
Abstract
Objectives:
This study aims to assess the vaccination uptake and attitudes of healthcare workers (HCWs) towards seasonal influenza vaccination after incorporating pandemic H1N1 (pH1N1) strain in the vaccines.
Methods:
A self-administered anonymous questionnaire was issued to nurses registered with any of three collaborating nursing associations in Hong Kong.
Results:
A total of 709 questionnaires were completed, representing a response rate of 28.4%. The coverage of 2010/11 seasonal influenza vaccines was 24.1%. It was lower than that of 2009/10 seasonal influenza vaccines, in which pH1N1 strain was not yet included (37.1%), but higher than that of monovalent pH1N1 vaccines introduced during the pandemic in 2009 (14.2%). The reduction in the number of vaccinated HCWs varied among sub-groups classified by age, duration of employment, type of contacts with patients or past seasonal influenza vaccination record. Early recipients of the vaccine were more likely to have already been vaccinated in the preceding year (odds ratio (OR)=2.95, 95% confidence interval (95% CI) =1.15–7.59) and showed an intention to be vaccinated in the following year (OR=2.78, 95% CI=1.13–6.83). However, incorporation of pH1N1 strain in trivalent seasonal vaccines did not significantly increase the desire for vaccination.
Conclusion:
In addition to upholding the efficacy and safety standard of influenza vaccines, compliance and acceptance strategies shall be developed as early as possible, and tailored to the needs of different sub-groups.
Introduction
The world experienced an influenza pandemic caused by a novel H1N1 virus in 2009. In addition to seasonal influenza vaccination, a separate monovalent vaccine against pandemic influenza H1N1 (pH1N1) was available in December of the same year (Centre for Health Protection, 2009). Immunisation against influenza for healthcare workers (HCWs) is crucial to reduce transmission in healthcare settings and to reduce extra healthcare expenditure (Carman et al, 2000; Speroni et al, 2005; Anikeeva et al, 2009). In the interest of public health and for evaluating infection control, studies on acceptance and coverage rate of the monovalent pH1N1 vaccines among HCWs have subsequently been conducted in various places (Rachiotis et al, 2010; Tagajdid et al, 2010; Virseda et al, 2010; Park et al, 2011; Seale et al, 2011). The strains included in trivalent seasonal influenza vaccines are updated annually. A seasonal influenza A/Brisbane/59/2007 (H1N1)-like virus was replaced with the pandemic A/California/7/2009 (H1N1)-like virus in 2010/11 trivalent seasonal influenza vaccines, but whether this replacement affected vaccination uptake among HCWs has not been fully evaluated yet.
To ensure that protective immunity has been attained before the peak of influenza activity, HCWs are recommended to receive vaccination as soon as the vaccines become available (Fiore et al, 2010). As a city located in a sub-tropical region in the northern hemisphere, Hong Kong has two influenza peaks, the first occurring between January and March, and the second from July to August (Chan et al, 2009). Practically, the last quarter (from October to December) of each year is often the appropriate time for vaccination to achieve effective prevention of seasonal influenza infection in the following year. Currently, the proportion of HCWs receiving vaccination in this period has not yet been documented. An understanding of the differences in characteristics of those vaccinated well before and during the influenza peak season, if any, would be helpful to inform future planning for increasing uptake and compliance of seasonal influenza vaccination.
In these connections, a study was conceptualised to assess the impacts of the incorporation of pH1N1 strain in seasonal vaccines on the coverage rate in HCWs before the 2011 influenza seasons in Hong Kong. Factors influencing the timing for seasonal influenza vaccination were also evaluated. Acceptance level among HCWs was determined by exploring changes in HCWs’ acceptance of vaccines incorporated with pH1N1 strain.
Methods
A self-administered anonymous questionnaire was employed to assess the vaccination practices among both registered nurses and enrolled nurses in Hong Kong. Both professionally qualified, registered nurses have completed three years of training in a recognised training school and are holders of a degree or diploma in nursing or equivalent, whereas enrolled nurses have completed two years of training under a hospital-based programme in a recognised training school.
Nurses registered as members of the Hong Kong Nurses General Union, the Nurse Branch, and the Enrolled Nurses Branch of the Hong Kong Chinese Civil Servants Association were invited to participate in the questionnaire survey. Attached with an introductory letter explaining the purpose and nature of the study and stating the protection of anonymity, the questionnaire was delivered to each member’s postal address through the nursing associations. The questionnaire was piloted and revised after discussions with practising nurses prior to administration.
As almost all frontline nurses in Hong Kong are ethnic Chinese, the questionnaire was constructed in the Chinese language. Respondents were asked about their status and reasons for receiving or refusing vaccination against seasonal influenza in (a) 2009/10; (b) 2010/11 seasons; and (c) pH1N1 vaccination during Pandemic (H1N1) 2009. An assessment was made of HCWs’ willingness and intention to receive an influenza vaccine containing the strain pH1N1, in the season 2011/2012. Respondents vaccinated against 2010/11 seasonal influenza were further asked to provide the date of vaccination. In light of the raised influenza activity in the beginning of 2011, respondents vaccinated for 2010/11 seasonal influenza on or before the last day of 2010 were categorised as the early vaccination group in the analysis. In the survey, respondents’ attitudes towards influenza epidemics were assessed by a 6-point Likert scale. A score equal to 4 or above was classified as an agreement with the respective statement on attitude. The questionnaire ended with questions about respondents’ experience related to influenza, demographics and work nature in terms of clinical exposure.
Statistical analysis was conducted with PASW Statistics 18 (SPSS Inc. Chicago, IL). Changes in vaccination status for each sub-category of respondents’ characteristics were tested by the McNemar test, which was a non-parametric test for two related dichotomous variables. To compare categorical differences, odds ratios (OR) were calculated by performing binary logistic regression analysis. Statistical significance was defined as p < 0.05.
Results
Characteristics of respondents
A total of 2494 questionnaires were sent out over a six-week period in March and April 2011. As of 14 April 2011, 709 completed questionnaires were returned with a response rate of 28.4%. Of these, 13 were discarded as the respondents were retirees and no longer in active nursing practice. The demographics of the 696 returned questionnaires available for analysis are shown in Table 1. Out of 691 respondents, only 84 (12.2%) had received seasonal influenza vaccination every year compared with 180 (26.0%) who never received any seasonal influenza vaccination.
Characteristics and vaccination rates of the respondents
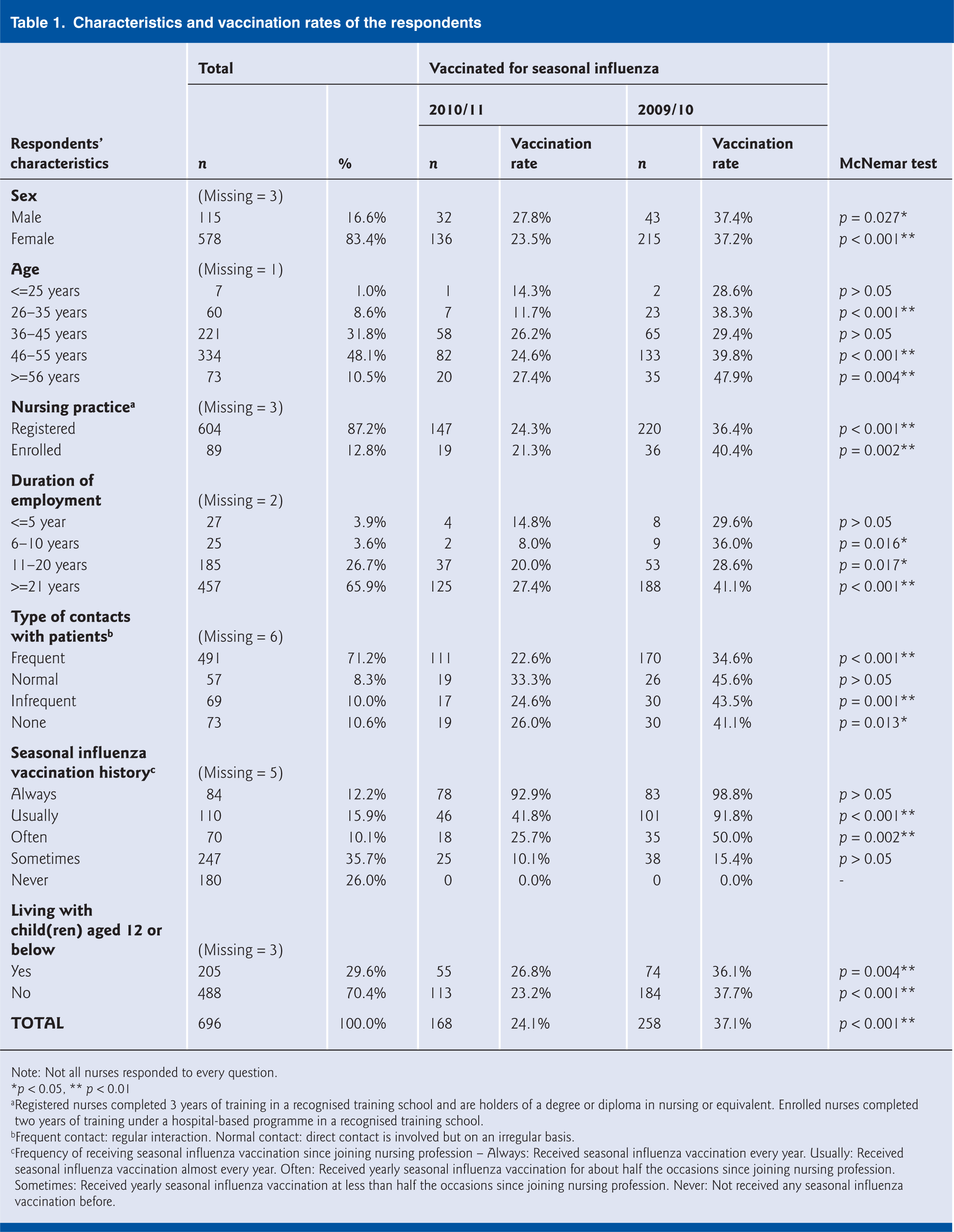
Note: Not all nurses responded to every question.
p < 0.05, ** p < 0.01
Registered nurses completed 3 years of training in a recognised training school and are holders of a degree or diploma in nursing or equivalent. Enrolled nurses completed two years of training under a hospital-based programme in a recognised training school.
Frequent contact: regular interaction. Normal contact: direct contact is involved but on an irregular basis.
Frequency of receiving seasonal influenza vaccination since joining nursing profession – Always: Received seasonal influenza vaccination every year. Usually: Received seasonal influenza vaccination almost every year. Often: Received yearly seasonal influenza vaccination for about half the occasions since joining nursing profession. Sometimes: Received yearly seasonal influenza vaccination at less than half the occasions since joining nursing profession. Never: Not received any seasonal influenza vaccination before.
Vaccination coverage for 2010/11 seasonal influenza
About a quarter of the respondents (168/696; 24.1%) were vaccinated for 2010/11 seasonal influenza. Self-protection was the most common reason for vaccination (154/164; 93.9%) whereas adverse reactions following vaccination remained the most popular concern for the non-vaccinated respondents (342/518; 66.0%). Almost all respondents (166/167; 99.4%) received vaccination by injection instead of nasal spraying. Most of the respondents’ vaccinations (150/165; 90.9%) were provided by their employers. Only six (3.6%) and eight (4.8%) respondents received self-funded vaccination in clinics or at home, respectively.
Among the respondents, the proportion receiving vaccination for 2010/11 seasonal influenza was approximately two thirds of that for the preceding year (258/696; 37.1%) and only 99 respondents (14.2%) had received pH1N1 vaccination during Pandemic (H1N1) 2009. Influenza vaccination history (i.e. vaccination for 2009/2010 seasonal influenza or pH1N1 in 2009) was a significant predictor of vaccination for 2010/11 seasonal influenza. Crude odds ratios for 2010/11 seasonal influenza vaccination recipients receiving vaccination for 2009/10 seasonal influenza and Pandemic H1N1 were 17.373 (95% confidence interval (95% CI = 11.028–27.369) and 9.169 (95% CI = 5.754–14.612) respectively. After adjusting for H1N1 vaccination during the pandemic, the odds ratio for having received the 2009/10 seasonal influenza vaccine remained significant at 12.892 (95% CI = 5.754–14.612).
Comparing the number of respondents vaccinated for 2010/11 seasonal influenza with that in the preceding year, there were statistically fewer respondents vaccinated for 2010/11 seasonal influenza. The observation was the same for both sexes and both registered and enrolled nurses. Whether the respondent was living with children aged 12 or below did not alter the significance of the decrease in the number of 2010/11 seasonal influenza vaccination recipients. However, the decrease was insignificant for vaccinated respondents aged between 36 and 45, those less than five years’ employment history, and nurses with direct but irregular contacts with patients. For those who were always vaccinated or sometimes vaccinated for seasonal influenza in the past, the vaccination rate for 2010/11 did not differ significantly (Table 1).
Time of vaccination for 2010/11 seasonal influenza
Out of 157 vaccinated respondents who indicated their time of vaccination for 2010/11 seasonal influenza, 115 (73.2%) were early vaccination recipients. Incorporating pH1N1 strain into 2010/11 seasonal influenza vaccination did not significantly affect the desire to be vaccinated for either early vaccination recipients (OR=0.60, 95% CI=0.23–1.54) or general 2010/11 seasonal influenza vaccination recipients (OR=1.17, 95% CI=0.45–3.02). However, having received vaccination against seasonal influenza in the preceding year was significantly associated with early vaccination for 2010/11 seasonal influenza (OR=2.95, 95% CI=1.15–7.59). Respondents with an intention to be vaccinated in the coming year were more likely to be vaccination recipients for 2010/11 seasonal influenza (OR=92.55, 95% CI=52.70–162.55) and to be in the early vaccination group for 2010/11 seasonal influenza (OR=2.78, 95% CI=1.13–6.83).
As regards risk perception, there was not any significant difference between early and late vaccination groups (Table 2). Nevertheless, some attitudes, such as perceived susceptibility of seasonal influenza (OR=2.00, 95% CI=1.20–3.33) and belief in effectiveness of vaccine for prevention of seasonal influenza outbreaks (OR=2.82, 95% CI=1.43–5.55), were more likely to be present in respondents who were vaccinated in both 2009/10 and 2010/11 influenza seasons.
Attitudes towards influenza epidemic of respondents receiving early vaccination for 2010/11 seasonal influenza and respondents receiving seasonal influenza vaccination in two consecutive years
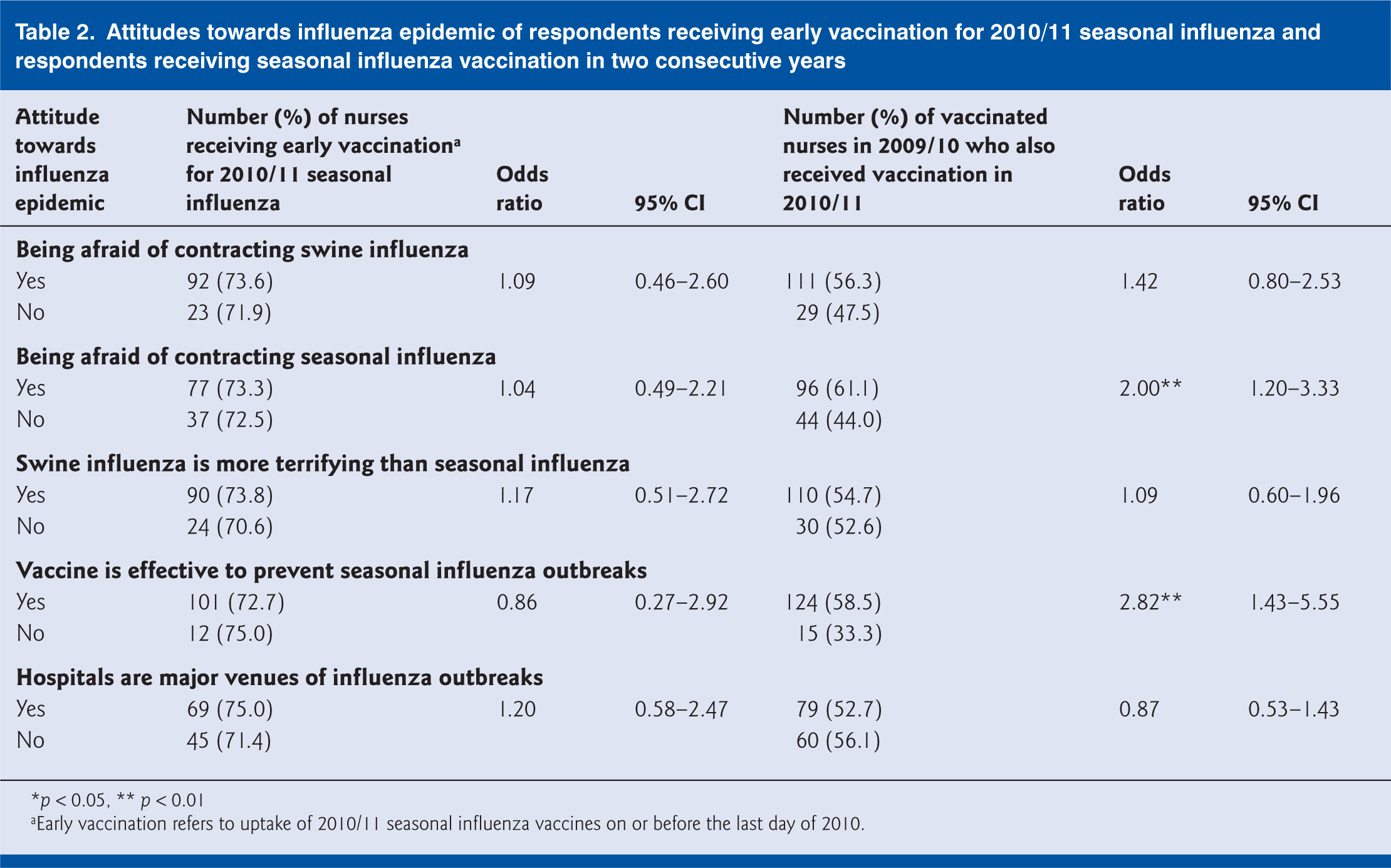
p < 0.05, ** p < 0.01
Early vaccination refers to uptake of 2010/11 seasonal influenza vaccines on or before the last day of 2010.
Among respondents vaccinated for 2010/11 seasonal influenza, 49 (31.2%) reported adverse reactions following a previous seasonal influenza vaccination, compared with that of 44.2% (226/511) in those who had ever been vaccinated for seasonal influenza. None of the respondents reported severe complications. On the other hand, mild soreness, redness or swelling at the injection site was not uncommon, but was less frequently reported by 2010/11 seasonal influenza vaccination recipients who had also been vaccinated in the preceding year (Table 3), compared with respondents vaccinated for 2009/10 seasonal influenza alone. However, there was an absence of association between discomfort or adverse reactions and the timing (i.e. early versus late recipients) of vaccination for 2010/11 seasonal influenza.
Experience following previous seasonal influenza vaccination of respondents receiving early vaccination for 2010/11 seasonal influenza and respondents receiving seasonal influenza vaccination in two consecutive years
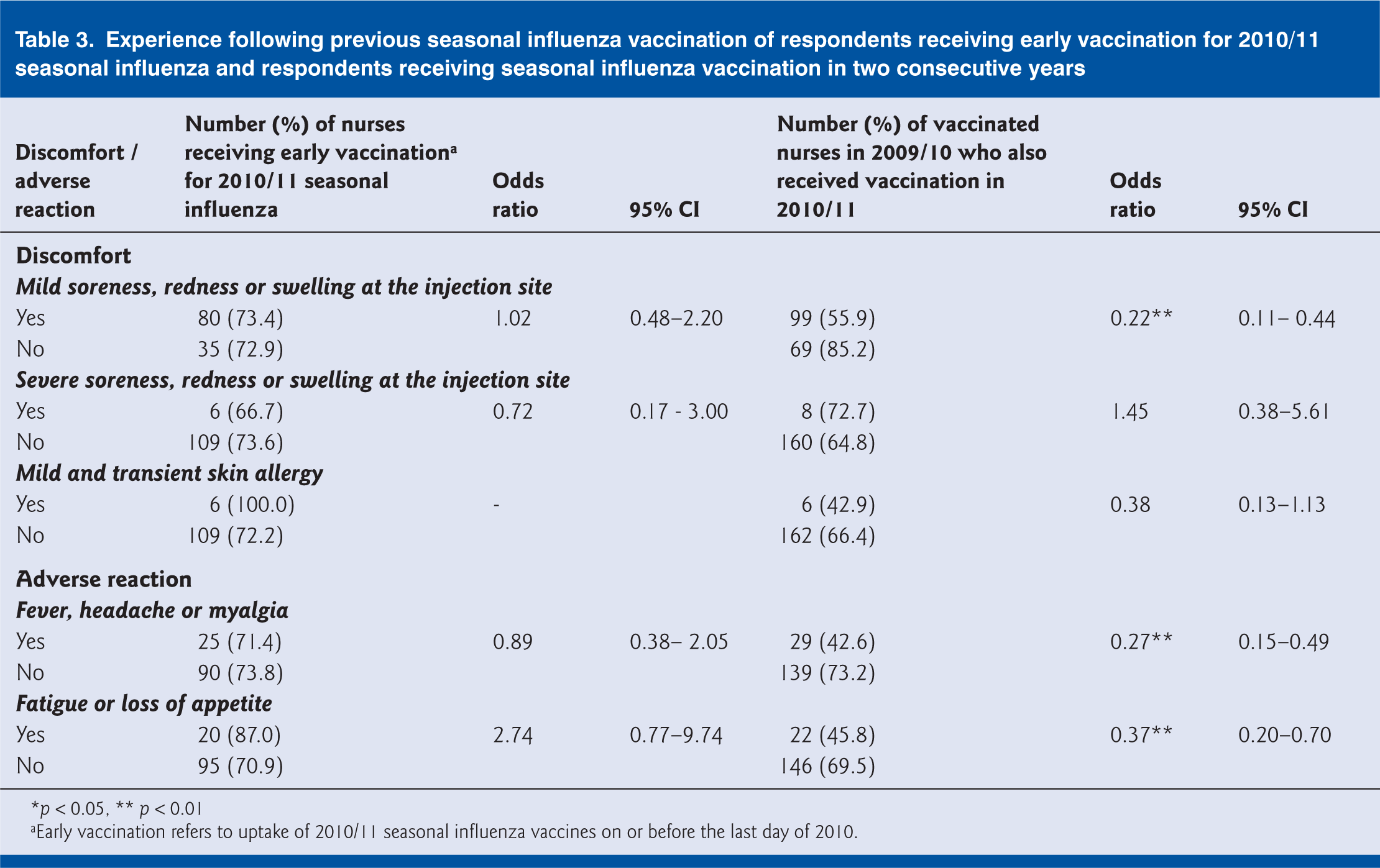
p < 0.05, ** p < 0.01
Early vaccination refers to uptake of 2010/11 seasonal influenza vaccines on or before the last day of 2010.
Discussion
In this study, we reported a 24.1% uptake of nurses for 2010/11 seasonal influenza vaccination after the incorporation of pH1N1 strain in the vaccine. This compares to 27.6% to 35.0% of healthcare professions vaccinated against influenza for the same season, reported in countries such as France, Germany and Spain (Brandt et al, 2011; Guthmann et al, 2011; Sánchez-Payá et al, 2011). The observation of a higher coverage rate of 2010/11 seasonal influenza vaccination than pH1N1 vaccination during the pandemic but a fall compared with that for 2009/10 seasonal vaccination concurred with the results in another study in Spain (Sánchez-Payá et al, 2011). The reduction in the number of vaccinated HCWs for 2010/11 seasonal influenza was however unevenly distributed in terms of age group, duration of employment, type of contacts with patients or past seasonal influenza vaccination record. Our results therefore suggest that recruitment strategies may need to be tailored to the specific needs of sub-groups in the healthcare profession, for example, targeting nurses of older age with a longer time in nursing practice or frequent contacts with patients, and nurses who received vaccination for seasonal influenza only on an occasional basis. The proportion of vaccines administered by injection, rather than intranasally, was much higher than that in another study in the United States (Christini et al, 2007). The administration of intranasal influenza vaccines should be considered as an initiative to raise uptake rates among HCWs, especially those who are needle phobic (Shah and Caprio, 2008).
The concern about adverse reactions among non-vaccinated respondents and the association between lower number of reported adverse reactions and nurses vaccinated for 2009/10 seasonal influenza alone might explain the reduced coverage of the 2010/11 seasonal influenza vaccine. Past experience of some adverse reactions after seasonal influenza vaccination could have discouraged HCWs from vaccination for the 2010/11 season when pH1N1 strain became incorporated in the vaccine. Only 7.4% (19/256) of 2009/10 seasonal influenza vaccination recipients reported a desire to be vaccinated against 2010/11 seasonal influenza. These results reflected the fact that the safety of the vaccines was still questioned among some HCWs one year after pH1N1 vaccines became available. To increase the general acceptance of the vaccines, assurance of quality and effectiveness of the vaccines would be required. Perceived effectiveness of vaccines for self-protection and prevention of seasonal influenza outbreaks influenced HCWs’ acceptance of vaccination in both years of the study, and has been noted elsewhere (Kraut et al, 2011).
To our knowledge, this is the first study that has explored the differences in characteristics of HCWs who received vaccination before and during the period of raised influenza activity. The early vaccination recipients had stronger commitment to be vaccinated for seasonal influenza, as they were more likely to have already been vaccinated in the preceding year and intend to be vaccinated in the following year. The influence of previous vaccination practice in accepting both seasonal and pandemic influenza vaccination has been reported (To et al, 2010; Chor et al, 2011). Our study echoed this finding, and supplemented it with an evaluation on its association with the timing of vaccination. This association could, however, be confounded by the vaccination schedule of respondents’ working organisation, because influenza vaccines for more than 90% of the respondents were provided by their employers. Other reports also highlighted the importance of convenient provision of seasonal influenza vaccines, especially by the employee’s organisation, on increasing the vaccination coverage (Hopman et al, 2011; Rebmann et al, 2012). For effective comparison, the proportion of respondents refusing to be vaccinated on time before 2011 would need to be reviewed in context. Unfortunately historical data about the timing of vaccination for seasonal influenza are not available for evaluation.
In the planning and development of a vaccination uptake strategy, an understanding of why some HCWs were immunised in the later period of the annual influenza vaccination campaign or had low intention to be vaccinated again was crucial. One of the possible reasons for late vaccination could be the change of public attitude following the reports of outbreaks and deaths due to influenza in Hong Kong or the United Kingdom in the first quarter (from January to March) of 2011, which were mostly related to vaccine-preventable pH1N1 virus (Centre for Health Protection, 2011). Although impending influenza epidemics and the associated influence of mass media may have impacted the acceptance of influenza vaccination, how long the effects of these factors could last is not known (Chor et al, 2009; Rachiotis et al, 2010; Park et al, 2011). The challenge of how one single exposure to vaccination could be turned into a habit of annual vaccination for seasonal influenza remains unanswered.
As a primary means to prevent nosocomial influenza, annual influenza immunisation of a high proportion of HCWs and other high-risk groups before the peak of influenza activity is important. However, the fluctuating coverage rate of seasonal influenza vaccination among nurses in Hong Kong observed from previous studies and belated vaccination reported in this study might weaken our preparedness against influenza transmissions (Tam et al, 2007, 2008; Chor et al 2009; Sypsa et al 2009; To et al, 2010). From the experience in the United States, a mandatory vaccination programme may be an option to maintain high rates of vaccination among healthcare personnel at the expense of professional autonomy (Rakita et al, 2010).
Finally, our study carries some limitations. First, the administration by post in the distribution and collection of the questionnaire might have caused a response bias by capturing those who would like to express their thoughts and opinions more readily. In this study, the response rate was about 30%, leaving the vaccination practices of more than half of the potential respondents unexplored. Second, most of the respondents of the questionnaire survey were experienced nurses who have been in the nursing profession for a long time. Notable characteristics of newly enrolled or registered nurses might have been missed in the study. The extrapolation of the results to the entire healthcare profession should also be done with caution as about 30% of the respondents were nurses without frequent contacts with patients in their practice. Third, the influenza vaccination coverage might be overestimated as vaccination statuses were self-reported (Zimmerman et al, 2003). Reporting of adverse reactions might also be subjective and an objective evaluation may not be possible in this context.
Footnotes
Acknowledgements
We would like to thank Cecilia So and Florence Lau for their assistance in the planning and development of the questionnaire surveys. Members and office bearers of Hong Kong Nurses General Union, the Nurse Branch, and the Enrolled Nurses Branch of the Hong Kong Chinese Civil Servants Association are acknowledged for affiliating the administration of the survey.
Ethical approval
Ethical approval was obtained from the Survey and Behavioural Research Ethics Committee of The Chinese University of Hong Kong.
Funding
This work was supported by the Hong Kong Mood Disorders Centre, the Chinese University of Hong Kong. The funding body was not involved in the collection, analysis, and interpretation of data, the writing of the article, or the decision to submit it for publication.
Conflict of interests
None declared.