
Abstract
The importance of SARS-CoV-2 transmission via contact routes and its stability on surfaces is becoming increasingly recognised. There is ongoing concern that patients can become infected through person-to-person spread and environment-to-person spread. This study assessed whether SARS-CoV-2 viral RNA can be detected in the environment either on staff members’ personal protective equipment (PPE), on high-touch surfaces or around the bedspace of COVID-19–positive patients in a range of different ward settings to evaluate if there was any contamination of these. Results showed all PPE and high-touch surface swabs were negative. All swabs taken in the negative-pressure room where aerosol-generating procedures (AGPs) were being undertaken detected viral RNA (5/5 positive), whereas there was minimal contamination in the intensive therapy unit (1/5 positive) and none detected in the cohort bay. These findings would be consistent with the understanding that areas where AGPs are regularly performed are at higher risk of environmental contamination.
Keywords
Background
Transmission of the new COVID-19 disease, a predominantly respiratory illness caused by the SARS-CoV-2 novel coronavirus is generally considered possible through airborne, droplet and contact routes (World Health Organization, 2020). There are likely multiple factors implicated in the transmission of SARS-CoV-2 and environmental contamination among them; using data derived from previous coronaviruses, contact of contaminated surfaces may be significant in the possibility of environment-to-person spread (Otter et al., 2016).
Some evidence suggests that different surfaces as well as aerosols allow the virus to survive for varying lengths of time. For instance, the virus has been shown to survive on steel or copper for up to 72 h and that both fomite transmission and aerosolisation are tenable (Van Dorelamen et al., 2020). Infection prevention guidance issued by Public Health England (PHE) acknowledges survival of the virus in the environment. They also advise that for aerosol-generating procedures (AGP), airborne precautions must be taken in addition to standard contact precautions, though negative-pressure isolation rooms are not necessary to prevent transmission, but to consider using these isolation rooms if high risk and capacity allow (PHE, 2020). Reassuringly, the coronaviruses can be sufficiently inactivated by surface disinfection (Kampf et al., 2020). Thus, cleaning is of paramount importance: cleaning with the right disinfectants, at the right time with meticulous attention to all potential exposed surfaces. In addition, when formulating an infection prevention strategy, due consideration of the risk factors and mitigating elements (such as ventilation) of the environment should all be factored in.
During the height of the COVID-19 pandemic in the UK and where NHS staff faced many uncertainties with regard to environmental contamination and contamination of healthcare workers’ (HCWs) attire, we performed environmental swabbing to assess whether SARS-CoV-2 viral RNA can be detected in the environment either on the personal protective equipment (PPE) of HCWs, on high-touch surfaces or around the bedspace of COVID-19–positive patients in a range of ward settings.
Methods
In April 2020 (our peak period) at a large tertiary care acute hospital trust, environmental viral swabs were taken for SARS-CoV-2 viral RNA testing.
Environmental sampling was performed on three ward settings: Area A, a segregated COVID-19–positive general intensive care unit (GICU); Area B: a COVID-19–positive cohort ward where AGPs are not performed; and Area C, a ward consisting of negative-pressure rooms, where AGPs including, but not limited to, non-invasive ventilation (NIV) are performed.
For PPE swabbing, eight nurses, three physiotherapists and a healthcare assistant were recruited who were caring for COVID-19–positive patients in these wards. Their duties included day-to-day clinical work such as observation of vital signs, assisting patients with eating or mobilising, moving equipment, performing ECGs, care of long lines, and monitoring ventilation and administering medications. On average, the Area A HCWs had worked for around 1.5 h caring for intubated patients in side rooms, the HCWs in Area B had worked for around 30–60 min in a 3–6-bedded bay, while the Area C HCWs had worked for 1–2 h in side rooms with patients either on oxygen or NIV.
PPE sampling was carried out immediately after HCWs finished their clinical tasks with patients with COVID-19, pre-doffing, in a systematic order: visor (if wearing); mask (either surgical or FFP-3 dependent on their area of work); forearms or gown arms; front of apron/gown; gloves; and shoes. In addition, a general head-to-toe swab, after doffing of PPE, was performed on the uniform or scrubs the HCWs were wearing. Furthermore, separate control swabs on each ward were taken from a nurse who had not been working with any patients with COVID-19 in any of these areas.
Environmental sampling was carried out on computer mice and keyboards that were located in general access areas outside COVID-19–positive patient rooms/bays. Furthermore, swabs were also taken from around the bedspaces of the most acute or recent COVID-19 admission to the respective areas. This included a negative-pressure side room with a patient on NIV, an intubated patient in a side room in the GICU and a four-bedded cohort bay. Swabs were taken from the beds and the floor around the bedspace.
All samples in this study were taken using standard viral liquid culture swabs in viral transport medium (VTM) for real-time polymerase chain reaction (RT-PCR). All swabs were hand-delivered to the laboratory. Samples were extracted and purified using magnetic particle extraction on the Thermo Scientific KingFisher Flex. PCRs were performed on the Applied Biosystems (ABI) 7500. ORF1ab and N gene targets were detected using the Viasure SARS-CoV-2 RT-PCR kit. In addition, primers and probes for the E gene assay, including an internal positive control, were also used to enhance sensitivity of the assay.
Ethical approval was not required for the present study. It was a Local Quality Improvement project.
Results
A total of 49 PPE swabs, shoe swabs and computer mice and keyboards swabs were negative for SARS-CoV-2 RNA across all three areas (Figure 1). All samples taken around the bedspace in Area B were also all negative. However, SARS-CoV-2 RNA was detectable in one of five samples (head rail of bed) in Area A, where closed circuit ventilation was performed at the time, and five of five bedspace samples taken from Area C where AGPs were in progress. It should be noted that the patient in Area C, the negative-pressure side room, was very early in the course of their illness and had been admitted less than 24 h before swabbing (Table 1).
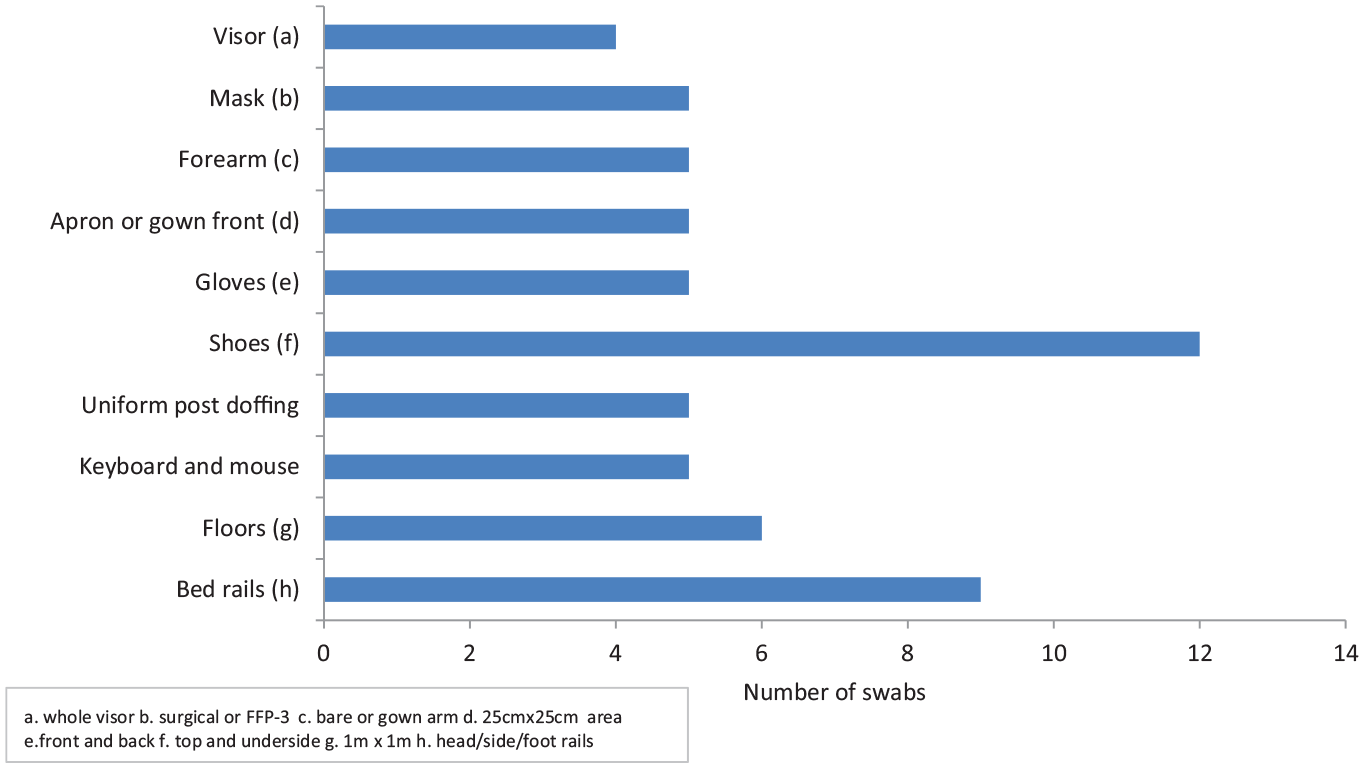
Swabbed sites (personal protective equipment and environmental samples).
Results of room swabbing.
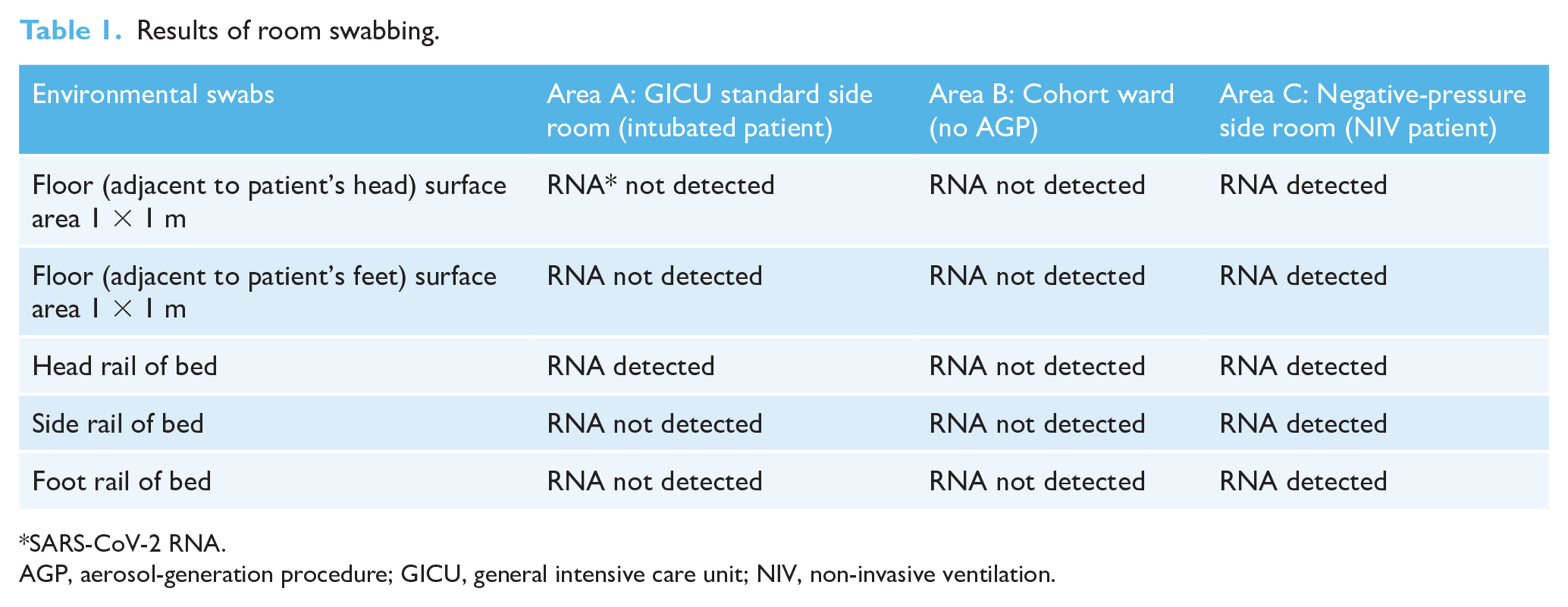
SARS-CoV-2 RNA.
AGP, aerosol-generation procedure; GICU, general intensive care unit; NIV, non-invasive ventilation.
Discussion
Initial results of real-world sampling revealed no SARS-2-CoV RNA on staff PPE. Similar to other NHS Trusts, in our hospital, considerable effort has been put into donning and doffing training and despite the sessional use of PPE, with a significant variation in time spent in PPE (up to 2 h in the same PPE for two of the nurses), no viral RNA was detectable even when staff were performing AGPs or when the patient was on NIV.
However, environmental sampling demonstrated limited contamination in the GICU side room (head rail of bed) and widespread contamination of the negative-pressure side room where the patient was receiving NIV. Enhanced environmental cleaning in the GICU side room could explain the level of low contamination. Second, the headrail in the GICU side room was slightly more difficult to access and therefore harder to clean.
It is interesting to note that NIV in a negative-pressure side room had evidence of greater environmental contamination than the intubated patient in the GICU side room on closed circuit ventilation. This underscores concerns that AGPs pose a greater risk of environmental contamination and subsequently cross-infection, particularly if infection prevention practices are breached. In addition, the patient in the negative-pressure side room was very early in their course of illness and although it is not known for sure, prevailing opinion and indirect data suggest that viral shedding is higher in the early stages of infection.
The limitations of this study include, but are not limited to, the knowledge of how results of PCR testing best correlate with viral shedding and infectivity; positive results may indicate both viable and non-viable virus, while negative results do not exclude the presence of virus. In addition, viral sequencing could have assisted in correlating infection in patients with environmental contamination but at the time of this study, was not available. Further, the PCR assay we used is not validated for non-respiratory tract sampling. It is nonetheless reassuring to note that our assay is capable of detecting the virus on a range of surfaces in the environment. Our findings are limited by the small sample size, assay sensitivity and the observational nature of this study. This was a pragmatic initial convenience cohort and in order to validate and explore these findings further this study would need to be repeated with a representative sample.
In conclusion, AGPs can result in higher environmental contamination; areas with ongoing AGPs (e.g. NIV) need enhanced cleaning as the risk of cross-contamination remains high. Cleaning to reduce the number of potentially contaminated surfaces and regular handwashing remain the best efforts of mitigating contact transmission. Second, patients undergoing NIV should remain in negative-pressure side rooms, if capacity allows, with adequate air changes per hour to try and mitigate this. Lastly, staff must comply with infection control polices with regard to PPE and handwashing.
Footnotes
Acknowledgements
The authors thank the patients and relatives and staff who not only provided samples, but also for their cooperation and professionalism during those challenging times. The authors also thank all staff at the Southampton Specialist Virology Centre at University Hospital Southampton, not only for their support with the testing, but also for their continuous enthusiasm throughout the pandemic.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Peer review statement
Not commissioned; blind peer-reviewed.