
Abstract
Background:
e-Bug is an international health education resource which support World Health Organization (WHO) public health recommendations by educating young people about microbes, hygiene and antibiotics use. The e-Bug team collaborated with Kingfisher Treasure Seekers to develop a six-session course for community groups called Beat the Bugs covering: microbes; hygiene; antibiotic use; and self-care. A pilot was used to inform further development and evaluation.
Methods:
Pilot courses with 9–12 adults with learning difficulties and young parents were delivered by community leaders and observed by researchers. Participants completed before and after knowledge questionnaires. Two participant focus groups and two course leader interviews explored views on the course and retention of knowledge.
Results:
Completed questionnaires and qualitative results showed an improvement in participant knowledge in each session; microbes and antibiotics sessions showed the greatest knowledge improvement. Self-care showed the greatest knowledge retention and participants reported behaviour change including an increase in appropriate hand-washing and tooth-brushing.
Conclusion:
The Beat the Bugs course is a useful intervention for communities to give individuals the knowledge and confidence to manage their own infection and change behaviour around hygiene, self-care and antibiotics. Beat the Bugs is freely available to download.
Background
Controlling antimicrobial resistance is a Public Health England (PHE, 2014) and Department of Health (DoH, 2013) priority. The UK Five Year Antimicrobial Resistance Strategy outlines seven key areas for future action (DoH, 2013) including improving public knowledge and understanding of antimicrobial resistance through education. e-Bug supports this key area for action by educating children and young people and is endorsed by the National Institute for Health Care Excellence (NICE, 2017).
e-Bug is an international health education evidence-based resource for children and young people on microbes, the spread, treatment and prevention of infection, and antibiotics. It is operated by PHE and has been developed with input from teachers, health professionals and students (Lecky et al., 2011). e-Bug aims to help control antibiotic resistance in the UK and worldwide by educating young people, who are our future antibiotic prescribers and antibiotic users, about hygiene to reduce rates of infections and the use of antibiotics (Lecky et al., 2011; McNulty et al., 2011). The school e-Bug activities have led to significant improvements in student knowledge around antibiotics, hygiene and antibiotics (Lecky et al. 2010).
Antibiotics prescribed in the community equate to 74% of all prescribed antibiotics in England (PHE, 2017) and up to 50% of these may be unnecessary or inappropriate (Davey et al., 2005; Wise et al., 1998). Furthermore, there is public misunderstanding about how long infections usually last and how to use antibiotics correctly (McNulty et al., 2007). Therefore, public education within the community on hygiene, infection prevention and self-care is important to increase appropriate antibiotic use. As community education in this area is so important, e-Bug has recently expanded its educational resources into the community through the Beat the Bugs course.
Beat the Bugs is a six-week community hygiene and self-care course developed by a collaboration between the e-Bug team and the Kingfisher Treasure Seekers (KTS) community group. KTS have extensive experience working with vulnerable adults and the collaboration enabled the learning outcomes and the key messages of the course to be framed in a way that was accessible and appropriate to vulnerable adults, a group that are often underrepresented when interventions like these are developed. The aim of Beat the Bugs is to target hard-to-reach groups in the community to increase awareness and change behaviour around hygiene, self-care and antibiotic use in an interactive and fun way. Beat the Bugs is designed to be delivered by community leaders including school nurses, public health nurses, health visitors and support workers, to a range of community groups, including vulnerable adults, young parents, guides and scouts. The Beat the Bugs course is freely available to download and use from the e-Bug website at www.e-Bug.eu/Beat-The-Bugs.
Use of health behavioural pledges including the Germ Defence (Little et al., 2015) and antibiotic guardian (Kesten et al., 2017) have shown to increase knowledge and influence behaviour. Therefore, action planning and pledges will form a key part of the Beat the Bugs activities in order to help change participants intentions into behaviour and reinforce the learning objectives.
The aim of this study was to pilot the Beat the Bugs hygiene and self-care intervention in two different learning environments. Key objectives were to assess: the impact of the course on knowledge; the impact on self-reported behaviour; its acceptability to users and course leaders; and to transferability to other settings.
Methods
Research design
The study was a mixed method evaluation using quantitative and qualitative methods of enquiry. Two pilots of the Beat the Bugs course were conducted. The first pilot was conducted with adults with learning, physical and/or mental health difficulties in a community learning environment; 7–9 participants attended each week. The course was delivered by a Community Leader who regularly delivers training to this group of adults. The second pilot was delivered in a children’s centre with young parents; 2–4 participants attended each week. The course was delivered by a Family Support Worker who regularly delivers training to groups of parents.
Sampling and recruitment
Data collection took place between September 2016 and April 2017 inclusive. The two pilot centres were recruited for the Beat the Bugs pilot course through convenience sampling of local community groups. Participants who normally attended the centres were invited to attend the free Beat the Bugs course.
Ethics
This study did not require National Research Ethics Service (NRES) approval as it was outside the National Health Service and was classed as a service evaluation. Consent was deemed accepted if participants completed the before and after knowledge questionnaires. Questionnaires were collected in line with the Data Protection Act 1998 and Caldicott 1999 regulations on handling and distributing sensitive participant information. Focus group and interview participants provided verbal and written informed consent for participation in the research, audio recording and the publishing of anonymised quotes. The community leader was present during the focus group with adults with learning difficulties and ensured that all participants understood what was being asked of them.
Data collection
Short, before and after, knowledge questionnaires developed by the e-Bug team and the community groups were completed by participants at the start and end of each session. Questionnaires for each learning environment had different completion methods to suit participant ability, but tested the same area of knowledge. See Appendix A for examples of the questionnaires used. Pilot 1 questionnaires were colourful one-page documents that had knowledge-based statements and participants circled a cross, a tick or a question mark image as to whether the statements were ‘right’, ‘wrong’ or ‘not sure’. The course leader read out the statements to the group to assist with any reading difficulties. All participants referred to the questionnaires as ‘quizzes’ to reduce any negative perceptions of ‘doing a test’. Pilot 2 questionnaires followed similar statements to Pilot 1 but participants used tick boxes to choose the correct answer. Pilot 2 questionnaires followed the format and questions from previous e-Bug evaluations.
Each session was observed by an e-Bug researcher to increase validity and monitor fidelity with the activity plans. Two semi-structured face-to-face focus groups with participants at each setting were conducted six weeks after the final session to explore in-depth participant views on the course and to establish retention of knowledge. CE and CH (researchers for Public Health England) facilitated one focus group each. During both focus groups, a second researcher was present to record notes and observe the group. Two course leader interviews were facilitated by CE, one face-to-face and one via telephone. Figure 1 is a process map of the pilot evaluations.
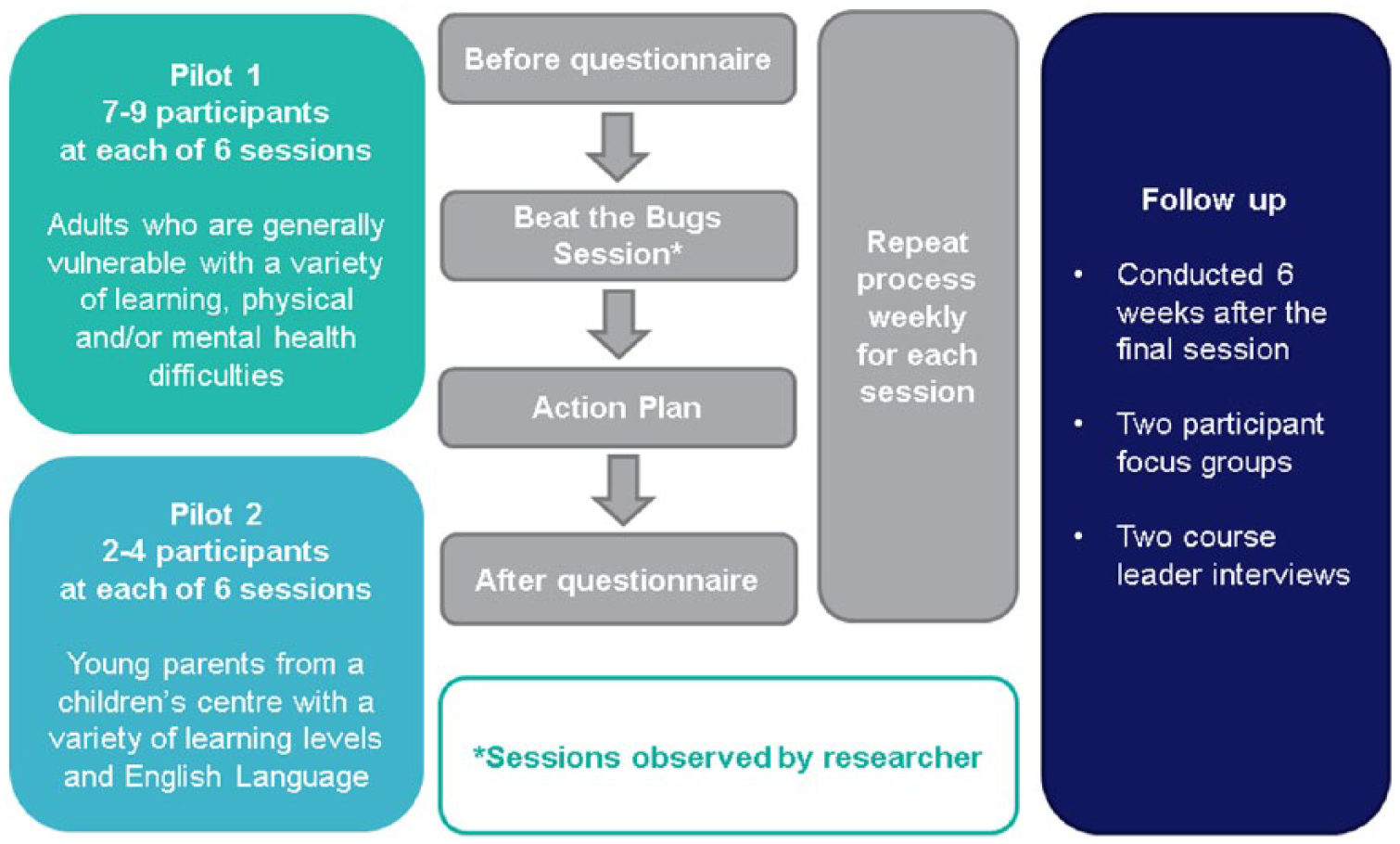
Process map of the pilot evaluations.
Quantitative data analysis
Before and after knowledge questionnaire data were analysed using Microsoft Excel software and visual graphs were used to represent the findings of quantitative results. Pilot 1 had six questionnaires each with six statements and the option for ‘right’, ‘wrong’ or ‘not sure’. Pilot 2 had a different number of questions for each session with 13, 12, 10, 11, 10 and 10, respectively. Each correct answer equated to 1 point. Individual participant before and after scores were calculated; corresponding percentages were also calculated. Individual before and after percentages were then comparable between the two pilots. Questions that were left empty by participants were given 0 points.
Qualitative data analysis
Interviews and focus groups were recorded, transcribed verbatim, checked for accuracy by CE and CH, anonymised and imported to NVivo (version 10). NVivo 10 qualitative data analysis software was used to organise, code and analyse the interview and focus group transcripts and open-ended evaluation responses.
Two researchers independently coded categories and themes. The lead researcher coded all transcripts and a second researcher (CH) coded one-quarter of the transcripts. Transcripts were revisited to ensure coding consistency and minor discrepancies over coding language were resolved through discussion; no major disagreements were raised. Initial themes and sub-themes were discussed with the whole study group. A descriptive analysis report was developed including illustrative quotes.
Results
Main findings
Before and after questionnaire data were collected from 9–12 participants for each of the six Beat the Bugs sessions: Figure 2 shows the before and after knowledge scores of both pilots.
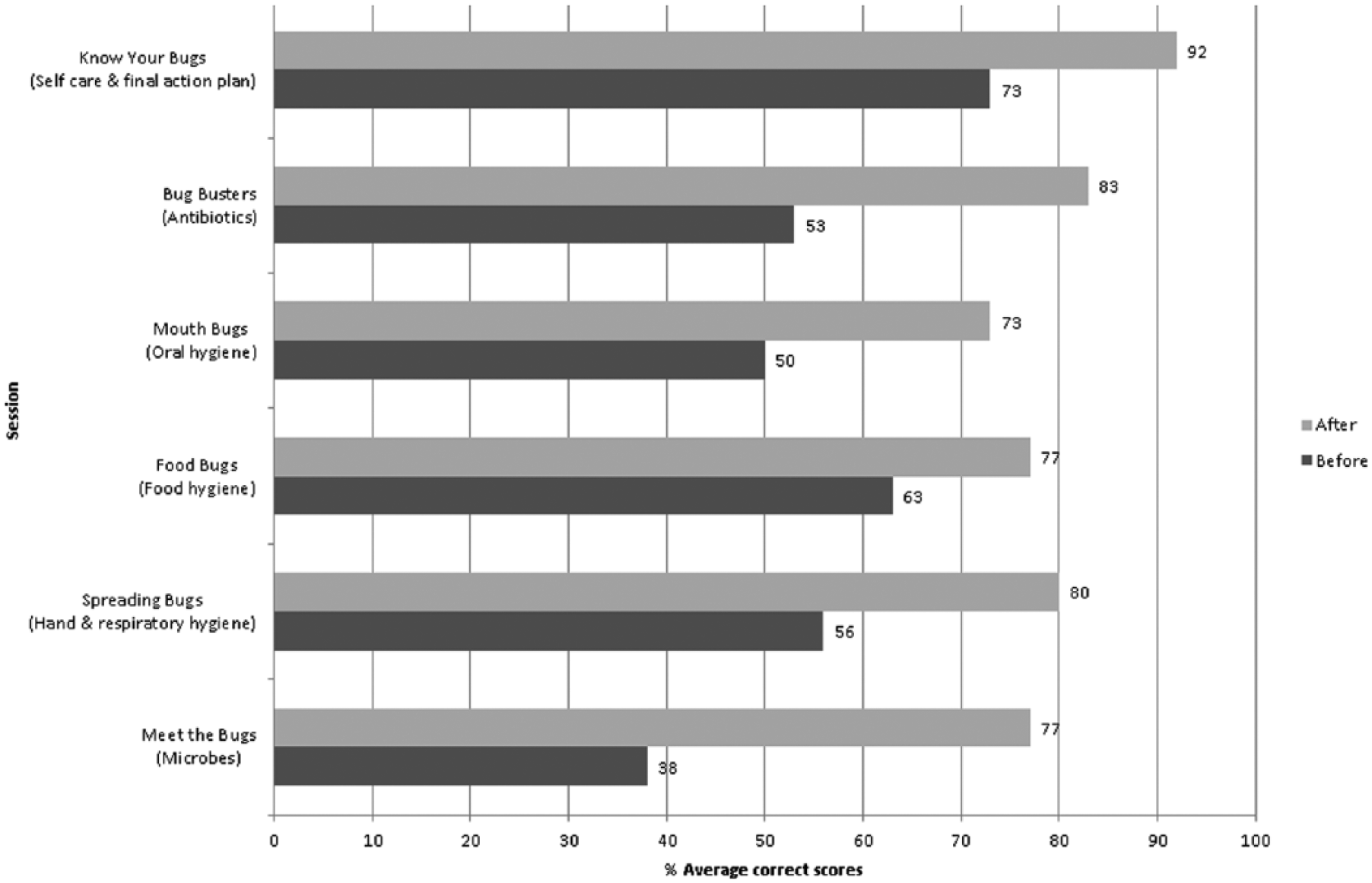
Before and after average knowledge scores of both pilots.
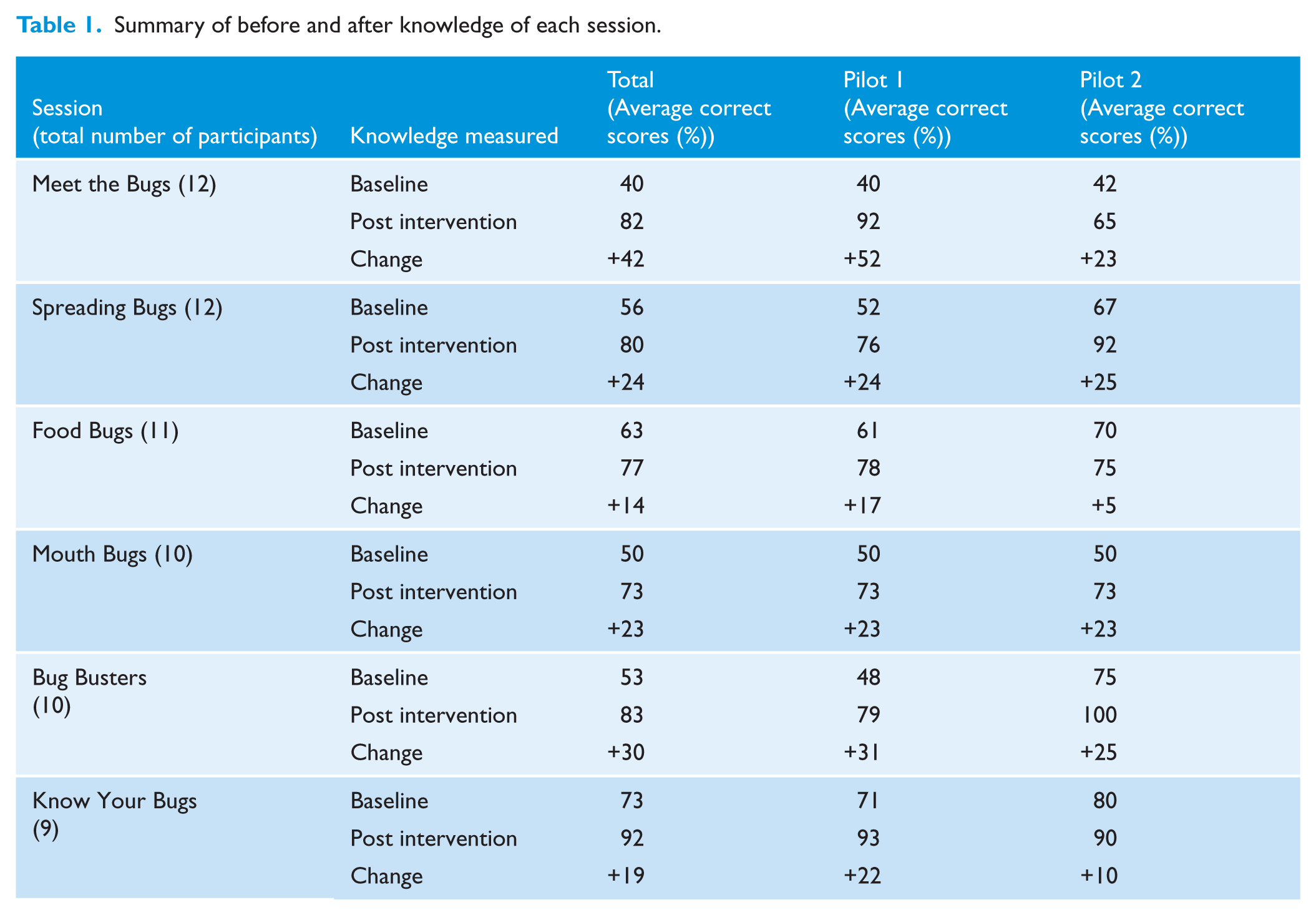
Quantitative results from the before and after knowledge questionnaires showed an improvement in participant knowledge in each session in both learning environments (Table 1). Overall in both pilots, a significant (P < 0.05) improvement in knowledge was seen in every sessions except Food Bugs which was approaching significance (P = 0.06). Overall the greatest improvement in knowledge was in the microbes and antibiotics session.
Summary of before and after knowledge of each session.
Two focus groups were conducted, one with five adults with learning difficulties and one with two parents from the children’s centre. Two course leader interviews were conducted, one face-face and one via telephone. Qualitative results showed that participants in both pilots had retained knowledge particularly around self-care. Positive behaviour change was also reported in the qualitative findings including an increase in appropriate hand-washing and tooth-brushing behaviour. Themes were common across the focus groups unless specified.
Session 1: Meet the Bugs
This session aims to give an overview of microbes. It explores different types and shapes of microbes and discusses useful and harmful microbes. Both pilots reported the lowest baseline knowledge in this session (40% and 42%). Overall this session had the greatest improvement in knowledge (Table 1). In this session about microbes, participant knowledge in Pilot 1 improved the most on statements: ‘Bacteria, Viruses and Fungi are the three main types of microbes’ (38% to 100% correct responses) and ‘It is important to protect our useful microbes’ (13% to 88%). Participant knowledge in Pilot 2 improved the most on the question ‘Which of these is not a microbe?” (0 to 100% correct responses).
Qualitative results showed that participants could recall the three types of microbes six weeks after the course.
‘The smallest [microbe] would be virus.’ (Participant, Pilot 1) ‘The three different types of microbes are “Viruses, and bacteria, and fungi”.’ (Participant, Pilot 2)
Course leaders reported enjoying delivering this session, especially the ‘make a microbe’ activity, but felt like they were also ‘learning along with the participants’ (Course Leader, Pilot 2).
‘I was really impressed with how well the plasticine went… I wasn’t expecting that degree of engagement with that. I think everyone took part in that one [making a microbe].’ (Course Leader, Pilot 1) ‘The parents really liked the visual activities, the arts and crafts especially; you had it spot on with the activities.’ (Course Leader, Pilot 2)
Session 2: Spreading Bugs
This session aims to give an overview of the spread of infection by learning how microbes are spread through sneezing and how correct hand-washing with soap can break the chain of infection. Both pilots reported average baseline knowledge of > 50% and both reported an improvement in knowledge by 24% and 25%, respectively. In this session, participant knowledge in Pilot 1 improved the most on the ‘wrong’ statement: ‘Microbes do not spread from person to person’ (22% to 67% correct responses). Participant knowledge in Pilot 2 improved the most on ‘The best way to stop microbes spreading is by using a tissue when you sneeze’ (33% to 100% correct responses).
Qualitative results at six-week follow-up showed that participants could explain why it is important to wash their hands and reported an increase in appropriate hand-washing behaviour and an increase in appropriate behaviours around using tissues when you sneeze. Parents at the children’s centre also reported improving their children’s health behaviours by encouraging them to wash their hands appropriately.
‘So we don’t get any germs to our foods or anywhere that you may catch a cold.’ (Participant, Pilot 1) ‘I try to use a tissue, to use a tissue if I can.’ (Participant, Pilot 1) ‘[Hand-washing] prevents spread of bacteria.’ (Participant, Pilot 2) ‘I’m taking him [child] to the bathroom a lot to wash his hands, rather than just using a wet wipe which I used to do. I take him to the bathroom and he uses his step and get him to wash hands with the soap now and before he eats, go and wash his hands, after he uses his potty, or when I take off his nappy I get him to wash his hands to get him used to it, so, yeah.’ (Participant, Pilot 2)
Course leaders reported enjoying the activities in this session, particularly the hand-washing and snot gun.
‘Oh, the snot gun. I think it generates quite a lot of interest but, oh yeah, it does cause a lot of discussion about where on the runway everything falls.’ (Course Leader, Pilot 1) ‘The snot gun was a visual activity and everybody understood how far a sneeze goes and it really caught the parents’ eyes. I think they enjoyed that one.’ (Course Leader, Pilot 2)
Session 3: Food Bugs
This session aims to give an overview of how easily potentially harmful microbes in raw food can transfer to humans causing illness, and how to store different foods in the fridge to prevent microbes spreading from one food (especially raw meat) to another. Both pilots had high baseline knowledge (61% and 70%, respectively) and there was less opportunity to increase in knowledge. In this session about food hygiene, participant knowledge in Pilot 1 improved the most on the ‘wrong’ statement: ‘You can reheat food as many times as you want’ (34% to 67% correct responses).
Qualitative results at follow-up showed that participants could explain why it is important to store food correctly in the fridge.
‘Also, the meats shouldn’t touch between like dairy or raw meat because it will contain salmonella or food poisoning.’ (Participant, Pilot 1) ‘The meat has to be at the bottom…otherwise it would be leaking down.’ (Participant, Pilot 2)
Course leaders reported that the activities worked well including the fridge raiders activity where participants have to store food correctly in the fridge.
‘The activities seemed to work really well and the people that did them definitely benefitted.’ (Course Leader, Pilot 1)
Session 4: Mouth Bugs
This session aims to give an overview of how to prevent tooth decay through limiting sugar intake and brushing teeth twice a day. Both pilots had average baseline knowledge of 50% and both had a 23% increase in knowledge. In this session about oral hygiene, participant knowledge in Pilot 1 improved the most on the ‘right’ statement: ‘Dental plaque is a build-up of bacteria on our teeth’ (63% to 100%). Participant knowledge in Pilot 2 improved the most on ‘Some foods and drinks cause tooth decay because they contain a lot of sugar’ (50% to 100%).
Qualitative results at follow-up showed that participants knew why they brush their teeth, recalled what drinks contained the most sugar and also reported an increase in appropriate tooth-brushing behaviours.
‘It is important to brush your teeth so you don’t get any cavities in them and also you won’t get any holes so you won’t get your teeth damaged.’ (Participant, Pilot 1) ‘I’ve started brushing [child’s] teeth too!’ (Participant, Pilot 2)
Course leaders reported an increase in appropriate health behaviours about oral hygiene including participants now registering with a dentist after not going for years.
‘I quite enjoyed doing the teeth cleaning with the little model that worked quite well…. Also, a couple of them actually have thought about how to go to the dentist now because there were a few of them … that hadn’t been for years so that’s good news as well.’ (Course Leader, Pilot 1)
Session 5: Bug Busters
This session aims to give an overview of what antibiotics are, when to take antibiotics and how to take antibiotics correctly. Higher baseline knowledge was reported in Pilot 2 of parents (75%) compared to Pilot 1 of adults with learning difficulties (48%). Both pilots saw a positive change in knowledge by 31% and 25%, respectively. In the antibiotics session, participant knowledge in Pilot 1 improved the most on the ‘right’ statements: ‘You should only take antibiotics if your doctor has prescribed them to you’ (50% to 100%); and ‘You must not use other people’s antibiotics’ (50% to 100%). Participant knowledge in Pilot 2 improved the most of statement ‘Antibiotics affect other bacteria in your body, not just the ones which cause infection’ (0 to 100%).
Qualitative results at follow-up showed that adults with learning difficulties in Pilot 1 struggled to explain what antibiotics were and when they should take them; however, they did understand that they should only take antibiotics if they really needed them, they should not share antibiotics with friends or family, and should only take antibiotics as the doctor or nurse has prescribed.
Researcher: What should you do if your doctor gives you antibiotics? ‘I would take them like they told me to and if you have any left take them to the pharmacy.’ (Participant, Pilot 1)
Parent participants in the Pilot 2 focus group displayed a very high knowledge about antibiotics particularly that antibiotics do not work on viruses.
Researcher: If your friend came to you and said ‘I’ve got a cold, I’m going to go to the doctor’, what would you say to them? ‘There’s no point visiting the doctor, because they won’t give you antibiotics.’ (Participant, Pilot 2) ‘Antibiotics doesn’t kill flu.’ (Participant, Pilot 2)
Course leaders expressed that this antibiotics session was difficult to deliver and improve understanding around.
‘I am still not convinced they know what antibiotics are, but I really got a sense during the course that they understood that they didn’t keep tablets, didn’t take tablets they didn’t know what they were for, and that they would take them back [to the pharmacy].’ (Course Leader, Pilot 1) ‘I think there is still loads of work we need to do with antibiotics… It’s just a really difficult concept to teach in a literal way.’ (Course Leader, Pilot 1) The key learning points that participants took away from the course would ‘definitely be about the antibiotics.’ (Course Leader, Pilot 2)
Session 6: Know Your Bugs
This session aimed to give an overview of how to self-care at home for common infections, make decisions on their own health, think about their own antibiotic use and action plan for the future. Both pilots had high baseline knowledge (71% and 80%, respectively), which may be because participants had already completed the previous sessions. Participants reported an increase in knowledge following the session (22% and 10% increase in knowledge, respectively). Participant knowledge in Pilot 1 improved the most on the ‘right’ statement: ‘A cold usually lasts 10 days’ (43% to 86%) and ‘If you need advice on whether to go to the doctors or not then ring NHS 111’ (29% to 86%). Participant knowledge in Pilot 2 improved the most on ‘A cold usually lasts 10 days’ (50% to 100%).
Qualitative results at follow-up showed that participants had retained knowledge around self-care, particularly the importance of getting plenty of rest and drinking enough fluids.
‘Always drink plenty of water, always get a good rest and always wash your hands and use a clean tissue and use paracetamol if you need them.’ (Participant, Pilot 1) ‘Stay at home, have a rest and drink plenty of water.’ (Participant, Pilot 2)
Course leaders described that this session brought all the previous sessions together to reinforce how individuals can look after themselves and prevent infection.
‘I am optimistic about participants’ self-care.’ (Course Leader, Pilot 1) ‘How long illnesses last and when they should and shouldn’t go to the doctors were the key learning points I think.’ (Course Leader, Pilot 2)
Discussion
Main findings
The Beat the Bugs pilot provides an insight into the benefits, learning outcomes and transferability of the course across different community groups. The course is a useful intervention in increasing awareness and educating the community on important public health topics including microbes, hand, respiratory, food and oral hygiene, self-care and antibiotics.
Action plans to pledge behaviour change were a useful addition to the Beat the Bugs course as participants reported an increase in appropriate health behaviours such as hand-washing and tooth-brushing behaviour.
Modifications to the Bug Busters session covering suggestions from participants and the course leaders, especially on the antibiotic activities, will be included in order to help community leaders facilitate the course and increase participant understanding.
Strengths and limitations
A strength of this study is the use of both quantitative and qualitative methods of enquiry to determine knowledge change and perceived behavioural change. The before and after knowledge questionnaire provided an insight into whether the learning outcomes of each sessions were being met and whether the sessions were pitched at the correct ability level. Qualitative interview and focus group follow-ups provided a more detailed insight into participants and course leader views on the course and what they have learnt. The qualitative data focused on reported behaviour change by the participants rather than measuring actual behaviour change. All sessions were observed by researchers and all qualitative data collection was conducted or observed by CE which increased validity.
The sample size of the two pilots was relatively small: 9–12 participants in each session in total and two course leaders. However, 4–10 individuals are the optimum size to deliver the Beat the Bugs course following feedback in the development stages from participants and course leaders. Obtaining feedback from two different community groups is very worthwhile as we attained knowledge and behaviour change data which are valuable. We also attained qualitative evaluation feedback that participants valued the course and community leaders found it feasible to run, informing researchers that an extended evaluation would be feasible on a larger scale.
The action plans that were pledged at the end of each session and revisited at the start of the next session helped to change intended behaviour into actual behaviour. Following the course, participants reported a higher understanding about hygiene, self-care and the consequences of their health behaviours which was a mechanism for behaviour change. However, as this study did not measure actual behavioural change, reported or perceived behaviour change may be subject to some acquiescence bias.
A further strength of this study is that it links to the guidance of the Medical Research Council (2006) in the processes involved in the development, pilot and feasibility of a complex intervention.
Comparison with existing literature
Previous evaluations of the e-Bug school activities have shown significant improvements in student knowledge around antibiotics (Lecky et al., 2010). Our study supports these findings in relation to antibiotic behaviours reported by the community groups. However, some participants struggled to understand exactly ‘what an antibiotic is’ and ‘when it is required’. Several of the individual activities within the Beat the Bugs community course—including making a microbe, the hand-washing activity, the snot gun and how clean is your kitchen—have previously been evaluated in a school environment as part of the e-Bug peer education project delivered to 9- to 11-year-olds, and found that there was a significant improvement in participant knowledge for all topics covered in the intervention (Young et al., 2017). This present study confirms that these activities are transferable to community groups.
A large randomised control trial with 20,066 participants, found that individuals who pledged to wash their hands more often using the Germ Defence website had fewer colds, flu and stomach upsets than those who hadn’t seen the website (Little et al., 2015). Germ defence is an online tool that suggests hand-washing pledges and action planning to change behaviour and reduce household infections, colds and flu (Little et al., 2015). A qualitative study with 22 individuals found that pledges made on the Antibiotic Guardian campaign website were fulfilled by either a behaviour change or the pledge reinforcing a pre-existing behaviour (Kesten et al. 2017). Our research supports these findings as the Beat the Bugs pledges have addressed the intention–behaviour gap in relation to appropriate hygiene, self-care and antibiotic use by supporting individuals to translate their health intentions into behavioural action.
Total page views from the official Beat the Bugs website launch on 9 September 2016 for 12 months were 2310 visits; the full Beat the Bugs pack was downloaded 342 times over 12 months. The Beat the Bugs website visits will need to be monitored regularly along with which learning resources are being downloaded from the website.
Implications for future research
Ongoing efforts will be made to refine and focus key messages in a way that is acceptable and accessible to course recipients. Future research will also include larger evaluations of Beat the Bugs with different community groups to determine the transferability of the course.
In response to feedback from the pilot courses, and after discussions with other community groups, a ‘Train the Trainer’ workshop has been developed for community leaders to learn about Beat the Bugs and provide them with the knowledge, confidence and skills to deliver the course in their community groups. In the year to October 2017, 64 community leaders have become Beat the Bugs approved trainers including teachers, school nurses, scout leaders, family support workers and community support workers. This presents a clear mechanism through which the course can and is being scaled up. e-Bug aims to deliver the ‘Train the Trainer’ workshops on a termly basis to further promote the course. Feedback from the training has been very positive: ‘It was all really helpful and interesting. The activities were great – very engaging’ and ‘The activities were fantastic; the children will love these interactive sessions. It educated me also’. Training dates and approved trainers are listed on the Beat the Bugs webpage at www.e-Bug.eu/Beat-The-Bugs.
Conclusion
The Beat the Bugs course is a useful intervention for community groups to help increase individuals’ confidence and knowledge on managing their own infections and change behaviour around hygiene, self-care and antibiotic use. e-Bug will continue to work with the community to develop and promote resources to educate the public including hard to reach individuals about hygiene, self-care and antibiotics. The pictorial self-care leaflet used in this resource is now endorsed by NICE.
Supplemental Material
JIP780990_Supplemental_Appendix1 – Supplemental material for A mixed methods pilot of Beat the Bugs: a community education course on hygiene, self-care and antibiotics
Supplemental material, JIP780990_Supplemental_Appendix1 for A mixed methods pilot of Beat the Bugs: a community education course on hygiene, self-care and antibiotics by Charlotte Victoria Eley, Vicki Louise Young, Catherine Victoria Hayes, Gill Parkinson, Katie Tucker, Nina Gobat and Cliodna Ann Miriam McNulty in Journal of Infection Prevention
Footnotes
Acknowledgements
The authors thank Kingfisher Treasure Seekers for collaborating on the Beat the Bugs course. They also thank Dr Nick Francis, Cardiff University, and Dr Sally Weston Price, Queen Mary University, for their assistance with developing the course. Additional thanks go to the participants who attended the pilot courses.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: At the time this work was conducted, the authors (CE, VY, CH, CM) all worked for Public Health England to produce and disseminate e-Bug teaching resources for schools covering microbes, the spread, treatment and prevention of infection, and antibiotic resistance.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Public Health England.
Peer review statement
Not commissioned; blind peer-reviewed.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.