
Abstract
Background:
The emergence of bacterial resistance caused health authorities to attempt to implement strict regulations for rational antibiotic prescription. However, supervision is often neglected in low- and middle-income countries, leading to inappropriate administration of antibiotics. The objective of our study is to highlight the lack of monitoring in the community setting of a middle-income country.
Material and methods:
We asked 68 patients presenting to an infectious diseases consultation office to report the antibiotic courses they had taken in the three months preceding their visit. We assessed for treatment indication, molecule choice, dosing and duration, as well as microbial cultures, demographics and specialty of the prescriber.
Results:
Among the 68 patients included in our study, we counted a total of 95 outpatient antibiotic courses, mostly composed of quinolones (36%), followed by amoxicillin-clavulanate (21%). The prescriber was most commonly a primary care physician, but we reported several cases of auto-medication and dispensation of antibiotics by pharmacists. Only 30% of cases had true indications for antibiotics.
Conclusion:
In sum, our results indicate an evident lack of regulation over the administration of antibiotics. This easy accessibility needs to be promptly addressed as we run the risk of inevitable bacterial resistance.
Background
In 2015, the World Health Organization (WHO) endorsed a global action plan (GAP) to tackle antimicrobial resistance (AMR), based on five strategic objectives: awareness; surveillance; lowering infection rates; optimising the use of antimicrobial agents; and economic investments. This is implemented on a national scale through a national action plan (NAP) on AMR.
Nowadays, bacterial resistance is a growing public health matter, encountered in hospitals and most commonly in the outpatient setting (Bätzing-Feigenbaum et al., 2016; Durkin et al., 2018; Kabbani et al., 2018). Antibiotics are frequently dispensed over-the-counter in low- and middle-income countries (Horumpende et al., 2018; Lindberg et al., 2017). Easy accessibility and lack of regulation play a major role in microbial resistance. Moreover, antibiotics are often incorrectly prescribed (Chauhan et al., 2018) or inappropriately administered.
This study takes place in a middle-income country, where a government-approved national AMR action plan is aligned with the GAP objectives mentioned above. However, despite having laws on the prescription and sale of antibiotics, they are often not executed. This portrays lack of vigilance, and underlines the importance of implementing WHO’s proposals, reinforcing antibiotic stewardships, and maintaining national surveillance programs.
The aim of this article is to assess the misuse of antibiotics by evaluating the antibiotic treatment taken by patients in the three-month period preceding a specialised infectious diseases consultation, while taking into account the prescriber, the demographics and six other variables.
Materials and methods
This is a prospective cohort study that took place from 1 October 2017 to 1 January 2018 in the community setting of an infectious diseases consultation office of a middle-income country. We included patients who took antibiotics in the three months before their visit, as previous antibiotic therapy can induce resistance. We assessed the following features: age; gender; molecule used; dose; duration of therapy; presence or absence of fever; indication for treatment; result of cultures (if performed); and the specialty of the prescriber. The data were collected and then analysed for statistics using Microsoft Excel. Informed consent was obtained from participants.
Results
A total of 70 patients were evaluated, of whom 68 were eligible to be included in the study. They accounted for a total of 95 courses of antibiotics (a mean of 1.4 antibiotic courses per patient). The female-to-male ratio was 5:2, with a median age of 43.7 years (age range = 18–82 years).
We found the most commonly used molecules to be quinolones, accounting for 34 courses of total antibiotic intakes (25 levofloxacin, seven ciprofloxacin, one ofloxacin and one moxifloxacin), followed by amoxicillin-clavulanate in 20 courses, and cephalosporins in 17 courses (nine third-generation, six second-generation and two first-generation cephalosporins). Other antibiotic intakes included five courses of amoxicillin, four of clarithromycin, four of azithromycin, three of clindamycin, two of doxycycline, two of metronidazole, two of rifampin, one of cotrimoxazole and one of oral Fosfomycin (Figure 1).
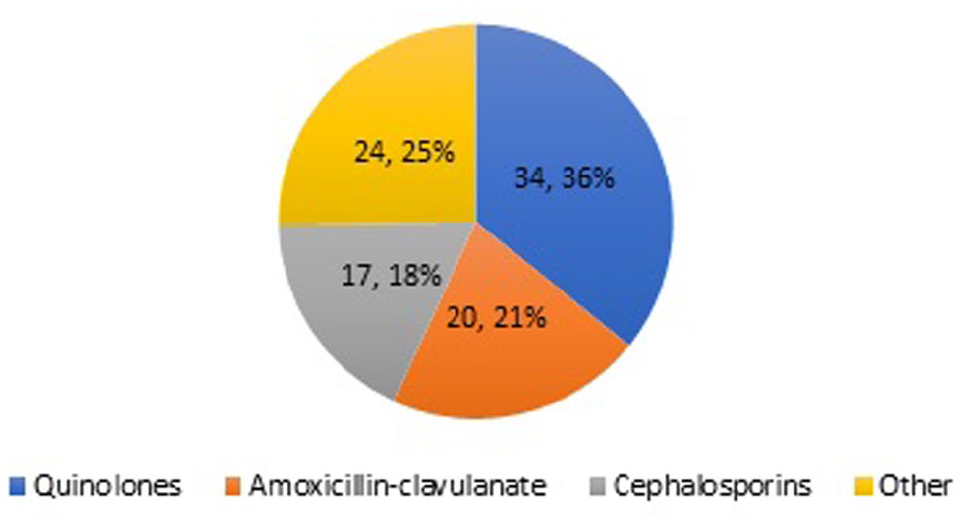
Percentage of antibiotic courses taken illustrated by class of antibiotics.
Fever was only present in 19 cases (representing 20% of indications). Nevertheless, despite the absence of fever in the remaining 80% of cases, antibiotics were still prescribed. The cases included in each category are illustrated in Figure 2.
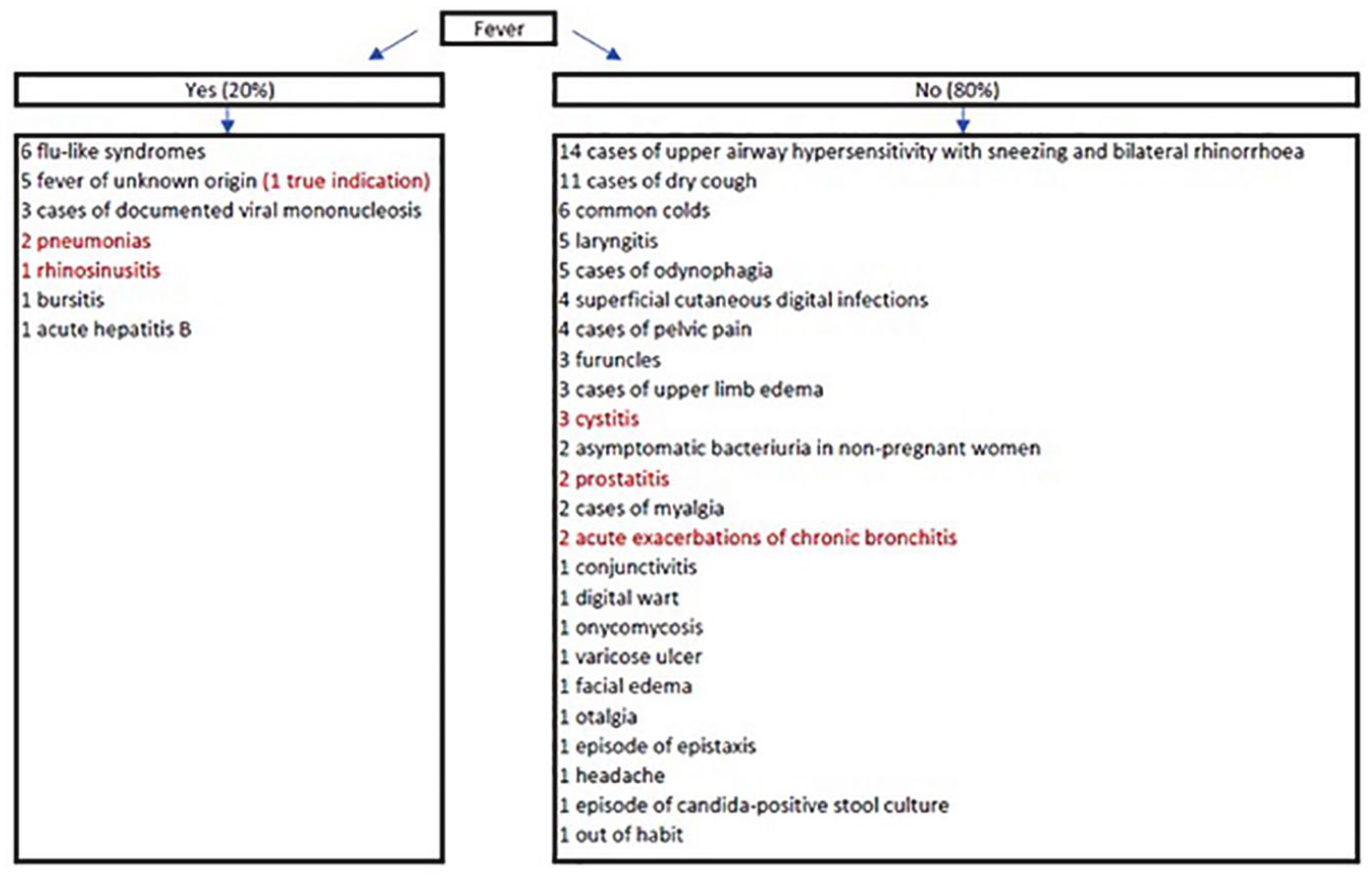
Illnesses for which antibiotics were prescribed, in the presence or the absence of fever, respectively (in red: true indications for antibiotic use).
Out of the aforementioned cases presenting without fever, only seven had true indications for antibiotic therapy: three cystitis; two prostatitis; and two acute exacerbations of chronic obstructive pulmonary disease (AECBs). The other 69 reported episodes had no indication for treatment with antibiotics. Furthermore, the antibiotic dosage was incorrect in 11 cases, including eight cases with inappropriate duration of therapy. Inversely, the duration of therapy was incorrect in 32 antibiotic courses, including eight with inappropriate medication dosage. In total, 35 antibiotic courses had either a wrong dosage or an erroneous duration of therapy. As for antibiotic acquisition, 11 patients had resolved to over-the-counter auto-medication. Antibiotics were prescribed by a pharmacist in one case, and by physicians in 23 cases. The physicians comprised 10 general practitioners, five dermatologists, four gynaecologists, one general surgeon, one ophthalmologist, one otolaryngologist and one pulmonologist (Figure 3).
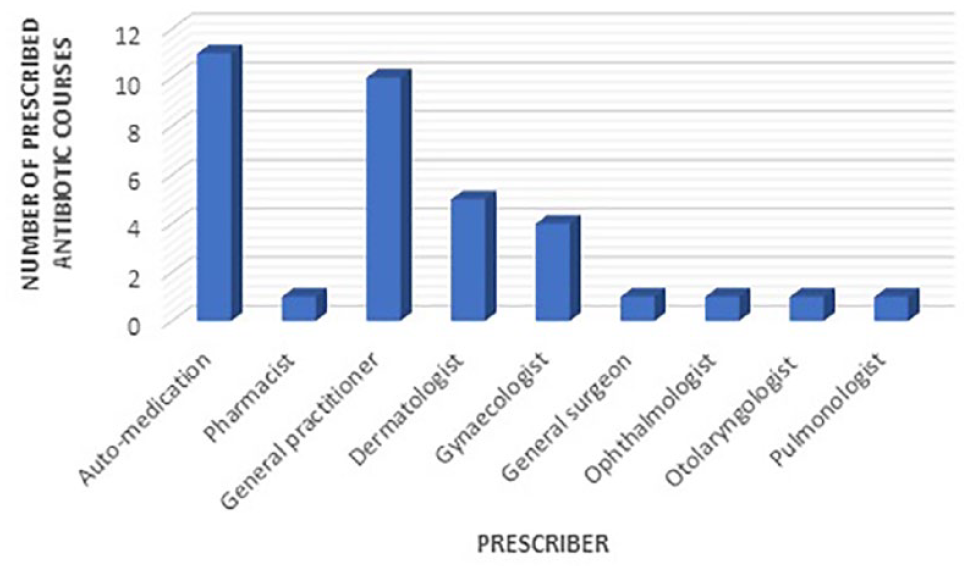
Number of antibiotic courses per prescriber specialty among the cases without fever.
In total, out of the 95 antibiotic courses, the prescribers were physicians in 49 cases (51%), pharmacists in 16 cases (17%) and the patients themselves through self-medication in 30 cases (32%).
Microbial cultures were only performed in nine cases and were positive in five cases: three urine cultures had gram-negative bacteria; one nail culture had Citrobacter koseri growth; and one stool culture was positive for Candida.
Discussion
The results described above are clear indicators of the lack of regulation regarding accessibility to antibiotic, a big factor leading to bacterial resistance. This is a call for imperative public health awareness to reduce the misuses of the antibiotics and their unfettered dispensation by pharmacists (Servia-Dopazo and Figueiras, 2018). Physicians outside the field of infectious diseases are sometimes rushed or pressured by the patient to prescribe antibiotics. Determining the factors that contribute to lax antibiotic dispensation could help delineate strategies to counter this limitation (Gidengil et al., 2016; Hicks et al., 2015; O’Connor et al., 2018). Furthermore, physicians should be encouraged to refer the patient to a specialist when the necessity for antibiotics is ambiguous (Chem et al., 2018; Lindberg et al., 2017; Yoshida et al., 2018), as overprescription for upper airway infections, for example, is commonly found in the primary care setting (Dekker et al., 2017; Glinz et al., 2017). A randomised controlled trial proposed that resorting to point-of-care C-reactive protein (CRP) measurement could withhold primary care physicians from prescribing antibiotics when levels of CRP are normal (Lemiengre et al., 2018). Antibiotic stewardships and collaboration between pharmacists and general practitioners could reduce the overprescription of antibiotics, as suggested by the systematic review led by Saha et al. (2018). In our study, only 30% of reported cases had a correct indication for antibiotic use. Nevertheless, even if the indication for antibiotics is correct, inappropriate molecules, doses or durations of treatment are often noted (Chauhan et al., 2018), thus also playing a role in the emergence of resistant organisms. Another crucial facet contributing to reduced inappropriate antimicrobial usage relies on proper public awareness on the dangers relating to AMR to understand the real-time impact of AMR emergence. We also encourage organising workshops, conferences and antibiotic stewardships to HCWs practising outside the field of infectious diseases. For instance, World Antimicrobial Awareness Week is a yearly campaign that contributes to global awareness on AMR, one of WHO’s five GAP objectives.
Despite having a national action plan for AMR per WHO’s recommendations through a system conceived for antimicrobial use surveillance (sales and consumption), the results found in this study did not reflect appropriate implementation. As a middle-income country, the cost of AMR can carry heavy economic repercussions. Although there is local AMR data collection for common bacteria, it lacks national coordination and standardised approaches. A national infection prevention and control program is available but not fully implemented.
This article highlights the often-underestimated inappropriate antibiotic dispensation. However, one of the limitations is the small population of study. Nationwide large-scale data collection would better render the underlying challenge and leave more emphasis on the need for pressing intervention.
Conclusion
In conclusion, the emergence of bacterial resistance is the most dreaded beast in the world of infectious diseases. Monitoring antibiotic dispensation could assist in regulating accessibility (Del Mar et al., 2017). Addressing the factors that perpetuate ill-advised prescriptions is chief to deliver appropriate interventions.
Low- and middle-income countries are in need for strengthened public health awareness and strict antibiotic regulation, to endorse rational antibiotic prescription (Chaw et al., 2018).
The root problem lies not in laws but in the absence of implementation, vigilance and regulation from authorities. It is the responsibility of the governing body to ensure NAP laws are properly executed, and healthcare workers’ duty to spread awareness on the risks entailed to widespread AMR.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
An ethics committee approval is not required as this study took place in a community setting, and did not include any experiments or interventions on participants.
Peer review statement
Not commissioned; blind peer-reviewed.