
Abstract
Background:
The concept of single-use of endodontic files remains controversial in the published literature. The extent and attitudes concerning the single-use of endodontic hand files is currently unknown in many countries.
Aim:
The prevalence and perceptions regarding the single-use of endodontic files was investigated in this descriptive observational study.
Methods:
A questionnaire regarding the perceptions and usage protocols of endodontic files was developed. Twenty-seven South African dental practices were included in this study. Participation was voluntary.
Results:
None of the respondents reported single-use of endodontic hand files. Several decontamination methods were used by the respondents for reprocessing endodontic files.
Discussion:
Financial constraints were reported as the primary reason for the reuse of endodontic files. As no standardised method of reprocessing these instruments exists for South Africa, written guidelines on this subject should be developed.
Background
Endodontic hand files are instruments used during endodontic treatment to mechanically prepare root canals. Historically, the reuse of these instruments on multiple patients has been standard practice, provided cleaning and sterilisation has taken place before reuse in subsequent clinical cases (Carrotte, 2004). In recent years, substantial evidence has been published in the literature advocating the single-use of endodontic files rather than reusing these instruments (Aasim et al., 2006; Letters et al., 2005; Morrison and Conrod, 2009; Walker et al., 2007).
Arguments for the single-use of endodontic files include:
Difficulty in adequately cleaning endodontic files (Walker et al., 2007);
The risk of transmission of infectious diseases (Laheij et al., 2001);
The potential transmission of prion disease (Kirby et al., 2012; Walker et al., 2007);
The unreliable and unpredictable nature of the processes used to clean endodontic files (Letters et al., 2005);
Corrosion and dulling of metal instruments (Carrotte, 2004).
Contrary to this view, literature supporting the routine reuse of endodontic files also exists (Messer et al., 2003; Parashos et al., 2004b). The most significant arguments in favour of reuse are:
Laboratory trials have demonstrated the ability to remove 100% of stained debris from the surfaces of endodontic files (Messer et al., 2003; Parashos et al., 2004b);
The accepted reuse of the other stainless-steel dental instruments that contact the dental pulp, in some territories (Messer et al., 2003);
The absence of prion proteins in the dental pulps of individuals diagnosed with Creutzfeldt-Jakob disease (Head et al., 2003);
The increased cost incurred in implementing single-use protocols (Letters et al., 2005; Messer et al., 2003; Parashos et al., 2004b);
Cleaning and sterilising procedures do not appear to be an important factor of the fracture resistance of nickel-titanium files (Hülsmann et al., 2005).
In 2007, the UK Department of Health advised dentists to treat all endodontic files and reamers as single-use instruments (Walker et al., 2007). Economic constraints, especially in developing countries, however, dictate the high likelihood that endodontic files will continue to be reprocessed and reused. South Africa currently has no official guidelines for the reprocessing of endodontic files. It is not known whether any South African dental practitioners have adopted a single-use approach regarding endodontic files and what the reasons for this may be.
Methods
This descriptive observational study investigated the use and decontamination methods of endodontic files of 27 dental practices in Pretoria, South Africa. Participants were recruited by convenience sampling. Selection was accomplished by contacting dental practices by telephone in Pretoria, South Africa, listed on an Internet database. Dental practitioners who were known to offer endodontic services were contacted directly. After a short telephone conversation with the owner of the dental practice, an appointment was scheduled—provided that the practice delivered endodontic services and the owner was interested in participating. During each appointment, the practice owner was provided with an overview of the intended study. Informed consent was obtained. A coding system guaranteed the anonymity of each participant.
Interviews were administered by an interviewer and questionnaires were actively completed with the person(s) responsible for the decontamination procedures of endodontic hand files in each specific dental practice.
The questionnaire was designed to evaluate:
Protocols followed for using endodontic hand files (i.e. single or multiple use);
Reasons for discarding files;
Decontamination methods used for endodontic hand files;
Quality control measures for assessing file cleanliness;
Reasons for multiple use;
Attitudes regarding the concept of single-use protocols.
All statistical analyses were performed using the SAS software suite, Release 9.4 (SAS Institute Inc., NC, USA). Simple descriptive statistical analysis was conducted. The data obtained were expressed as simple percentages.
The research protocol for this study was approved by both the Research Committee of the School of Dentistry, Faculty of Health Sciences, University of Pretoria and the Ethics Committee of the Faculty of Health Sciences, University of Pretoria.
Results
The following results describe the answers to the questionnaire as provided by the 27 respondents.
Protocols followed for using endodontic hand files
None of the respondents used endodontic hand files as single-use instruments. Endodontic hand files were only used for a maximum of five clinical cases by 40.7% (n = 11) of the respondents; 44.4% (n = 12) used these instruments for between five and ten cases before disposal. Some respondents (n = 3, 11.1%) used endodontic files to complete more than ten cases before being discarded. One respondent did not answer the question.
Reasons for discarding files
The reason provided by 70.4% (n = 19) of respondents for discarding an endodontic hand file was damage. Examples of damage included files that had separated (i.e. fractured), bent or deformed. Only 14.8% (n = 4) of the respondents discarded an endodontic file after a predetermined number of uses, regardless of the file’s condition. The remaining 14.8% (n = 4) of respondents used a file for a set amount of cases but also discarded a file sooner had the instrument become damaged during use, despite not having reached the predetermined maximum number of uses.
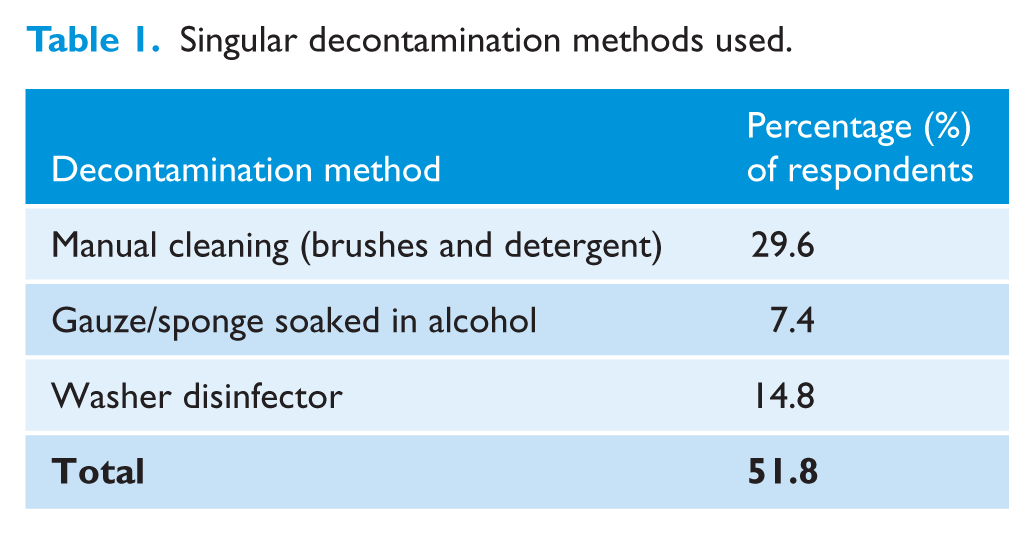
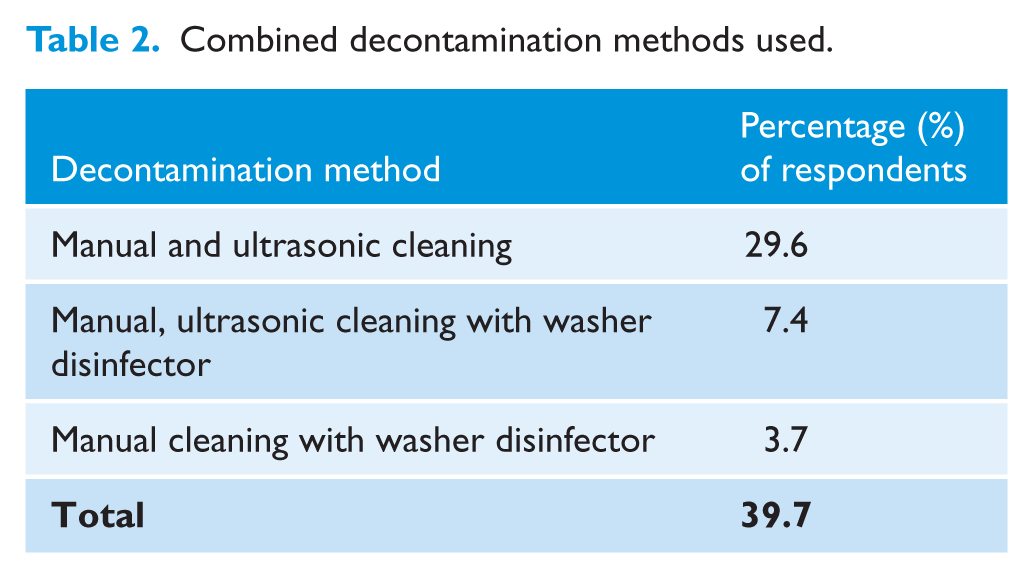
Decontamination methods used for endodontic hand files
Methods of decontamination reportedly used by the respondents are summarised in Tables 1 and 2. No answer was provided to this question by 7.4% (n = 2) of respondents.
Singular decontamination methods used.
Combined decontamination methods used.
Quality control measures for assessing file cleanliness
Methods of assessment of the cleanliness of files following routine decontamination procedures were reported as either: visual inspection with the naked eye, as reported by 77.8% (n = 21) of participants; or inspection with magnification aids such as magnifying loupes or operating microscope, as stated to be routinely used by 7.4% (n = 2) of the participants. Some of the of respondents (n = 3; 11.1%) did not inspect their files before reuse. One respondent provided an invalid answer to this question.
Reasons for multiple use
Two respondents (n = 2; 7.4%) believed that complete decontamination of endodontic hand files was achievable by applying routine decontamination methods.
One respondent asserted that endodontic hand files were reused because achieving complete decontamination was attainable and often these instruments were still in good working condition after clinical use and reprocessing. Another respondent reused endodontic files that were in good working condition, unless a file had been damaged during initial use, in which case it was discarded.
Invalid responses by 22.2% (n = 6) of the respondents discounted their views to this question. Furthermore, this question was not answered by 37% (n = 10) of the respondents.
Attitudes regarding the concept of single-use of endodontic hand files
One-third (n = 9; 33.3%) of the respondents had considered only using endodontic hand files once and then discarding them. The remaining two-thirds (n = 18; 66.6%) of the respondents had never considered the single-use of endodontic hand files.
Of those respondents who had never considered single-use to be an option in their practices, one-third (n = 6; 22.2%) reported that the single-use of endodontic hand files would be too expensive. Almost one-quarter (n = 6; 22.2%) of the respondents believed it unnecessary to discard endodontic files that were still in good working condition. A combination of these factors was given by 7.4% (n = 2) of the respondents.
The most common reason given by 22.2% (n = 6) of respondents for considering single-use of files was the belief that single-use would be safer for their patients. One respondent stated single-use would be safer for the personnel working with these instruments. Some respondents (n = 4; 14.8%) believed that better endodontic treatment outcomes could be achieved if single-use protocols were implemented. One respondent named all the above-mentioned reasons in reply to this question. Several respondents (n = 15; 55.5%) failed to answer this question.
Discussion
None of the respondents of this study had adopted the policy of single-use endodontic instruments. The finding that hand files are reused for 5–10 cases the majority of the time and the fact that they are most often discarded due to damage is in agreement with previous research (Parashos et al., 2004a).
Research has demonstrated that South Africa has an extremely low number of dentists, as low as 0.13 per 1000 population ratio (Strachan et al., 2011). A survey conducted in 2009 placed the total best estimate of South African dentists working in the private sector to be only 3121 (Strachan et al., 2011). At the time of writing, an online database (Medpages, 2017) estimated the number of dentists in Pretoria to be 360. The results of this study therefore provide insight into the perceptions and practice of single-use instruments only within the context of the city of Pretoria. Future studies may consider a larger scale investigation into the subject.
Dental practitioners make use of referenced articles to assist them when making decisions on new treatment and practices. The abundant literature demonstrating that endodontic files can be effectively cleaned and sterilised may be a strong influence on the trend of multiple use of these instruments (Messer et al., 2003; Parashos et al., 2004b). The decision to reuse instruments should, however, be made in conjunction with the international standard ISO 17664:2017, which specifies the information that medical device manufacturers must provide to users for reprocessing instruments in order for them to be safe to use, especially if instruments are labelled as single-use items. The absence of guidelines for reprocessing endodontic files in South Africa leaves the decisions regarding reprocessing and reuse of these instruments with the individual dentist.
Single-use of endodontic hand files significantly increases the number of instruments that must be purchased by a practice, increasing the overheads associated with the provision of endodontic treatment and decreasing the profit margin of providing such services. Some of the participants from this study attributed the trend of multiple use of endodontic hand files to the cost of the instruments. Such financial considerations may deter not only private dental practitioners, but also public and academic dental hospitals from implementing the single-use of endodontic files as policy (Messer et al., 2003). While previous research has suggested financial reasons as a factor for not implementing single-use policies in dental practice (Messer et al., 2003), the results of this survey confirm that this is indeed the case. No data are available on the cost of reprocessing dental instruments in South Africa; therefore, a direct comparison between reprocessing these instruments versus single-use is not possible. Future research should aim to address this gap in knowledge and a cost–benefit analysis may be conducted to provide clarity.
Great variation in the methods for decontamination of endodontic files was found among the respondents to this survey. This finding indicates a lack of a standardised procedure for the reprocessing of these instruments and is likely due the lack of written guidelines on the subject in South Africa. It has previously been demonstrated that dental instruments may not be effectively cleaned and sterilised to an acceptable standard within the South African context (De Kock and van Wyk, 2001; Mehtar et al., 2007; Oosthuysen et al., 2010; Yengopal et al., 2001). Previous research from other territories has, however, demonstrated the unreliability of cleaning endodontic files, regardless of the reprocessing method used (Letters et al., 2005).
The finding that some respondents used magnification aids for instrument inspection before reuse is encouraging and demonstrates an increase in acceptance of this quality-control method. Whether this method of inspection resulted in better detection of remaining debris on endodontic files after reprocessing is not clear. Further investigation into the use of magnifying aids to detect the failure of decontamination should be conducted.
A small number of respondents stated that complete decontamination of previously used endodontic files was possible. This finding is confounding, considering all the respondents implemented multiple-use protocols and reused their endodontic files. It is clear from the responses to this question that the attitudes of dental practitioners and their staff regarding infection control procedures may not necessarily be aligned with their beliefs.
Just over one-quarter of the participants responded that the single-use of endodontic files would increase patient and personnel safety. This finding indicates that a significant proportion of the respondents felt that the single-use of files was probably better clinical practice than reusing them.
Despite the controversy surrounding the concept of single-use endodontic files in the published literature, dentists have a moral and ethical responsibility towards their patients to practise infection control procedures to a high standard (Scarlett and Grant, 2015). Inadequate infection control practices may lead to violation of these ethical principles. Currently, in some territories, the decision to implement single or multiple use of endodontic instruments rests with the individual practitioner.
The single-use of endodontic hand files is currently not in place in private dental practices surveyed in Pretoria, South Africa. Furthermore, files are reprocessed and reused on multiple clinical cases. There is no standard decontamination method used to reprocess files in South Africa and written guidelines should be developed for reprocessing these instruments. The primary reason for the reuse of these instruments are concerns surrounding the financial implications of introducing single-use protocols.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Peer review statement
Not commissioned; blind peer-reviewed.