
Abstract
High-touch surfaces contributing to infection transmission are particularly concerning in the ophthalmology clinic where frequent contact exists between ophthalmologists and various ophthalmic instruments. Areas of surface contamination from an ophthalmologist’s contact with the slit lamp environment were identified using ultraviolet fluorescence as a surrogate for pathogen contamination. Ultraviolet fluorescent product was applied on the ophthalmologist’s hands after thorough hand washing to indicate the contamination that may be derived from multiple sources in the ophthalmology clinic, such as touching the patient or the patient’s folder during eye examinations and transfers. The ophthalmology clinic was run normally, with the ophthalmologist wiping down patient-contact surfaces on the slit lamp and performing thorough hand hygiene after every patient. Using ultraviolet black light, persistence of surface contamination in the slit lamp environment was identified and evaluated across five days. High-touch surfaces of suboptimal disinfection were inclined towards those touched only by the ophthalmologist, for example: joystick and chin-rest adjustment knob, as compared to patient-contact surfaces. Persistent contamination on the same surfaces revealed inefficacy of current hand hygiene and clinical disinfection practices. This poses a significant risk for pathogen transmission and underscores the importance of including these specific clinician high-touch surfaces in existing cleaning protocols.
Keywords
Background
High-touch surfaces in the clinical setting are a significant culprit in the spread of nosocomial infections. This is of particular concern in ophthalmology clinics, where healthcare professionals utilise equipment liable to frequent contact. Researchers have detected Methicillin-resistant Staphylococcus aureus on headrests and chin-rests of slit lamps, indicating risks of pathogen transmission via high-touch surfaces should there be suboptimal disinfection of surfaces between patients (Reem et al., 2014: 781–787.e2).
Regular cleaning and disinfection practices are mandated and outsourced to qualified cleaning personnel at the designated ophthalmology clinic of this investigation. Terminal room cleaning is conducted at the end of each workday. Room assistants and clinicians wipe down instrument surfaces before clinic sessions and between patients. However, these processes are fallible, exposing patients and healthcare staff to infection transmission risks. We documented surface contamination from an ophthalmologist’s contact with the slit lamp environment using fluorescent powder and oil as a surrogate marker and evaluated for the persistence of contamination across multiple days to assess the efficacy of current ophthalmic disinfection practices. In daily ophthalmic practice, multiple sources of pathogen transmission exist – for example, handling of patient folders and appointment cards between instances of hand hygiene, and touching of the patient during examination and transfer. These are possible sources of fomite transmission to the ophthalmologist’s hands, causing them to harbour pathogens despite prior hand hygiene, even before any eye examination has been performed. Hence, we sought to bring to attention specific high-touch surfaces that may be neglected during cleaning and further contribute to infection transmission.
Methods
This investigation was performed in accordance with the tenets of the Declaration of Helsinki, and institutional review board approval was not needed. Following thorough cleaning of the slit lamp surface and ophthalmologist’s hands, surfaces were first examined with ultraviolet black light (Glo Germ Company, Moab, UT) to ensure null contamination. Fluorescent powder and oil (Glo Germ Company, Moab, UT) were then applied to the ophthalmologist’s hands as a surrogate marker for contamination from either a patient or the clinic surroundings. Consultations were conducted in the usual manner, with use of the slit lamp (Haag-Streit BM900, Germany) as indicated. The ophthalmologist performed strict hand hygiene and cleaned patient-contact surfaces on the slit lamp with 70% isopropyl alcohol wipes between patients. This has been assessed to be effective in removing traces of fluorescent powder and oil prior to the commencement of the investigation. Surfaces were re-examined at the end of the day with the same ultraviolet black light, revealing areas of fluorescence which represented contaminated surfaces. The slit lamp was subsequently utilised by other ophthalmologists with no further application of fluorescent-based substances on their hands. Surfaces were re-examined on day 3 and day 5 with photographic documentation of fluorescent areas. The photographs captured were compared, with identified areas of persistent fluorescence illustrated (Figure 1).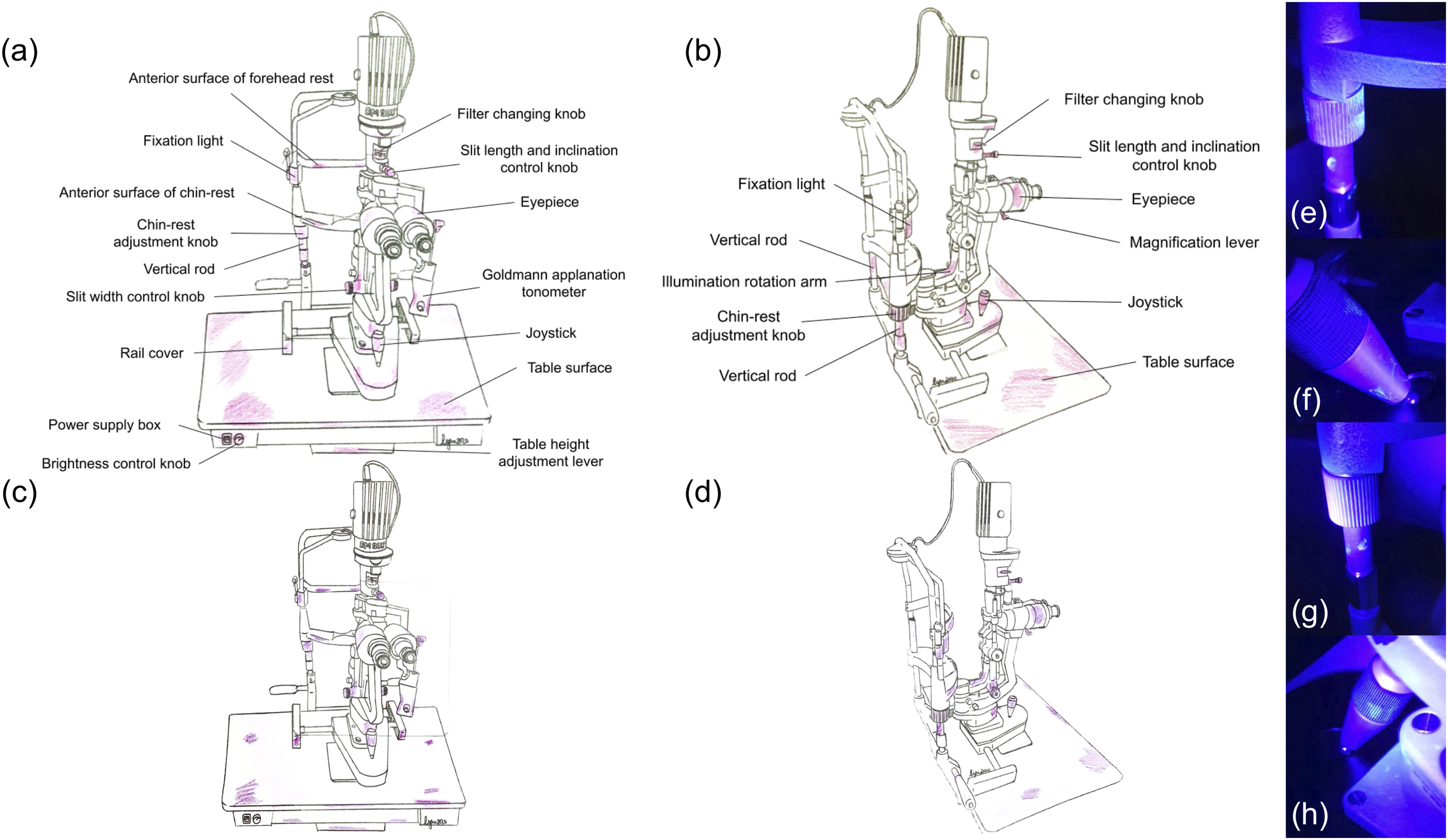
Results
The slit lamp and table surfaces with fluorescent areas on day 1 were highlighted and labelled on illustrations of the slit lamp (Figure 1(a) and (b)). On days 3 and 5, similar surfaces on the same slit lamp and table were found to retain contamination from the fluorescent powder and oil – these surfaces were thus marked out in two other slit lamp illustrations (Figure 1(c) and (d)).
Although areas of contamination were demonstrated to be reduced on days 3 and 5 following the usual disinfection protocols, all identified surfaces retained evidence of contamination persisting across all 5 days (Figure 1(c) and (d)). This suggests that strict adherence to hand hygiene practice and wiping down of patient-contact surfaces (e.g. forehead rest and chin-rest) before examining each patient were insufficient to prevent persistent contamination, as there were many other clinician high-touch surfaces (e.g. eyepiece and joystick) on the slit lamp that have been overlooked during disinfection.
Discussion
Thorough disinfection of high-touch surfaces is particularly crucial in light of the coronavirus disease 2019 (COVID-19) pandemic. Notably, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has been isolated from ophthalmic surfaces (Aytogan et al., 2020: 990–993) and can remain infectious for days (Van Doremalen et al., 2020: 1564–1567). During this period, contaminated surfaces can be prime sources of pathogen transmission the longer they are left poorly disinfected. The identification of ophthalmic high-touch surfaces thus brings particular surfaces to attention for disinfection which may occur on oversight in the interest of time during cursory cleaning. Furthermore, it is evidenced that SARS-CoV-2 can be transmitted by presymptomatic, asymptomatic and mildly symptomatic individuals (Furukawa et al., 2020). As there are difficulties in distinguishing them from uninfected individuals based on respiratory symptoms alone, entry may be unknowingly granted to these individuals. These potentially SARS-CoV-2 positive patients may shed respiratory droplets that contaminate various surfaces in the clinic environment, which in turn becomes a dangerous source for silent pathogen transmission. Thus, by including identified high-touch surfaces specifically in existing cleaning protocols, pathogen transmission risk may be reduced. This is especially significant in light of the limitations presented by hand hygiene practices highlighted in our investigation.
Apart from the limitations of hand hygiene, persistence of high-touch surface contamination is also decidedly concerning. While alcohol has no detergent properties, it is recommended that all components of the slit lamp are wiped down with 70% alcohol (Haag-Streit Diagnostics, 2020). A systematic review by Schabrun and Chipchase has demonstrated the utility of 70% alcohol in achieving a mean reduction of surface contamination by 82.1% across 12 studies (Schabrun and Chipchase, 2006: 239–245). The review, however, acknowledged the limitations in the quality of data analysed and variations in the types of equipment evaluated for contamination, along with no standardised protocols for cleaning that may affect the results. For our study, we similarly acknowledge that real world efficacy is likely to be further curtailed by a range of other factors. This is evidenced in a further study whereby comparison of experimental and field studies showed discrepancies in cleaning efficacy of alcohol wipes (Ribeiro et al., 2015: 741–752).
This demonstrates a need for a cleaning solution that would circumvent real-world limitations. For example, irregular surfaces may hinder thorough cleaning (Ellis et al., 2018: 906–912). Intrinsic design issues of the slit lamp that compromises effective cleaning include ridges on various knobs and tight spaces that are difficult to reach with current cleaning strategies. These surfaces have demonstrated persistent contamination in our study. Despite an emphasis on training clinical staff in disinfection procedures for clinical equipment, thorough disinfection is still limited by short turnaround times between patients in high patient volume practices. Time constraints may necessitate prioritisation of certain patient-contact surfaces with cursory disinfection of other areas. Furthermore, human errors are inevitable, and lapses in the stringency of disinfection protocols can occur – this can be circumvented by reduced dependency on manual disinfection through automated cleaning technologies.
A limitation of this investigation is that the contributory role of patients and other healthcare staff in surface contamination was not explored. However, this was deliberately omitted to identify persistent surface contamination solely by the treating ophthalmologist. Future studies investigating contamination of clinic surfaces through interactions amongst clinic staff and patients will be enlightening in this regard. Another limitation of this study involves the use of fluorescent markers as a surrogate for contamination. This may not be reflective of other contributing components to persistent contamination such as biofilm formation. However, well-established evidence surrounding transmission of hospital-associated pathogens through contaminated surfaces in the environment already exists (Weber et al., 2013: 338–344), and the aim of this study was to identify specific surfaces where these pathogens reside in the ophthalmology clinic for implementation of preventive disinfection measures. Lastly, high-touch surfaces were identified by the presence of persistent contamination at the end of days 1, 3 and 5. This does not account for contact frequency of these surfaces during consultations. Future studies could include observation of clinic activity to yield a proper assessment of the number of contact-episodes for the high-touch surfaces.
In conclusion, although surface cleaning appears intuitive, the type of surface, ease and convenience of cleaning, availability of cleaning products and lack of awareness of high-touch surfaces may affect thoroughness of cleaning. High patient volumes requiring short turnover of clinic spaces may also perpetuate suboptimal cleaning regimens. Additionally, the emergence of undetected presymptomatic or asymptomatic COVID-19 cases in the community warrants more stringent disinfection measures in clinic spaces to curb any silent disease transmission. Disinfection efforts may be supplemented by implementing technologies such as self-disinfecting coatings and ultraviolet light based disinfection systems, in tandem with recommended public health measures, to improve disinfection efficacy and infection control (Boyce, 2016: 10).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.