
Abstract
urgical site infections (SSI) account for a major proportion of healthcare associated infections (HCAI) yet many hospitals capture little data on the risk of SSI in patients undergoing surgery and therefore have little assurance about the quality of infection prevention in their operating departments. This paper is the first part of a two part series that will examine the principles and practice of surveillance of SSI. Part 2 will examine the analysis of SSI data and the use of the results to change practice. This paper reviews the principles that underpin SSI surveillance methodology, key concepts that affect the accuracy of data capture systems and strategies for addressing them, including risk factors and active case finding systems to ensure detection of SSI, including those that develop after discharge from hospital.
Introduction
The risk of a patient developing an infection of the tissues involved in an operative procedure (a surgical site infection (SSI)) depends on a combination of factors including: the number of micro-organisms introduced into the operative site, the number that remain when the wound is closed, the ability of micro-organisms to multiply and invade tissues, and the efficacy of the host’s immune defences against them (National Collaborating Centre for Women’s and Children’s Health, 2008). Prevalence surveys indicate that SSI is the third most common healthcare associated infection (HCAI), accounting for approximately 15% of all HCAI (Smyth et al, 2006; Health Protection Agency, 2012). However such surveys underestimate the true risk of SSI because many infections do not become apparent while the patient is still in hospital, and only patients undergoing surgery can acquire an SSI; in this group the prevalence is estimated to be 5% (Smyth et al, 2006). Surgical site infections are associated with considerable morbidity and mortality, estimated to double the length of postoperative stay, and in the most severe infections significantly increase the risk of death (Astagneau et al, 2001; Coello et al, 2005). In addition, as demonstrated in a case control study of patients undergoing proximal femoral fracture repair, when repeat admissions to hospital, re-operations and other treatments are taken into account, severe SSI can quadruple the costs of care and decrease the quality of life of affected patients (Whitehouse et al, 2002). Similar effects on costs and mortality have been identified in cardiac surgery (Hollenbeak et al, 2000).
Pathogens that cause SSI may derive from the patient’s own microbial flora on the skin and in the body, or from the skin or mucous membranes of operating personnel, or from the operating room environment (including air), and the instruments and tools used during the procedure. Occasionally, micro-organisms from a distant infection in the body can establish an SSI by attaching to a prosthesis or other implant left in the operative site (David and Vrahas, 2000).
Practices to prevent SSI are therefore aimed at minimising the number of micro-organisms introduced into the operative site, for example removing micro-organisms that normally colonise the skin; preventing the multiplication of micro-organisms at the operative site using prophylactic antibiotics; enhancing the patients’ defences against infection, for example by minimising tissue damage and maintaining normal body temperature during the procedure; and preventing access of micro-organisms into the incision postoperatively by use of a wound dressing (Mangram et al, 1999; National Collaborating Centre for Women’s and Children’s Health, 2008). Although guidance exists to endorse these principles, adherence to best practice is more difficult to assure and in the absence of data on patient outcomes, the connection between theatre practice and subsequent surgical site infections can be overlooked.
Evidence for the potential impact of surveillance of SSI was first published by Cruse and Foord (1973, 1980), who analysed the impact of 10 years of surveillance on the epidemiology of SSI, demonstrated key factors that influenced the rate of SSI and significant reductions associated with systematic monitoring and feedback of rates to surgeons. In 1980, the Centers for Disease Control and Prevention (CDC) initiated a large, controlled, multicentre study to determine the magnitude of the problem of HCAI in hospitals and the extent to which the surveillance and control programme approach was effective in reducing the risk of infection. The study drew on a sampling frame of more than 6,000 hospitals with programmes of varying levels of intensity. A stratified random sample of 338 of these hospitals was used to estimate the impact of surveillance and control activities on rates of HCAI by reviewing case records of a random sample of 500 patients in 1970 and 1976 (Haley et al, 1980). This study demonstrated that hospitals with the most effective programmes reduced their rate of hospital-acquired infection of 32% during this period, and parallel analyses of surgical site infection, indicated that rates of SSI were reduced by up to 38% where surveillance with feedback to surgeons was in place and a healthcare epidemiologist was involved in reporting (Haley et al, 1985). The SENIC study had a major impact on HCAI surveillance systems. It not only endorsed the value of the investment required to establish robust data capture and reporting, but also provided the basis for developing standardised case definitions and approaches to risk adjustment (Culver et al, 1991).
Rates of SSI derived from a robust surveillance system can be used to assess the quality of infection control practice related to surgical procedures, increase awareness of the risk of SSI and encourage surgical teams to take appropriate action if rates increase. Indeed, as the SENIC study concluded, “Infection control problems and the need for prevention efforts were not apparent to physicians, nurses or administrators until they were given quantitative measures of the problem derived from surveillance data” (Haley et al, 1985). In addition, although there is a clear expectation that patients will be provided with reliable information about risks of SSI, in reality this is rarely possible in the absence of robust surveillance systems (National Collaborating Centre for Women’s and Children’s Health, 2008). Enabling comparison with other similar organisations can enhance the impact of surveillance through identifying outliers and driving reduction strategies. The potent effect of benchmarking has been demonstrated by significant reductions in rates of SSI in hospitals that participate in national surveillance schemes (Geubbels et al, 2004; Gastmeier et al, 2005; Rioux et al, 2007). However, while external benchmarks can be a powerful driver for change they require considerable effort and co-ordination to develop and must use principles that assure, as far as possible, the validity of comparisons, including standardised case definitions and case finding methods, analysis that accounts for variation in case mix, precision of estimated rates and period of postoperative follow-up and some assurance about the quality of data through validation systems (Cooke et al, 2000; Gaynes et al, 2001; Wilson et al, 2002).
Definition of SSI
The ability to consistently identify SSI in operative wounds is essential for reliable surveillance systems, because changes in rates of SSI observed must reflect true changes in occurrence of infection rather than the accuracy of case finding. Because skin is normally colonised by a range of micro-organisms that could cause infection, defining an SSI cannot rely only on the micro-organisms present in a wound culture sent to the laboratory but should be determined by evidence of clinical signs and symptoms of infection. A number of approaches to defining SSI have been proposed, ranging from simply the presence of pus in the wound (Cruise and Foord, 1970) to more complex scoring criteria such as ASEPSIS (Wilson et al, 1986) most of which include subjective elements that could be prone to error. Although scoring systems such as ASEPSIS provide a more objective method, they may not be easy to apply in a routine surveillance system and if comparability with other published data or institutions is a key aim of the surveillance, rates based on different definitions will not be comparable (Wilson and Elgohari, 2008). Most SSI surveillance systems use definitions based on those described by the Centers for Disease Control and Prevention, which recognise that SSI can affect the following parts of the operative site (Horan et al, 1992, 2008):
Superficial incisional: involves only the skin or subcutaneous tissue of the incision
Deep incisional: involves the deep tissues (i.e. fascia and muscle layers)
Organ/space infection: involves any part of the anatomy (i.e. organ and/or space), other than the incision, opened or manipulated during the surgical procedure.
To meet the definition SSI must align to a specific set of criteria and superficial incisional SSI must occur within 30 days of the operation. Deep incisional and organ/space SSI must occur within 30 days of the operation provided non-human material (implant) is not left permanently in the operative site, in which case an SSI can occur up to one year from the operation (Horan et al, 1992; Horan and Emori, 1997). Objective criteria are more difficult to apply to superficial SSI. Microbiological cultures from the wound may reflect colonisation rather than infection and whilst the CDC criteria refer to ‘aseptically obtained tissue or fluid’ the detailed provenance of specimens is often not documented. The presence of clinical signs (such as inflammation) may be variously interpreted as SSI by the attending physician and some surveillance systems have chosen to address this subjectivity by requiring specific evidence of clinical signs rather than only a clinician’s diagnosis (Health Protection Agency, 2011a). The presence of pus is less prone to subjectivity, although reliance on this as a sole indicator of infection would reduce the sensitivity of case findings. Evidence from the analysis of criteria used to define 436 superficial SSI reported to a national SSI surveillance service in England between January 2003 and December 2007 suggests that pus is used to define over 40% of superficial SSI, with a combination of clinical signs and clinician’s diagnosis or opening of wound a further 38% (Figure 1). (Wilson and Elgohari, 2008).
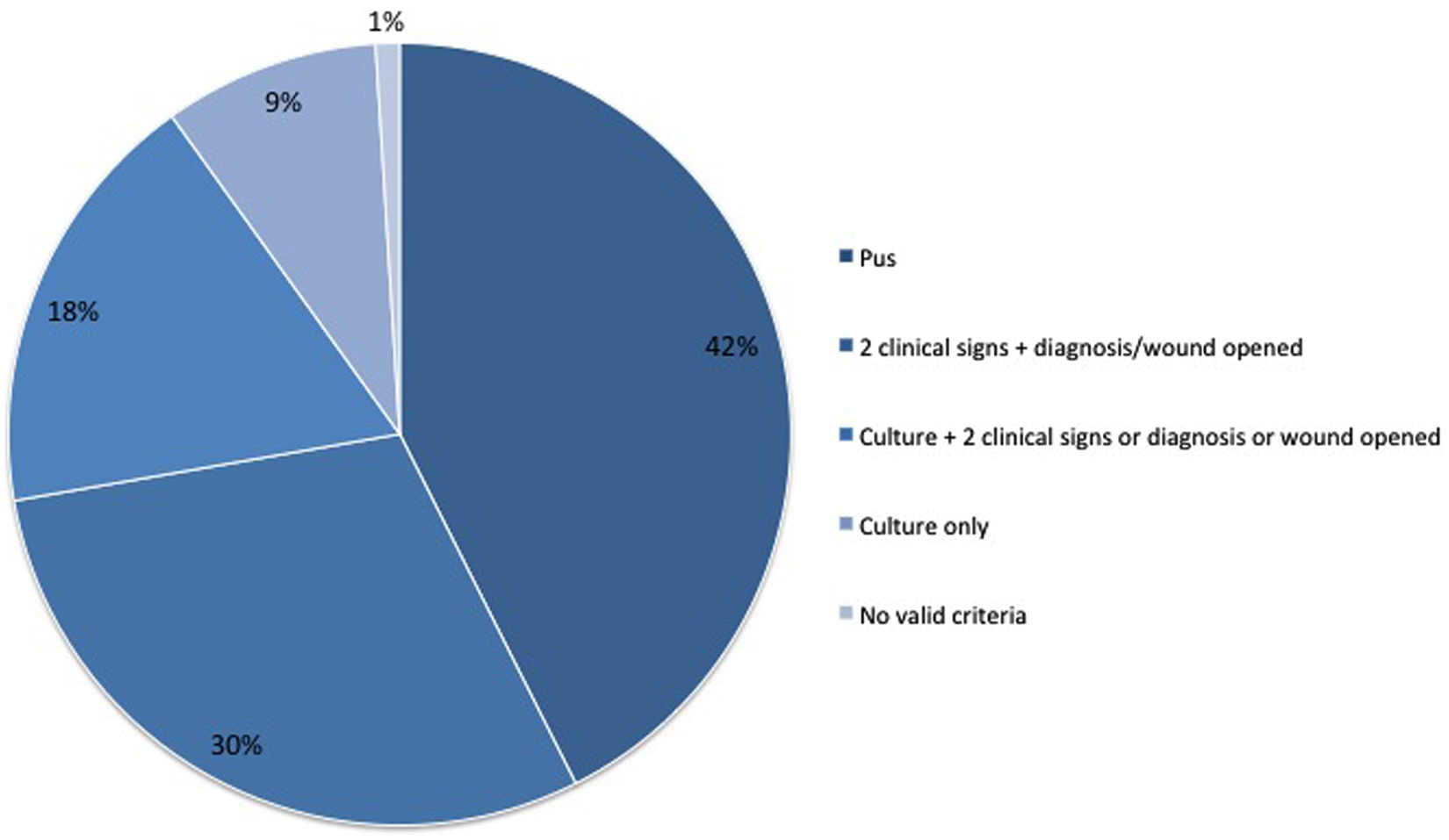
Criteria used to define superficial SSI in data submitted to Surgical Site Infection Surveillance Service in England between January 2003 and December 2007.
SSI surveillance methods
Most national SSI surveillance systems use methods based on those developed in the 1990s for the National Nosocomial Infection Surveillance System (NNIS) in the USA and which were built on the findings of SENIC (Emori et al, 1991). Surveillance is structured to monitor a set of operations and determine the risk of SSI, usually calculated as the cumulative incidence or percentage of operations that result in SSI. To calculate this metric, each patient who has a relevant operation needs to be followed-up prospectively to determine if they develop an SSI. However, the methods of case finding have a major effect on the probability of detecting SSI and therefore the accuracy of the metric. Prospective, active surveillance will find more cases of infection than retrospective or passive methods, i.e. those where infections are reported by staff who do not have designated responsibility for the surveillance programme (Perl, 1997). In addition, Glenister et al (1992) showed that even active methods of surveillance have different sensitivities of case finding depending on the reliability of the data sources queried. Surveillance based on the telephone follow-up of laboratory reports identified only 36% of HCAI compared to the 76% detected by a combination of follow-up of laboratory results, liaison with ward staff and review of case notes to identify.
National surveillance systems must prescribe methods designed to minimise the risk of selection and measurement bias in order to support their primary aim of permitting inter and intra-hospital comparisons. In the case of SSI Surveillance Service in England, these principles were guided by a defined method of identifying patients eligible for surveillance (the denominator), the application of standard, and as far as possible objective, criteria to determine cases of infection (the numerator) with prescribed methods of case finding based on previous research evidence (Glenister et al, 1992; HPA, 2011).
In the USA, responsibility for surveillance generally lies with the infection control team, often under the auspices of the quality assurance structures within the hospital. Indeed, the finding of SENIC that one infection control nurse (ICN) for every 250 beds was required to achieve reductions in HCAI was on the basis that ICNs spent a considerable proportion of their time on surveillance activities (Haley et al, 1985). While the day-to-day data capture may not need to be the responsibility of a qualified ICN, accurate rates can only be measured if active methods are employed and this requires the use of trained personnel, designated to employ a variety of methods to follow-up all patients included in the denominator. Such commitment is unlikely to be possible for clinical staff with other responsibilities, and designating responsibility for surveillance to them is likely to result in a passive surveillance system with accompanying inaccurate representation of rate of SSI. SSI surveillance undoubtedly requires considerable organisation and commitment of resources to ensure that it can be conducted systematically and consistently over sufficient periods to provide accurate estimates of SSI rate. However, evidence from Wilson et al (2007) suggests that a comprehensive surveillance programme, which collected post discharge surveillance (PDS) data from 80% of patients, cost less than £100,000 per annum, was associated with significant reductions in rates of SSI, and costs were outweighed by the savings made from reductions in rates of SSI after 2 years (Wilson et al, 2007). Similarly, Stockley et al (2001), who followed up 667 patients in five categories of surgery estimated the time for surveillance as 30 minutes per patients with an additional 10 minutes for telephoning patients post-discharge.
Post-discharge surveillance: For many categories of surgery, SSI do not become apparent until after discharge. Many studies have found that up to 70% of SSI were detected post-discharge, depending on the type of surgery and median length of postoperative stay (Stockley et al, 2001; Reilly et al, 2006). Table 1 shows the median time to detection of SSI for a range of categories. Apart from large bowel surgery, the median time to SSI as detected during the admission or on readmission to hospital is several days after the median length of stay. This presents particular problems as SSI are much more difficult to detect when the patient has left hospital. Active surveillance after discharge is difficult to implement consistently, and variation in the intensity of case finding is likely to introduce significant variation in reported rates (Reilly et al, 2006). A number of different approaches to PDS have been developed although the efficacy of detection methods varies (Petherick et al, 2006). Common approaches include review of patients at outpatient visits, surgeon questionnaire, electronic search of patient records, patient questionnaires, report cards or telephone interviews. The more passive approaches tend to suffer from poor response rates. Low sensitivity and specificity of case finding by healthcare professionals not trained in application of the case definitions is also a key problem (Manian et al, 1997; Whitby et al, 2002; Sands et al, 2003; Taylor et al, 2003; Manniën et al, 2006; McNeish et al, 2007). Several studies have based PDS on patient reporting. These studies suggest response rates of approximately 80% are achievable, together with a high negative predictive value, with over 90% of patients able to reliably indicate that they did not have an SSI. The positive predictive value of patient reporting of SSI appears to be lower (approximately 30–50%) and therefore possible signs of SSI reported by a patient should be confirmed either by trained surveillance staff or by contact with the GP or other healthcare personnel who have seen the wound (Whitby et al, 2002; Wilson et al, 2006).
Cumulative incidence and time to surgical site infection, NHS hospitals in England, April 2006 – March 2011
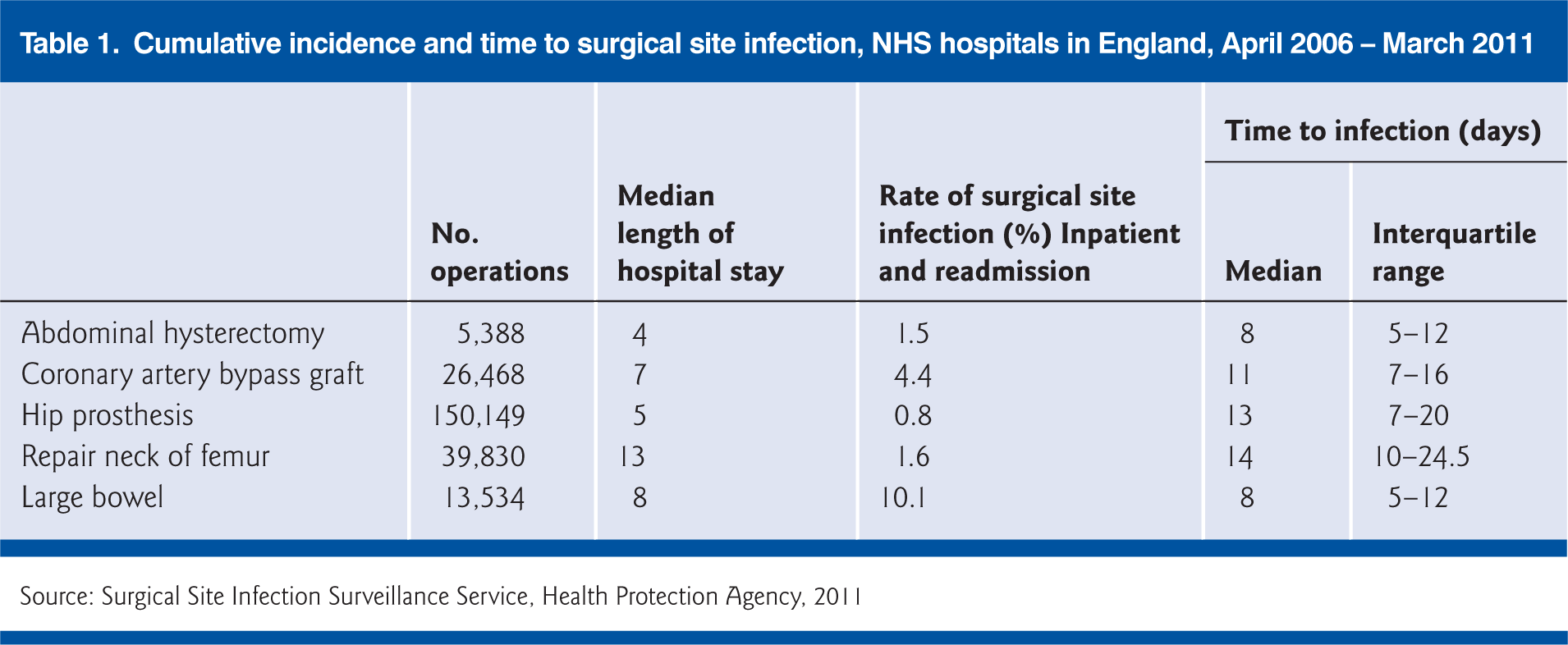
Source: Surgical Site Infection Surveillance Service, Health Protection Agency, 2011
Another approach to PDS is to systematically capture SSI in patients readmitted with SSI. This has the advantage of detecting most severe, deep and organ/space infections but will underestimate the occurrence of superficial SSI where the patient is likely to be treated in the community (HPA, 2011b). Figure 2 illustrates the increase in proportion of deep and organ/space SSI reported in the English surveillance system once readmission surveillance was made mandatory. In the orthopaedic categories, which have a short length of stay and prolonged risk of developing, readmission surveillance markedly increases the proportion of deep and organ/space SSI detected. Whatever method used for PDS, caution should be used when comparing rates either over time or between institutions, as both the length of postoperative stay and the proportion of patients followed up post-discharge is likely to have a significant impact on the estimated rate of SSI.
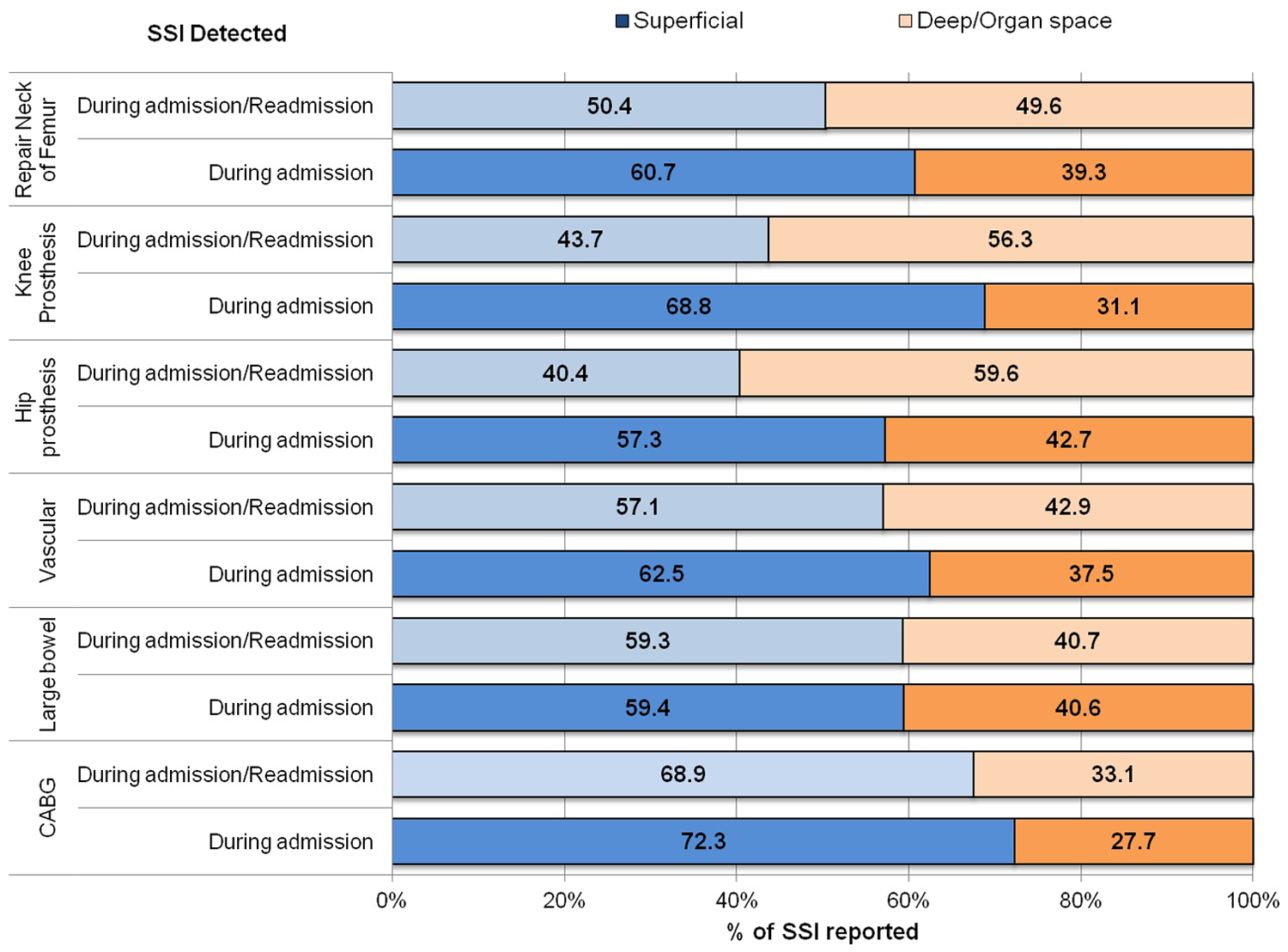
Variation in distribution of type of surgical site infection (superficial and deep/organ space) by detection during admission only and detection during admission and on readmission.
Risk factors for SSI
The case-mix of patients undergoing surgery may have a significant effect on the risk of SSI, and methods of adjusting rates of infection for intrinsic variation in the population at risk have been developed to support valid comparisons between centres or within centres over time. Most SSI surveillance systems use a risk stratification system first developed from analysis of the SENIC data. Culver et al (1991) developed a risk index based on the presence of three factors at the time of the operation and demonstrated a significant association between increasing score and risk of SSI. This risk index became the standard method of risk stratification for comparing rates of SSI and was adopted by the majority of national surveillance systems. This risk index comprises three factors: wound classification of contaminated or dirty, a preoperative American Society of Anesthesiologists’ (ASA) classification of physical status score of 3 or more and a duration longer than the T time for the category of procedure. A wound classification developed by the National Research Council in the USA is used to distinguish the likelihood and degree of wound contamination at the time of operation, taking account of both microbial contamination associated with normal flora present at the operative site, evidence of infection or inflammation at the site at the time of surgery or an intra-operative event that results in contamination of the operative site. The preoperative ASA score provides an assessment of the patient’s preoperative physical condition, and whilst it is vulnerable to inter-rater variation, it provides a crude but easily captured measure to distinguish patients with systemic underlying illness, and despite its limitations it does seem to be reliably associated with risk of SSI, especially if comparing groups with scores below 3 with those of 3 and above between which adjusted odds ratios for risk of SSI of between 1.5 and 3 have been reported (Ridgeway et al, 2005; Kaye et al, 2005; Neumayer et al, 2007).
The T time represents the duration of surgery at the 75th percentile of the distribution of operation times within a given category of surgical procedures. This time is then rounded up to the nearest hour to indicate procedures of prolonged duration which may be considered to represent increased risk of SSI due to the complexity of the procedure, although this may also reflect the experience of the surgeon. While the standard T times were derived from data captured for the SENIC study (Culver et al, 1991), they have been shown to be sufficiently robust to apply to most categories of surgical procedures undertaken in the UK now. Procedures with durations longer than the T times are significantly associated with increased risk of SSI (Russo and Spelman, 2002; Ridgeway et al, 2005; Leong et al, 2006). Each of these three risk factors contributes one point to the risk index, and each operation is allocated a score of between 0 (none of the risk factors present) to 3 (all of the risk factors present). If captured on all patients at risk of SSI it can be used to determine rates of SSI for specific risk groups and the effect that variation in distribution of risk groups has on the rate of SSI and observed differences between centres. Although the risk index represents a relatively simple approach to adjustment, it does appear to discriminate differences in risk of SSI (Figure 3), and although it does not explain all variation in risk, it is a better indicator of risk than wound classification (Culver et al, 1991; Freidman et al, 2007). More complex systems of risk adjustment have been recommended for some types of surgery (Rosso and Spelman, 2002; Neumayer et al, 2007), however, any form of risk index stratification is dependent on data being available for all three variables and practical problems emerge when incomplete data is captured as part of a surveillance programme. These issues will be covered in more detail in Part 2.
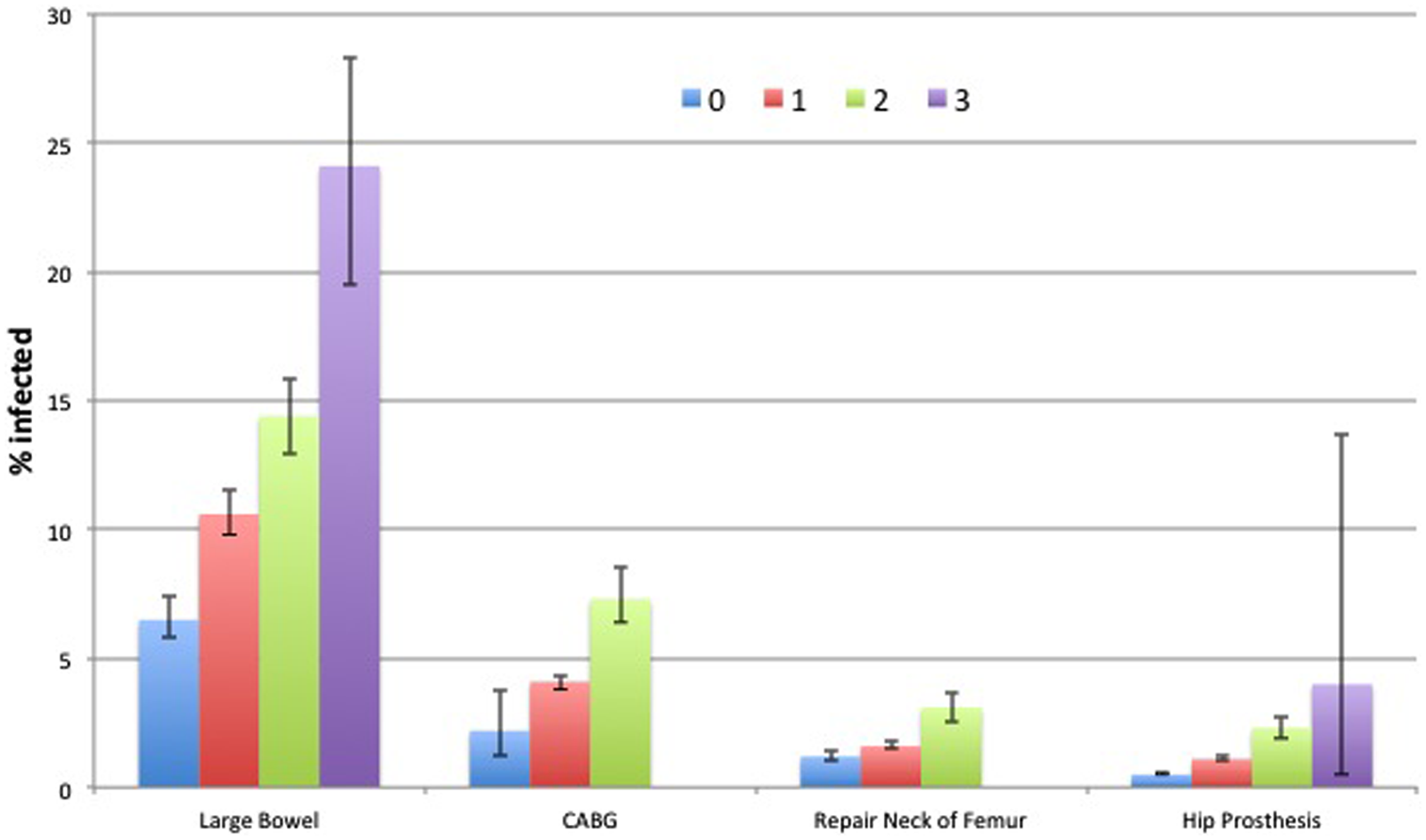
Trends in rates of surgical site infection by National Nosocomial Infection Surveillance System risk index group with 95% confidence limits by category of procedures. Source: HPA, 2011b
There is evidence that other factors increase the risk of SSI. In particular the risk significantly increases with age, obesity, diabetes, peripheral vascular disease and malnutrition (Kaye et al, 2005; National Collaborating Centre for Women’s and Children’s Health, 2008; Neumayer et al, 2007; HPA, 2011a). However, as most of these factors are captured in an ASA score of 3 or more there may be little additional benefit in capturing detailed data on each one. Since the standard approach to SSI surveillance requires detailed risk factor data to be collected on each patent included in the denominator in addition to prospective methods of case finding, it is particularly resource intensive. One way to reduce the time taken to undertake SSI surveillance has been proposed by the European Centre for Disease Control (ECDC) in its new protocol for SSI surveillance. This provides a ‘light’ option where risk factor data are not captured and rates are calculated using an aggregate denominator for the hospital or surgical unit (ECDC, 2012). An aggregate denominator determining eligible procedures undertaken during a defined period can be obtained from the hospital patient administration system, and surveillance effort can therefore focus on identifying patients who develop an SSI that meets the case definitions. This approach may be very valuable in providing ongoing feedback on changes in rates of SSI that could be used to trigger more detailed investigations where results indicate this may be necessary. However, risk adjusted rates may be more appropriate when surveillance is initiated to address concerns of surgical teams of the impact of risk factors on their rates of SSI.
Validation of surveillance data
Reliability of surveillance methods to accurately determine the denominator and numerator is desirable if surveillance data is to be trusted by surgical teams and effectively support decision making in relation to infection control practice. Some national surveillance systems have established mechanisms of validating data capture systems in participating hospitals (Huotari et al, 2007). For example, in the Netherlands hospitals are required to undergo a one-day onsite validation visit every three years when the data collection methods are assessed by a structured interview and case finding validated by a review of medical records (Manniën et al, 2007).
In conclusion, SSI accounts for a major proportion of HCAI and yet many hospitals have little data on the risk of SSI in patients undergoing surgery and therefore offer little assurance about the quality of infection control in their operating departments. The direct costs of SSI are significant and it is associated with considerable morbidity and mortality. There is considerable evidence that surveillance and feedback of rates of SSI contribute to reduction in rates particularly when combined with benchmarking. However, surveillance systems must incorporate robust systems for capturing accurate denominator data on patients undergoing surgery within specified categories and active case finding systems to ensure detection of SSI, including those that develop after discharge from hospital.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interests
None declared.