
Abstract

Having decided that the topic for Outbreak Column 12 would be Staphylococcus aureus the problem came in deciding where to start, what to include and what to omit. It soon became clear that one column would not suffice. Therefore this is the first column which looks back at some early work; the second will discuss outbreaks, guidance evolution and the current situation. This has been a difficult challenge. Trying to produce useful Outbreak Columns on nosocomial outbreaks of S. aureus is like trying to describe the world’s weather in a very short synopsis. Having got the defeatist part over, I will attempt to highlight valuable information for those who work in infection prevention and control (IPC) in clinical settings where this commensal and sometime pathogen has been and remains a constant companion and threat.
I have left the title bland so as to include any strain of S. aureus regardless of resistance pattern and virulence. The column was going to do the usual, extract useful information from outbreak reports and relate this to implications for practice. However, I have been drawn to explore what I shall call the ‘Wyllie conundrum’. In my search for useful reports to include I found a paper which suggests that reductions in meticillin resistant Staphylococcus aureus (MRSA) began before efforts at control were introduced. Obviously, this needed to be explored before any advice on the control of outbreaks of S. aureus could be offered.
The Wyllie conundrum
One recent interpretation of the MRSA story is puzzling. Wyllie et al (2011) analysed Oxford Hospitals’ specimen data from 1998 to June 2010. They found that MRSA rates rose rapidly from 1998–2003, and then declined. The decline accelerated from mid-2006. Rates of meticillin sensitive Staphylococcus aureus (MSSA) changed little. The conclusion of this paper is that: ‘MRSA isolation rates were falling before recent intensification of infection-control measures.’ Further the authors ‘strongly suggest’ that along with strain specific changes much of the recent variation in MRSA can be attributed to incompletely understood biological factors. In addition, the authors stated that: ‘We find it difficult to estimate how much, if any, of the observed decline in MRSA isolations is attributable to recent infection-control measures’ (Wyllie et al, 2011). There will be many specialists in IPC who will be outraged by this statement; surely the, in some cases, career-long efforts must have made a detectable impact. So where to start to look for evidence that IPC contributes to the control of epidemic S. aureus?
Staphylococcus aureus (MRSA and MSSA) – what is included in the problem space?
The narrative on what is happening, or has happened, with S. aureus epidemiology in any clinical setting(s) will vary depending on how far back you look, how wide is the geographical focus, how many strains you include, how and what you count and finally, and probably most importantly, the continuously evolving systems of healthcare. For example:
The review period could include: weeks, months, recent years (since 2000), or be more in-depth to include from the 1980s or further back to include outbreaks arising during and shortly after the second world war.
The geographical areas could include: individual clinical areas/wards, multiple clinical areas, directorate(s), hospital(s), board(s)/trust(s), or more widely include region(s), country (within UK), UK, Europe-wide, other continents or the world.
The data could include: incidence, prevalence, or both; all specimens or only selected specimens and all or selected MRSA/MSSA strains.
The system could include: people (including their interconnections), environment, equipment, methods and information used, and availability to deliver care in the relevant time periods/geography.
The early years…
I am privileged to be the custodian of a series of early HMSO pamphlets on the Control of Cross Infection in Hospitals (Figure 1). The first published in 1944, (price 6d) provides general infection control advice before listing the conditions/organisms for which ‘additional special precautions’ are required, i.e. the Transmission Based Precautions list of 1944. This War Memorandum (No. 11), was prepared ‘in the hope that in the face of all the present difficulties, some attempt would be made to reduce the incidence of infections contracted unnecessarily in hospital’ (Harries et al, 1944).
Early pamphlets providing national guidance on infection control in hospitals.
The general measures in the 1944 pamphlet included the oiling of floors to matt the dust that contained organisms and prevent them from recirculating in the air (Harries et al, 1944). Blankets could also be impregnated with ‘technical white oil’ to reduce the number of bacteria scattered from them (Harries et al, 1944). The alert organisms and conditions requiring the ‘additional precautions’ were listed as: Haemolytic Streptococcus Infection, Diphtheria, Measles, Pertussis, Gastro-enteritis of Infants, Epidemic Diarrhoea of the Newborn, Dysentery, Paratyphoid, Typhoid and Food-poisoning, Chicken-pox, Herpes zoster, Rubella or Mumps or Vulvo-vaginitis’ (Harries et al, 1944). The historically important omission here – due to either its insignificant healthcare presence or a failure to recognise its nosocomial origin – was S. aureus.
The Control of Infection in Hospitals (War Memorandum No. 11) was updated and reissued in 1951 (now costing 1s 9d) (Harries et al, 1951). The alert organism and condition list in this version is unchanged from the 1944 text with the addition of ‘Pemphigus neonatorum’, for which a mention of staphylococcus was included: ‘When isolated cases or outbreaks occur, it must be borne in mind that staphylococcal conjunctivitis (‘sticky eye’) and Pemphigus neonatorum are both manifestations of staphylococcal infection’ (Harries et al, 1951). That was the only mention of staphylococcus in the updated guidance. Even in a section on wound infection (p. 9) there is no mention of S. aureus. However by 1959, something had changed, which necessitated the production of a report dedicated solely to the organism, entitled ‘Staphylococcal Infections in Hospitals’ (Sub-Committee of the Standing Medical Advisory Committee, 1959) (2s 6d). The object of the report was: ‘To draw attention to the prevalence of staphylococcal disease in hospitals’ (Sub-Committee of the Standing Medical Advisory Committee, 1959). Ergo, the importance of S. aureus changed from absence in 1944, to a brief mention in 1951, to the requirement for deliberations of a specialist sub-group of the Standing Medical Advisory Committee of the Ministry of Health in 1959. Staphylococcus aureus had arrived in hospitals. It will not have escaped the reader’s notice that the first infection control nurse was also appointed in 1959.
What happened was summarised by Williams (1959), in what must have been a state of the art paper on epidemic staphylococci. He reported on 32 epidemics of staphylococcal infection in maternity hospitals and 15 surgical wards between 1954 and 1957 that ‘emphasise the frequency with which epidemic spread had been attributed to a particular dangerous carrier – either a person with a septic lesion or a healthy carrier’ (Williams, 1959). This was perhaps the most important issue in shaping the guidance that appeared in the 1980s and 1990s. However there were also other outbreaks reported where it was not possible to identify one individual as the source of the outbreak. Results of phage-typing found that over 50% of the recognised epidemic spread was due to just six phage types (Williams, 1959).
Some of the key statements from the Sub-Committee report (1959) are noted below:
The control of staphylococcal disease depends largely on the application of aseptic methods. The use of antibiotics either for treatment or for prophylaxis, is by itself unreliable.
Staphylococcal infection may give rise to disease in any department in the hospital. It is particularly troublesome in the surgical and maternity units.
The need for voluntary reporting of minor ailments including septic lesions of the skin should be impressed on all members of the hospital staff.
Records of clinical evidence of infection should be maintained in a simple, comprehensive and readily available form.
The hospital Control of Infection Committee should meet regularly to review the sepsis record
(Sub-Committee of the Standing Medical Advisory Committee, 1959).
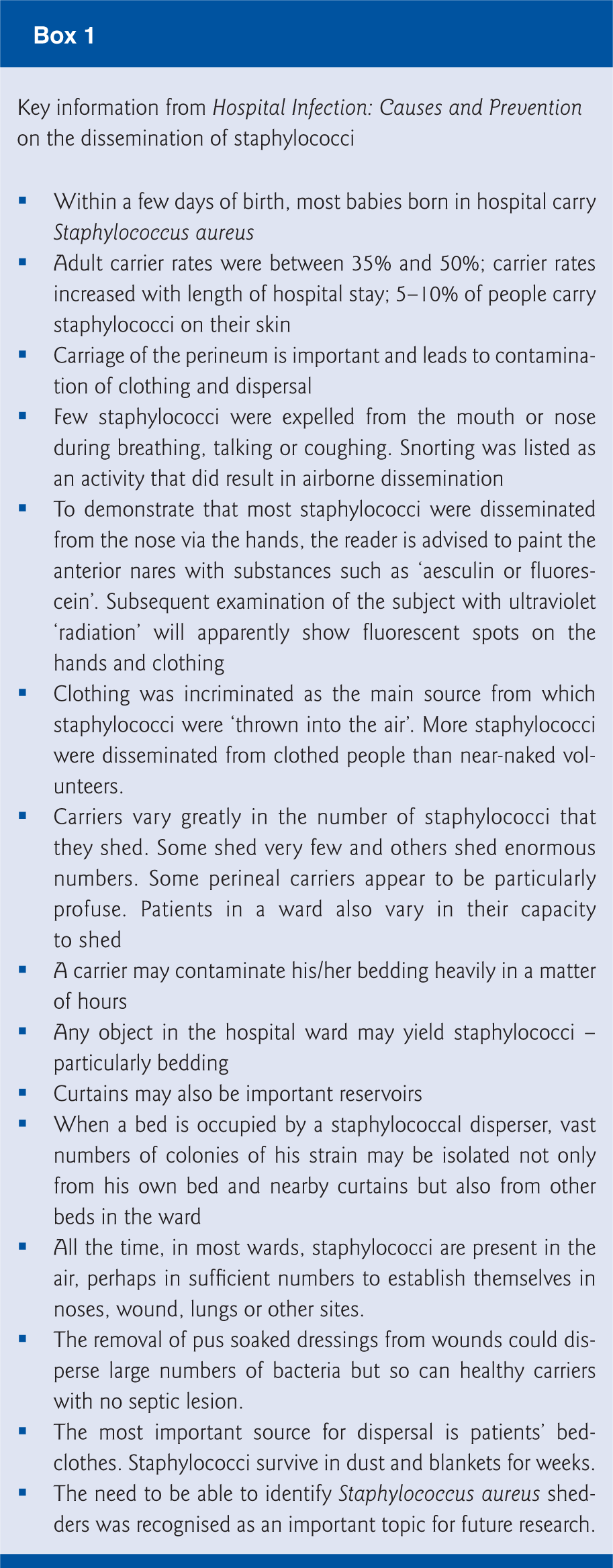
Further evidence that presence of S. aureus was not always a ubiquitous infection control challenge is provided in a book by Williams et al (1960), who state: ‘In the last 20 years the staphylococcus has replaced the streptococcus as the chief cause of infection in maternity units, and with the change of organism there has been a change from mother to baby as the chief victim’ (Williams et al, 1960, p. 44). However, as the problem of S. aureus was being recognised there was puzzlement because of the uncertainty as to whether it was new, or merely newly recognised. ‘… if the present concern over its frequency is due to an actual increase or to the recent appreciation of a long-standing problem thrown into light by a decline in streptococcal sepsis’ (Williams et al, 1960, p. 63). This early infection control tome on hospital infection, its causes and prevention provides some useful information as to what was and was not known about S. aureus at the time; in particular about the dispersal within a clinical environment (Box 1) (Williams et al, 1960).
Williams et al (1960) stated that ‘the term ‘Staphylococcus aureus’ or ‘staphylococcus’ used throughout their book referred to staphylococci (with golden or white colonies) able to form coagulase (p. 24).
Williams et al (1960) note that phage typing had been available since 1945 to distinguish between strains of staphylococci. Phage-typing divided staphylococci into four main groups, which behaved differently. Strains responsible for minor septic lesions developing in the community belonged to phage group II. This included up to 70% of staphylococci from acute cases of impetigo. Phage group III contained the majority of staphylococci that had been responsible for food poisoning. Group III strains acquired most resistance to antibiotics, other than penicillin (Williams et al, 1960).
The epidemic strain which was prevalent in Britain, America and Australia at that time was known as phage-type 80/81 (Williams, 1959). This strain gave rise to more outbreaks than any other strain (Williams, 1959). However other strains did cause outbreaks. In surgical units epidemics of group III strains included 47/53/75/77, 75/77, 83A and group I 52/52A/80 (Williams et al, 1960). Most research on S. aureus was undertaken in the clinical areas of concern – the maternity and surgical wards. It was shown that the epidemic strains could be present in the absence of epidemics (Williams et al, 1960). One of the book’s authors quotes his own study which found 186 different strains of staphylococci isolated from a surgical ward over an 8.5 month period (Williams et al, 1960). Of import, only 13 of these strains were responsible for ‘any observable clinical sepsis’ and only three were responsible for sepsis in more than one patient (Williams et al, 1960). Staphylococcus aureus was everywhere, but at times did relatively little damage. In a useful synopsis the authors conclude that ‘There was nothing to suggest that lack of sepsis with some strains could be explained by a lack of opportunity’ (Williams et al, 1960, p. 29). Additionally, they found that three of the strains that were present in the ward almost throughout the period, often in large numbers, were among the strains not responsible for any sepsis. Under good nursing conditions it seemed to the authors that only a few strains would cause sepsis (Williams et al, 1960).
Williams et al (1960) argued that there was little evidence to back up the assertion that phage type 80/81 was deriving its virulence from its resistance. Some strains of S. aureus colonised and rarely caused lesions, others were common in the nose and produced sporadic lesions but rarely epidemics, and a few strains caused both sepsis and were communicable. There is much talk of septic lesions in both patients and staff on the wards in these reports (Sub-Committee of the Standing Medical Advisory Committee, 1959; Williams et al, 1960). In recent research it has been discovered that the community-acquired MRSA carrying the Panton-Valentine leucocidin gene, which are also famed for skin and soft tissue infections, were genetically descended from the early phage type 80/81 (Robinson et al, 2005). Other researchers have reported similar findings.
Staff carriage was a significant problem. Williams et al (1960) report that during epidemics, staff carriage had been reported as high as 73%; however, in other outbreaks, investigators did not find any carrier state. Williams et al (1960) also report on the discoveries that implicated asymptomatic surgeons or people circulating in the operating theatre as being the source of outbreaks. It is not surprising therefore that it was stated for surgeons with an active lesion ‘even a minor one can infect his patients’ (p. 74). One report of an outbreak of wound infections (80/81) identified the source as a theatre orderly who suffered from a dry generalised eczema (Ayliffe and Collins, 1967).
What is important to consider is the circular nature of the problem:
Prevalent strains of staphylococci including the notorious antibiotic resistant 80/81 resulted in high prevalence of carriage and in skin and soft tissue infections among staff as well as patients
Skin and soft tissue infections and high-carriage rates resulted in vast numbers of staphylococci being disseminated into the healthcare environment
The environment and healthcare procedures exposed patients to carriage
The invasive procedures performed by staff with carriage and lesions resulted in more patients becoming infected and a high prevalence on the wards
A similar circle can be drawn for maternity units.
Maternity units
In maternity units in the mid-1950s it was concluded from the available data that even in the absence of a recognised epidemic it was not uncommon for 10–20% of babies to develop skin lesions or sticky eye while in hospital and that the incidence of breast abscess (usually to mothers who breast fed) was at least 1–2%. When epidemics occurred and were reported, rates of between 7% and 29% were recorded (Williams et al, 1960, p. 64). Such was the state of surveillance, or non-surveillance, the use of sepsis registers and the local interpretation of sepsis itself, that the authors commented, ‘it is tempting to believe that an outbreak of sepsis is sometimes no more than the sudden recognition of a state of affairs that had long existed’ (Williams et al, 1960, p. 65).
There was excellent research at that time which identified how the dissemination of staphylococci occurred in hospitals – particularly coming from bedding (Box 1). However, the system to prevent or minimise this dissemination can only be described as insufficient: ‘Sheets and other cotton goods are washed at the laundry at a temperature which will kill staphylococci. Blankets and woollen articles, on the other hand are thought to be damaged at high temperatures and are therefore frequently washed at a temperature which will not kill all the staphylococci they contain’ (Williams et al, 1960, p. 38). There is a problem here with the use of the term ‘frequently’; because the washing of blankets places ‘a great burden on the laundry and increases the washing and depreciation costs’, it was recommended that ‘hospital bedding be washed and disinfected at regular intervals, say, four times a year, or whenever it is soiled’ (Williams et al, 1960, p. 205). The 1959 pamphlet did advise that blankets be laundered, ‘at least with each change of occupant of a hospital bed or cot, by a process which effectively reduces the bacterial load which they carry’ (Harries et al, 1951). Of note this was a ‘should’ and not a ‘must’.
And then…
So in the midst of (or if you prefer in a mist of) epidemic staphylococcal outbreaks, Williams and Dean (1974) report something remarkable. In the phage-type testing of 4,547 strains of S. aureus, between 1961 and 1972, it was shown that after 1967 there was a decline in the number of infections in hospitals, which was largely accounted for by a great reduction in four ‘epidemic’ types. Multi-resistant staphylococci also declined. The authors stated that ‘One can only speculate on the cause of these changes. An isolation ward was opened in 1961 and was replaced by a larger one in 1966. There was a steady increase in the general “hygienic” facilities in the hospital and latterly in the use of disposable materials. But there was no explicit antibiotic policy.’ Finally the authors pondered that ‘it may be we are going through a fortunate period when there happen to be no very communicable staphylococci in circulation’ (Williams and Dean, 1974). These authors looked at potential changes in infection control per se but did not consider potential changes in healthcare itself that may have accounted for a decline in cross-transmission or cross-infection opportunities.
A series of papers on isolation in the 1970s comment on the decline in incidence but added a cautious note: ‘The virtual disappearance of many infectious diseases had not removed the need to isolate patients. Sporadic cases and occasional outbreaks of the classical infectious diseases do occur’ (Bagshawe et al, 1978a). However, all was not yet perfect. There was an overt defeatist attitude: ‘Precautions against infection are often costly in money and the time of skilled staff and may be exasperating impediments to medical and surgical work’ (Bagshawe et al, 1978a). And although disposables were available the use of the term ‘disposable’ was not as we use it today. In advising glove use because of the deleterious drying effects of hand washing or alcohol on the skin it was recommended thus: ‘Under non-sterile conditions gloves may be washed, more quickly and effectively than the skin without any unpleasant effects on the skin of too-frequent washing’ (Bagshawe et al, 1978b).
In a later work which will be familiar to many mature infection and prevention control teams, Lowbury et al (1988) advocated for patients with staphylococcal infection (sensitive or resistant only to penicillin), ‘No isolation room needed, unless in maternity and neonatal wards’. Isolation was recommended for patients with epidemic strains until ‘the organism is no longer isolated from the lesion’ (Lowbury et al, 1988, p. 143). [This work was reprinted in 1988, the original published in 1981]. The rationale for different precautions for effectively the same organism was also provided: ‘Certain strains of Staph. aureus have a propensity for spreading and causing sepsis in a ward and are known as epidemic strains’ (Lowbury et al, 1988, p. 148). The preceding line to this is also worthy of special note: ‘Except in special units, where staphylococcal infection is still common, Staph. aureus is today less often transmitted in hospital’. To those of us who have fought these beasts for most of our career in any and every clinical area this must seem like a blissful time to have been in infection control – an infection prevention utopia.
In a paper describing MRSA epidemic waves, Chatterjee and Otto (2013), suggest that ‘due to its prominence as a health-care related pathogen, it has been a cause for serious concern for clinicians for over a century’. This statement is referenced to a paper by Lowy (1998) on S. aureus infections in what seems to be a possible misinterpretation. Lowy (1998) comments on Ogston’s observations and discoveries and states that ‘More than 100 years later, Staphylococcus aureus remains a versatile and dangerous pathogen in humans.’ Lowy (1998) did
From 1940s–1980s
In summary thus far, from the 1940s to, and including the early 1950s, S. aureus was not on the radar. It was put on the radar by epidemic strains causing outbreaks principally in maternity and surgical wards in the context of the disappearance of a much more formidable foe – Group A Streptococcus. It is worth asking this: apart from the hospital microbiology what also changed at that time? In the late 1940s healthcare changed fundamentally because it became available to all through the new NHS. Whether this change in access to hospital healthcare brought about a change in hospital microbiology should be explored further (a great topic for a thesis). However, some practices can be assessed today for the potential of increasing the risk of patient harm. The practice of keeping mothers and healthy babies in hospital for 10–14 days for their ‘well-being’ would have exposed them to hospital pathogens. The practice of putting healthy babies in a common nursery (which doubtless would not have had a single wash-hand basin) would surely have ensured effective spread from any one colonised baby. Although in the 1950s knowledge on how staphylococci were being disseminated in the care environment was advanced (Box 1), the ability to control such dissemination and thus prevent outbreaks was primitive. There were wards of a Nightingale design only, there were few cubicles for patients with infections and the blankets were of a material that meant they could not be washed after each patient. Problems of mattress decontamination was recognised but not solved – ‘All other [mattress decontamination methods] present difficulties. Horse hair and flock shrink in steam and springs rust’ (Williams et al, 1960, p. 261). The assessment of the practice of healthcare at that time could be that it aided cross-transmission of pathogens, and the assessment of advocated guidance can only be that it was insufficient to prevent it. I remember as late as 1980, while working at a London hospital, regularly using sleek tape to patch up slits in polyvinyl mattress covers after the discharge of patients – replacement covers were just simply not available.
So the next question is: what changed again to get to Lowbury’s blissful utopia of ‘Staph. aureus being less often transmitted in hospital’ in the early 1980s? The main change was healthcare itself. For example, the practice of putting healthy babies in a common room to share micro-organisms stopped. The healthcare of healthy people moved back to where it belonged – in the community. And gradually in a wealthier post-war Britain there were blankets that could be heat treated after each use, mattresses that could be cleaned after each patient, and new better designed hospitals appeared. The era of the disposables, in the first instance with gloves and aprons, dawned. Other changes which could have impacted are in the circulating strains. Small changes in prevalent strains may also have had a huge effect. A strain prevalent in Glasgow in the 1990s was difficult to initially identify. This undoubtedly facilitated spread within several clinical areas before control measures were instigated. The strain subsequently disappeared as EMRSA15 established itself.
So… how does the above relate to the Wyllie conundrum?
It would appear that waxing and waning of nosocomial S. aureus has occurred in the past. Factors that may have facilitated both its presence and its demise include the system of healthcare as practised and improved over time. My assessment of the infection prevention guidance of the day (c.1940s–1960s) is that even if fully implemented, it would have been insufficient to gain control.
It is possible that S. aureus took over the position vacated by streptococci in post-war Britain, exacerbated by the increase in access to healthcare that was perhaps at that time not quite ready or resourced to cope. Over time with improvements in healthcare and healthcare environments the outbreaks that plagued both surgical and maternity wards reduced. The dreaded phage-type 80/81 had packed its bags as the streptococci had done before. All was relatively quiet until the mid-1980s when along with Wham and Culture Club, new epidemic strains of MRSA emerged.
In Part 2, more recent comings and goings of MRSA and the outbreaks caused will be discussed.
Limitations
This is an Outbreak Column and it does not pretend to be a systematic historical review. Interpretations are, however, made from the national guidance work of the day.
Footnotes
Acknowledgements
I would like to acknowledge Dr GFS Edwards of the Meticillin Reference Laboratory in Scotland for his most wise contribution to this column (and for all the learning he has shared with a very grateful infection control nurse over many years).
Declaration of conflicting interest
The author declares that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.