
Abstract
Background:
Continuous subcutaneous foslevodopa/foscarbidopa (FLD/FCD) is the first 24-h levodopa-based subcutaneous infusion therapy for advanced Parkinson’s disease (PD). Real-world data from the Middle East region are absent.
Objectives:
To report the first Middle Eastern clinical experience with foslevodopa/foscarbidopa, evaluating motor and non-motor outcomes, safety profile, and treatment continuation rates in routine clinical practice.
Design:
Retrospective, single-center, observational cohort study.
Methods:
Twenty-eight consecutive patients with advanced PD underwent inpatient foslevodopa/foscarbidopa initiation between January 2025 and January 2026 at a quaternary academic medical center in Abu Dhabi, United Arab Emirates. Primary outcomes were Movement Disorder Society Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) Part III, daily OFF/ON hours, and Hoehn and Yahr stage; secondary outcomes included Non-Motor Symptoms Scale (NMSS) total and domain scores and MDS-UPDRS Parts I and II. Motor assessments were conducted in the practically defined OFF state at baseline and in the ON state at follow-up on stable foslevodopa/foscarbidopa therapy. Safety was assessed by systematic recording of adverse events. Paired comparisons used Wilcoxon signed-rank tests.
Results:
Mean age was 61.3 ± 13.5 years; disease duration 10.1 ± 7.4 years; baseline levodopa equivalent daily dose 1018 ± 574 mg. MDS-UPDRS Part III improved from 50.7 ± 14.5 (OFF-state baseline) to 27.1 ± 13.6 (ON-state follow-up; change −23.6 ± 8.3, p < 0.0001), representing elimination of wearing-off disability. Daily OFF time fell from 2.8 ± 1.4 to 0.9 ± 0.6 h (−1.9 ± 1.4 h; p < 0.0001), and good ON time increased by 2.0 ± 1.3 h (p < 0.0001). Hoehn and Yahr stage improved from median 3 (interquartile range (IQR) 3–4) to 2 (IQR 2–3; p < 0.0001). Non-motor symptom burden decreased substantially: MDS-UPDRS Parts I and II fell by 22.7 ± 9.3 points (p = 0.001) and NMSS total score by 29.7 ± 18.7 points (~49% reduction; p = 0.0007). Infusion site reactions occurred in 22 patients (79%) but were generally manageable. Six patients (21%) discontinued therapy (median 4.8 months), primarily because of skin reactions or compliance difficulties.
Conclusion:
Foslevodopa/foscarbidopa produced clinically meaningful improvements in motor fluctuations and non-motor symptom burden in this first Middle Eastern real-world cohort, supporting its role as an effective and feasible non-surgical device-aided therapy for advanced PD.
Plain language summary
Parkinson’s disease causes shaking, stiffness, and slow movement that worsens over time. As the disease advances, standard levodopa tablets stop working smoothly, leaving patients unable to move or function for unpredictable periods each day. Existing advanced treatments, including brain surgery and intestinal tube pumps, require invasive procedures that many patients cannot undergo due to age, cognitive difficulties, or other medical reasons. Foslevodopa/foscarbidopa is a newly approved therapy that delivers levodopa continuously through a small wearable pump placed under the skin, requiring no surgery. This study reports the first real-world experience with this treatment in the Middle East. Twenty-eight patients with advanced Parkinson’s disease were treated at a specialist centre in Abu Dhabi, UAE, and followed for a median of nine months. Patients spent nearly two fewer hours per day unable to move and gained two additional hours of good functional time daily. Motor severity improved substantially. Non-motor symptoms, including anxiety, sleep disturbance, depression, and cognitive difficulties, improved by approximately 49%. Skin reactions at the pump site were common but resolved in all cases. Only 21% of patients discontinued therapy, and 75% reported satisfaction with treatment. These findings show that foslevodopa/foscarbidopa is effective and well-tolerated in a diverse real-world population, supporting its use beyond the settings studied in clinical trials.
Keywords
Introduction
Parkinson’s disease (PD) affects over 8.5 million individuals worldwide and is projected to double in prevalence by 2040, with disproportionate growth in the Middle East, North Africa, and Gulf Cooperation Council countries.1,2 As PD progresses, oral levodopa therapy becomes increasingly problematic because of motor fluctuations, wearing-off phenomena, and dyskinesia driven by pulsatile dopaminergic stimulation and variable gastric absorption. 3 Advanced PD patients often experience debilitating OFF periods that significantly compromise quality of life, despite optimized oral medication regimens.
Device-aided therapies (DATs) have emerged as critical management options for advanced PD when oral therapies fail to adequately control motor fluctuations. Currently available modalities include deep-brain stimulation (DBS), levodopa-carbidopa intestinal gel (LCIG) infusion, and continuous subcutaneous apomorphine infusion (CSAI). 4 Network meta-analyses demonstrate that LCIG and DBS provide superior improvements in OFF time and quality of life compared to CSAI and best medical therapy at 6 months. 5 However, each modality carries significant limitations: DBS requires neurosurgical intervention with associated risks; LCIG necessitates percutaneous endoscopic gastrojejunostomy with potential tube-related complications; and apomorphine infusion may cause neuropsychiatric side effects and subcutaneous nodules.
Foslevodopa/foscarbidopa (FLD/FCD), approved by the U.S. FDA in October 2024, represents the first continuous 24-h subcutaneous levodopa-based infusion therapy for advanced PD. 6 Foslevodopa and foscarbidopa are phosphate prodrugs of levodopa and carbidopa, respectively; their superior aqueous solubility at physiological pH enables delivery at therapeutically sufficient concentrations via a small-gauge subcutaneous cannula, circumventing the gastric absorption variability that underlies wearing-off. 7 The pivotal M15-736 phase III trial demonstrated superior efficacy versus oral immediate-release carbidopa/levodopa, with increased good ON time without troublesome dyskinesia (+2.72 vs +0.97 h; p = 0.0083) and reduced OFF time (−2.75 vs −0.96 h; p = 0.0054) at 12 weeks. 8 Long-term extension studies confirmed sustained benefits over 96 weeks. 9 Real-world evidence is emerging: the ROSSINI observational registry interim data (n = 105) reported significant reductions in OFF time and non-motor symptoms at 6 months, 10 and European single-center series have provided practical insights on tolerability and dose optimization.11,12 Practical initiation guidelines have been published to support implementation. 13
Despite these advances, no published data exist from the Middle East. Middle Eastern PD populations may exhibit distinct clinical profiles and genetic heterogeneity in Parkinsonisms in Gulf populations, which may influence treatment response and tolerability. 14 We report the first Middle Eastern experience with foslevodopa/foscarbidopa in 28 consecutive patients with advanced PD treated at Cleveland Clinic Abu Dhabi, a quaternary academic center in the United Arab Emirates.
Methods
Study design and setting
This retrospective observational cohort study (reported in accordance with the STROBE statement) analyzed consecutive patients with advanced PD initiated on foslevodopa/foscarbidopa between January 2025 and January 2026 at Cleveland Clinic Abu Dhabi, a quaternary academic medical center in the United Arab Emirates. The study was conducted as part of routine clinical care quality assessment and was approved by the Cleveland Clinic Abu Dhabi Institutional Review Board.
Patient selection
Patients were considered for foslevodopa/foscarbidopa if they met the following criteria: (1) diagnosis of idiopathic PD according to Movement Disorder Society criteria; (2) advanced disease with motor fluctuations inadequately controlled by optimized oral therapy; (3) preserved cognitive function sufficient for pump management or availability of capable caregivers; and (4) patient willingness and ability to manage continuous subcutaneous infusion. Cognitive capacity for device management was assessed as part of the standard clinical evaluation by the treating movement disorder neurologist, incorporating functional assessment of the patient’s ability to understand pump operation and cannula management, and the availability of a capable caregiver to assume these tasks where required. No formal cognitive scale was applied as a systematic inclusion criterion. Exclusion criteria included dementia precluding safe device management, active psychosis, and severe skin conditions contraindicating subcutaneous infusion. Among the 28 patients initiated, several had features making DBS less suitable or acceptable: 3 were explicitly hesitant about surgery; 4 were of advanced age; 2 had cognitive impairment; and 16 had prominent gait freezing, falls, postural instability, or severe balance impairment.
Inpatient titration protocol
All 28 patients underwent structured inpatient titration. Baseline assessments included complete medication history, levodopa equivalent daily dose (LEDD) calculation using the Tomlinson et al. 15 conversion factors, MDS-UPDRS Parts I–III, Hoehn and Yahr staging, patient diary recording of daily OFF and good ON hours, and non-motor symptom evaluation using the Non-Motor Symptoms Scale (NMSS). 16 The pump system used a programmable infusion device connected to a subcutaneous cannula placed in the abdominal wall. Initial infusion rates were calculated from baseline LEDD. Titration occurred over a median of 5 days (range 2–11) with adjustments based on motor response and tolerability. Upon discharge, patients received comprehensive training on pump operation, cannula site changes (typically every 1–3 days), troubleshooting, and 24-h support access. AbbVie-provided patient coaches offered home visits and ongoing support in the majority of cases.
Clinical assessments
Motor function was assessed using MDS-UPDRS Part III in the OFF state at baseline and in the ON state at follow-up on foslevodopa/foscarbidopa, reflecting routine clinical assessment practice. Patient diaries captured daily OFF hours, good ON hours (ON time without troublesome dyskinesia). Systematic diary recording of ON time with troublesome dyskinesia was not collected as a separate variable in this retrospective study. Hoehn and Yahr staging was performed at baseline and follow-up. Non-motor symptoms were evaluated using MDS-UPDRS Parts I and II and the NMSS, a 30-item clinician-administered scale covering nine domains (cardiovascular, sleep/fatigue, mood/cognition, perceptual problems, attention/memory, gastrointestinal, urinary, sexual function, and miscellaneous), scored on frequency × severity product per item. Follow-up assessments were performed at the first structured clinic visit after a stable dose was achieved (median follow-up from pump initiation: 9.0 months, interquartile range (IQR) 6.2–11.7, range 0.2–13.2 months). Non-motor assessments were not systematically administered at all visits during the early program phase; paired data were available for n = 11 (MDS-UPDRS Parts I and II) and n = 15 (NMSS).
Statistical analysis
Continuous variables are presented as mean ± standard deviation (SD) or median (IQR) as appropriate. Categorical variables are reported as counts and percentages. Paired comparisons between baseline and follow-up were performed using Wilcoxon signed-rank tests. For domain-level NMSS and MDS-UPDRS analyses, Benjamini–Hochberg false discovery rate (FDR) correction was applied; corrected q-values are reported alongside uncorrected p-values. These domain analyses are considered pre-specified exploratory secondary analyses. Statistical significance was defined as p < 0.05 (q < 0.05 for FDR-corrected analyses). Subgroup analyses compared patients who continued versus discontinued therapy. All statistical analyses were performed using Python (SciPy library, version 1.11).
Results
Patient characteristics
Twenty-eight consecutive patients with advanced PD underwent inpatient foslevodopa/foscarbidopa initiation (Table 1). Mean age was 61.3 ± 13.5 years (range 35–85), with 17 males (61%) and 11 females (39%). Mean disease duration was 10.1 ± 7.4 years (median 7.0, range 4–41 years). Motor phenotypes included tremor-dominant (n = 14, 50%), akinetic-rigidity dominant (n = 5, 18%), and postural instability and gait difficulty (n = 9, 32%), classified prospectively at clinical assessment. 17 Eight patients (29%) had prior exposure to another advanced therapy: three had undergone DBS; two had used LCIG; and five had used subcutaneous apomorphine rescue injections. Two patients had prior exposure to two modalities (DBS and apomorphine). Baseline mean LEDD was 1018 ± 574 mg/day (median 1197 mg, range 150–2400 mg).
Baseline demographic and clinical characteristics (N = 28).
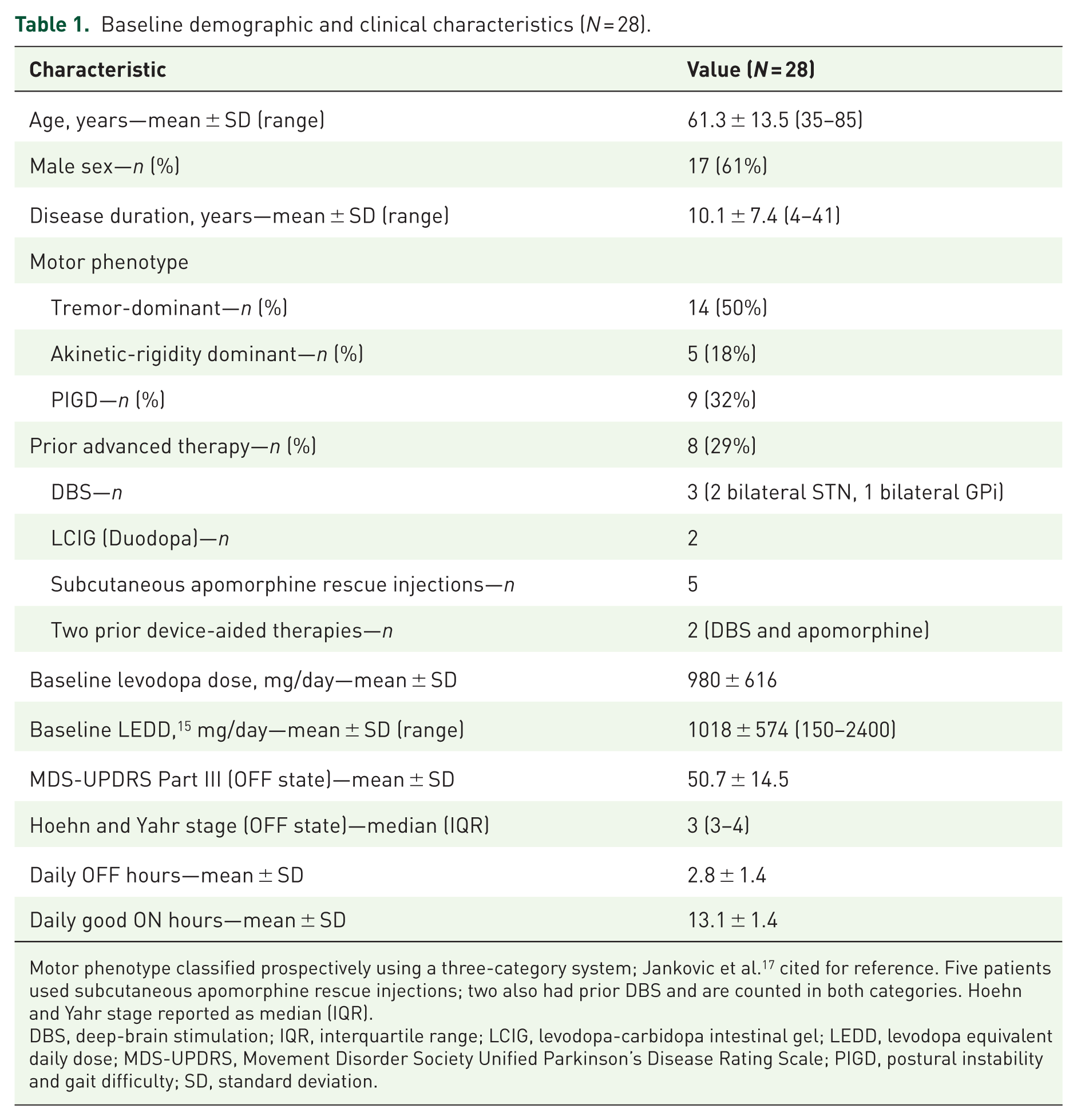
Motor phenotype classified prospectively using a three-category system; Jankovic et al. 17 cited for reference. Five patients used subcutaneous apomorphine rescue injections; two also had prior DBS and are counted in both categories. Hoehn and Yahr stage reported as median (IQR).
DBS, deep-brain stimulation; IQR, interquartile range; LCIG, levodopa-carbidopa intestinal gel; LEDD, levodopa equivalent daily dose; MDS-UPDRS, Movement Disorder Society Unified Parkinson’s Disease Rating Scale; PIGD, postural instability and gait difficulty; SD, standard deviation.
Infusion parameters, titration, and concomitant medications
Inpatient titration averaged 5.1 ± 2.2 days (Table 2). Initial pump base rates ranged from 0.15 to 0.51 mL/h (mean 0.30 ± 0.11 mL/h), with nighttime rates of 0.27 ± 0.10 mL/h. Discharge base rates were 0.37 ± 0.10 mL/h, reaching stable 1-month rates of 0.38 ± 0.10 mL/h. Cannula replacement intervals averaged 2 days. Follow-up pump-delivered LEDD equivalent was 1303 ± 362 mg/day (n = 24 with available rate data), representing a 28% increase from baseline LEDD. LEDD equivalence for foslevodopa/foscarbidopa was calculated using the manufacturer-specified conversion factor of 0.82, reflecting the specific bioavailability profile of the subcutaneous route. After initiation, 19 patients (68%) discontinued all oral levodopa-containing medications; 8 (29%) continued low-dose supplemental oral levodopa to reduce total infusion dose requirements, mainly because of cost-effectiveness considerations and insurance coverage limitations. Twelve patients were on a COMT inhibitor at baseline (11 on entacapone as part of a levodopa/carbidopa/entacapone combination, and 1 on opicapone); all 12 discontinued the COMT inhibitor at pump initiation. Dopamine agonists were present in 23 patients (82%) at baseline and continued post-initiation in 10 patients (36%), reflecting a degree of dopaminergic simplification while maintaining symptom control with continuous infusion therapy. Safinamide was used at baseline in 12 patients (43%); 2 continued post-initiation. Amantadine was used at baseline in 15 patients (54%); 6 continued post-initiation.
Infusion parameters and medication adjustments.
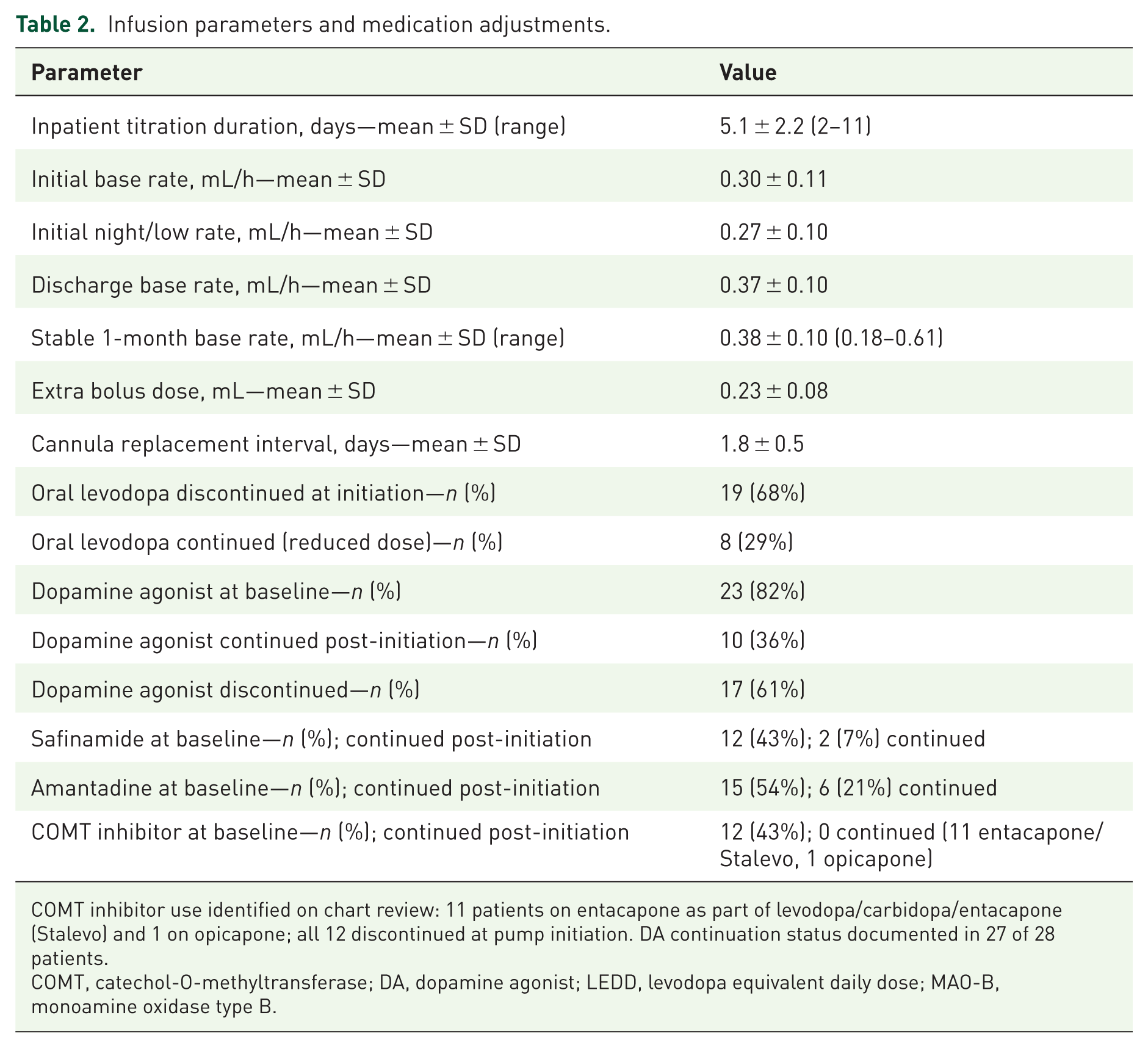
COMT inhibitor use identified on chart review: 11 patients on entacapone as part of levodopa/carbidopa/entacapone (Stalevo) and 1 on opicapone; all 12 discontinued at pump initiation. DA continuation status documented in 27 of 28 patients.
COMT, catechol-O-methyltransferase; DA, dopamine agonist; LEDD, levodopa equivalent daily dose; MAO-B, monoamine oxidase type B.
Motor outcomes
Motor outcomes are summarized in Table 3. MDS-UPDRS Part III in the OFF state at baseline was 50.7 ± 14.5, compared to 27.1 ± 13.6 in the ON state at follow-up (mean change −23.6 ± 8.3; p < 0.0001). This OFF → ON change reflects the functional gain, the difference between daily OFF-state disability and on-pump function, and not an incremental benefit above the baseline ON-state response. These results were consistent in the 22 continuers (mean change −24.4 ± 8.1; p < 0.0001).
Motor outcomes at follow-up (Wilcoxon signed-rank test).
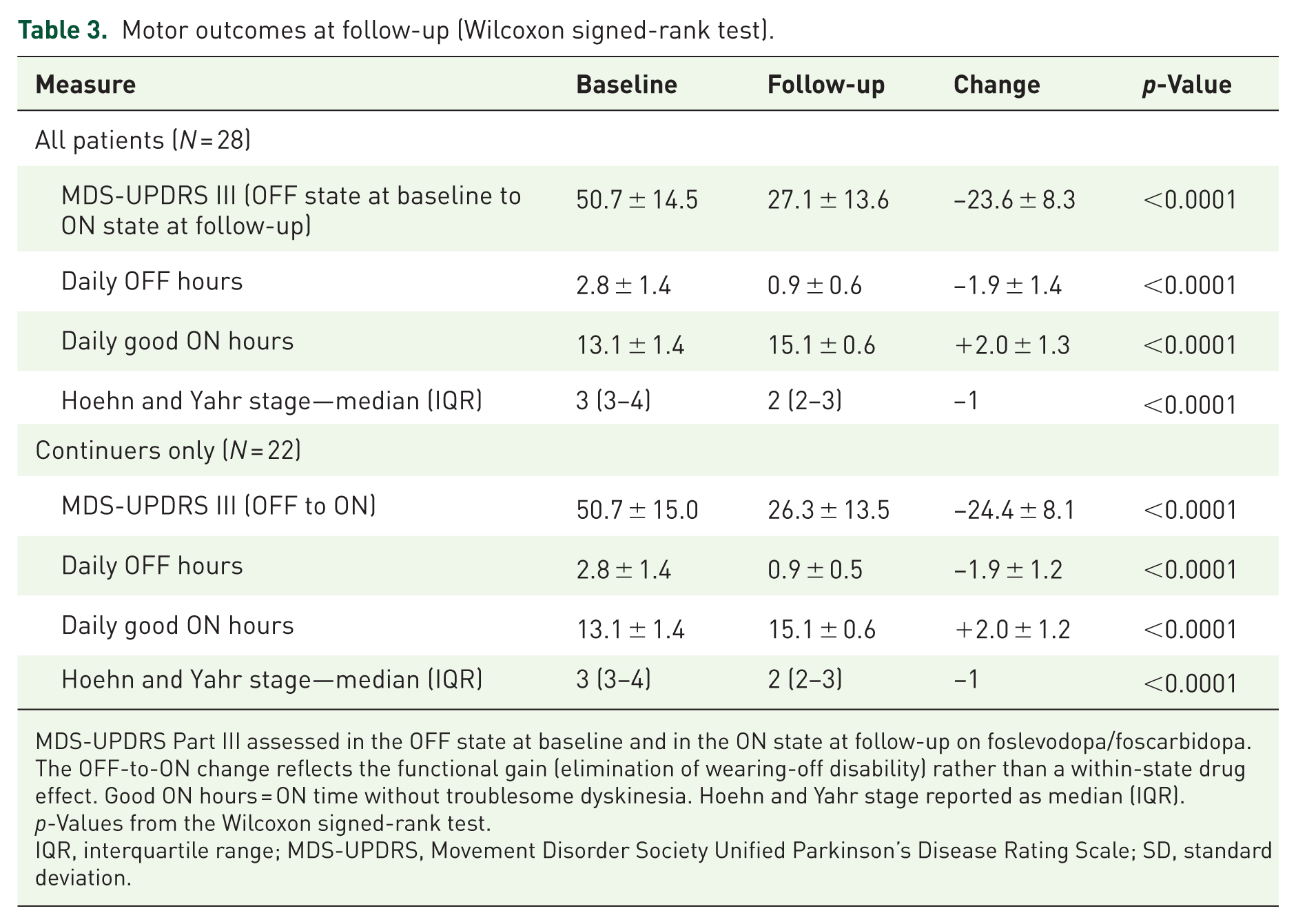
MDS-UPDRS Part III assessed in the OFF state at baseline and in the ON state at follow-up on foslevodopa/foscarbidopa. The OFF-to-ON change reflects the functional gain (elimination of wearing-off disability) rather than a within-state drug effect. Good ON hours = ON time without troublesome dyskinesia. Hoehn and Yahr stage reported as median (IQR). p-Values from the Wilcoxon signed-rank test.
IQR, interquartile range; MDS-UPDRS, Movement Disorder Society Unified Parkinson’s Disease Rating Scale; SD, standard deviation.
Daily OFF time reduced from 2.8 ± 1.4 to 0.9 ± 0.6 hours (mean reduction −1.9 ± 1.4 h; p < 0.0001). Good ON time increased from 13.1 ± 1.4 to 15.1 ± 0.6 h (mean gain +2.0 ± 1.3 h; p < 0.0001). No patient had troublesome dyskinesia documented as a clinical concern requiring management, consistent with a cohort where the primary indication was wearing-off disability. Hoehn and Yahr stage improved from median 3 (IQR 3–4) to 2 (IQR 2–3; p < 0.0001). A sensitivity analysis comparing patients with ⩾6 months (n = 21) versus <6 months of follow-up (n = 7) showed similar OFF-time reductions (−1.7 vs −2.0 h) and UPDRS III improvements (−22.7 vs −26.4 points), indicating results are not materially influenced by follow-up duration heterogeneity (Figures 1 –3).
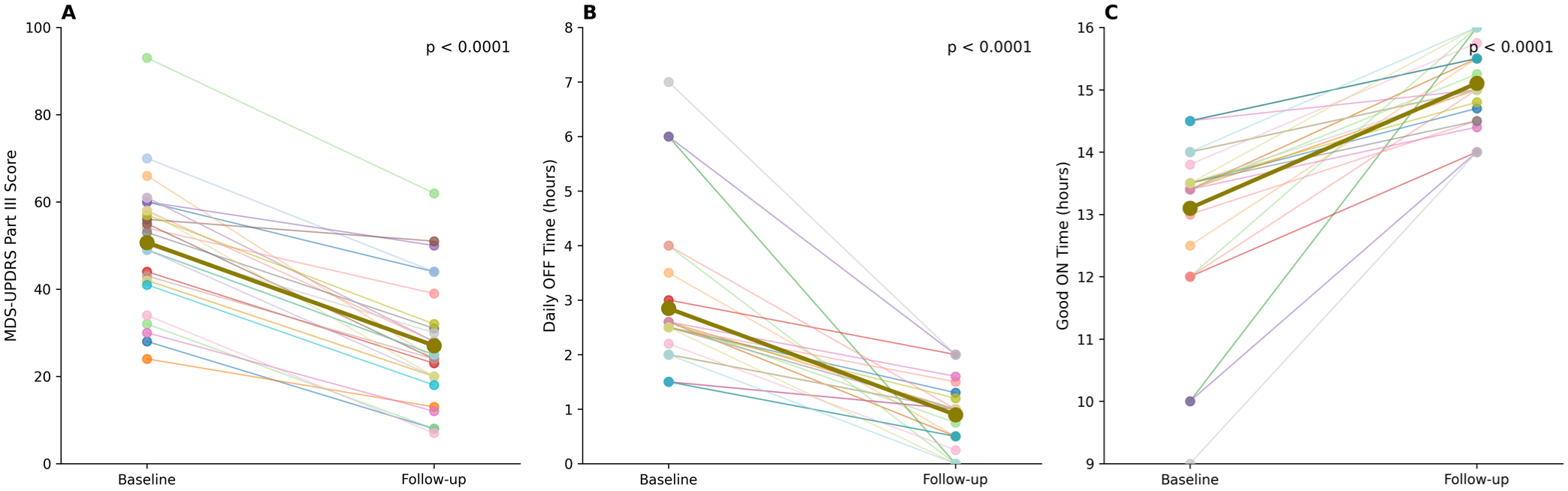
Motor outcomes following foslevodopa/foscarbidopa therapy. Individual patient trajectories and group mean (bold line) for (a) MDS-UPDRS Part III scores (OFF state at baseline; ON state at follow-up), (b) daily OFF time, and (c) good ON time from baseline to follow-up. p-Values from the Wilcoxon signed-rank test are shown above each panel.
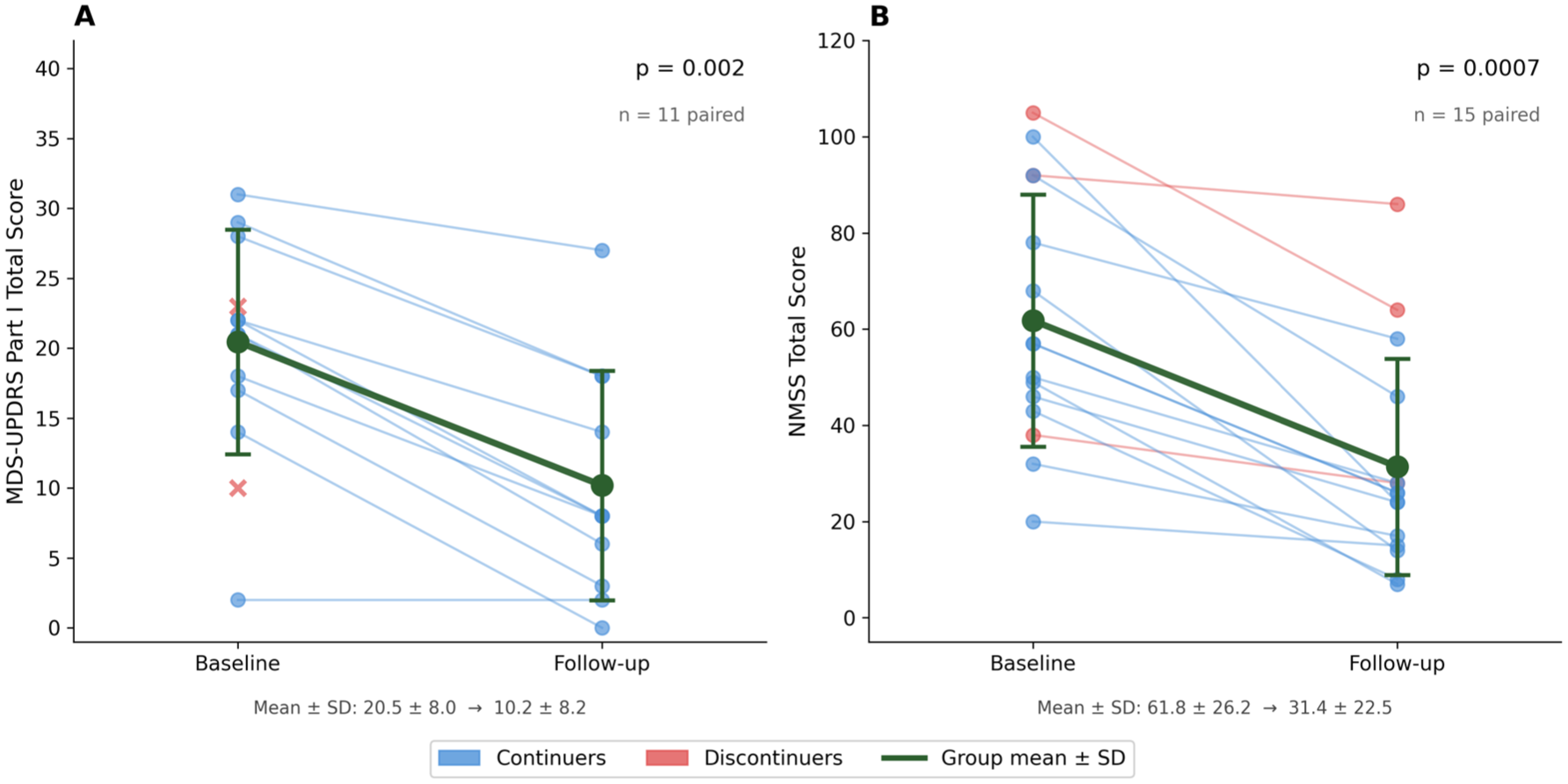
Non-motor symptom improvement following foslevodopa/foscarbidopa therapy. Individual patient trajectories and group mean (±SD) for (a) MDS-UPDRS Part I total score and (b) NMSS total score at baseline and follow-up.
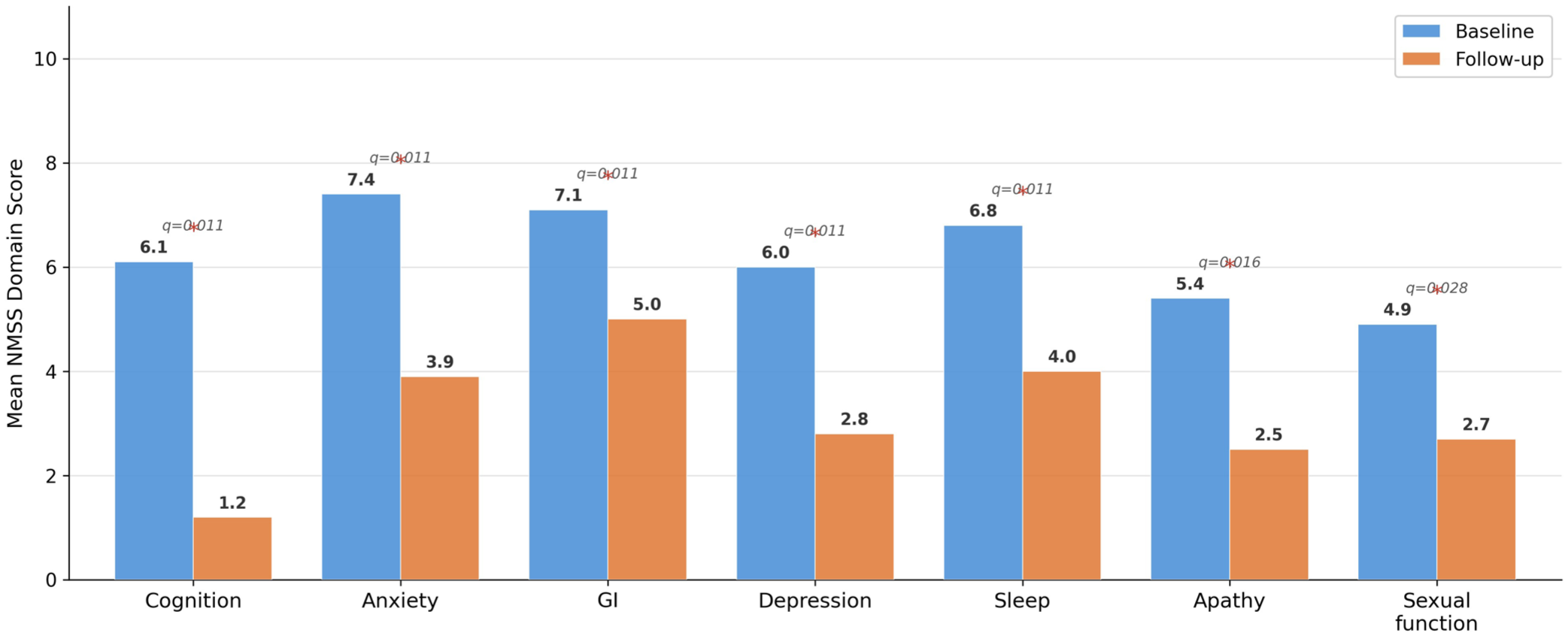
Domain-level improvement in NMSS. Mean NMSS domain scores at baseline (blue) and follow-up (orange) across seven statistically significant domains after FDR correction: cognition, anxiety, depression, GI symptoms, sleep, apathy, and sexual function. Asterisks denote FDR-corrected q < 0.05.
Non-motor outcomes
Non-motor outcomes are summarized in Table 4. MDS-UPDRS Parts I and II paired data were available for 11 patients. Part I (non-motor experiences of daily living) decreased from 20.5 ± 8.0 to 10.2 ± 8.2 (mean change −10.3 ± 4.7; p = 0.002). Part II (motor experiences of daily living) improved from 24.9 ± 13.2 to 12.5 ± 12.6 (mean change −12.5 ± 6.0; p = 0.001). Combined Parts I and II decreased from 45.4 ± 20.2 to 22.6 ± 19.8 (mean change −22.7 ± 9.3; p = 0.001).
Non-motor outcomes at follow-up (Wilcoxon signed-rank test).
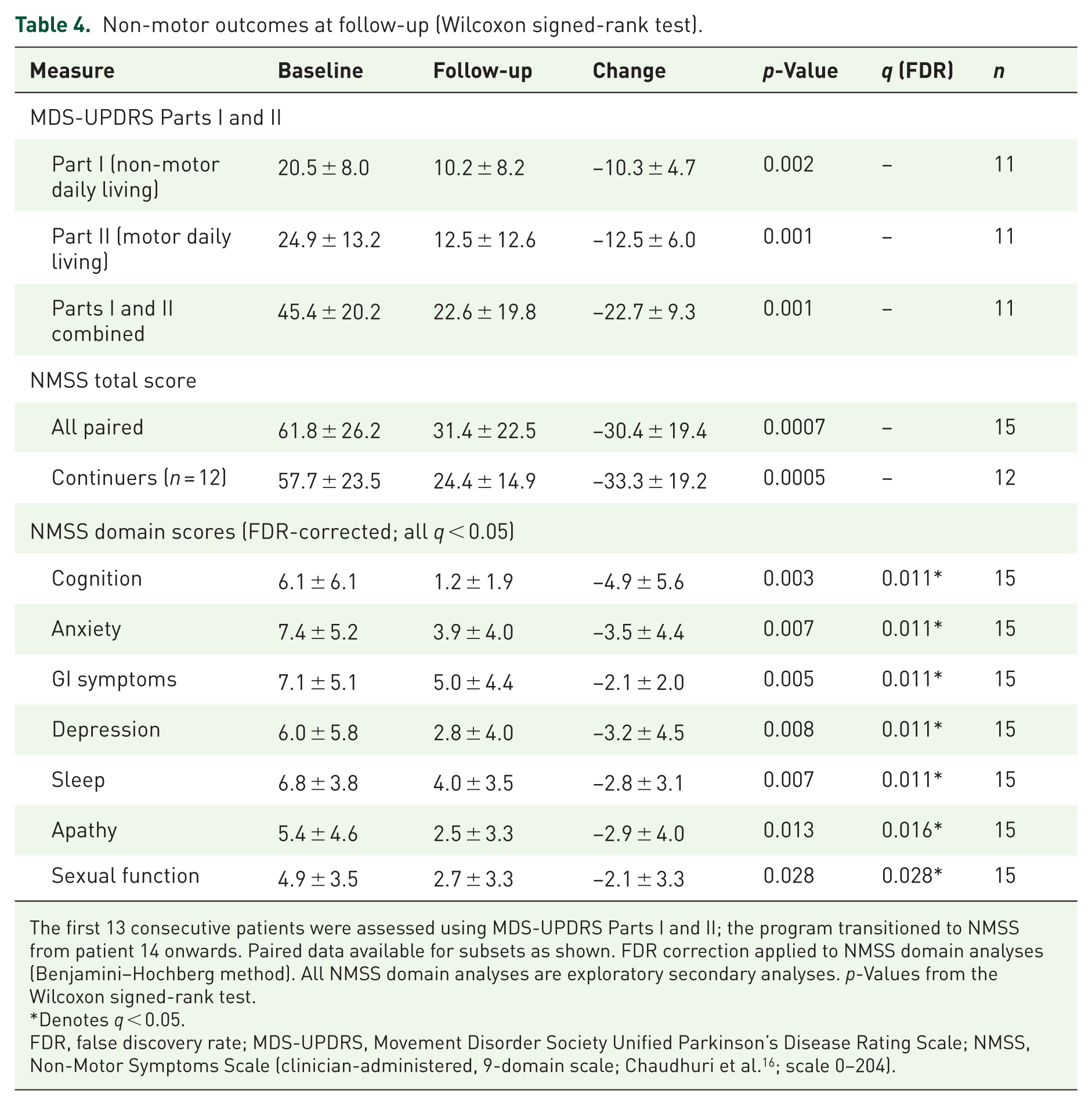
The first 13 consecutive patients were assessed using MDS-UPDRS Parts I and II; the program transitioned to NMSS from patient 14 onwards. Paired data available for subsets as shown. FDR correction applied to NMSS domain analyses (Benjamini–Hochberg method). All NMSS domain analyses are exploratory secondary analyses. p-Values from the Wilcoxon signed-rank test.
Denotes q < 0.05.
FDR, false discovery rate; MDS-UPDRS, Movement Disorder Society Unified Parkinson’s Disease Rating Scale; NMSS, Non-Motor Symptoms Scale (clinician-administered, 9-domain scale; Chaudhuri et al. 16 ; scale 0–204).
NMSS total scores were available for 15 patients with paired data. Baseline missing data were due to protocol evolution during the early program phase rather than selective non-completion; patients with and without paired NMSS data did not differ materially on age, LEDD, MDS-UPDRS III, or discontinuation rate. Mean NMSS scores decreased from 61.8 ± 26.2 to 31.4 ± 22.5 (mean change −30.4 ± 19.4; p = 0.0007), representing a 49% reduction in non-motor symptom burden. In the 13 continuers with paired data, improvement was −29.2 ± 19.7 points (p = 0.0002). After FDR correction, significant domain-specific improvements were observed in cognition (−4.9; q = 0.011), sleep (−2.8; q = 0.014), anxiety (−3.5; q = 0.014), GI symptoms (−2.1; q = 0.014), depression (−3.2; q = 0.014), apathy (−2.9; q = 0.020), and sexual function (−2.1; q = 0.036). These domain analyses are considered exploratory (Figures 2–3).
Safety, tolerability, and treatment discontinuation
Safety and treatment continuation outcomes are summarized in Tables 5 and 6. Infusion site adverse events (ISAEs) occurred in 22 of 28 patients (79%), with erythema, localized swelling, subcutaneous nodules (n = 18, 64%), and site bleeding. ISAEs were graded as mild (topical antiseptic only; n = 5, 18%), moderate (oral antibiotics required; n = 14, 50%), or severe (systemic antibiotics; n = 2, 7%). Seven patients (25%) developed infusion site cellulitis. No patient required hospitalization or intravenous antibiotics. All 22 ISAEs were resolved completely (100%). With appropriate site rotation (every 1–3 days) and patient education, the majority of ISAEs were managed without therapy discontinuation.
Safety and tolerability outcomes in 28 patients with advanced Parkinson’s disease treated with continuous subcutaneous foslevodopa/foscarbidopa.
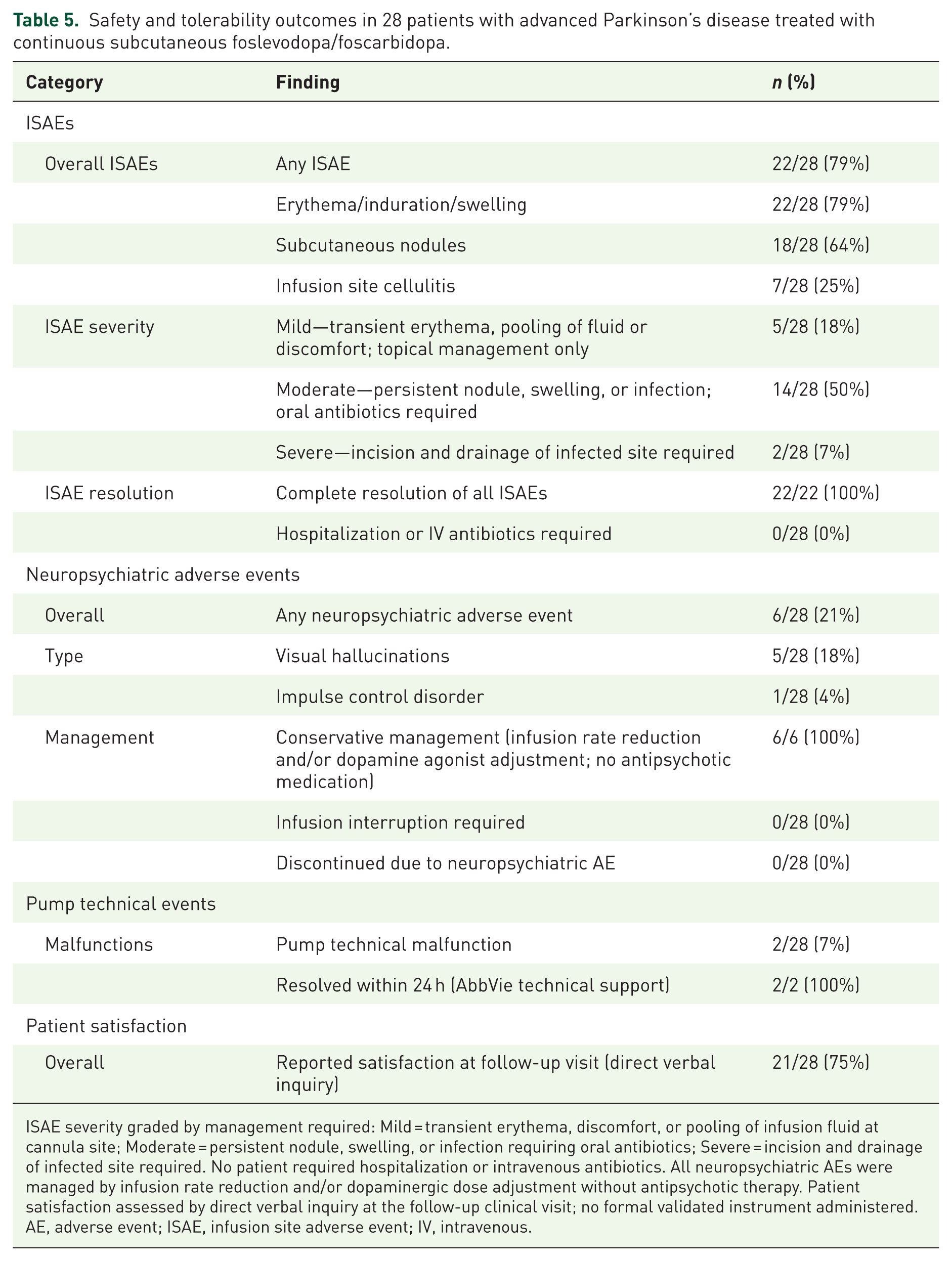
ISAE severity graded by management required: Mild = transient erythema, discomfort, or pooling of infusion fluid at cannula site; Moderate = persistent nodule, swelling, or infection requiring oral antibiotics; Severe = incision and drainage of infected site required. No patient required hospitalization or intravenous antibiotics. All neuropsychiatric AEs were managed by infusion rate reduction and/or dopaminergic dose adjustment without antipsychotic therapy. Patient satisfaction assessed by direct verbal inquiry at the follow-up clinical visit; no formal validated instrument administered.
AE, adverse event; ISAE, infusion site adverse event; IV, intravenous.
Treatment discontinuation outcomes in 28 patients with advanced Parkinson’s disease treated with continuous subcutaneous foslevodopa/foscarbidopa.
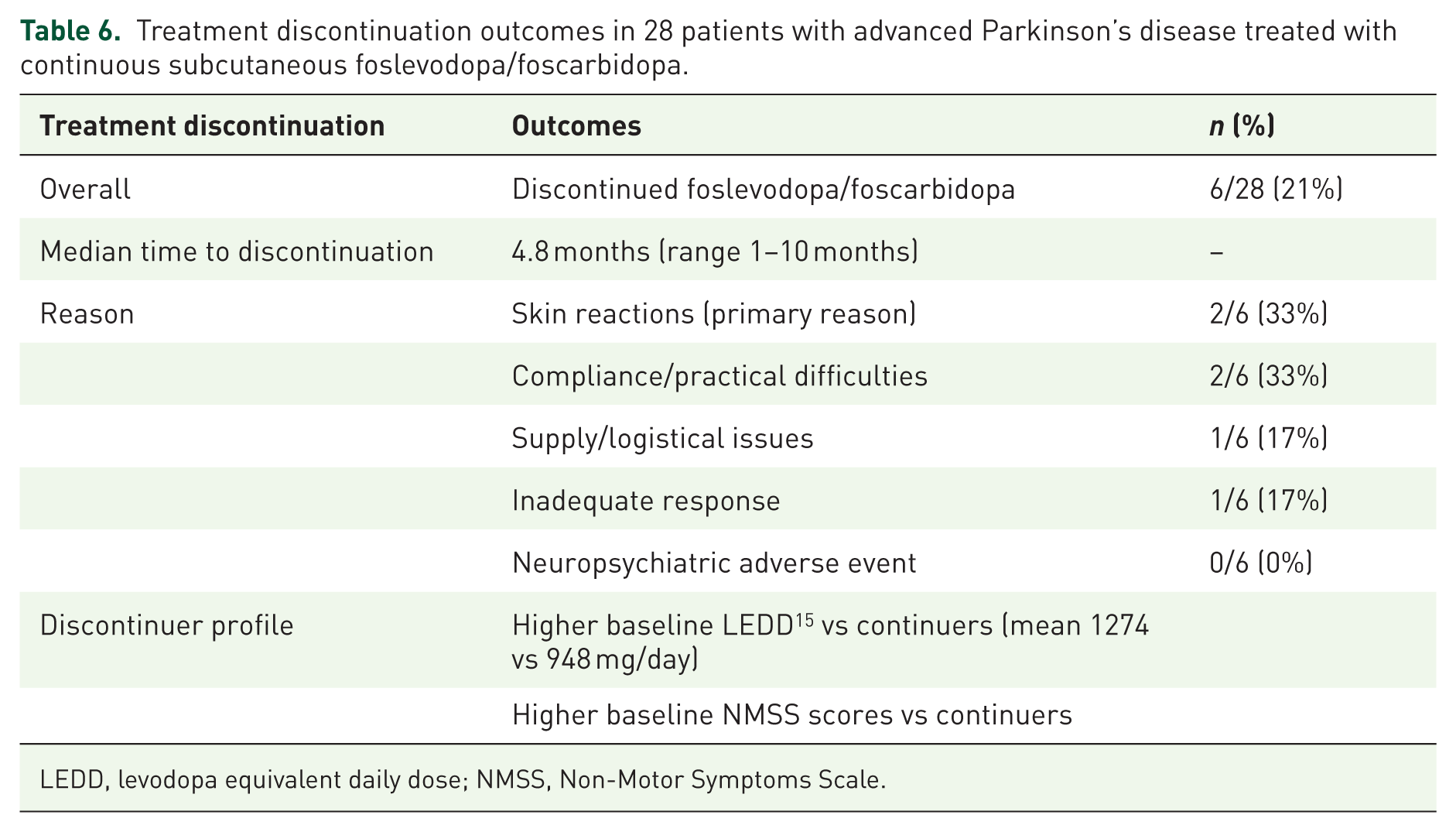
LEDD, levodopa equivalent daily dose; NMSS, Non-Motor Symptoms Scale.
Neuropsychiatric adverse events occurred in six patients (21%): visual hallucinations (n = 5, 18%) and impulse control disorder (n = 1, 4%). All were managed conservatively, with a reduction of the foslevodopa/foscarbidopa nocturnal infusion rate and/or dopaminergic dose adjustment in all cases. No patient required temporary infusion interruption or discontinued foslevodopa/foscarbidopa because of a neuropsychiatric adverse event. Pump technical malfunctions occurred in two patients (7%), both resolved within 24 h by the technical support team. Of 28 patients initiated, 21 (75%) reported satisfaction with therapy at follow-up. Patient satisfaction was assessed by direct verbal inquiry at the follow-up clinical visit, recorded as a binary yes/no response by the treating neurologist; no formal validated satisfaction instrument was administered.
Six patients (21%) discontinued foslevodopa/foscarbidopa over a median of 4.8 months (range 1–10 months; Table 6). Skin reactions were the primary reason in two patients (7% of all; 33% of discontinuations), compliance and practical issues in two, supply/logistical issues in one, and inadequate response in one. No discontinuation was because of a neuropsychiatric adverse event. Discontinuers had higher baseline LEDD (mean 1274 vs 948 mg/day) and higher NMSS baseline scores compared to continuers, suggesting more advanced disease at initiation. Among the 8 DAT-experienced patients, OFF-time reduction (−2.0 ± 1.6 h) was similar to that of DAT-naïve patients (−1.9 ± 1.3 h), though the small subgroup size precludes firm conclusions. Among DAT-experienced patients, five had prior subcutaneous apomorphine exposure and two had prior LCIG; dedicated real-world switch studies demonstrate that transitioning from apomorphine to foslevodopa/foscarbidopa is feasible and effective, 18 and that switching from LCIG is safe with modest symptomatic benefit, 19 consistent with outcomes in our DAT-experienced subgroup.
Discussion
This report presents the first real-world experience with continuous subcutaneous foslevodopa/foscarbidopa in the Middle East, demonstrating clinically meaningful reductions in motor fluctuations and non-motor symptom burden across a diverse advanced PD cohort at a quaternary academic center in the UAE.
Motor outcomes in context
The primary motor finding, a 65% reduction in daily OFF time (−1.9 h/day) and gain of 2.0 h in good ON time, is consistent with the pivotal M15-736 trial 8 and the ROSSINI real-world registry. 10 The OFF → ON UPDRS III change of −23.6 points represents the functional gain patients experience, the difference between daily OFF-state disability and stable on-pump function. As no formal levodopa challenge was performed in this real-world cohort, the OFF → ON change of −23.6 points reflects the total functional gain, the difference between the patient’s pre-treatment OFF-state disability and their on-pump ON-state function. This framing avoids overinterpretation as a classical within-state drug effect and is consistent with the approach used in published real-world foslevodopa/foscarbidopa series.20,21 The improvement in Hoehn and Yahr stage from median 3 to 2, consistent across continuers, is likely attributable to elimination of OFF-period postural instability rather than any disease-modifying effect. The absence of a control group and the observational design mean that regression to the mean and expectation effects cannot be fully excluded.
Non-motor outcomes
The approximately 48% reduction in NMSS total score (p = 0.0007), with significant FDR-corrected improvements across six domains including cognition, sleep, anxiety, GI symptoms, depression, and apathy, represents one of the more comprehensive non-motor datasets in a real-world foslevodopa/foscarbidopa series to date. These improvements likely reflect multiple concurrent mechanisms: continuous dopaminergic stimulation eliminates the peaks and troughs of oral pulsatile therapy, thereby reducing dopamine-related cognitive and mood fluctuations; improved nocturnal motor control enhances sleep quality; and reduced OFF-period pain, autonomic disturbance, and anxiety are direct consequences of fewer motor fluctuations. 22 The significant improvements in NMSS cognition and sleep are consistent with post hoc analyses of the phase III trial demonstrating benefits in these domains with continuous infusion. 23 These domain analyses are exploratory and hypothesis-generating; the paired data available for 15 of 28 patients introduce selection bias risk that limits generalizability.
Safety profile
The 79% ISAE rate is consistent with published clinical trial 8 and real-world data.11,12 Importantly, no patient required hospitalization or intravenous antibiotics; all ISAEs resolved completely, and skin reactions led to discontinuation in only two patients (7%). The neuropsychiatric AE rate of 21% is lower than the up to 47% reported by Desjardins et al. 24 in a similarly vulnerable real-world population, and lower than the up to 47% reported in other emerging series. 25 This likely reflects proactive dopaminergic simplification in our cohort specifically, discontinuation of COMT inhibitors at pump initiation in all 12 patients taking them, and tapering of dopamine agonists in 61% of patients. Desjardins et al. 24 identified COMT inhibitor use as a significant modifiable risk factor for neuropsychiatric and cognitive worsening (worsening group 70.6% vs stable group 21.1%; p = 0.006), consistent with our management approach. Importantly, Desjardins et al. 24 demonstrated that proactive clozapine use in patients with prior psychiatric histories enabled safe foslevodopa/foscarbidopa treatment in patients who would otherwise be considered high risk; a strategy not employed in our cohort but warranting prospective evaluation. 25 All neuropsychiatric events were managed conservatively through infusion rate reduction and/or dopaminergic dose adjustment, without antipsychotic therapy; none required foslevodopa/foscarbidopa discontinuation.
Discontinuation and patient selection
The 21% discontinuation rate mirrors pivotal trial 8 and European real-world data.11,26 Notably, at least three of the six discontinuations appear potentially modifiable through enhanced patient education and proactive skin monitoring. The breadth of clinical indications in our cohort, including DBS refusal, advanced age, cognitive comorbidity, and axial-dominant disease, reflects the real-world niche of foslevodopa/foscarbidopa as a genuinely non-surgical option for patients who cannot or will not undergo surgery. Cleveland Clinic Abu Dhabi was the first center and only center in the UAE to perform DBS and remains its highest-volume provider 27 ; foslevodopa/foscarbidopa fills an important complementary role for patients unsuitable for surgery.
Middle Eastern context
The UAE’s diverse patient population, including Emirati nationals and expatriates from Arab, South Asian, and other ethnic backgrounds, 28 did not demonstrate clinically apparent differences in outcomes across ethnic groups, though formal subgroup analyses were not performed, and this observation requires prospective validation. Healthcare delivery considerations unique to the region, extended family caregiving, and variable health literacy were navigated through a structured support infrastructure. As PD prevalence grows across the Gulf Cooperation Council, foslevodopa/foscarbidopa offers an accessible, non-surgical treatment pathway.
Limitations
This study has several important limitations. A key methodological limitation is that ON and OFF-state assessments during infusion therapy were not directly compared with corresponding ON and OFF-state assessments during prior oral medication therapy; the comparison of pre-infusion OFF-state scores with post-infusion ON-state scores may inherently magnify the observed treatment effect and should be interpreted accordingly. The retrospective design and absence of a control group limit causal inference; regression to the mean and expectation effects cannot be excluded. Follow-up duration was heterogeneous (median 9.0 months, range 0.2–13.2), though a sensitivity analysis showed consistent results by follow-up duration. Non-motor paired data were available for subsets only (n = 11 and n = 15); patients with and without paired data did not differ materially on key baseline characteristics, but selection bias cannot be fully excluded. The comparison of the OFF-state baseline to the ON-state follow-up MDS-UPDRS Part III reflects clinical practice but differs from within-state trial designs and should not be interpreted as a classical treatment effect. The small cohort (n = 28) limits subgroup analyses. Quality-of-life instruments (e.g., PDQ-39) were not systematically collected.
Conclusion
This first Middle Eastern real-world series of foslevodopa/foscarbidopa in advanced PD demonstrates clinically meaningful reductions in OFF time, motor severity, and non-motor symptom burden, with a safety and discontinuation profile consistent with global trial and real-world data. Infusion site reactions are common but manageable; the 79% continuation rate compares favorably with other DATs. These findings support foslevodopa/foscarbidopa as a valuable non-surgical treatment option for advanced PD, with implications for practice across the Middle East and globally.
Supplemental Material
sj-docx-1-tan-10.1177_17562864261464300 – Supplemental material for Real-world implementation of continuous subcutaneous foslevodopa/foscarbidopa in advanced Parkinson’s disease: first clinical experience from the Middle East
Supplemental material, sj-docx-1-tan-10.1177_17562864261464300 for Real-world implementation of continuous subcutaneous foslevodopa/foscarbidopa in advanced Parkinson’s disease: first clinical experience from the Middle East by Shivam Om Mittal, Kiran Waqar, Emma De Freitas, Yasmin Abdelmajid, Arshiya Anjum, Leanne Brown and Moncy Thomas in Therapeutic Advances in Neurological Disorders
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.