
Abstract
This paper reflects upon the development of an interprofessional education project and the learning derived from the pilot event, which focused upon interprofessional learning in action and its potential to enable collaborative working to reduce avoidable healthcare associated infections in an acute NHS foundation trust.
Keywords
Introduction
Healthcare associated infections (HCAIs) remain high on the political agenda and our trust had an ambition to develop an interprofessional learning (IPL) project focused upon reducing avoidable HCAIs (the terms ‘interprofessional learning’ and ‘interprofessional education’ (IPE) are used interchangeably). Funding for a two year project was secured, with a requirement for the project to be developed and formally evaluated through an action research study to provide evidence of outcomes and the impact of IPL in an acute hospital setting (Reeves et al, 2008).
The project specifically sought to improve communication and understanding of roles within multidisciplinary healthcare teams by bringing different professions together to promote learning and collaborative team working in support of the trust’s multi-professional action plan to reduce avoidable HCAIs. The IPL programme was designed to reinforce infection prevention and control (IPC) policies, to deliver key messages and to focus on the behaviours and practices of healthcare teams.
Critical to the project’s success was the preparation of a team of IPL facilitators and development of a pilot event adopting an action research approach, to inform the trust’s future IPL programme (Carr and Kemmis, 1986) (Figure 1).
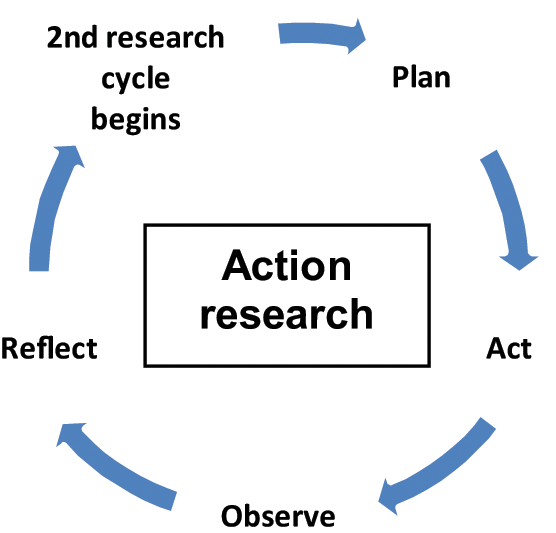
Action research cycle (Carr and Kemmis (1986))
The pilot event, named ‘The Patient’s Journey’, centred upon our fictitious patient ‘Mr Brown’ following his passage from admission to discharge, his exposure to multidisciplinary healthcare staff and his experience of HCAI in an acute healthcare setting.
IPL in the National Health Service
Although IPL has existed for over 40 years, national strategies were not established within education until the late 1990s. Initially these involved post-qualifying work-based events, followed by university-based postgraduate courses and later by qualifying initiatives (Barr, 2002).
The National Health Service (NHS) Plan (Department of Health (DH), 2000) set out the government’s vision to modernise the health service to make it fit for the 21st century. Education and training became central to the delivery of the modernising agenda – ‘Patients … depend upon … skills and knowledge of… staff. Education … training… development are crucial to maintaining and enhancing… abilities’ (Audit Commission, 2001, p.5).
Investment in learning and development was considered fundamental for provision of care by competent, skilled and appropriately trained staff, working effectively together rather than autonomously, to improve the patient’s experience (DH, 2002). As part of this plan, commitment was made by the government to four sites for workforce development funding to lead on interprofessional education (IPE) progression. Further to this, a multi-professional post-registration framework for continuing professional development (CPD) was implemented which sought to develop pathways supporting new ways of working.
Additionally, the NHS development agenda emphasised the importance of collaborative working as a means of modernising services and traversing professional boundaries. As a result, the development of collaborative learning gathered strength and IPE was supported as a way of changing practice and the nature of the workforce (DH, 1999, 2000, 2006). Organisations were advised to commission IPE in professional education, to create an interprofessional workforce (DH, 2007). The introduction of quality-based commissioning highlighted the need for evaluation of IPE in comparison with other types of professional education, both in terms of educational value and ongoing effects in the quality of clinical practice.
In 2007, changes to pre-registration education and training were announced to account for emerging and developing roles (DH, 2007). This meant changing educational systems to accommodate NHS needs, requiring more flexible approaches and greater emphasis on learning in practice. It was argued IPE should become an essential part of education where inclusion of core skills and common learning with other professions and groups was the norm, contributing to business success and organisational strategy. Johnson et al (2003, p. 80) assert the essence of collaboration is based upon ‘trust… stable working relationships’, however, in practice there are numerous reasons why collaboration may prove difficult to achieve; e.g. differing political agendas, values, goals, cultural differences, workloads and demands.
The theory supporting IPL is concerned with the concept of advancement of learning, improving patient outcomes through interprofessional working and the need to consider relationships between theory and practice, values, knowledge and skills. IPE provides a platform for two or more professions learning with, from and about each other to improve collaboration and the quality of care (CAIPE, 2007). Johnson et al (2003, p. 70) intimate that effective collaboration is dependent upon ‘collective efficacy; … combined efforts… each… capable… willing to do its share’.
The introduction of IPL to our organisation was to bring about change which challenged practice and culture. As change can stir emotions and bring resistance, insight into change theory, and how to influence and enable change was essential to the potential success or failure of the project (Deegan et al, 2005). Meads (2007) advises sustainable change as being reliant upon effective cultural change, thus, our team was required to consider historical bases, professional roles, purpose, potential barriers, educational staff and learners’ attitudes, differing knowledge bases and previous experiences.
Methodology
Bell (2001, p. 9) suggests the ‘practical, problem-solving nature of action research makes this approach attractive to practitioner-researchers who have identified a problem during the course of their work and see the merit of investigating it and if possible improving practice.‘
For our trust, this project provided the occasion for a journey of discovery, seeking to improve infection prevention and control practice, enabling ideas to be developed, tried, tested and adjusted with the opportunity to show the learning along the way through action research. The self-reflective cycles of planning, acting, observing, reflecting and re-planning processes formed the basis for educational change and practice improvement (McNiff and Whitehead, 2002) (Figure 2).
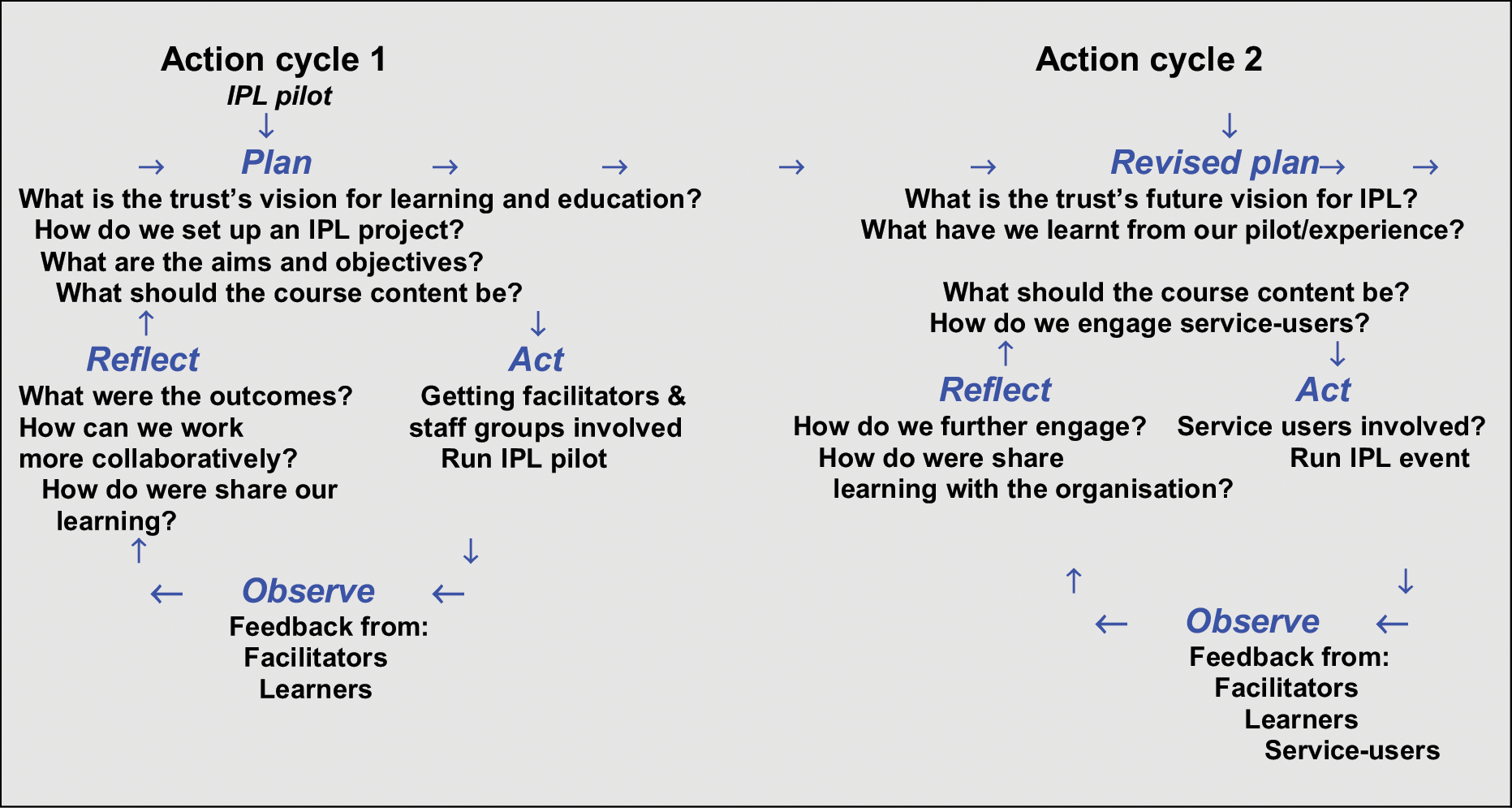
Action research cycles (model after Carr and Kemmis (1986))
Plan
A multidisciplinary strategy group was established to set out the trust’s IPL vision, develop themes for IPL education, articulate aims and objectives and design a pilot session which would inform future IPL sessions and development of the trust project.
Following a tried and tested structure, the Department of Health clinical governance framework (DH, 1999) was used to guide project development. Consideration was given to:
Purpose
Establishing leadership, accountability, working arrangements and relationships
Inclusion
Gaining ‘top level’ organisational commitment
Communications
Aims were determined by focusing upon a framework used to plan the programme and its evaluation:
Where are we now?
Where did we want to be and when?
How would we get there?
Actions and timescales?
Funding?
Project funding supported the appointment of an IPL lead, continuing facilitator development and purchase of resources and equipment. Accommodation for simulation exercises was identified and a plan was submitted for development of the area.
A multi-professional facilitation team was established to develop, manage and review the IPL pilot event, prior to formally launching the full IPL programme.
In preparation, the IPL team participated in an advanced facilitation study day which afforded facilitators the opportunity to meet, work interprofessionally, discuss expectations, seek support and address concerns.
Evaluation of the pilot was considered particularly valuable as Reeves et al (2008) highlight the shortage of IPL evidence in acute hospital settings.
Content of the pilot
The pilot event was underpinned by specific themes for IPL development, identified by the strategy group. Content of the interactive workshops focused upon:
Teams and leadership
Decision making
Stress
Systems, processes and outcomes
Communication
Safety
Situation awareness
The intention was to observe and evaluate IPE from both learners and facilitators perspectives in order to:
Develop participant leadership, management and communication skills through IPL
Develop facilitators’ leadership, management, facilitation and communication skills through their interaction
Increase knowledge about reducing avoidable HCAIs by reinforcing policies, reviewing working practices, changing behaviours and improving communications
Pilot event objectives were therefore focused upon:
Exploring learners’ perceptions of IPE, teams and teamwork at the beginning and end of the event
Exploring facilitators’ perceptions of interprofessional and educational interaction
Observing logistics within the learning environment
Evaluating the pilot in terms of acceptability, process, strengths, weaknesses and areas for improvement to establish content of future sessions
A decision was made to limit places to 25–30 people, permitting manageable interactive workshops. The event was promoted three months in advance on the trust intranet and additional flyers seeking voluntary nominations were distributed. Staff were informed of the purpose of the IPL pilot and the intention to use evaluative data to inform our action research and the future series of IPL events.
Act
The IPL pilot event was facilitated by seven multi-professionals, including the interprofessional learning lead, senior clinical teaching fellow, infection prevention control nurse/educator, patient environment manager, decontamination lead, specialist nurse and antibiotic pharmacist. Facilitation roles involved: one co-ordinator/observer/time keeper, one facilitator per workshop and one role-player – ‘Mr Brown’s daughter’.
Learners comprised 21 multi-professional healthcare staff: five patient-environment, one doctor, one matron, one midwife, four pharmacists, seven registered general nurses (RGN) in preceptorship, one x-ray assistant and one RGN x-ray.
Registration including lunch, offered learners the opportunity to meet informally before the event began. This was followed by welcome, introductions, aims and objectives and a PowerPoint presentation to set IPC and HCAIs in context.
Learners were reminded of their voluntary attendance status and of our intention to use evaluative data to inform the research and future series of IPL events; therefore consent was requested.
‘The Patient’s Journey’
Learners were introduced to ‘Mr Brown’, a 70 year old man admitted from his nursing home with pneumonia, meticillin resistant Staphylococcus aureus (MRSA), past history of stroke, type 2 diabetes and recent diarrhoea.
Facilitators then divided learners into five mixed occupational groups prior to all of us embarking upon both ‘The Patient’s Journey’ and our individual IPE journey.
‘The Patient’s Journey’ comprised five, 20 minute interactive team-based workshops following ‘Mr Brown’ from admission to discharge.
Before completion of each workstation, a ‘five minute’ alert gave facilitators an opportunity for workstation summary and capture of key learning for later large group discussion.
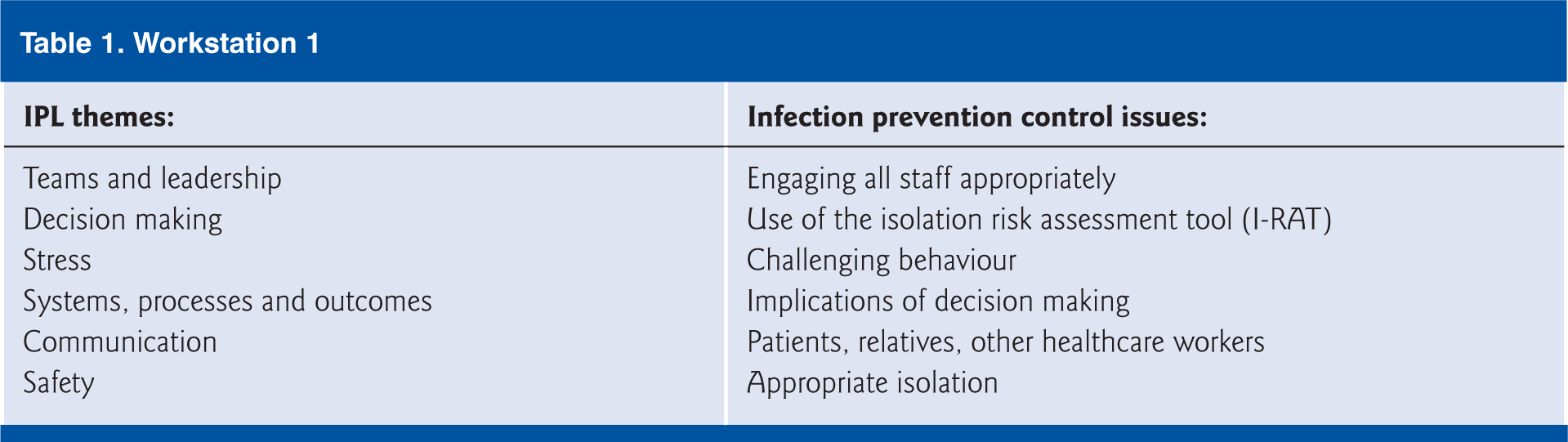
Workstation 1– Admission (Table 1)
The group were presented with a ward plan detailing patients by sex, age and diagnosis and were asked to admit ‘Mr Brown’ to an appropriate ward area. This exercise required:
Demonstrating knowledge of infection precautions and risk along with appropriate isolation precautions
Reference to and application of the trust’s isolation risk assessment tool (I-RAT)
Use of the Bristol stool form chart
Workstation 1
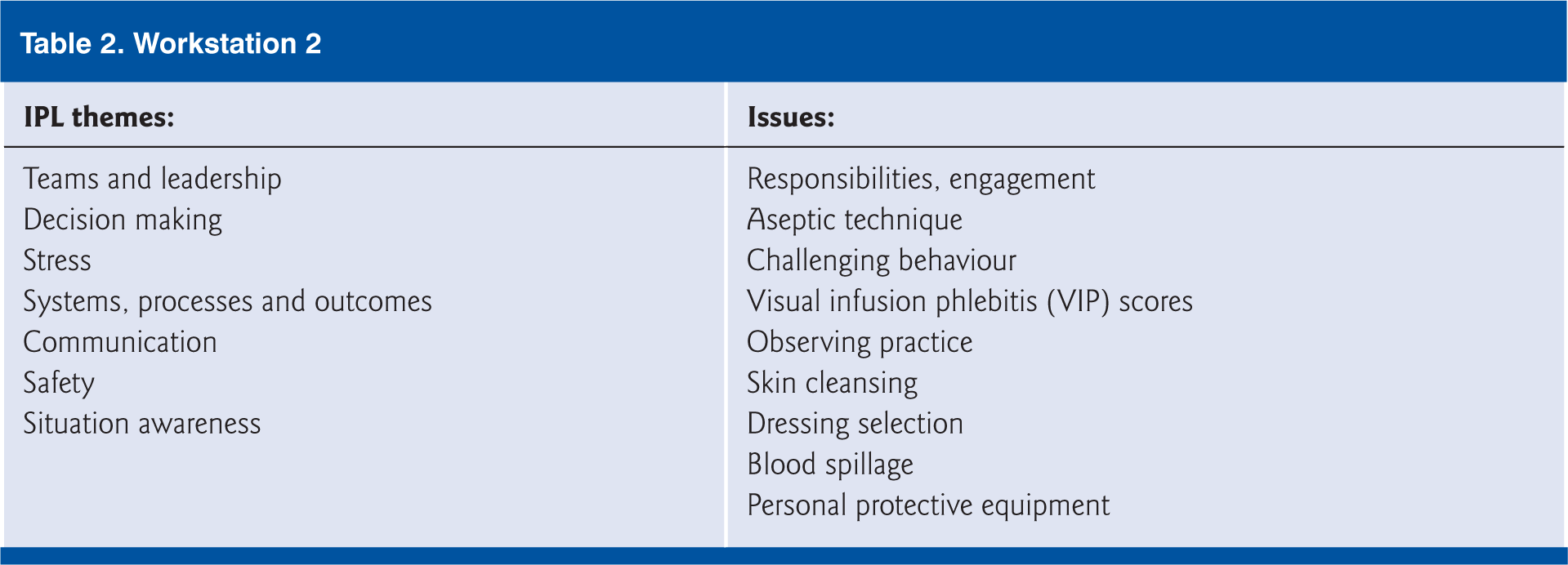
Workstation 2 – Cannulation (Table 2)
The facilitator performed a poor cannulation procedure to provoke debate regarding policy, correct technique and challenging behaviour.
Workstation 2
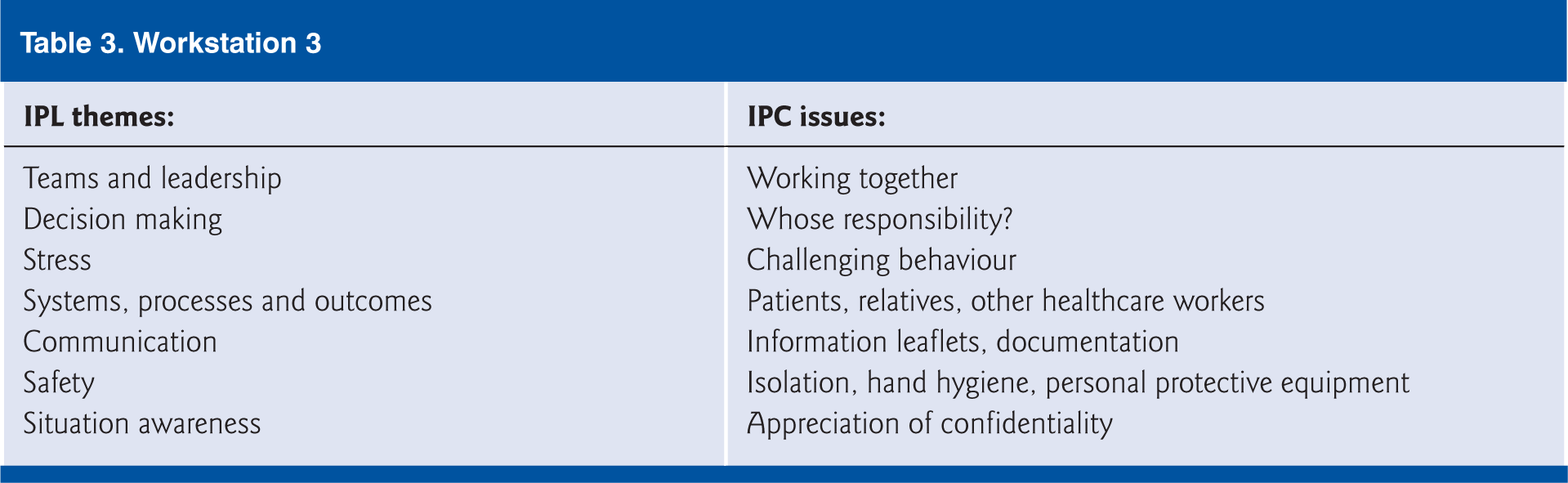
Workstation 3 – Communicating bad news; HCAI (Table 3)
Learners were informed ‘Mr Brown’s stool sample was confirmed as positive Clostridium difficile (C. diff) infection’ and were requested to break this bad news to his worried daughter who asked numerous questions:
How did this happen?
Who is responsible?
I have heard about this in the news, people die; is that what’s happening?
What does this mean for my father?
Was this preventable?
Workstation 3
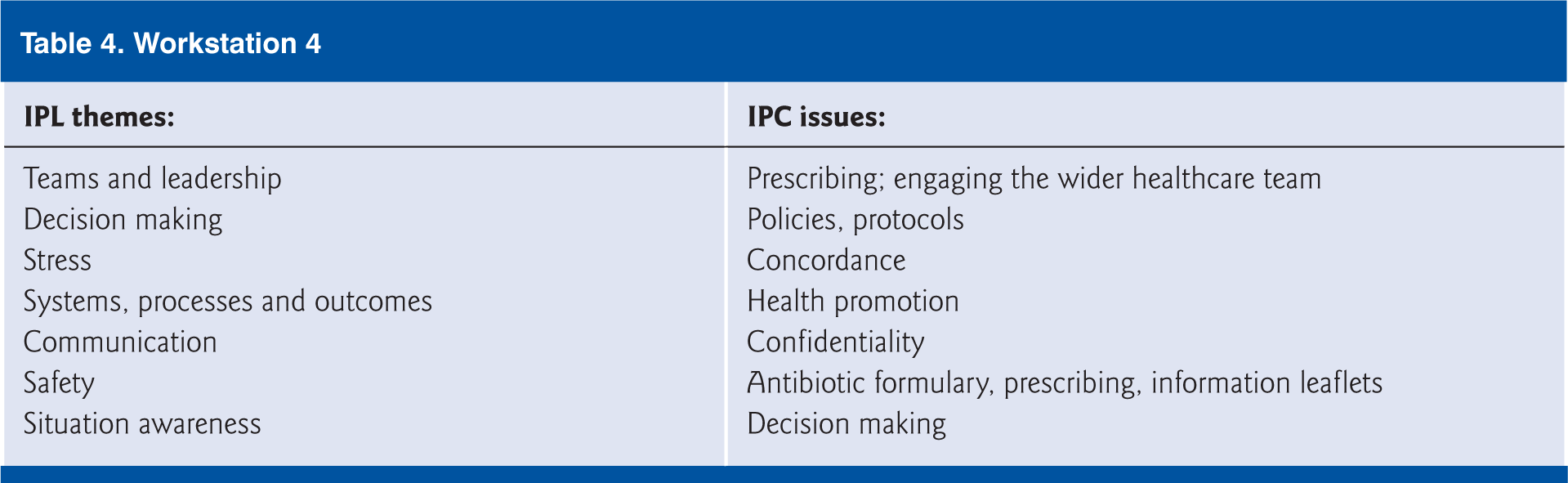
Workstation 4 – Prescribing (Table 4)
This station focused upon:
Treatment for pneumonia, requiring review of the trust’s antibiotic formulary
MRSA protocol
C. diff. protocol
Workstation 4
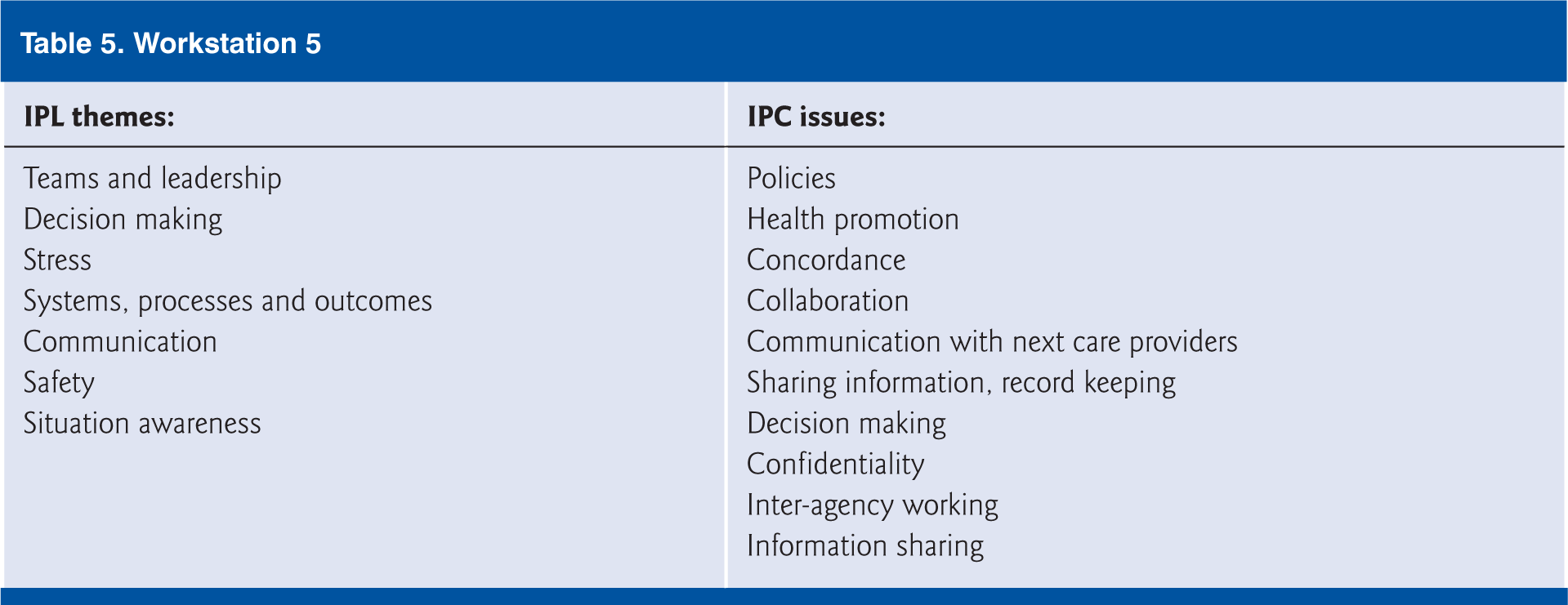
Workstation 5 – Discharge (Table 5)
Learners were requested to reflect upon a number of discharge issues:
What do we need to do to get ‘Mr Brown’ home?
Will his nursing home take him back?
What, if any, precautions will the nursing home need to take?
Who needs to know about ‘Mr Brown’s infectious status and how much information should we give?
Workstation 5
‘House of horrors’
Before the start of the event, facilitators planted a number of infection risk ‘horrors’ (e.g. overfilled sharps bin, bloodstained gloves on table, urinal on bedside-locker) in the clinical area where the interactive workstations were based. These ‘horrors’ were revisited in final group discussion to focus upon healthcare staff behaviours.
Patient involvement
Throughout the IPL programme development, consideration was given to patient involvement. The trust determined to run the pilot event and reflect upon the experience before seeking formal patient engagement. However, to ensure the theme of patient involvement was enabled at the pilot event, a display board was used to present letters received by the trust from patients and relatives regarding HCAI.
IPL – what can we take back to the workplace?
The event concluded with learner and facilitator discussion, consolidation and evaluation.
Observe
To provide direction for the future IPL project and determine content of further events, quantitative and qualitative data were collated from both formal learner post-event written evaluation and informal learner and facilitator observation and verbal feedback.
IPL pilot post-session evaluation
Learners were requested to evaluate the pilot by scoring Content, Organisation, Delivery, Relevance and Overall rating (CODRO), using a system where 0=poor to 10=excellent (Figure 3).
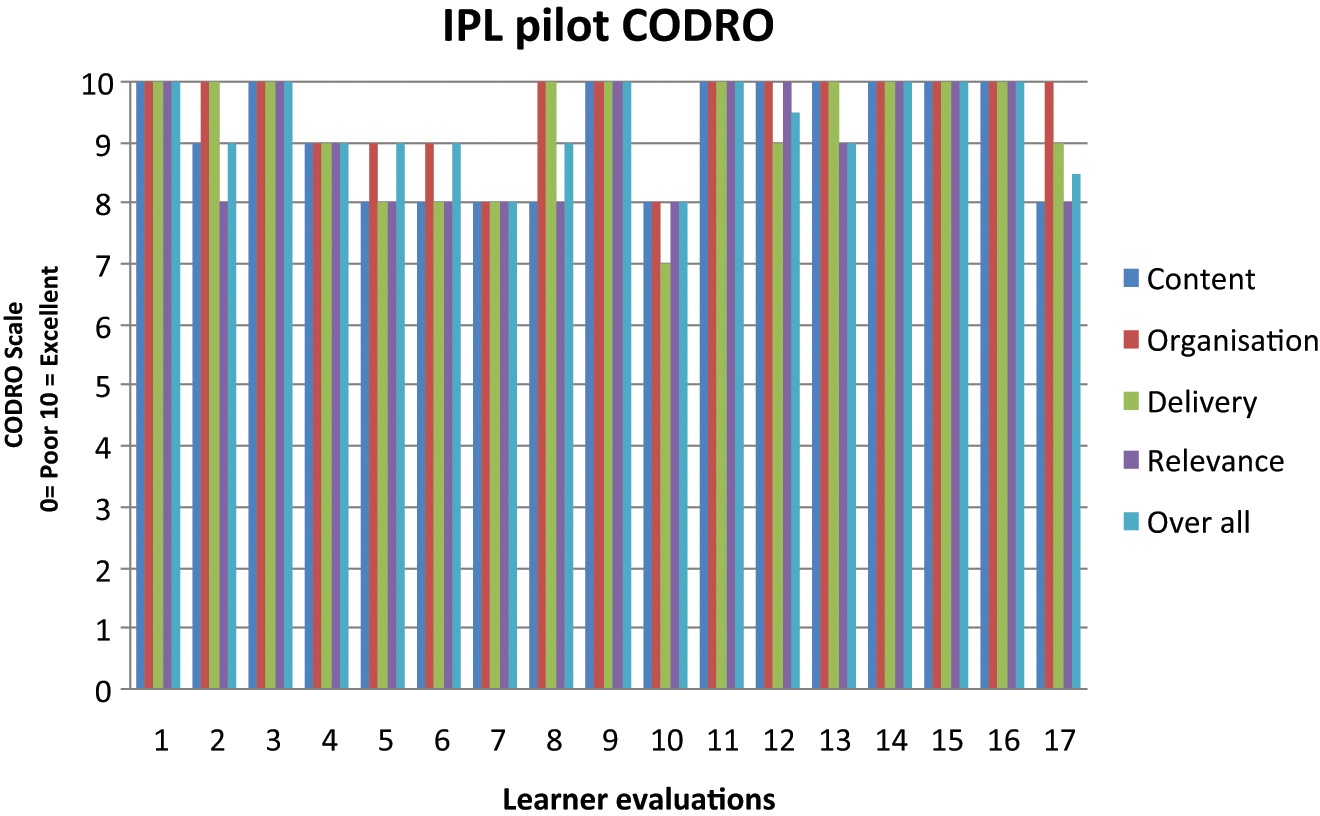
Bar chart representing IPE CODRO scores
Evaluations were completed by 17 (81%) learners with CODRO scores >90%.
Additionally, learners were asked to feedback:
Two positive points from the session; 17 (48%) responded
Learning to take back to their workplace; 16 (76%) commented
Areas for improvement/inclusion; 10 (48%) replied
Further general comments; 10 (48%) offered information
Reflect
Overall, the evaluative data provided evidence that the IPL pilot was successful in terms of meeting objectives and provision of IPL.
Missed opportunities
Facilitators observed missed IPL opportunities at registration/lunch before the formal event began, where although learners were presented with the occasion to meet and mix informally with people from other professional groups they gravitated to those they already knew or to others from similar occupations.
When facilitators divided learners into mixed occupational groups for the workshops, many appeared uncomfortable until reminded they had signed up to an IPL event. In light of this conduct, facilitators reinforced the definition of IPL during introductions and while outlining aims and objectives. Learners were amused when facilitators deliberated over the ‘self-grouping’ conduct at lunch and apparent discomfort at the group selection. This experience afforded an early appreciation of how behaviours can potentially facilitate or create barriers to interprofessional or collaborative team working.
CODRO scores
CODRO scores were high; however, content and relevance returned lowest learner satisfaction, so subsequently these areas were identified for review prior to formal roll-out of the full IPE programme.
Positive aspects
Most reference was made to good organisation/structure, but specific references were made to workstations being ‘a good method of learning …’, ‘practical…’ and provided learning from and with each other.
Learning to take back to the workplace
Emerging themes were identified from these comments, including increased learner awareness about colour coding for cleaning equipment, general infection prevention and control issues (although no specific examples were given) and team working.
Areas for improvement/inclusion
Varied suggestions were made including: ‘A few more doctors’, ‘More from domestic point of view’, ‘Statistics of positive practice’.
General comments
This feedback mostly conveyed learners’ views that the event was ‘Very good… well organised’. More specifically, a doctor determined ‘Possibly a little “over the heads” for domestic staff – terminology, patient assess, care etc and drugs’, which generated interesting later debate, since the domestic staff did not hold the same view, highlighting the benefit of learning with, from and about each other. One insightful learner observed that it was ‘too early to know if outcomes for patients are improved’, which is, at the crux of the matter.
Workstation 1 – Admission
Learners found this workstation challenging in terms of reaching agreement to which area ‘Mr Brown’ should be admitted. The majority were unfamiliar with the trust’s isolation risk assessment tool (I-RAT); however, once directed, they were enabled to rationalise and formulate evidence-based decisions. The doctor expressed surprise by the evident IPC knowledge of patient-environment staff, as they readily made risk assessments and took decisions regarding bed allocation.
Workstation 2 – Cannulation
There was general consensus that this workstation was demanding for the facilitator in terms of engaging all learners due to diversity of professional roles. Some non-clinical learners felt this ‘not relevant to them’. The facilitator reported feeling ‘it went against the grain’ demonstrating ‘poor’ technique, having spent a career ‘doing the right thing’ while educating staff.
Workstation 3 – Communicating bad news; HCAI
With the exception of one nurse, all learners, ‘allowed’ or ‘expected’ doctors to communicate bad news to ‘Mr Brown’s daughter’, with a general consensus by each of the groups that ‘it’s (doctors) their job’.
Later group discussion identified a majority of learners lacked the confidence to communicate bad news because they felt they had limited infection prevention control knowledge ‘about MRSA and C. diff.’. This feedback provoked facilitators to consider how future learners could be supported; one suggestion was to provide pre-course information, e.g. patient information leaflets relating to specific infections.
Workstation 4 – Prescribing
In terms of IPL, this workstation was considered the most challenging; the facilitator expressed difficulty moving from teaching to facilitation and the majority of learners, with the exception of the doctor, felt prescribing issues were ‘nothing to do with them’. This effectively became a taught session and for future sessions would require adjustment to ensure facilitation of learning and fuller learner engagement, irrespective of profession. In later large group debate, learners were prompted to reflect upon this workstation and learning in terms of team-working and supporting each other to manage patient and family care, rather than simply focus on prescribing issues.
Workstation 5 – Discharge
Discussion focused upon the number of healthcare professions involved in ‘Mr Brown’s’ safe discharge, their roles, team-working/collaboration and effective communication. Critical learning involved raising staff awareness of sharing information regarding ‘Mr Brown’s’ infection risk/status with the next care providers, while protecting confidentiality, particularly in relation to diagnosis.
‘House of horrors’– infection prevention and control risks
Integral to the final large group discussion, learners were asked to report any ‘horrors’ they had observed as they moved around the workstations. This was supported with a slide-show of photographs of planted ‘horrors’ and commentary of additional ‘horrors’ created by learners as they had moved around the workstations, e.g. sitting on the patient’s bed, using the commode lid (which had been planted on a patient’s bed) as a place to write, using the lever tap as a toilet-roll holder.
Although the majority had in fact observed ‘horrors’, they had chosen not to identify or comment upon these during the interactive work. This discussion enabled a significant learning point about the behaviour of healthcare staff, i.e. in practice people often observe ‘horrors’ but perhaps choose not to address them, challenge offenders or take action.
The event provided occasion to address and discuss critical HCAI issues within our trust, including those around infection prevention control practice compliance and how to challenge non-conformity. Randle and Clarke (2011, p. 224) state a “comprehensive approach where all staff groups, especially medical staff work together to reduce HCAIs” is necessary, but found conformity with the Code of Hygiene (DH, 2010) was primarily driven by organisational change and top-down approach by senior managers to compel change but consequentially, this enabled others.
One of the key reasons for considering IPL as a learning method for our organisation was to proffer cultural change; professions learning with, from and about each other to improve collaboration and practice. Creedon et al (2008) suggest compliance with infection prevention and control practice is predominantly influenced by organisational culture. Post-event, learners demonstrated a fuller appreciation of the wider healthcare team, the roles of others and were better informed and therefore felt more empowered to challenge practice.
Patient involvement
Learners found the letters board thought provoking; this presented a clear reminder that patients and visitors are often informed and very aware of what is happening around them and to them.
Facilitator feedback
Facilitators were encouraged to discuss their role and experience post-event. They determined theirs was a positive experience; they felt that they had taken ownership of the programme development, delivery and learning and were afforded opportunities to extend knowledge, skills, leadership and management roles. However, they recounted that while the facilitation workshop had prepared them for the event, the reality of moving from teaching to facilitation was challenging and on occasion some felt out of their comfort zone and exposed, but accept this will change with experience over time.
Facilitators and barriers to IPL
Project funding permitted the trust to bring its vision for IPL to fruition. An IPL lead was employed for a fixed term to drive the project. Funding also permitted development of a clinical work area to host the events and development of a large multidisciplinary team of staff as facilitators, though despite this only a small number of facilitators were actually willing to engage in the IPL event when requested. For the future, staff attending a facilitation development day will be expected to commit to engagement at future IPL events to ensure responsibilities are equally shared.
These are challenging times in healthcare and resources are limited; IPL is resource intensive in terms of time and staff engagement; one facilitator is required for each small group of learners and facilitators/learners require time out of the workplace to participate. Furthermore, a multidisciplinary mix of learners is essential to the underpinning learning philosophy. Although we are fairly confident we will succeed in engaging doctors (as IPL fits with their compulsory programme) and students (who are supernumerary) in future IPL events within our organisation, we recognise attendance at future IPL events may be limited without the support of all managers.
Effective planning, organisation and structure were critical to the smooth running of the event. With hindsight, we appreciate some learners may have benefited from receipt of a pre-event pack to support preparation and their learning.
Group discussion and pilot evaluation provided useful feedback to permit adaptation to the programme and workstation content. It was apparent through discussion and evaluative data that some learners had misconceptions regarding the roles of others and IPC practice. Therefore future IPL events will focus upon introducing this theme as a key aspect of the introductory session where learners will have the opportunity to explore the roles of others with others. Additionally some workstations require review and a focus that ensures the engagement of all learners.
If IPL is to become a successful and accepted learning method within the trust, it is essential to communicate the philosophy of team-working throughout the organisation and employ this more widely, e.g. for delivery of mandatory educational sessions and for development of other healthcare topics.
Conclusions
Effective leadership and management of IPL and team-working are fundamental to outcomes for healthcare improvement. Collaborative working is challenging; it depends upon a common vision, shared aims and understandings and is sometimes difficult to achieve in reality. However, this pilot has demonstrated the trust’s capacity for professions learning with, from and about each other to improve collaboration and the quality of care to enable focus upon the trust’s ability to reduce avoidable HCAIs agenda and practice improvement.
Following the IPL pilot, the trust has determined to venture ahead with the action research and progress a series of IPE events to enable formal evaluation of the project and its impact upon healthcare practice to reduce avoidable HCAIs.
Footnotes
Funding
This project was supported by the Strategic Health Authority Workforce Development and Innovation Fund.
Conflict of interests
None declared.