One of today’s most significant organizational priorities, including healthcare organizations, is to improve the quality of work-life (QoWL), which leads to offering high-quality services to patients.
Aim
The study aimed to explore the effect of the perceived risk of infection and its impact on the quality of work-life (QoWL) on HCWs during the COVID-19 pandemic.
Methods
A cross-sectional survey was conducted on 484 healthcare workers. Respondents were recruited using convenience sampling methods.
Results
: The study findings revealed a better QoWL with a decreased perceived risk of COVID-19 infection.
Conclusion
Increasing the quality of work life will be reflected in adherence to health protocols, which creates a work environment capable of dealing with challenges, including the risk of infection such as COVID-19.
The quality of work-life (QoWL) has recently become a major global social issue and one of today's most important organizational goals. QoWL is among the most significant factors for many healthcare organizations (Lebni et al., 2021). Improving the quality of work-life for HCWs is critical to the healthcare system's long-term viability and ability to offer patients high-quality services (Spence Laschinger, 2008; Ortega-Soto, 2019; Suleiman et al., 2019) and essential in maintaining its long-term strategic plan. Organizational performance and lower turnover may be achieved by organizations that focus on providing the highest possible quality of work-life (Afroz, 2017).
Different studies have examined the QoWL impact on the quality of service offered to patients worldwide, as working pressures and a lack of suitable stress management techniques may affect the psychological and physical well-being of medical professionals (Laserna Jiménez et al., 2021; Lebni et al., 2021). The QoWL is essential to healthcare institution management, and they constantly strive to improve it through their human resource department (Hemanathan et al., 2017).
Methods
A quantitative, cross-sectional design was carried out using Google Forms, an online platform, from May 10th to June 30th, 2021. A well-adapted instrument was created and used for data collection based on the available literature (Van Laar et al., 2007; Peres et al., 2020; Wong et al., 2020; Saadeh et al., 2022). The google-form questionnaire was disseminated through social media platforms, groups, and pages, to the HCWs working at different public, private, military, and Jordanian university hospitals. To promote the self-reported questionnaire to HCWs, the researcher produced, uploaded, and administered it to all healthcare workers' official public and private channels. For this research, three primary dimensions were used: socio-demographic and participants' work profiles, QoWL, and finally, the perceived risk of infection due to the hospital workplace.
Study participants
The research population included healthcare personnel from various specialties and institutions in Jordan, including 117 different hospitals. The population included physicians (general practitioners, specialists, consultants), dentists, pharmacists (pharmacists and clinical pharmacists), nurses, midwives, laboratory technicians, radiology technicians, and other medical staff actively working in a Jordanian hospital. The sample chosen in the study was convenience sampling.
Research instrument
The self-reported questionnaire, which includes three significant parts, was used in the study. The questionnaire contained the following:
Part 1: Socio-demographic and participants' work profiles
This section included 11 items. Study variables were as follows: age, gender, marital status, having children at home, having care responsibilities toward the elderly parents at home, educational level, healthcare institution (public, private/NGO, military, or university), professional classification (physician, general practitioner, specialist, consultant, nurse, pharmacist/clinical pharmacist, midwives, laboratory technicians, radiology technicians, paramedics, and other healthcare staff), years of experience, employment-status (full-time, part-time), and the health status.
Part 2: Work-related quality of Life (WRQoL) scale
The WRQoL scale has been demonstrated to be a psychometrically robust scale based on six subscales, with excellent reliability and validity (Van Laar, Edwards, and Easton, 2007; Easton and Van Laar, 2013). Job and Career Satisfaction (JCS), General Well-Being (GWB), Stress at Work (SAW), Control at Work (CAW), Home-Work Interface (HWI), and Working Conditions (WCS) were the six elements utilized to construct the 24-item WRQoL scale. These six factors are based on replies to 23 items. The addition of a 24th item, “I am satisfied with the overall quality of my working life,” is a measure of overall WRQoL, is not included in the total score, and is used as an indicator of construct validity when correlated with participants' scores. The Overall WRQoL factor score is determined by finding the average of all 23 WRQoL items (not including the 24th “Overall” item), please see table number 2.
Part 3: Perception risk of infection due to COVID-19 by occupational groups
This section measured the perceived risk of infection due to the workplace (Peres et al., 2020), including six items and by using a 4-point scale.
1. “What is the probability of you being infected with this virus?”
2. “What is the probability of your family/friends being infected with this virus?”
3. “How effective do you think ‘prophylactic isolation’ (quarantine) is in controlling this virus?”
4. “How prepared are Health Services to deal with this virus?”
5. “What is the level of communication adequacy of the Health Authorities with the population?”
6. “When will it be possible to control this pandemic at the Jordanian level?” (In months)
Data analysis
Descriptive statistics and frequencies were estimated using the custom tables procedure. The data were tested for normality using Kolmogorov–Smirnov test of normality. However, the data were not normally distributed; thus, non-parametric tests were used in the analyses. Pearson correlation and Regression analysis were performed to verify our model and hypotheses.
Ethical considerations
The protocol of this study was reviewed and approved by the Institutional Review Board (IRB) at Jordan University of Science and Technology in Jordan (Reference Number:2021/140/48).
Results
Perception risk of infection by HCWs
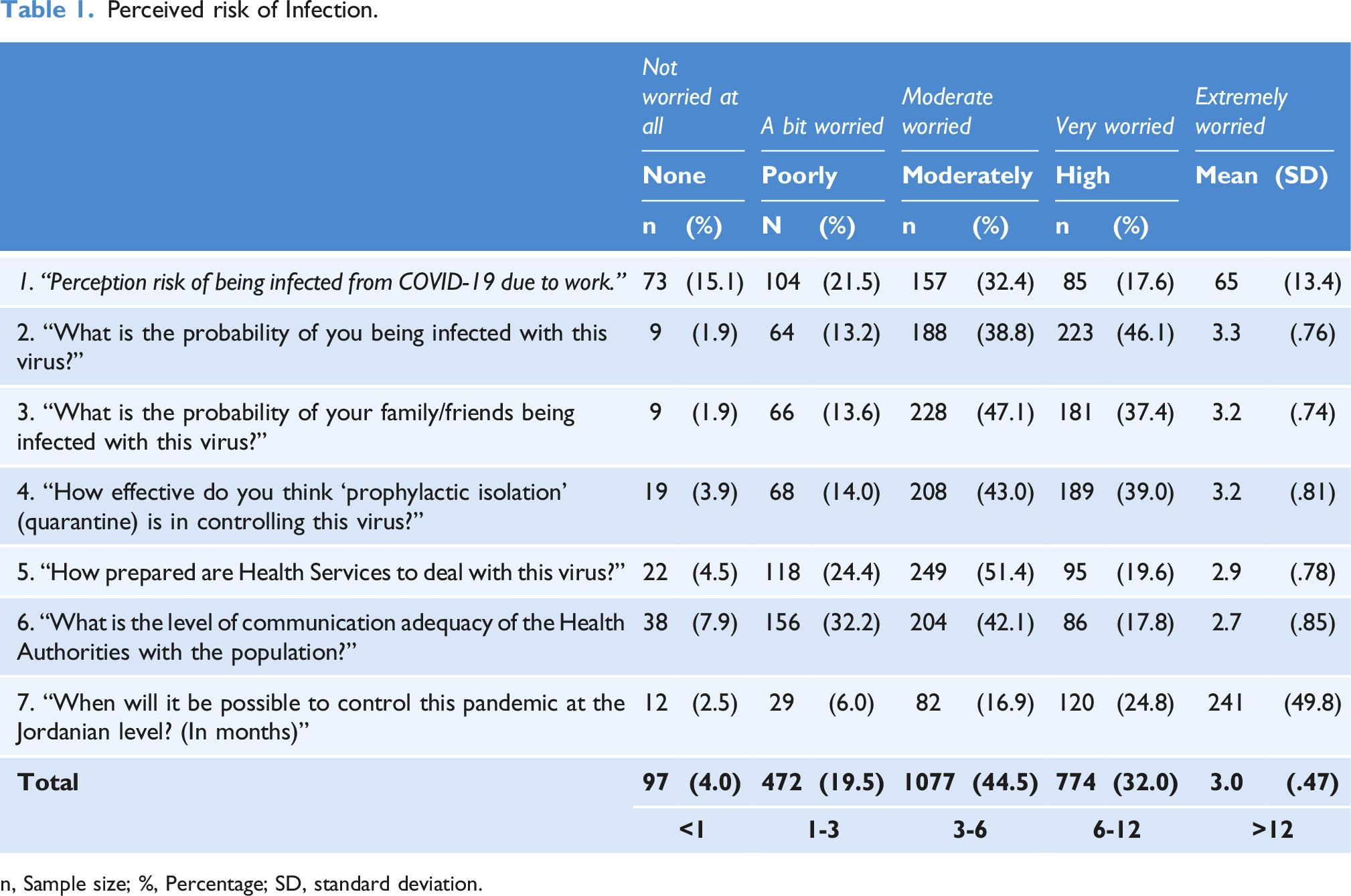
The majority (84.9%) of respondents reported a moderate or high probability of being infected with COVID-19 (Table 1). Similarly, 84.5% reported a moderate or high probability of one family member being infected. About 82% reported moderate or high efficiency of prophylactic isolation (quarantine) in controlling this pandemic. Nevertheless, only 71% reported that health services are moderately or highly prepared to deal with the virus. Furthermore, only 59.9% of respondents said the medical associations' contact with the general public was moderate to excellent. Nearly half of the respondents said more than 12 months would be needed to control the pandemic on the national level.
Perceived risk of Infection.
Not worried at all
A bit worried
Moderate worried
Very worried
Extremely worried
None
Poorly
Moderately
High
Mean
(SD)
n
(%)
N
(%)
n
(%)
n
(%)
1. “Perception risk of being infected from COVID-19 due to work.”
73
(15.1)
104
(21.5)
157
(32.4)
85
(17.6)
65
(13.4)
2. “What is the probability of you being infected with this virus?”
9
(1.9)
64
(13.2)
188
(38.8)
223
(46.1)
3.3
(.76)
3. “What is the probability of your family/friends being infected with this virus?”
9
(1.9)
66
(13.6)
228
(47.1)
181
(37.4)
3.2
(.74)
4. “How effective do you think ‘prophylactic isolation’ (quarantine) is in controlling this virus?”
19
(3.9)
68
(14.0)
208
(43.0)
189
(39.0)
3.2
(.81)
5. “How prepared are Health Services to deal with this virus?”
22
(4.5)
118
(24.4)
249
(51.4)
95
(19.6)
2.9
(.78)
6. “What is the level of communication adequacy of the Health Authorities with the population?”
38
(7.9)
156
(32.2)
204
(42.1)
86
(17.8)
2.7
(.85)
7. “When will it be possible to control this pandemic at the Jordanian level? (In months)”
12
(2.5)
29
(6.0)
82
(16.9)
120
(24.8)
241
(49.8)
Total
97
(4.0)
472
(19.5)
1077
(44.5)
774
(32.0)
3.0
(.47)
<1
1-3
3-6
6-12
>12
n, Sample size; %, Percentage; SD, standard deviation.
Work-related quality of Life Scale
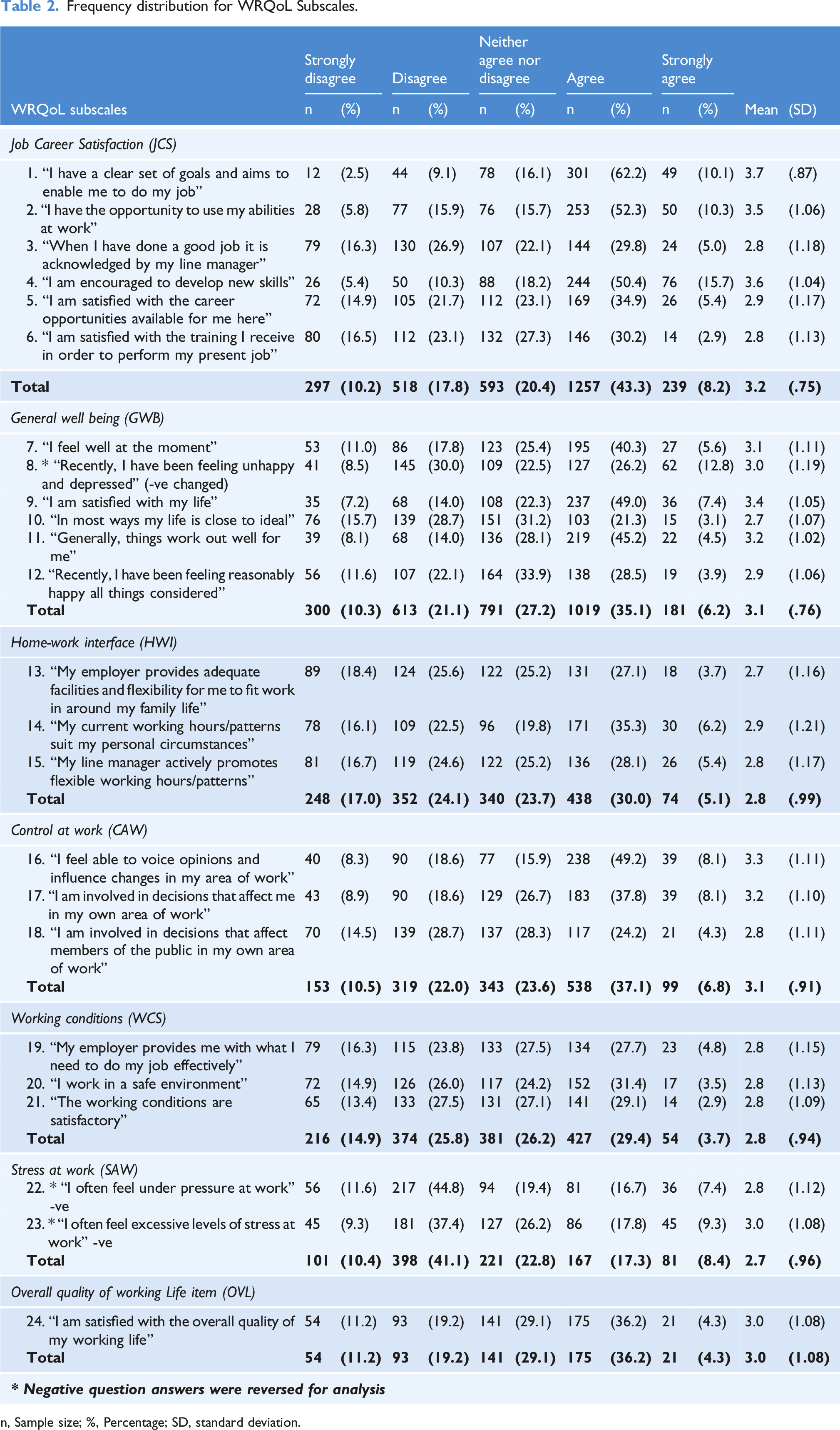
Table 2 shows the WRQoL subscales; the first is Job Career Satisfaction (JCS) items, and the second is General Well-Being (GWB) items. It is clear that more than 50% of the respondents either agreed or strongly agreed with the items on the JCS. This is judged by the mean total of 3.2 out of 5 scores on this subscale. While less than half (41.3%) of the respondents either agreed or strongly agreed with the items of the GWB subscale. For the third subscale, which is Home-Work Interface (HWI), about 41.1% of the respondents were in disagreement with the items of this subscale. This means there was a higher disagreement on the HWI. For the fourth subscale, which is Control at Work (CAW) items, about 44% of the respondents either agreed or strongly agreed with the items of the CAW subscale. On the other hand, 40.7% of the respondents were in disagreement with the items on Working Conditions (WCS) subscale. Clearly, there was a relatively high level of Stress at Work (SAW) among respondents. About half (51.5%) of the respondents either agreed or strongly agreed that they feel under pressure or excessive stress at work. The last section of the table presents the respondents' satisfaction with the overall quality of their working life, with current OVL giving a mean of 3.0 out of 5 scores.
Frequency distribution for WRQoL Subscales.
WRQoL subscales
Strongly disagree
Disagree
Neither agree nor disagree
Agree
Strongly agree
Mean
(SD)
n
(%)
n
(%)
n
(%)
n
(%)
n
(%)
Job Career Satisfaction (JCS)
1. “I have a clear set of goals and aims to enable me to do my job”
12
(2.5)
44
(9.1)
78
(16.1)
301
(62.2)
49
(10.1)
3.7
(.87)
2. “I have the opportunity to use my abilities at work”
28
(5.8)
77
(15.9)
76
(15.7)
253
(52.3)
50
(10.3)
3.5
(1.06)
3. “When I have done a good job it is acknowledged by my line manager”
79
(16.3)
130
(26.9)
107
(22.1)
144
(29.8)
24
(5.0)
2.8
(1.18)
4. “I am encouraged to develop new skills”
26
(5.4)
50
(10.3)
88
(18.2)
244
(50.4)
76
(15.7)
3.6
(1.04)
5. “I am satisfied with the career opportunities available for me here”
72
(14.9)
105
(21.7)
112
(23.1)
169
(34.9)
26
(5.4)
2.9
(1.17)
6. “I am satisfied with the training I receive in order to perform my present job”
80
(16.5)
112
(23.1)
132
(27.3)
146
(30.2)
14
(2.9)
2.8
(1.13)
Total
297
(10.2)
518
(17.8)
593
(20.4)
1257
(43.3)
239
(8.2)
3.2
(.75)
General well being (GWB)
7. “I feel well at the moment”
53
(11.0)
86
(17.8)
123
(25.4)
195
(40.3)
27
(5.6)
3.1
(1.11)
8. * “Recently, I have been feeling unhappy and depressed” (-ve changed)
41
(8.5)
145
(30.0)
109
(22.5)
127
(26.2)
62
(12.8)
3.0
(1.19)
9. “I am satisfied with my life”
35
(7.2)
68
(14.0)
108
(22.3)
237
(49.0)
36
(7.4)
3.4
(1.05)
10. “In most ways my life is close to ideal”
76
(15.7)
139
(28.7)
151
(31.2)
103
(21.3)
15
(3.1)
2.7
(1.07)
11. “Generally, things work out well for me”
39
(8.1)
68
(14.0)
136
(28.1)
219
(45.2)
22
(4.5)
3.2
(1.02)
12. “Recently, I have been feeling reasonably happy all things considered”
56
(11.6)
107
(22.1)
164
(33.9)
138
(28.5)
19
(3.9)
2.9
(1.06)
Total
300
(10.3)
613
(21.1)
791
(27.2)
1019
(35.1)
181
(6.2)
3.1
(.76)
Home-work interface (HWI)
13. “My employer provides adequate facilities and flexibility for me to fit work in around my family life”
89
(18.4)
124
(25.6)
122
(25.2)
131
(27.1)
18
(3.7)
2.7
(1.16)
14. “My current working hours/patterns suit my personal circumstances”
78
(16.1)
109
(22.5)
96
(19.8)
171
(35.3)
30
(6.2)
2.9
(1.21)
15. “My line manager actively promotes flexible working hours/patterns”
81
(16.7)
119
(24.6)
122
(25.2)
136
(28.1)
26
(5.4)
2.8
(1.17)
Total
248
(17.0)
352
(24.1)
340
(23.7)
438
(30.0)
74
(5.1)
2.8
(.99)
Control at work (CAW)
16. “I feel able to voice opinions and influence changes in my area of work”
40
(8.3)
90
(18.6)
77
(15.9)
238
(49.2)
39
(8.1)
3.3
(1.11)
17. “I am involved in decisions that affect me in my own area of work”
43
(8.9)
90
(18.6)
129
(26.7)
183
(37.8)
39
(8.1)
3.2
(1.10)
18. “I am involved in decisions that affect members of the public in my own area of work”
70
(14.5)
139
(28.7)
137
(28.3)
117
(24.2)
21
(4.3)
2.8
(1.11)
Total
153
(10.5)
319
(22.0)
343
(23.6)
538
(37.1)
99
(6.8)
3.1
(.91)
Working conditions (WCS)
19. “My employer provides me with what I need to do my job effectively”
79
(16.3)
115
(23.8)
133
(27.5)
134
(27.7)
23
(4.8)
2.8
(1.15)
20. “I work in a safe environment”
72
(14.9)
126
(26.0)
117
(24.2)
152
(31.4)
17
(3.5)
2.8
(1.13)
21. “The working conditions are satisfactory”
65
(13.4)
133
(27.5)
131
(27.1)
141
(29.1)
14
(2.9)
2.8
(1.09)
Total
216
(14.9)
374
(25.8)
381
(26.2)
427
(29.4)
54
(3.7)
2.8
(.94)
Stress at work (SAW)
22. * “I often feel under pressure at work” -ve
56
(11.6)
217
(44.8)
94
(19.4)
81
(16.7)
36
(7.4)
2.8
(1.12)
23. * “I often feel excessive levels of stress at work” -ve
45
(9.3)
181
(37.4)
127
(26.2)
86
(17.8)
45
(9.3)
3.0
(1.08)
Total
101
(10.4)
398
(41.1)
221
(22.8)
167
(17.3)
81
(8.4)
2.7
(.96)
Overall quality of working Life item (OVL)
24. “I am satisfied with the overall quality of my working life”
54
(11.2)
93
(19.2)
141
(29.1)
175
(36.2)
21
(4.3)
3.0
(1.08)
Total
54
(11.2)
93
(19.2)
141
(29.1)
175
(36.2)
21
(4.3)
3.0
(1.08)
* Negative question answers were reversed for analysis
n, Sample size; %, Percentage; SD, standard deviation.
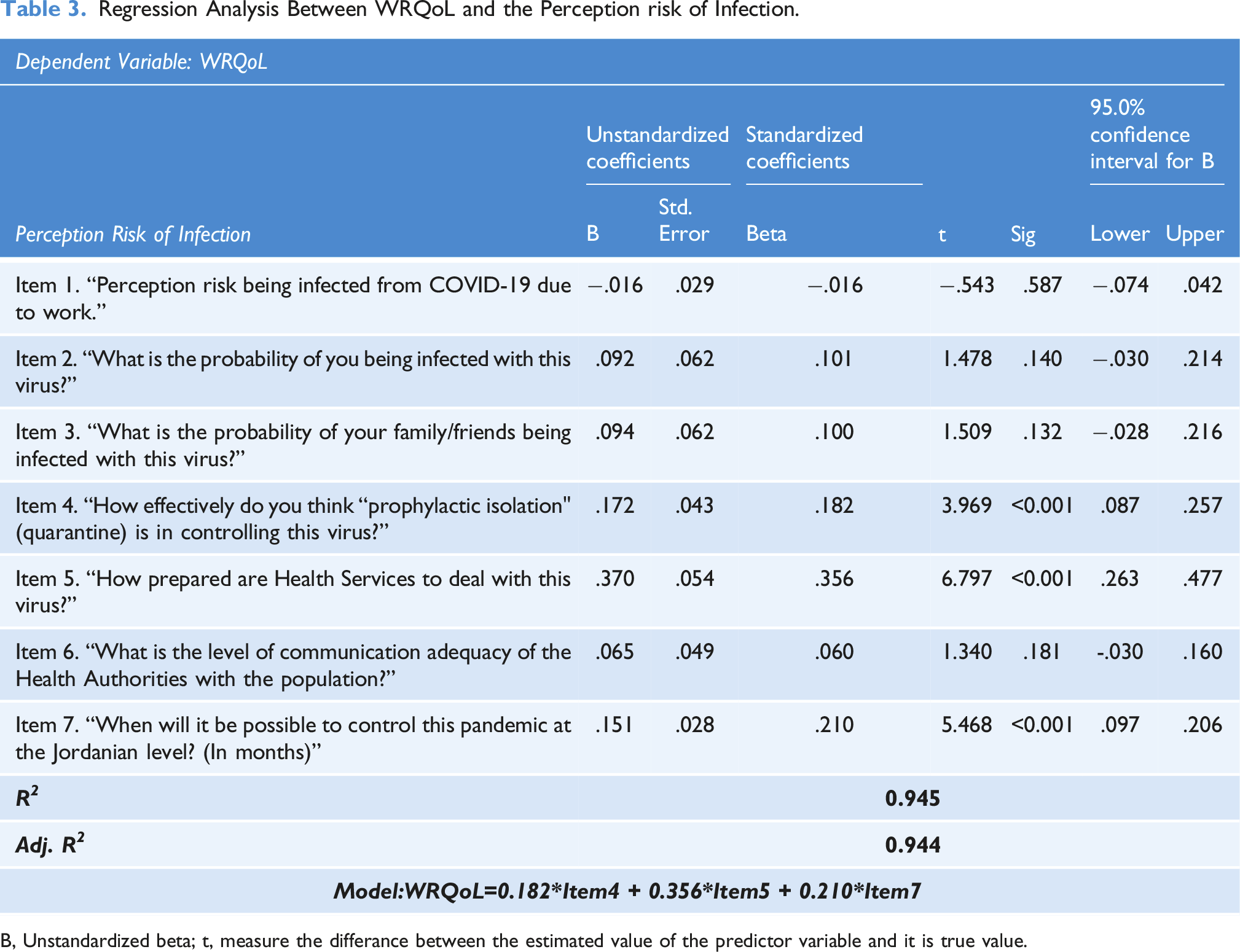
The research hypothesis states that the better the quality of life the lower the perceived risk of infection. Risk perception items in Table 3 were regressed against the WRQoL. The model shows that only three items of the perceived risk scale are in positive correlation and affect WRQoL; the perceived effectiveness of prophylactic isolation (Item4), the perceived preparedness of health authorities to deal with the pandemic (Item5), and the expectation for the period needed to control the pandemic at the local level (Item7). The last item suggests the perceived ability of the authorities to control the pandemic on time.
Regression Analysis Between WRQoL and the Perception risk of Infection.
Dependent Variable: WRQoL
Perception Risk of Infection
Unstandardized coefficients
Standardized coefficients
t
Sig
95.0% confidence interval for B
B
Std. Error
Beta
Lower
Upper
Item 1. “Perception risk being infected from COVID-19 due to work.”
−.016
.029
−.016
−.543
.587
−.074
.042
Item 2. “What is the probability of you being infected with this virus?”
.092
.062
.101
1.478
.140
−.030
.214
Item 3. “What is the probability of your family/friends being infected with this virus?”
.094
.062
.100
1.509
.132
−.028
.216
Item 4. “How effectively do you think “prophylactic isolation" (quarantine) is in controlling this virus?”
.172
.043
.182
3.969
<0.001
.087
.257
Item 5. “How prepared are Health Services to deal with this virus?”
.370
.054
.356
6.797
<0.001
.263
.477
Item 6. “What is the level of communication adequacy of the Health Authorities with the population?”
.065
.049
.060
1.340
.181
-.030
.160
Item 7. “When will it be possible to control this pandemic at the Jordanian level? (In months)”
B, Unstandardized beta; t, measure the differance between the estimated value of the predictor variable and it is true value.
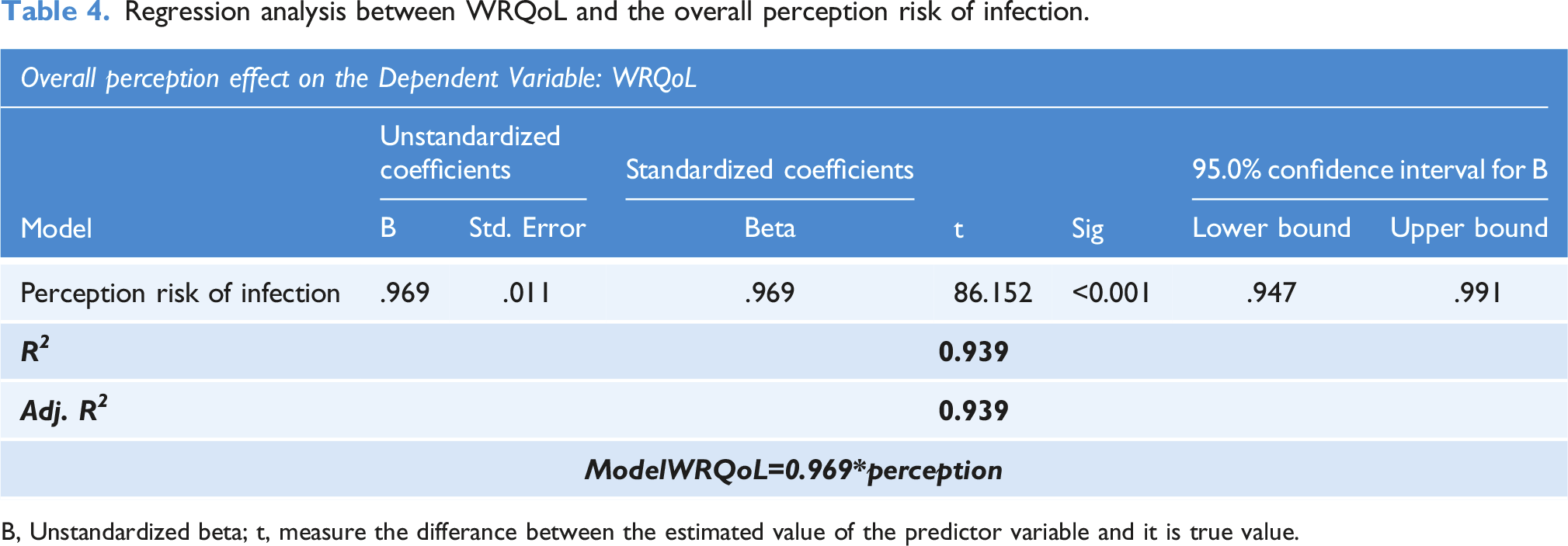
To sum up this hypothesis, Table 4 and the model below shows a high positive correlation between the perception of the ability to tackle the risk of the pandemic and the work quality of life (β = 0.969, 95% CI: [0.947–0.991], p < .001).
Regression analysis between WRQoL and the overall perception risk of infection.
Overall perception effect on the Dependent Variable: WRQoL
Model
Unstandardized coefficients
Standardized coefficients
t
Sig
95.0% confidence interval for B
B
Std. Error
Beta
Lower bound
Upper bound
Perception risk of infection
.969
.011
.969
86.152
<0.001
.947
.991
R2
0.939
Adj. R2
0.939
ModelWRQoL=0.969*perception
B, Unstandardized beta; t, measure the differance between the estimated value of the predictor variable and it is true value.
Discussion
The current study findings supported the research hypothesis; it revealed that the perceived ability to deal with the risk of becoming infected was significantly associated with higher QoWL of HCWs in Jordanian hospitals. The findings showed a considerable positive influence of the overall perceived risk of infection during the pandemic on the WRQoL score, with a good fit of the proposed model (Adj. R2 = 0.939).
In line with Wong et al. (2020), in which 58% of occupational groups reported moderate to extreme concerns about being infected at work, our findings revealed that more than half of HCWs (63.4%) were moderate to extremely worried about contracting COVID-19 at work. A similar result was also reported by Abdelghani, in which Egyptian physicians' fear of COVID-19 infection was significantly associated with anxiety, depression, burnout, emotional fatigue, and depersonalization symptoms. On the other hand, negatively with quality of life measures (Abdelghani et al., 2020).
Consistent with the literature, much research has explored the psychological impact of COVID-19 on frontline workers after the World Health Organization proclaimed the disease to be an international pandemic (Afulani et al., 2021). Qualitative research of HCWs in China showed that exhaustion from continuous use of personal protective equipment, heavy workloads, anxiety of caring for infected persons and the fear of spreading infection to someone else were among the obstacles experienced in responding to COVID-19. At the same time, support network and consciousness approaches helped HCWs cope with frustration (Liu et al., 2020). Furthermore, a systematic review discovered that HCWs are suffering psychological distress as a result of the COVID-19 pandemic, including the following averaged values for anxiousness (26%), depression (25%), discomfort (35%), pressure (40%), sleeplessness (32%), and PTSD (3% to 16%) (Luo et al., 2020). None of these investigations were conducted in Africa (Afulani et al., 2021).
On the other hand, healthcare professionals in African contexts have been operating under high workloads and in psychologically charged circumstances where demand exceeds capacity due to a lack of employees and restricted resources (Amnesty International, 2020; Chersich et al., 2020).
COVID-19 is a highly contagious infection, and understanding of Covid is now more advanced. The hospital-related risk of COVID-19 is a considerable reward for HCWs, especially frontline nurses who play a critical role throughout the patient-care spectrum. During the COVID-19 pandemic, keeping nurses healthy physically and psychologically is crucial. Nurses in China have been protected against infection by several practical measures used in clinical practice. In order to prevent overstressing the nursing staff, it is essential to formulate a satisfactory work schedule, promote hand hygiene in the wards, properly dispose of medical waste, continue to educate nurses on the proper use of personal protective equipment (PPE), sterilize patient care equipment, and manage occupational exposure (Huang et al., 2020).
Conclusion
Psychological health is as vital as physical health, but frontline nurses aren't getting enough help to enhance their psychological health (Søvold et al., 2021). During the COVID-19 pandemic, the WHO released a recommendation in March 2020 emphasizing the need to monitor healthcare workers' mental and psychosocial well-being (WHO, 2020). As a result, health care personnel required psychological help and counseling to cope with the COVID-19 outbreak. Additional studies are needed to determine the best psychosocial intervention for nurses dealing with the COVID-19 pandemic (Li et al., 2021).
Footnotes
Acknowledgements
We would like to thank the deanship of research in Jordan University of Science and Technology.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Orcid iD
Main Naser Alolayyan
References
1.
AbdelghaniMEl-GoharyHMFouadE, et al. (2020) Addressing the relationship between perceived fear of COVID-19 virus infection and emergence of burnout symptoms in a sample of Egyptian physicians during COVID-19 pandemic: a cross-sectional study. Middle East Current Psychiatry27(1). DOI: 10.1186/s43045-020-00079-0
2.
AfrozS (2017) Quality of work life: a conceptual model. Advances in Economics and Business Management (AEBM)4(8): 570–578.
3.
AfulaniPAGyamerahAONutorJJ, et al. (2021) Inadequate preparedness for response to COVID-19 is associated with stress and burnout among healthcare workers in Ghana. PLoS One16(4 April): 1–20. DOI: 10.1371/journal.pone.0250294
ChersichMFGrayGFairlieL, et al. (2020) Covid-19 in Africa: care and protection for frontline healthcare workers. Globalization and Health16(1): 1–6. DOI: 10.1186/s12992-020-00574-3
6.
EastonSVan LaarD (2013) Evaluation of outcomes and quality of working life in the coaching setting.The Coaching Psychologist9(2): 71–77.
7.
HemanathanRSreelekhaPrakasamPGoldaM (2017) Quality of work life among nurses in a tertiary care hospital. JOJ Nurse Health Care5(4): 1–8. DOI: 10.19080/JOJNHC.2017.05.555667
8.
HuangChaolin, et al. (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. DOI: 10.1016/S0140-6736(20)30183-5
9.
Laserna JiménezCCasado MontañésICarolM, et al. (2021) Quality of professional life of primary healthcare nurses: a systematic review. Journal of Clinical Nursing, 31, 1–16. DOI: 10.1111/jocn.16015
10.
LebniJYToghroliRAbbasJ, et al. (2021) Nurses’ work-related quality of life and its influencing demographic factors at a public hospital in western Iran: a cross-sectional study. International Quarterly of Community Health Education42(1): 37–45. DOI: 10.1177/0272684X20972838
11.
LiXZhouYXuX (2021) Factors associated with the psychological well-being among frontline nurses exposed to COVID-2019 in China: a predictive study. Journal of Nursing Management29(2): 240–249. DOI: 10.1111/jonm.13146
12.
LiuQLuoDHaaseJE, et al. (2020) The experiences of healthcare providers during the COVID-19 crisis in China: a qualitative study. Lancet Global Health8(6): e790–e798. DOI: 10.1016/S2214-109X(20)30204-7
13.
LuoMGuoLYuM, et al. (2020) The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public – a systematic review and meta-analysis. Psychiatry Research291(June): 113190. DOI: 10.1016/j.psychres.2020.113190
14.
Ortega-SotoA (2019) Quality of working life of nurses in emergency service and their in- fluence on quality of care of the hospital cayetano heredia - LIMA 2017. Gaceta Científica4(2): 6–11. DOI: 10.46794/gacien.4.2.360
15.
PeresDMonteiroJAlmeidaMA, et al. (2020) Risk perception of COVID-19 among Portuguese healthcare professionals and the general population. Journal of Hospital Infection105(3): 434–437. DOI: 10.1016/j.jhin.2020.05.038
16.
SaadehRKhaderYAlyahyaM, et al. (2022) Water, sanitation, and hygiene and infection prevention and control in Jordanian hospitals in the context of COVID-19: a national assessment. Risk Management and Healthcare Policy. April, 571–582.
17.
SøvoldLENaslundJAKousoulisAA, et al. (2021) Prioritizing the mental health and well-being of healthcare workers: an urgent global public health priority. Frontiers in Public Health9: 679397. DOI: 10.3389/fpubh.2021.679397
18.
Spence LaschingerHK (2008) Effect of empowerment on professional practice environments, work satisfaction, and patient care quality: further testing the nursing worklife model. Journal of Nursing Care Quality23(4): 322–330. DOI: 10.1097/01.NCQ.0000318028.67910.6b
19.
SuleimanKHijaziZAl KalaldehM, et al. (2019) Quality of nursing work life and related factors among emergency nurses in Jordan. Journal of Occupational Health61(5): 398–406. DOI: 10.1002/1348-9585.12068
20.
Van LaarDEdwardsJAEastonS (2007) The Work-Related Quality of Life scale for healthcare workers. Journal of Advanced Nursing60(3): 325–333. DOI: 10.1111/j.1365-2648.2007.04409.x
21.
WHO (2020) Covid-19 Response in the World Health Organization AFRICAN REGION. Republic of Congo: World Health Organization Regional Office for Africa.
22.
WongEL-YHoK-FWongSY-S, et al. (2020). Views on workplace policies and its impact on health-related quality of life during coronavirus disease (COVID-19) pandemic: cross-sectional survey of employees. International Journal of Health Policy and Management, 201911(3): 1–10. DOI: 10.34172/ijhpm.2020.127