
Abstract
Background:
Transrectal ultrasound-guided prostate biopsy (TRUS-guided biopsy) remains widely used for the diagnosis of prostate cancer, but it is associated with a risk of infectious complications despite antibiotic prophylaxis.
Objectives:
To evaluate the effect of disinfecting the prostate biopsy needle with different antiseptic agents after each core sampling on post-procedural infectious complications.
Design:
A prospective, randomized, single-center clinical study.
Methods:
Between February and May 2025, 240 patients undergoing TRUS-guided prostate biopsy were randomly assigned to four groups (n = 60 each): no needle disinfection, povidone-iodine disinfection, 10% formalin disinfection, or 70% isopropyl alcohol disinfection after each biopsy core. All patients received standardized empirical antibiotic prophylaxis based on the institutional protocol and local antibiogram data. Prophylaxis consisted of oral cefixime initiated on the day of biopsy and continued for 5–7 days. Patients were actively followed for 30 days for febrile urinary tract infection, hospitalization, sepsis, and microbiological culture results.
Results:
The rate of febrile urinary tract infection was highest in the non-disinfection group (11.6%). No cases of fever, hospitalization, or sepsis were observed in the formalin group. Povidone-iodine and isopropyl alcohol disinfection were associated with lower infection rates than no disinfection, but were less effective than formalin. Escherichia coli was the most frequently isolated microorganism in positive cultures.
Conclusion:
Disinfection of the biopsy needle after each core sampling is associated with a meaningful reduction in infectious complications following TRUS-guided prostate biopsy. Among the evaluated agents, 10% formalin demonstrated the greatest protective effect; however, further multicenter studies with longer follow-up are required to confirm long-term safety and generalizability.
Trial registration:
This trial was prospectively registered at ClinicalTrials.gov (Identifier: NCT06836271; Local trial ID: HititUrology001).
Keywords
Introduction
Prostate cancer (PCa) is the second most frequently diagnosed malignancy among men worldwide. 1 In 2020, approximately 1.4 million new cases were reported globally, 2 with autopsy studies showing a comparable prevalence. 3 The risk of PCa increases after the age of 50, 4 and it is further elevated in men with a family history of PCa or those of African descent.5,6 The discovery of prostate-specific antigen (PSA) represented a major advancement in PCa diagnosis, and PSA remains the most widely used biomarker in clinical practice. 7 Initial suspicion of PCa is usually based on digital rectal examination (DRE) findings and elevated PSA levels.
Multiparametric magnetic resonance imaging (mpMRI) has become an essential step in the diagnostic pathway following PSA elevation. Randomized controlled trials have demonstrated that mpMRI reduces unnecessary biopsies while improving the detection of clinically significant PCa. Particularly in patients with PSA > 3 ng/mL, the Prostate Imaging Reporting and Data System (PI-RADS) optimizes detection of clinically significant cancers and reduces overdiagnosis of low-risk disease. 8 Despite these advances, histopathological confirmation through prostate biopsy remains the gold standard.9,10
Prostate biopsy can be performed either transperineally or transrectally. When performed by experienced urologists, transrectal ultrasound-guided prostate biopsy (TRUS-Bx) remains the standard approach. 11 However, because the procedure involves multiple needle passes through the rectum into the highly vascular prostate tissue, rectal flora may be introduced into the prostate, leading to postoperative infectious complications. Although generally well tolerated, TRUS-Bx can result in urinary tract infections, epididymo-orchitis, prostatitis, and, in rare cases, life-threatening urosepsis.12,13 Reported rates of dysuria are approximately 14%, urinary tract infection 10%, while more severe complications requiring hospitalization, such as sepsis and septic shock, occur in 5.7% and 0.45% of cases, respectively, with a mortality rate of 0.2%. 13 Recent studies have shown that urinary tract infection rates after TRUS-Bx range from 0.1% to 7%, sepsis from 0.1% to 1% (up to 3% in some series), and hospital admissions from 0.5% to 2%, with mortality remaining extremely rare.13,14 By contrast, large meta-analyses have demonstrated that infection and sepsis rates after transperineal prostate biopsy are typically below 0.5%, indicating that this approach is a safer alternative with respect to infectious complications.15,16 Nevertheless, although recent European Association of Urology (EAU) guidelines recommend the transperineal approach, the transrectal route continues to be widely used in many centers, including ours, due to its shorter procedure time, minimal anesthesia requirements, lower cost, and limited availability of equipment for the transperineal technique. 17
Both the EAU and the American Urological Association recommend appropriate antibiotic prophylaxis before TRUS-Bx to reduce infectious complications. In countries where fluoroquinolones are restricted, fosfomycin or augmented prophylactic regimens are viable alternatives, although no standardized combination has been established. 18 Several strategies have been explored to further reduce infectious complications, including rectal swab cultures to guide prophylaxis, needle disinfection with agents such as formalin or chlorhexidine, and the use of transperineal biopsy as an alternative.19,20 While diagnostic yields between transperineal and transrectal approaches are comparable, 21 transperineal biopsy has been shown to significantly reduce infectious complications. 16 However, longer procedure times and the need for specialized equipment limit its widespread use.
Current preventive strategies typically combine systemic antibiotics and local antiseptics. Povidone-iodine and chlorhexidine are widely used antiseptics, while fluoroquinolones, particularly ciprofloxacin, have traditionally been the cornerstone of antibiotic prophylaxis. Increasing antibiotic resistance has prompted the exploration of alternative regimens, including third-generation cephalosporins such as cefpodoxime.22,23 Despite these approaches, the optimal prophylactic regimen remains a matter of debate, and the influence of local resistance patterns on efficacy is not fully understood.
This study aimed to prospectively compare the effectiveness of biopsy needle disinfection using povidone-iodine, isopropyl alcohol, or formalin after each puncture with the standard approach without disinfection, to determine the most effective method to reduce infectious complications following TRUS-Bx.
Materials and methods
Study design and ethical approval
This prospective, randomized, single-center study was conducted at the Department of Urology, Hitit University, between February 2025 and May 2025. The study protocol was approved by the Hitit University Clinical Research Ethics Committee (Approval No: 2024-58; Approval date: August 14, 2024). Written informed consent was obtained from all participants prior to enrollment. The study was conducted in accordance with the Declaration of Helsinki and relevant national regulations.
Patient selection
Between February and May 2025, 240 patients scheduled to undergo TRUS-Bx due to elevated PSA levels (>2.5 ng/mL) and/or suspicious findings on DRE were enrolled. Benign prostatic hyperplasia (BPH) was not an inclusion criterion; BPH status was recorded only as a baseline characteristic. Eligible patients were oriented, cooperative, without an active urinary tract infection (UTI), and with normal coagulation parameters. Exclusion criteria included untreated UTI, known allergy to povidone-iodine, ongoing immunosuppressive therapy, antibiotic treatment for UTI within the past 10 days, prostate biopsy within the past 3 months, planned saturation biopsy, and presence of an indwelling urinary catheter.
Randomization and groups
Patients were randomly assigned to four groups (n = 60 each):
Group 1: No needle disinfection (control)
Group 2: Povidone-iodine disinfection after each core
Group 3: 10% formalin disinfection after each core
Group 4: 70% isopropyl alcohol disinfection after each core
Participants were randomized in a 1:1:1:1 ratio using a computer-generated permuted-block sequence (block sizes of 4 and 8, randomly varied) to maintain equal allocation across the four groups. Allocation concealment was ensured with sequentially numbered, opaque, sealed envelopes.
Procedure
Rectal preparation was performed in all patients with a cleansing enema followed by povidone-iodine rectal cleansing. All biopsies were performed by the same experienced urologist. Twelve-core biopsies were obtained from the base, mid-gland, and apex of both prostate lobes using an 18-gauge side-cutting needle under transrectal ultrasound guidance.
Periprostatic local anesthesia was administered with 10 mL of prilocaine hydrochloride at two standard sites in each patient. Prostate volume was measured by transrectal ultrasound and calculated using the prolate ellipsoid formula (volume = 0.52 × length × height × width).
All patients received standard empirical antibiotic prophylaxis based on our institutional protocol and local antibiogram data. Given the increasing prevalence of fluoroquinolone-resistant Escherichia coli in rectal flora, fluoroquinolones were not routinely used. Therefore, prophylaxis consisted of oral cefixime 400 mg once daily, initiated on the day of the procedure and continued for 5–7 days. Rectal swab–guided targeted prophylaxis was not routinely performed.
After each core, the biopsy needle was managed according to the randomized arm (no disinfection, povidone-iodine, 10% formalin, or 70% isopropyl alcohol) using a standardized procedure. In the formalin arm, disinfection was immediately and mandatorily followed by copious rinsing with sterile normal saline, flushing the needle lumen, and wiping the outer shaft with saline-moistened sterile gauze to minimize residual formaldehyde exposure. This rinsing step was performed uniformly for all participants in the formalin group.
Post-procedural follow-up
Patients were contacted daily by telephone during the first postoperative week and assessed for fever, hematuria, hematospermia, rectal bleeding, and lower urinary tract symptoms. Outpatient follow-up was scheduled on postoperative day 14 to assess infectious and non-infectious complications. At 30 days, an additional telephone follow-up was conducted.
Patients who developed fever >37.8°C with urinary symptoms were classified as febrile UTI and hospitalized. In patients with suspected febrile urinary tract infection, urine and blood cultures were obtained before initiation of empirical antibiotic therapy whenever clinically feasible. The diagnosis of febrile UTI was based on the presence of fever accompanied by urinary symptoms, supported by laboratory and microbiological findings when available. Laboratory investigations included complete blood count, renal and liver function tests, urinalysis, urine and blood cultures, C-reactive protein (CRP), and procalcitonin levels. Sepsis was defined according to the American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference criteria, requiring at least two systemic inflammatory response syndrome (SIRS) criteria. At the time of study design, this definition was used, and the study was not powered to detect differences in sepsis rates between groups; therefore, febrile urinary tract infection was selected as the primary outcome. Patients with sepsis were admitted to the intensive care unit (ICU) and managed in consultation with infectious disease specialists.
Data collection
The following data were recorded: patient demographics, comorbidities (diabetes mellitus, hypertension, coronary artery disease), medication use (anticoagulants/antiplatelets), PSA (total and free), prostate volume, and pathology results. Patients diagnosed with atypical small acinar proliferation or high-grade prostatic intraepithelial neoplasia in more than three cores were scheduled for re-biopsy.
Statistical analysis
All data were tested for normality using the Kolmogorov–Smirnov test and found to be normally distributed. Continuous variables were expressed as mean ± standard deviation (SD). Comparisons among the four groups were performed using one-way ANOVA, followed by Duncan or Games–Howell post hoc tests depending on variance homogeneity. Categorical variables were analyzed using Fisher’s exact test. The sample size was calculated using a power analysis with a significance level (α) of 0.05 and power (1 − β) of 80%, indicating that at least 57 patients per group were required to detect a clinically significant difference in infection rates. To account for potential dropouts, 60 patients were included in each group. A p value < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS for Windows version 24.0 (IBM Corp., Armonk, NY, USA).
This randomized controlled trial was reported in accordance with the CONSORT guidelines, and the patient selection process is illustrated in the CONSORT flow diagram (Supplemental Material; Figure 1).
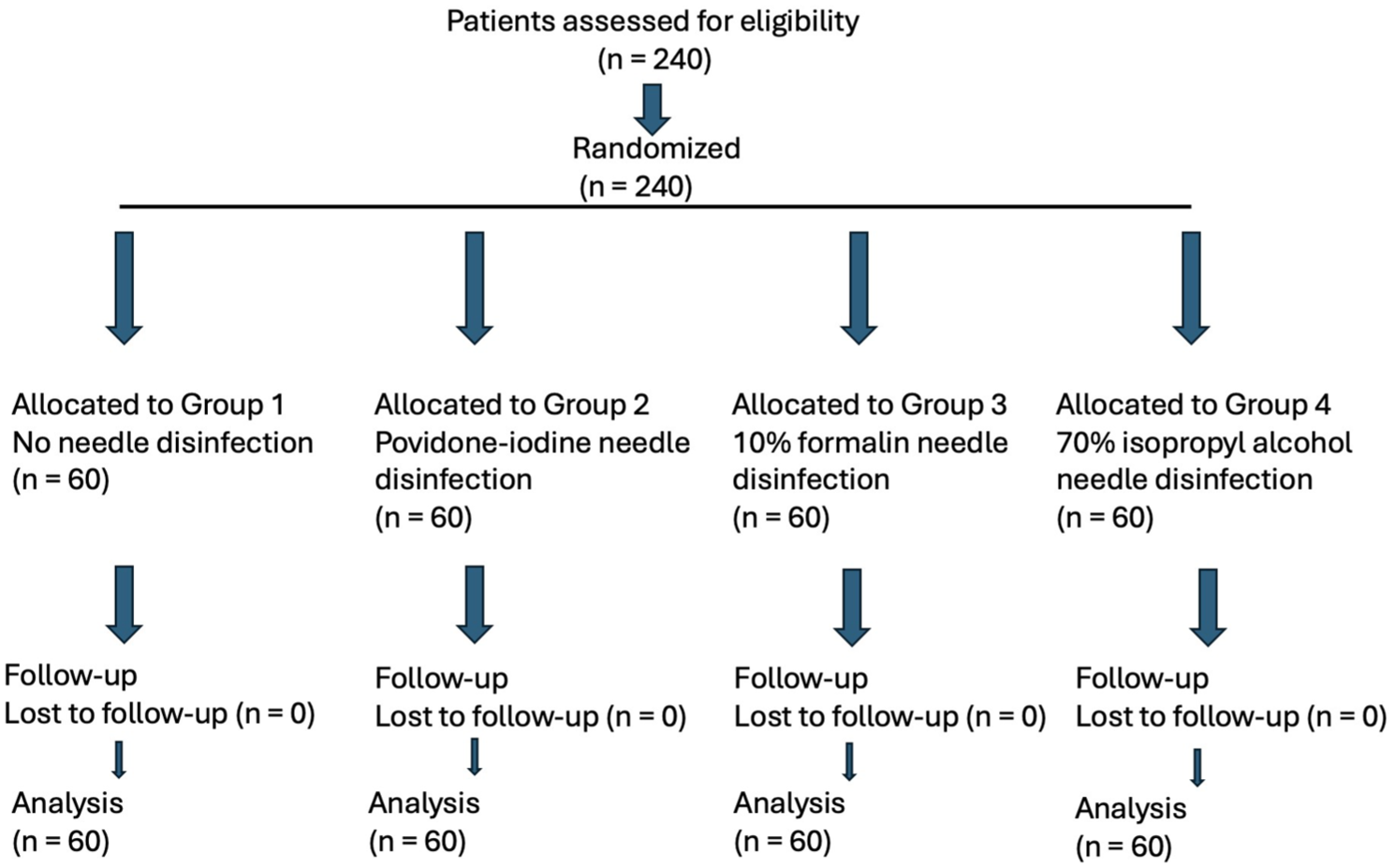
CONSORT flow diagram of participant randomization, allocation, follow-up, and analysis in the four-arm trial (n = 240).
Results
A total of 240 patients who underwent TRUS-Bx were included in the final analysis. The mean age was 65.8 ± 7.3 years (range: 35–86), the mean BMI was 27.2 ± 4.9 kg/m2, the mean PSA value was 5.9 ± 2.4 ng/mL, and the mean prostate volume was 59.5 ± 11.7 cc. Comorbidities included hypertension in 36%, diabetes mellitus in 25.8%, and coronary artery disease in 17.2% of patients. There were no statistically significant differences among the four groups in baseline characteristics such as age, BMI, prostate volume, PSA levels, or comorbidities (Table 1).
Baseline characteristics of patients according to groups.
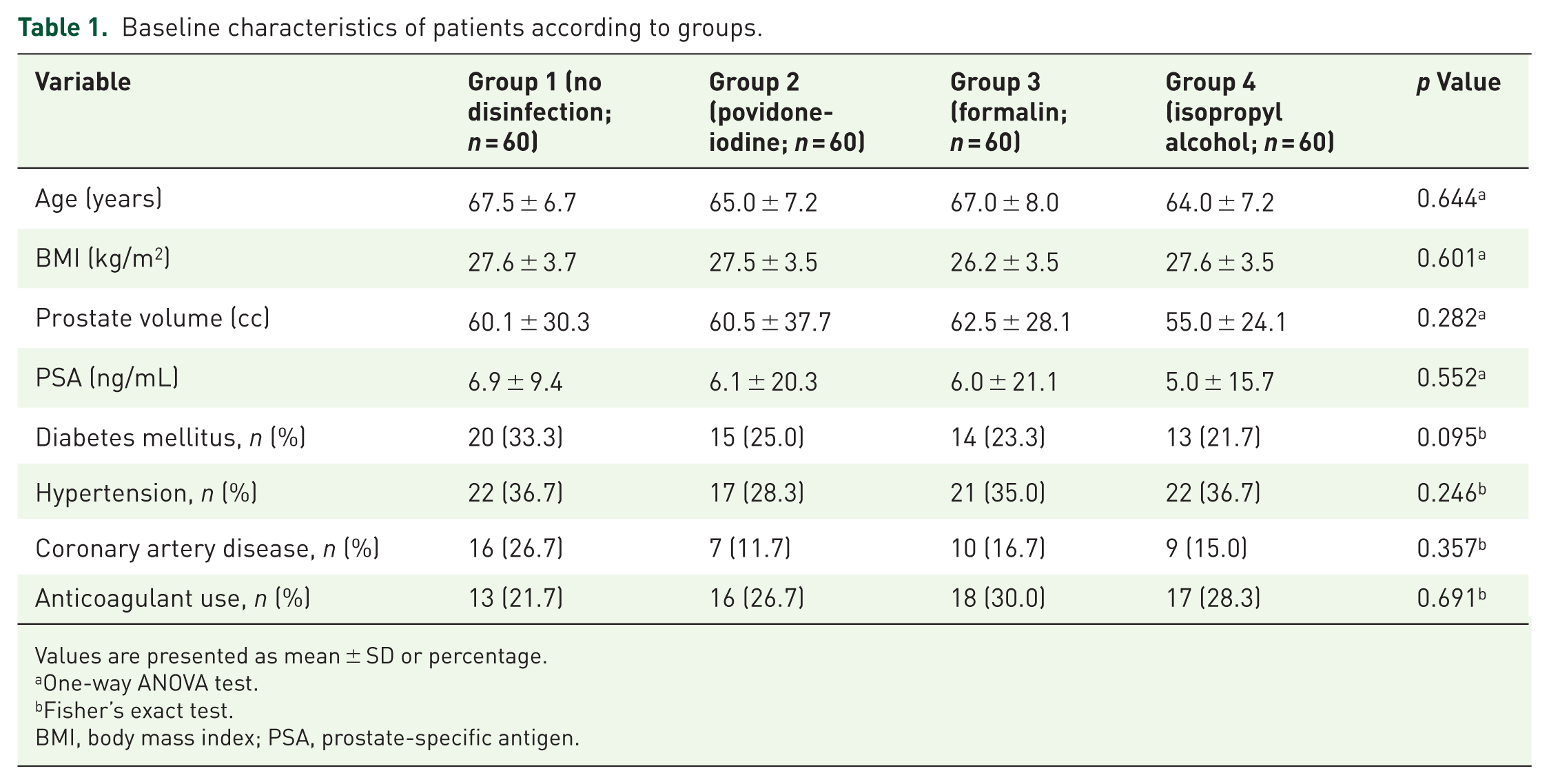
Values are presented as mean ± SD or percentage.
One-way ANOVA test.
Fisher’s exact test.
BMI, body mass index; PSA, prostate-specific antigen.
Infectious complications
Fever was observed in seven patients (11.6%) in Group 1, three patients (5.0%) in Group 2, and four patients (6.6%) in Group 4, whereas no cases were reported in Group 3. The difference was statistically significant between Group 1 and Group 3 (p = 0.036). Fever duration was also significantly shorter in Group 3 than in Group 1 (p = 0.029). All patients were actively followed with scheduled outpatient visits and daily telephone contact during the first postoperative week, allowing for systematic detection of febrile urinary tract infections.
Hospitalization was required in six patients (10.0%) in Group 1, one patient (1.6%) in Group 2, and three patients (5.0%) in Group 4, while no patient in Group 3 required hospitalization. The difference between Group 1 and Group 3 was statistically significant (p = 0.025). Intravenous antibiotic therapy was administered to seven patients (11.6%) in Group 1, two patients (3.3%) in Group 2, and three patients (5.0%) in Group 4, while none of the patients in Group 3 required treatment (p < 0.001).
Sepsis occurred in two patients (3.3%) in Group 1 and in one patient (1.6%) in Group 4. No cases of sepsis were observed in Groups 2 or 3. The difference among groups was not statistically significant (p = 0.158). ICU admission was required for two patients (3.3%) in Group 1 and one patient (1.6%) in Group 4, while no ICU admission occurred in Groups 2 and 3 (p = 0.158).
Positive urine cultures were detected in six patients (10.0%) in Group 1 and in one patient (1.6%) in Group 2, whereas no positive cultures were observed in Groups 3 and 4. The difference between Group 1 and Groups 3–4 was statistically significant (p = 0.045). Blood culture positivity was found in two patients (3.3%) in Group 1 and one patient (1.6%) in Group 2, while none of the patients in Groups 3 and 4 had positive blood cultures (p = 0.281). The most frequently isolated microorganism was Escherichia coli (85.7%). Approximately 40% of E. coli isolates were resistant to first-line empirical antibiotics, whereas all isolates were sensitive to carbapenems and third-generation cephalosporins (Table 2).
Infectious outcomes among groups.
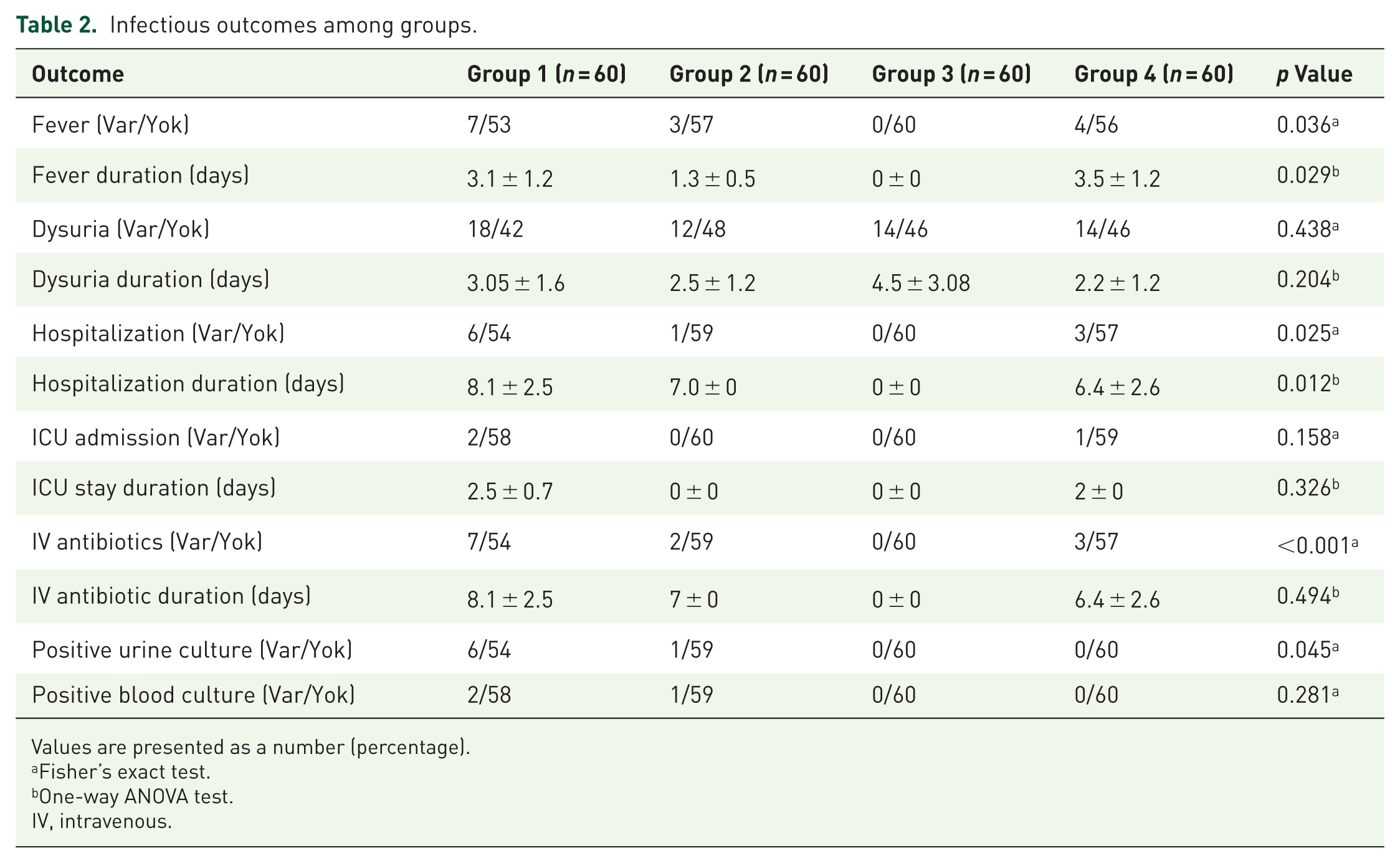
Values are presented as a number (percentage).
Fisher’s exact test.
One-way ANOVA test.
IV, intravenous.
Non-infectious complications were mild and self-limited. Transient hematuria and hematospermia were observed across all groups and resolved spontaneously without the need for intervention. No patient required urinary catheterization due to acute urinary retention, and no clinically significant rectal bleeding or chemical irritation attributable to needle disinfection was observed in any group.
Discussion
TRUS-Bx remains the most widely used method for diagnosing PCa. However, this procedure can lead to significant infectious complications due to the introduction of rectal flora into the prostate via repeated needle insertions. 24 Despite antibiotic prophylaxis, the increasing prevalence of antimicrobial resistance continues to pose a major challenge in reducing post-biopsy sepsis and hospitalization rates. 14 Consequently, local antiseptic measures have gained increasing importance.
The relatively high rate of febrile urinary tract infection observed in the control group warrants careful interpretation. All patients in this study were actively monitored with scheduled outpatient visits and daily telephone contact during the first postoperative week, which may have increased the overall detection of infectious events compared with studies relying on passive reporting. Importantly, this active surveillance was applied uniformly across all study groups and therefore does not account for the higher infection rate observed exclusively in the non-disinfection group. A more plausible explanation is the cumulative bacterial inoculation associated with repeated needle passages through the rectal mucosa when no disinfection is performed. By contrast, antiseptic needle disinfection after each core likely reduced bacterial load and prevented progressive contamination, thereby mitigating the clinical impact of local antimicrobial resistance despite identical systemic antibiotic prophylaxis.
Our study is one of the few prospective, randomized trials directly comparing needle disinfection methods for their impact on infectious complications after TRUS-Bx. The findings showed that 10% formalin disinfection was particularly effective, with no cases of fever, hospitalization, or sepsis in that arm. These results are consistent with Singla et al., 25 who reported significantly lower infection rates with formalin needle disinfection.
The use of formalin as a needle disinfectant raises understandable concerns regarding potential toxicity and carcinogenicity. In the present study, a 10% formalin solution was applied with very brief contact after each biopsy core, followed by mandatory and thorough rinsing of both the needle lumen and external surface with sterile normal saline. No clinically evident rectal irritation, chemical injury, or procedure-related adverse effects attributable to formalin exposure were observed. Although residual exposure cannot be completely excluded, meticulous saline rinsing is considered effective in minimizing direct mucosal contact. Nevertheless, the absence of long-term follow-up data regarding repeated formalin exposure should be acknowledged as an important limitation. 26
Distinguishing between febrile urinary tract infection and sepsis is essential when interpreting infectious outcomes after TRUS-guided prostate biopsy. While sepsis represents a severe but relatively infrequent complication, febrile UTI occurs more commonly and more accurately reflects the overall infectious burden of the procedure. Accordingly, febrile UTI was selected as the primary outcome of the present study, as the sample size was not powered to detect statistically meaningful differences in sepsis rates. This approach allows a more sensitive evaluation of preventive strategies aimed at reducing clinically relevant post-biopsy infections.
Povidone-iodine has long been used in rectal preparation to reduce bacterial load prior to TRUS-Bx. Previous studies and a recent meta-analysis demonstrated that rectal povidone-iodine irrigation effectively decreases minor complications such as fever and urinary tract infection, although it appears less effective in preventing severe infections such as sepsis. 27 In our study, povidone-iodine needle disinfection significantly reduced infection rates compared with the control group but was less effective than formalin.
Isopropyl alcohol is another well-established antiseptic with broad bactericidal properties. In our cohort, its use was associated with a reduction in fever and positive urine culture rates, with no cases of sepsis observed. This finding aligns with a 2024 validation study that confirmed the effectiveness of alcohol needle washing in reducing sepsis rates after TRUS-Bx. 28
Limitations
This study has several limitations that should be acknowledged. First, the single-center design may limit the generalizability of the findings. Second, although no clinically evident adverse effects related to formalin exposure were observed, the lack of long-term follow-up precludes definitive conclusions regarding the safety of repeated formalin use. Third, rectal swab–guided targeted antibiotic prophylaxis was not performed, and antibiotic selection was based on the institutional antibiogram rather than individual culture results. Finally, other antiseptic agents with prolonged mucosal activity, such as chlorhexidine, were not evaluated. Future multicenter studies with larger sample sizes and longer follow-up are warranted to validate these findings and to further refine preventive strategies for infectious complications after TRUS-guided prostate biopsy.
Conclusion
This prospective randomized study demonstrates that disinfection of the prostate biopsy needle after each core sampling is associated with a meaningful reduction in infectious complications following TRUS-guided prostate biopsy. Among the evaluated antiseptic agents, 10% formalin showed the most pronounced protective effect, while povidone-iodine and isopropyl alcohol provided partial benefit compared with no disinfection. Although the findings suggest that routine needle disinfection may enhance patient safety when TRUS-guided biopsy is performed, particularly in settings with increasing antimicrobial resistance, caution is warranted regarding the long-term safety of repeated formalin exposure. Larger multicenter studies with extended follow-up are needed to confirm these results and to better define the optimal role of needle disinfection strategies in contemporary prostate biopsy practice.
Supplemental Material
sj-docx-1-tau-10.1177_17562872261458100 – Supplemental material for Effect of needle disinfection with different antiseptic agents on infectious complications after TRUS-guided prostate biopsy: a prospective randomized study
Supplemental material, sj-docx-1-tau-10.1177_17562872261458100 for Effect of needle disinfection with different antiseptic agents on infectious complications after TRUS-guided prostate biopsy: a prospective randomized study by Mustafa Serdar Çağlayan, Mustafa Kestel, Musa Ekici, Cemil Aydin, Muhammet İhsan Öztürk, Ahmet Taşcı and Mehmet Murat Baykam in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.