
Abstract
Nosocomial pneumonia is common in critically ill patients and is associated with high mortality rates. The development of pneumonia in the intensive care unit (ICU) has been associated with bacterial colonisation within the oral cavity and translocation into the respiratory tract. Over recent years, several strategies have been employed and recommended for preventing ventilator associated pneumonia in the ICU. Chlorhexidine, a topical antiseptic, is a promising agent in preventing nosocomial pneumonia because of its wide antimicrobial spectrum of activity, ease of administration, minimal concerns of contributing to bacterial resistance and relatively benign side effect profile. To evaluate the safety and efficacy of chlorhexidine in preventing nosocomial pneumonia in critically ill patients, we conducted a literature search by using PubMed, EMBASE, CINAHL, Web of Science, and MEDLINE databases; Google Scholar, and the Cochrane Central Register of Controlled Trials (1966– February 2013) for relevant studies. Overall, seven clinical trials were identified. These studies showed mixed results and the majority failed to demonstrate a significant reduction in the incidence of nosocomial pneumonia with the use of chlorhexidine. However, the cardiothoracic surgery ICU patient population may benefit from its use. Further studies are warranted to clearly define the role of chlorhexidine in preventing nosocomial pneumonia.
Introduction and background
Ventilator associated pneumonia (VAP) is one of the most common nosocomial infections in the intensive care unit (ICU) (Safdar et al, 2005). In mechanically ventilated patients, VAP accounts for about 90% of all infections (Cook et al, 1998). The overall incidence occurs in 7–40% of ICU patients, translating into a rate of 14.8 cases per 1,000 ventilator-days or 5–10 episodes per 1,000 hospital admissions (Cook et al, 1998; Safdar et al, 2005). The daily risk for developing VAP peaks at about 3% /day during the patient’s first five days in the ICU, decreases to about 2% /day for the second week and is approximately 1% /day throughout the remainder of the patient’s ICU stay (Cook et al, 1998).
Significant deleterious outcomes including increased risk of morbidity and mortality have been associated with VAP. Crude mortality rates have been reported to reach 50–70%, but the increased risk of mortality attributable to VAP has been estimated at approximately 33% (Heyland et al, 1999; Safdar et al, 2005). Ventilator associated pneumonia has a significantly higher death rate compared with community, hospital acquired, and healthcare associated pneumonias (Kolleff et al, 2005). However, some studies have not corroborated these findings of increased mortality risk associated with VAP (Baker et al, 1996; Papazian et al, 1996). Medical ICU patients with VAP have been shown to have significantly increased mortality compared with surgical or trauma critically ill populations (Magret et al, 2010; Heyland et al, 1999). Other negative outcomes resulting from VAP include increased ICU stay, hospital stay, mechanical ventilation duration, and increased resource utilisation (Cook et al, 1998; Safdar et al, 2005). The treatment costs of an episode of VAP have been estimated to range from $10,000 to >$75,000 (£6,500 to >£49,000; ₤7,700 to >₤58,000) and primarily attributed to increased ICU length of stay (Heyland et al, 1999; Safdar et al, 2005; Restrepo et al, 2010).
The definition of VAP signifies a nosocomial pneumonia developing ≥48 hours after endotracheal intubation, which was not incubating upon hospital admission or prior to intubation (American Thoracic Society, Infectious Diseases Society of America, 2005). While healthcare professionals have relatively accepted this broad definition, establishing an accurate diagnosis of VAP remains difficult and controversial. Consequently, several proposed strategies have targeted a clinical diagnosis of suspected VAP, which include the Johanson method, clinical pulmonary infection score (CPIS) as well as the Centers for Disease Control and Prevention criteria (Table 1) (Klompas, 2007; Rea-Neto et al, 2008). However, the clinical signs and symptoms comprising the diagnostic criteria for VAP are nonspecific (Rea-Neto et al 2008; Wiener-Kronish and Dorr, 2008). Alternatively, bacteriological techniques may be utilised to diagnose VAP (American Thoracic Society, Infectious Diseases Society of America, 2005). Major limitations with solely depending upon microbiological data to establish a diagnosis involves the culture technique, cutoff values for quantitative samples, and the time delay associated with the reporting of final culture results (American Thoracic Society, Infectious Diseases Society of America, 2005). Unfortunately, neither the clinical nor microbiological approach alone is considered ideal or reliable in providing an accurate diagnosis with relatively high sensitivity and specificity (American Thoracic Society, Infectious Diseases Society of America, 2005). Although published guidelines recommend a combined strategy in diagnosing VAP, a universally accepted ‘gold-standard’ using established clinical and microbiological objective criteria remains elusive (American Thoracic Society, Infectious Diseases Society of America, 2005).
Comparison of various ventilator associated pneumonia diagnosis definitions.
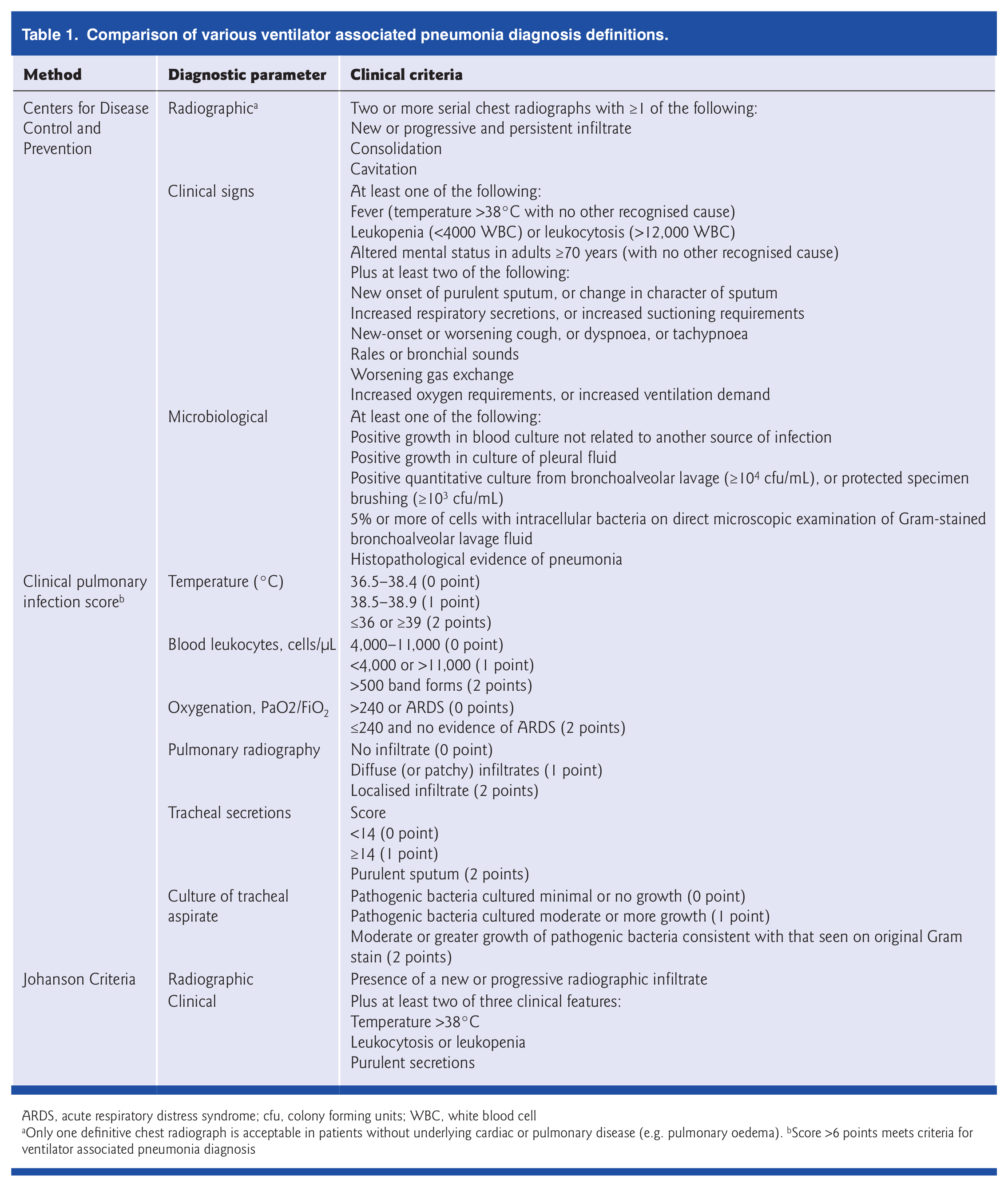
ARDS, acute respiratory distress syndrome; cfu, colony forming units; WBC, white blood cell
Only one definitive chest radiograph is acceptable in patients without underlying cardiac or pulmonary disease (e.g. pulmonary oedema). bScore >6 points meets criteria for ventilator associated pneumonia diagnosis
Non-pharmacologic and pharmacologic strategies have been proposed to prevent VAP (American Thoracic Society, Infectious Diseases Society of America, 2005; Muscedere et al, 2008). These strategies include patient positioning techniques (head of bed elevation to 45°, rotating beds, etc), physical prevention techniques (orotracheal intubation route, closed endotracheal suctioning system, subglottic suctioning, etc.), as well as inhaled, intravenous, and topical prophylactic antibiotics (American Thoracic Society, Infectious Diseases Society of America, 2005; Muscedere et al, 2008; O’Grady et al, 2012). Also, oral antiseptics including chlorhexidine have shown some promising results in preventing VAP (Muscedere et al, 2008). A positive side effect profile, broad spectrum of activity and low cost make chlorhexidine an attractive option in preventing VAP. The implementation of chlorhexidine use as a component of the ‘ventilator bundle’ within healthcare institutions is gaining recognition (Morris et al, 2011). The Institute for Healthcare Improvement (IHI), an independent, non-profit organisation promoting best practices in healthcare systems, also endorses its use (O’Grady et al, 2012). However, the overall consensus from several published clinical guidelines on the routine use of chlorhexidine oral care in ICU patients remains equivocal (American Thoracic Society, Infectious Diseases Society of America, 2005; Muscedere et al, 2008). The purpose of this review was to evaluate the clinical efficacy and safety of oral chlorhexidine in preventing VAP.
Methods
We performed a systematic review of the literature by using the PubMed, EMBASE, CINAHL, Web of Science, and MEDLINE databases; Google Scholar, and the Cochrane Central Register of Controlled Trials. Our search was limited to English, human, and clinical trial published between January 1966 and February 2013 using the terms respiratory infection, nosocomial infection, pneumonia, ventilator-associated pneumonia, antiseptic, decontamination, chlorhexidine, intensive care unit, critical care, AND critical illness. The overall search strategy was to identify clinical studies evaluating the use of oral chlorhexidine in the prevention of VAP. Articles meeting the following criteria were included in this review: study design was prospective, randomised, double-blind, controlled clinical trial; subjects included the adult patient population ≥18 years; chlorhexidine was orally administered; and either nosocomial pneumonia or nosocomial infection rates were reported. Abstracts were excluded as well as studies that exclusively administered topical chlorhexidine outside the oropharyngeal cavity. Two investigators independently identified the titles and abstracts of potentially eligible studies. Articles with indeterminate abstracts or potentially meeting our criteria were obtained for full manuscript review and evaluated for our inclusion criteria. The references of all identified articles were also manually searched to identify additional studies. The literature search yielded 35 potential articles, seven met the inclusion criteria and were reviewed (Figure 1). A summary of the clinical trials included in this review are shown in Table 2.
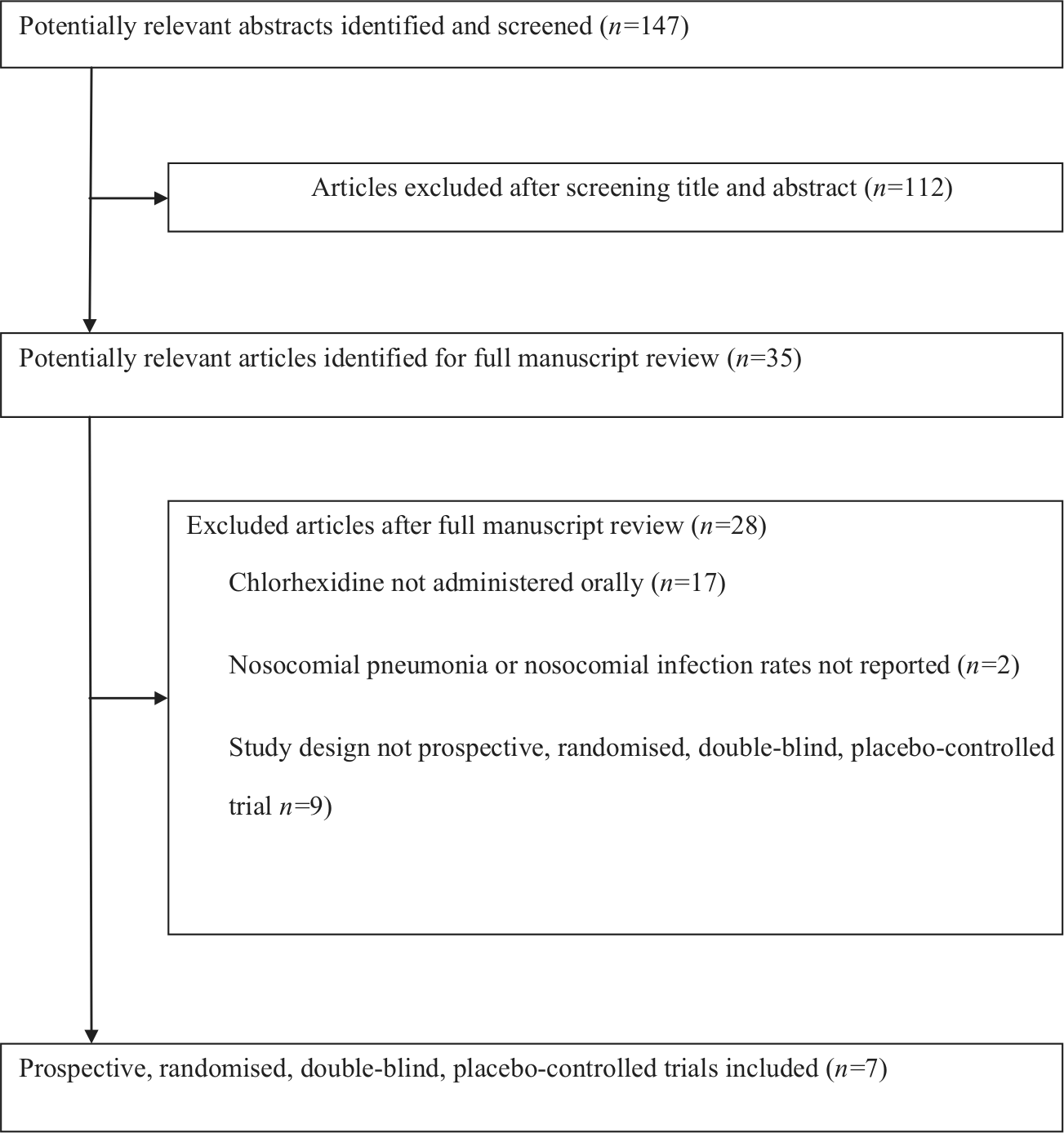
Literature search strategy.
Summary of prospective, randomised, double-blind, clinical trials using chlorhexidine for ventilator associated pneumonia prevention.
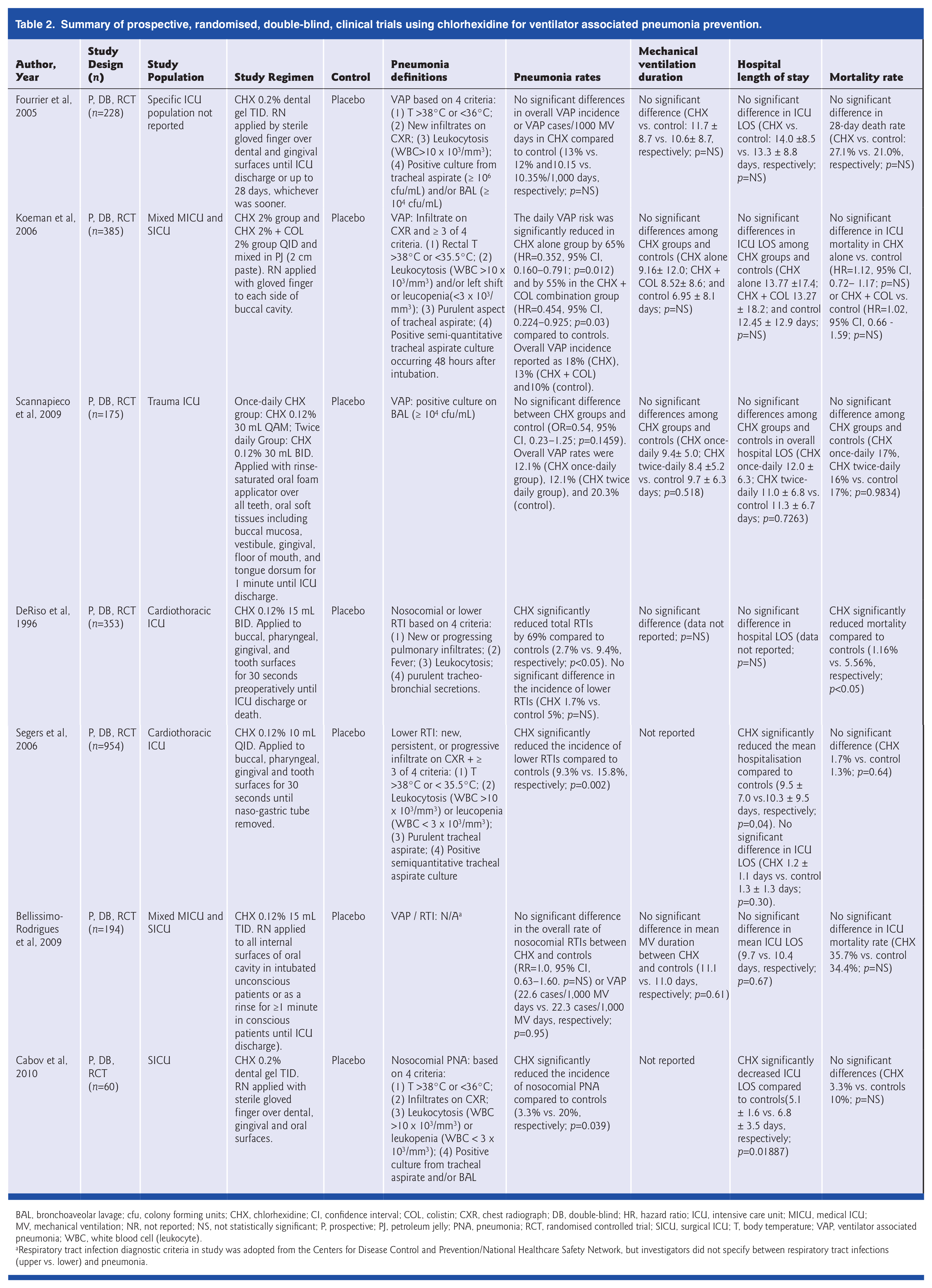
BAL, bronchoaveolar lavage; cfu, colony forming units; CHX, chlorhexidine; CI, confidence interval; COL, colistin; CXR, chest radiograph; DB, double-blind; HR, hazard ratio; ICU, intensive care unit; MICU, medical ICU; MV, mechanical ventilation; NR, not reported; NS, not statistically significant; P, prospective; PJ, petroleum jelly; PNA, pneumonia; RCT, randomised controlled trial; SICU, surgical ICU; T, body temperature; VAP, ventilator associated pneumonia; WBC, white blood cell (leukocyte).
Respiratory tract infection diagnostic criteria in study was adopted from the Centers for Disease Control and Prevention/National Healthcare Safety Network, but investigators did not specify between respiratory tract infections (upper vs. lower) and pneumonia.
Findings – clinical efficacy
Dental plaque and oral colonisation
Formation of dental plaques and subsequent oral colonisation may serve as a nidus for the development of VAP in mechanically ventilated patients (Fourrier et al, 2005). Up to 38% of patients are colonised with aerobic bacteria upon admission into the ICU with a significant increase in the amount of dental plaque developing during an ICU stay (Fourrier et al, 2005). Efforts to reduce dental plaque formation and oral colonisation in ICU patients with chlorhexidine have yielded mixed results on overall rates of pneumonia (Fourrier et al, 2005; Scannapieco et al, 2009).
Fourrier et al (2005) conducted a randomised, controlled, multi-center study designed to establish the impact of dental plaque decontamination with chlorhexidine on pneumonia rates (Fourrier et al, 2005). Patients were included if their expected length of ICU stay was five days or more and required mechanical ventilation. This study failed to demonstrate a statistically significant reduction in ICU acquired nosocomial infections or VAP rates in the chlorhexidine treated patients as compared with controls. There was no significant difference between chlorhexidine and placebo groups on the dental plaque colonisation rates at baseline or on study day #5. Interestingly, in those subjects with dental plaque sampling data up to study day #10 who had a positive culture at baseline, the incidence of these cultures remaining positive on day #10 was significantly lower in the chlorhexidine group compared to placebo (29.0% vs. 65.6%, respectively; p<0.05). Although this study showed decreased dental plaque colonisation after 10 days of chlorhexidine prophylaxis, this did not translate into lowered VAP rates.
Another randomised, placebo controlled study was conducted that evaluated the reduction of oral colonisation by respiratory bacterial pathogens through the comparison of chlorhexidine to placebo. This study enrolled trauma patients expected to receive mechanical ventilation for ≥48 hours (Scannapieco et al, 2009). The use of chlorhexidine reduced the number of colony forming units of S. aureus on dental plaque, but there was no significant reduction in total respiratory bacterial pathogen counts between the groups. Chlorhexidine also did not reduce the incidence of pneumonia as compared with controls.
Cardiothoracic surgery patients
DeRiso and colleagues (1996) evaluated patients undergoing coronary artery bypass graft (CABG), valve surgery, septal surgery, cardiac tumour excision or combined CABG/valve surgery. Chlorhexidine was superior to placebo in several of the outcomes measured. Overall total respiratory tract infection rates (upper and lower airway combined) were significantly reduced in the chlorhexidine group. In addition, the number of patients who developed an infection was reduced in the chlorhexidine group by 65% and required less non-prophylactic antibiotics. Chlorhexidine reduced Gram negative organisms identified by culture, but did not impact Gram positive or fungal organisms. Although a mortality benefit was seen, patients were selected for infection risk, not mortality risk; therefore, further study is needed to investigate chlorhexidine’s impact on mortality.
The most recently published trial in cardiac surgery evaluated chlorhexidine’s impact on nosocomial infection (Segers et al, 2006). Although the study cites nosocomial infection as defined according to criteria for the Centers for Disease Control and Prevention, pneumonia was not differentiated from other lower respiratory tract infections, such as tracheobronchial infections without pneumonia. The incidence of lower respiratory tract infections was significantly lower in the chlorhexidine group than the placebo group. Staphylococcus aureus nasal carriage was significantly reduced with chlorhexidine from 35.5% at admission to 15.5% at the time of operation (p<0.001). Upon discharge, this rate was increased to 21.2%. Positive cultures did not differ upon admission compared to discharge in the placebo group. No differences in resistant organisms, ICU length of stay, adverse drug reactions, surgical site infections or mortality between study groups were observed.
Overall, there have been two major trials using chlorhexidine in cardiothoracic surgery patients. Both trials showed a significant reduction in respiratory tract infection rates. Although one of the trials found a significant total respiratory tract infection rate reduction with chlorhexidine, significance was lost when analysing only lower respiratory tract infections, which would be more consistent with pneumonia (DeRiso et al, 1996). Only one study evaluated adverse drug events, which reported only one patient developing minor temporary tooth discolouration (Segers et al, 2006).
Medical and surgical ICU populations
Koeman et al (2006) studied the effects of oral decontamination on time to developing VAP, using chlorhexidine or chlorhexidine plus colistin paste compared with placebo. This robust trial showed a significantly lower risk of VAP in both the chlorhexidine alone and chlorhexidine with colistin groups compared with placebo. The combination chlorhexidine and colistin group was more effective against Gram negative colonisation than chlorhexidine alone. The investigators confirmed the diagnosis of VAP by calculating a corresponding CPIS as well as having independent experts verify the diagnosis, which were major study strengths. However, the VAP episodes were not adjusted for mechanical ventilator days so it remains speculative if ventilation duration differences among study groups biased the results.
Another trial evaluated the impact of chlorhexidine gel on overall nosocomial infections as well as nosocomial pneumonia in the surgical ICU (Cabov et al, 2010). In addition to lower rates of nosocomial pneumonia, chlorhexidine compared with placebo significantly reduced nosocomial infections (6.7% vs. 26.7%, p=0.0418; respectively). Furthermore, this study was the only clinical trial to demonstrate a significant reduction in mean ICU length of stay with chlorhexidine vs. placebo. Although the investigators did not report subjects’ baseline risk factors for developing pneumonia or comorbidities, chlorhexidine was shown to impressively decrease nosocomial pneumonia rates.
Bellissimo-Rodrigues et al (2009) investigated overall respiratory tract infections as well as VAP rates with chlorhexidine compared with placebo. Although evaluating respiratory tract infections may not be the most ideal endpoint, because this may not accurately reflect pneumonia from other infectious processes, the investigators separately analysed VAP rates. Chlorhexidine was not found to significantly lower the incidence of either clinical endpoint.
Safety and tolerability
Overall, chlorhexidine is well tolerated with minimal adverse drug events. As expected, due to the minimal systemic absorption, the side effect profile is positive relative to other antimicrobials. Adverse effects reported include unpleasant taste, dysgeusia, mild oral mucosa irritation and staining of teeth. All of these adverse effects were reversible (Segers et al, 2006; Bellissimo-Rodrigues et al, 2009). There is a lack of significant safety and tolerability concerns about the use of chlorhexidine; therefore, the benefit to risk ratio favours its use in the prevention of VAP as supported by the side effect profile.
Discussion and chlorhexidine role in therapy
Numerous clinical trials have evaluated the use of chlorhexidine in preventing VAP. The contrasting results from these studies warrant further research. Significant variability among these studies may explain these conflicting results. The majority of the studies included a medical or mixed medical-surgical critically ill study population (Table 2). Two studies exclusively included cardiothoracic ICU patients; whereas trauma patients were studied in only one trial. The diagnosis of pneumonia was inconsistently defined among all studies based upon microbiologically confirmed results, radiographic evidence and/or clinical criteria. It is important to emphasise that the chlorhexidine regimens varied with regard to concentration, frequency, administration technique, and duration. These inconsistencies may have contributed to mixed study results. Unfortunately, most studies failed to disclose other VAP preventative measures employed during the study, including head-of-bed elevation, subglottic suctioning, stress ulcer and venous thromboembolism prophylaxis. The majority of clinical trials investigating chlorhexidine in preventing nosocomial pneumonia were largely underpowered. A large number of these trials did not have an adequate sample size; therefore, inconclusive findings may have been a result of type II error. Interestingly, all three trials reporting power analyses and meeting adequate sample size did not show any significant reduction in VAP with chlorhexidine (Fourrier et al, 2005; Bellissimo-Rodrigues et al, 2009; Scannapieco et al, 2009). As previously mentioned, two studies found a significant reduction in respiratory tract infections (DeRiso et al, 1996; Segers et al, 2006). However, it is important to note that a respiratory tract infection is not synonymous with pneumonia. Overall, five studies specifically assessed nosocomial pneumonia rates as an endpoint (Fourrier et al, 2005; Koeman et al, 2006, Bellissimo-Rodrigues et al, 2009; Scannapieco et al, 2009; Cabov et al, 2010). Only two of these trials found a significant reduction with the use of chlorhexidine over placebo (Koeman et al, 2006; Cabov et al, 2010).
The conflicting clinical data pose a challenge to clinicians about whether to implement widespread use of chlorhexidine in their respective institutions. Widespread use should be discouraged in the ICU patient population, because a clear benefit has not been firmly established and clinical practice guidelines recommend against its routine use. Nonetheless, the reality remains that many healthcare institutions in the United States are using this agent given the potential beneficial effects over its relatively benign side effect profile and low cost. Based upon the clinical data, the cardiothoracic ICU patients expected to require mechanical ventilation for >48 hours have been shown to benefit most. Being the most commonly studied regimen, it seems reasonable to use chlorhexidine 0.12% (10–15mL) applied at least twice daily to the buccal, pharyngeal, gingival and tooth surfaces. Also, it may seem feasible to use chlorhexidine for the entire time the patient requires mechanical ventilation although the optimal duration of use remains debatable. Therefore, the overall use of chlorhexidine in preventing VAP should only be considered rather than recommended in the ICU patient population.
Conclusion
Ventilator associated pneumonia is a common occurrence in critically ill patients and is associated with an increased risk of mortality and morbidity. Oral decontamination with chlorhexidine in mechanically ventilated patients has been recognised as a potential preventative strategy. Several clinical trials have shown discordant results on lowering the incidence of VAP in critically ill patients. Healthcare improvement organisations consider chlorhexidine as standard practice in preventing VAP despite lacking robust data supporting its use and clinical guidelines recommending against it. The widespread use of chlorhexidine in mechanically ventilated patients to prevent VAP remains controversial. However, cardiothoracic ICU patients may benefit. Further studies are needed to define the role of chlorhexidine and identify the optimal regimen.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The author(s) declare that there is no conflict of interest.