monitoring precluded an analysis of blood pressure variability, a parameter potentially more reflective of impaired cerebral autoregulation than a single admission measurement, resulting in END. 27 Third, the high proportion of strokes classified as undetermined etiology, due to the lack of systematic vascular imaging, may have obscured stronger etiologic associations. Fourth, we lacked data on genetic polymorphisms (e.g., CYP2C19) that influence clopidogrel response. 28 Fifth, without advanced imaging (e.g., angiography, perfusion studies), we could not explore imaging predictors of END or elucidate mechanistic roles of vessel occlusion or cerebral edema. Finally, some imbalance (e.g., history of diabetes, stroke, or myocardial infarction) between included and excluded patients in the current study may introduce potential selection bias.
Conclusion
This analysis indicates that a residual risk of END persists despite DAPT and continues to predict poor functional outcomes. Patients presenting with elevated systolic blood pressure, earlier time after symptom onset, or a non-LAA etiology (cardioembolism or small artery occlusion) appear to be at particular risk. These findings suggest that treatment strategies beyond standard DAPT—such as meticulous hemodynamic management, consideration of adjunctive antithrombotic agents in select cases, and rigorous control of vascular risk factors—may be needed to mitigate END in high-risk subgroups. These hypotheses require prospective validation in larger, more comprehensively phenotyped cohorts, including non-Chinese populations.
Supplemental Material
sj-docx-1-tan-10.1177_17562864261461421 – Supplemental material for Residual early neurological deterioration following dual antiplatelet in stroke: post hoc analysis of the ATAMIS trial
Supplemental material, sj-docx-1-tan-10.1177_17562864261461421 for Residual early neurological deterioration following dual antiplatelet in stroke: post hoc analysis of the ATAMIS trial by Yu Cui, Xiang-Ru Kong, Jing Zhang and Hui-Sheng Chen in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.