
Abstract
Patients who carry nasal methicillin-resistant Staphylococcus aureus (MRSA) may also harbour MRSA in the oro-pharyngeal cavity. However, the naso-oro-pharyngeal co-carriage is infrequently assessed. The incidence of concurrent MRSA carriage of the naso-oro-pharynx was ascertained, and the sensitivity of two methods, a throat swab and a phosphate buffered saline (PBS) oral rinse, for MRSA detection was investigated. Among nasal MRSA carriers, 80% harboured MRSA in the oro-pharynx. Among these patients, 15% had MRSA detected in the oro-pharynx and not in the throat. Oro-pharyngeal colonisation represents a significant reservoir to persistence as well as nasal recolonisation. Decolonisation methods effective in reducing oro-pharyngeal MRSA in addition to nasal carriage should be investigated.
Background
Colonisation with methicillin-resistant Staphylococcus aureus (MRSA) is associated with an increased risk of infection. The odds of MRSA bloodstream infection among carriers is 20 times that of non-colonised individuals (Marzec and Bessesen, 2016) and infection after placement of cardiac electronic implant device is sixfold in carriers (Asundi et al., 2019) leading to extended hospitalisation (Cosgrove et al., 2005) and higher 90-day postoperative mortality (Engemann et al., 2003). Eradication of MRSA carriage forms an integral part of strategies to prevent and control MRSA transmission and infection (Calfee et al., 2014; Coia et al., 2006). Eradication of nasal colonisation is commonly attempted using mupirocin 2% nasal ointment and eradication from skin sites using antiseptics such as chlorhexidine. MRSA frequently colonise the nose as well as extra-nasal sites such as the throat, perineum and wounds (Harbarth et al., 1999; Leigh and Joy, 1993). MRSA colonisation of the oropharynx may be an overlooked anatomical reservoir, contributing to the persistence of nasal MRSA carriage via translocation from the oral cavity but decolonisation strategies frequently only address nasal MRSA. Multisite screening including the throat is recommended by best practice guidelines (Coia et al., 2014; Cookson et al., 2011). However, the relationship between oro-pharyngeal and nasal MRSA co-carriage is rarely investigated. The aim of the present study was to determine the incidence of concurrent nasal and oro-pharyngeal MRSA carriage and to investigate the sensitivity of two methods for detection of oro-pharyngeal MRSA carriage. Quantification of the MRSA burden in the oro-pharynx of nasal MRSA carriers will better inform enhanced methods for decolonisation.
Methods
This was a prospective observational cohort pilot study. The study was conducted in accordance with the Declaration of Helsinki and institutional ethical standards, endorsed by an approved Research and Ethics Committee (REC) at Beaumont Hospital (BH), Dublin, Ireland (REC number 18/09). Written informed consent was obtained from all patients.
Setting and study population
The study was conducted between March and May 2018 at a tertiary care adult acute hospital in Dublin, Ireland, which has 820 beds and 25,000 admissions annually. Potential participants were identified from routine microbiology reports. MRSA carriers aged ⩾ 18 years were eligible if colonised in the nose and an inpatient at the time of study enrolment. After obtaining consent, a swab sample was collected from the throat, and an oral rinse sample obtained by an experienced infection prevention and control nurse. Swab samples were taken from the throat using sterile cotton-tipped swabs with transport media (EUROTUBO®, Deltalab), pre-moistened with sterile saline. For oral rinse samples, patients were then provided with 20 mL of sterile phosphate buffered saline (PBS), asked to rinse and gargle their mouth for at least 20 s, and then empty the rinse solution into a sterile container. Swab samples were routinely processed with other swabs in the hospital microbiology diagnostic laboratory. MRSA was detected using chromogenic agar plates (MRSASelect™ II; bioMérieux, Marcy-l’E’toile, France) after 24 h of incubation, according to Cherkaoui et al. (2007). Presumptive MRSA colonies were identified as deep pink colonies and their identity definitely confirmed by coagulase latex agglutination using the Pastorex® Staph-Plus test. Laboratory personnel were blinded to the origin of the throat screening samples.
Oral rinse samples were processed separately. Briefly, 1-mL aliquots were centrifuged (10,000 × g for 1 min), pelleted bacteria were re-suspended in 300 µL of PBS, and 100-µL aliquots were spread onto MRSASelect™ II. Plates were incubated at 37 °C for 24 h and deep pink colonies (presumptive MRSA) were counted and confirmed as S. aureus using the Pastorex® Staph-Plus test (EUCAST, 2013).
The patients’ dependency, a measure of their healthcare needs, was assessed using the BH Nursing Information System (NIS) score. This weighted cumulative score, is in the range of 1–5. A higher score denotes fully dependent/specialised care, which often correlates with frequency of contact with a healthcare worker (Cohen et al., 2012).
Results
In total, nasal MRSA was reported from 49 patients during the recruitment period. Excluding 12 outpatients, the remaining 37 (100%) were assessed for eligibility. Twenty-one (56%) patients were eligible, of which 20 (95%) consented in writing and were enrolled.
Of the 20 patients who had nasal MRSA, 16 (80%) yielded oral MRSA using the oral rinse method and 13 (65%) yielded MRSA from throat swabs. Therefore, the sensitivity of swab sampling was 65% versus 80% using PBS. The demographic, clinical and microbiological characteristics of study participants are summarised (Table 1).
Demographic, clinical and microbiological characteristics of study participants.
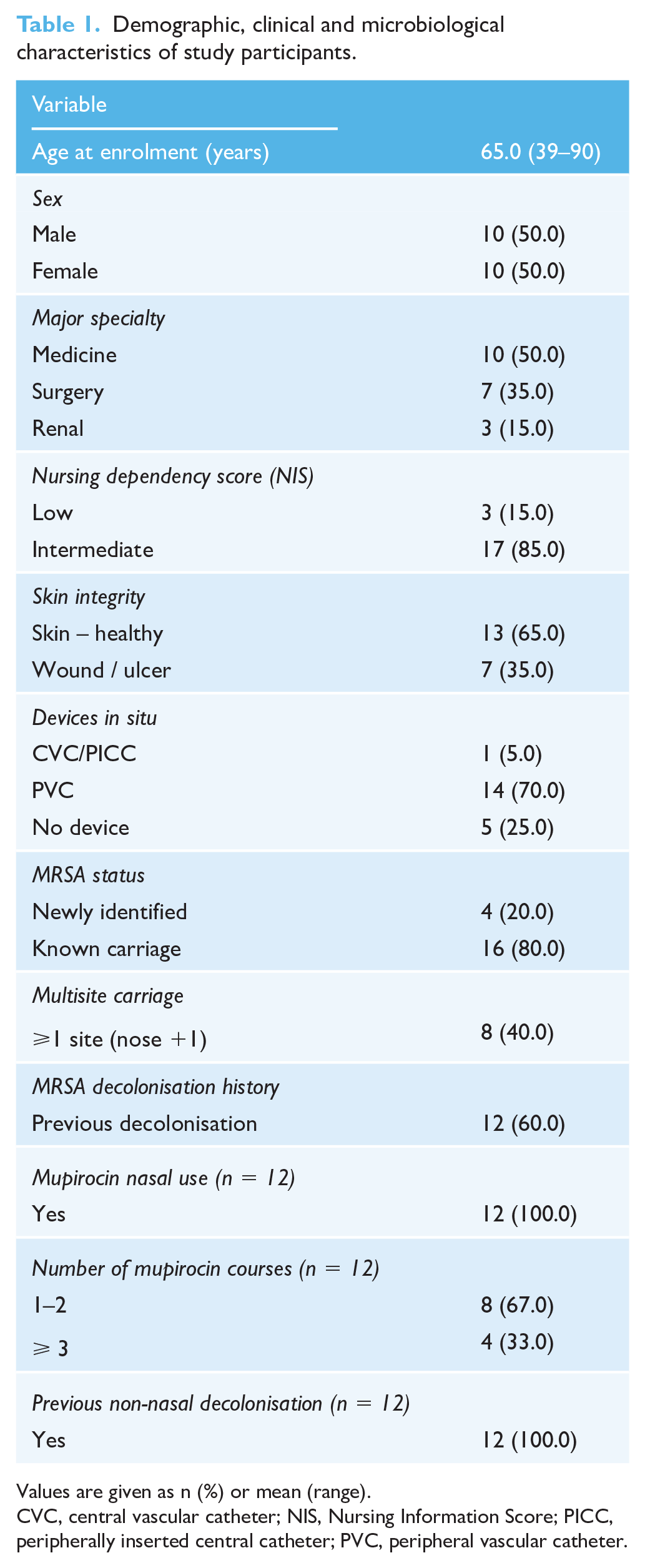
Values are given as n (%) or mean (range).
CVC, central vascular catheter; NIS, Nursing Information Score; PICC, peripherally inserted central catheter; PVC, peripheral vascular catheter.
A concordant positive (n = 13) or negative (n = 4) result using PBS oral rinse and throat swabs was obtained from 17 (85%) patients. Three patients (15%) had a negative throat swab but MRSA was detected from their oral rinse sample.
The comparative MRSA screening data of all 20 participants is presented in Table 2.
MRSA detection from throat and oral rinse including colony count.
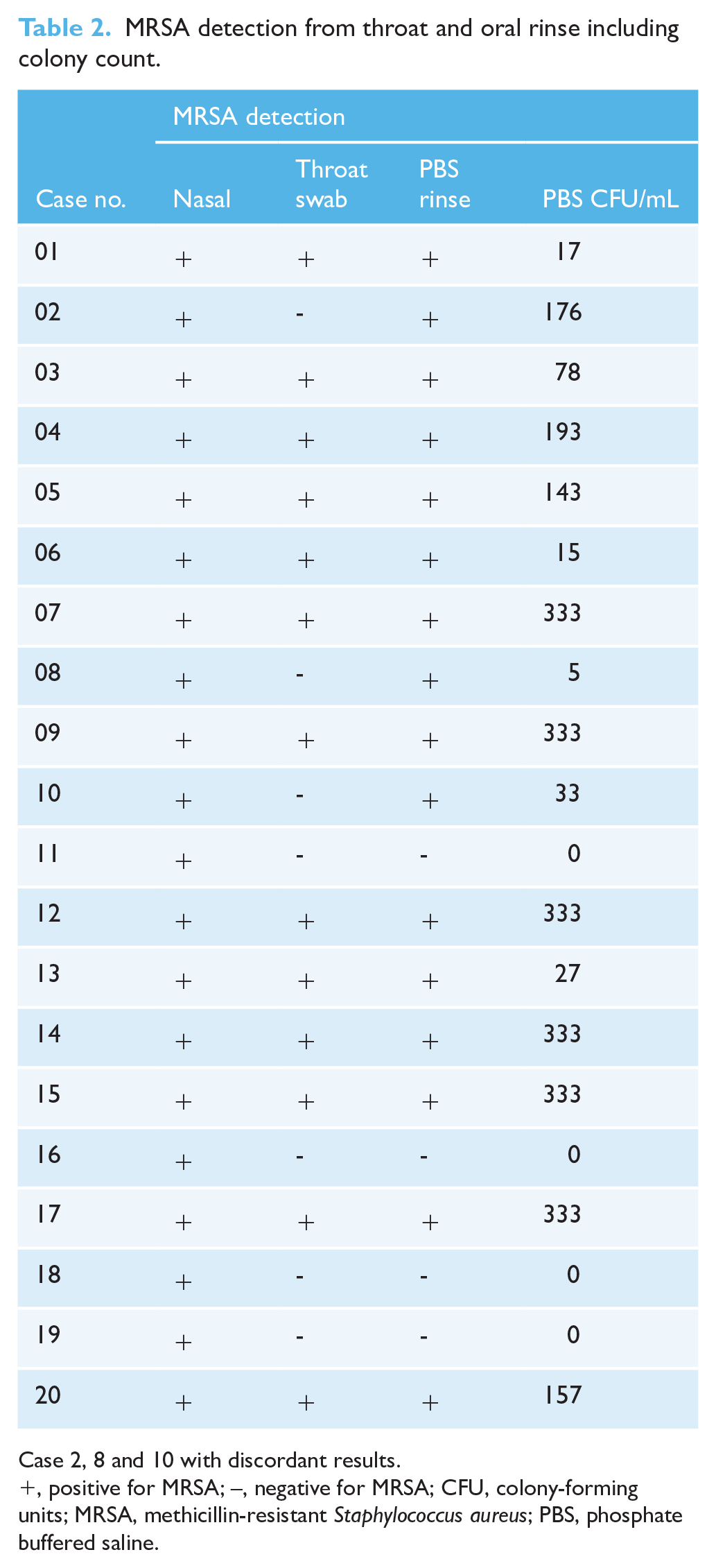
Case 2, 8 and 10 with discordant results.
, positive for MRSA; –, negative for MRSA; CFU, colony-forming units; MRSA, methicillin-resistant Staphylococcus aureus; PBS, phosphate buffered saline.
Discussion
Decolonisation of MRSA is frequently difficult. Multi-site MRSA carriage impedes nasal decolonisation (Harbarth et al., 2000). Previous findings from a nasal decolonisation randomised controlled trial we undertook reported short-term nasal decolonisation success rates of 50% (Poovelikunnel et al., 2017) similar to other studies (Harbarth et al., 1999). The present study demonstrates that most nasally colonised patients (80%) are also colonised in the throat/oral cavity. Although based on different methodologies, this finding supports a previous study which suggested that throat carriage of MRSA was a better predicator of infection than nasal carriage (Jang et al., 2014).
Translocation of staphylococci between the nose and the oral cavity is well documented. (Bitterman et al., 2010; Lauderdale et al., 2010; Williamson et al., 2016). Oro-pharyngeal colonisation therefore is likely to serve as a source of persistent re-colonisation, limiting the longevity of successful nasal decolonisation. This has major implications for clinical practice and provides a plausible explanation as to why nasal decolonisation is frequently unsuccessful. Moreover, practices that contribute to ineffective decolonisation of the oro-naso-pharynx may enhance the development of antimicrobial resistance, due to, for example, repeated courses of nasal mupirocin. Therefore, the need for simultaneous decolonisation of the throat/oral cavity should be considered when nasal decolonisation is attempted.
Many laboratories rely on culture for MRSA surveillance and improvements in chromogenic media have increased colony discrimination and reduced processing times. Furthermore, for throat sampling, swab-based methods are unpleasant for many patients, and may be a deterrent during routine MRSA screening. Although a small study, the lower rate of recovery of MRSA using direct throat swabbing, compared to oral rinse methods found here, highlights reduced sensitivity of throat screening. The superior detection sensitivity afforded by the oral rinse method, where the cell fraction was concentrated by re-suspension in sterile PBS before inoculation of MRSASelect™ II, makes this an attractive alternative with potential for MRSA surveillance.
The present study has some limitations, including a single centre and a relatively small number of patients. In routine clinical practice, oral rinse sample collection and processing are likely to be resource-intensive in comparison to a swab. However, oral rinse sampling offers a potentially superior alternative to a throat swab for MRSA detection. Further larger studies are warranted to investigate how common oro-pharyngeal colonisation is without nasal carriage, the most appropriate anatomical sampling site for MRSA colonisation detection that considers sensitivity, reliability in clinical practice and surveillance, cost and ease-of-use for patients and healthcare workers.
Footnotes
Acknowledgements
Part of the study findings was presented at the HIS International Conference (2018) during free papers session, oral presentation.
Author’s Note
Hilary Humphreys and Toney Thomas Poovelikunnel are also affilaited with Department of Clinical Microbiology, Royal College of Surgeons in Ireland, ERC, Dublin, Ireland.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: HH is in receipt of research funds from Pfizer and Astellas and has in the recent past received consultancy fees from Pfizer. All other authors have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Peer review statement
Not commissioned; blind peer-reviewed.