
Abstract
Background
The Center for Disease Control’s National Healthcare Safety Network (NHSN) reported increased Standardized Infection Ratios (SIRs) for hysterectomy at a large community hospital.
Objective
To promote a surgical site infection (SSI) prevention bundle implemented to reduce hysterectomy-associated SSI.
Methods
A multidisciplinary Workgroup implemented the Hysterectomy SSI Prevention Bundle in 2020 to enforce standardization of perioperative techniques. This study included all benign hysterectomies pre-implementation (n = 857) and post-implementation (n = 772). Per NHSN categorization guidelines, “abdominal hysterectomy” includes both open and laparoscopic routes. “Inpatient surgery” is date of discharge different from date of surgery; “outpatient surgery” is same date of discharge. “SSI” includes superficial, deep, and organ/space; “complex SSI” includes deep and organ/space. Patient demographics were categorized and evaluated for statistical significance.
Results
After implementation of the SSI bundle, SIRs for hysterectomy were reduced to <1.0, indicating infection prevention. Reductions in SIR were significant for outpatient abdominal hysterectomy (0.868 [p = .007]), inpatient vaginal hysterectomy (0 [p < .001]), inpatient complex abdominal hysterectomy (0 [p = .040]), and inpatient complex vaginal hysterectomy (0 [p < .001]). Differences between groups were significant for increased laparoscopic and decreased vaginal hysterectomies (p < .001), increased outpatient surgeries (p < .001), and longer procedure duration (p < .001).
Conclusion
Implementation of an SSI prevention bundle at a large community hospital has significantly reduced SIR for inpatient vaginal hysterectomies, outpatient abdominal hysterectomies, and all inpatient complex hysterectomies.
Keywords
Background
Patient demographics, surgical characteristics, and standardized infection ratios pre- and post-implementation of hysterectomy surgical site infection prevention bundle.
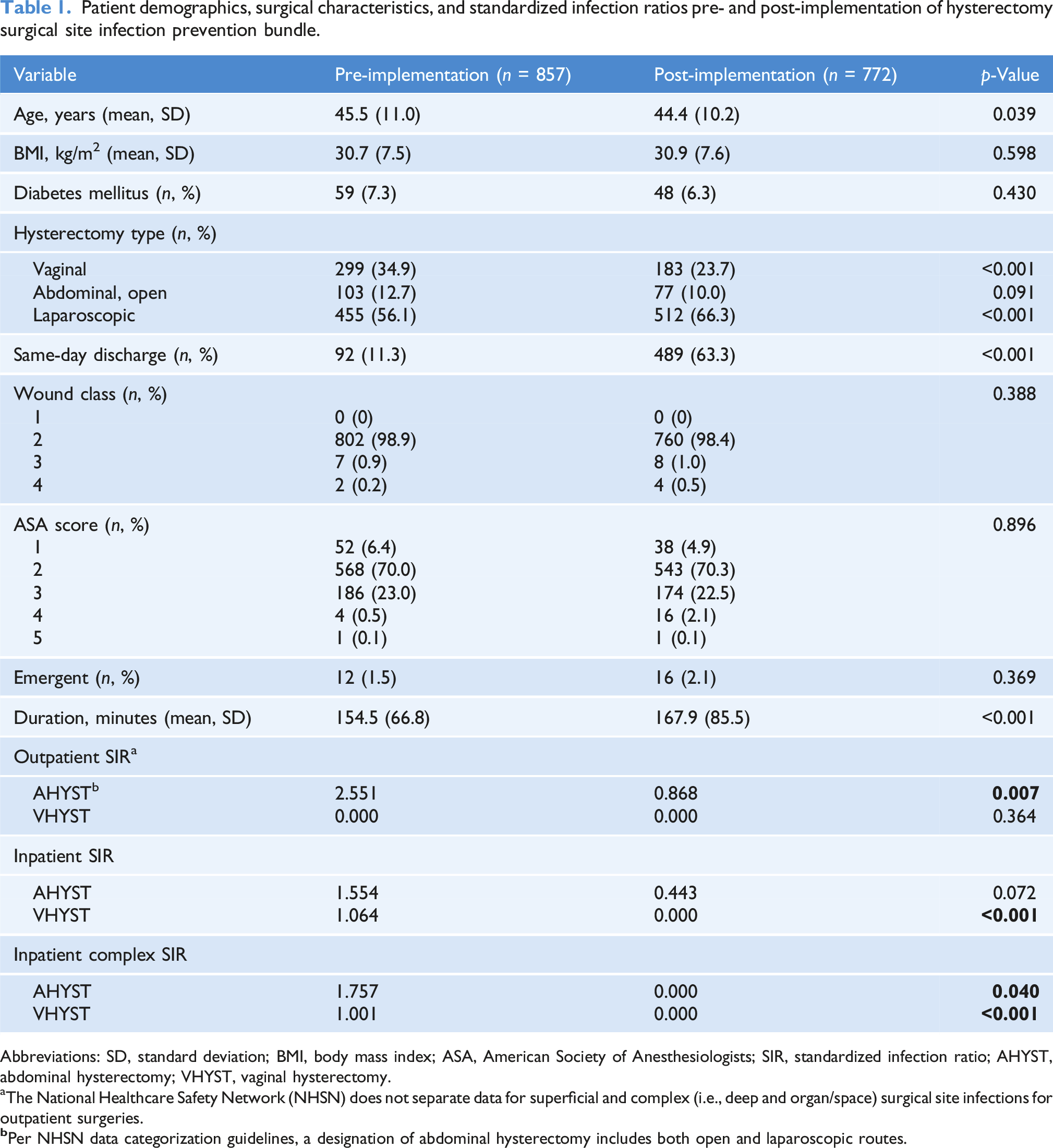
Abbreviations: SD, standard deviation; BMI, body mass index; ASA, American Society of Anesthesiologists; SIR, standardized infection ratio; AHYST, abdominal hysterectomy; VHYST, vaginal hysterectomy.
aThe National Healthcare Safety Network (NHSN) does not separate data for superficial and complex (i.e., deep and organ/space) surgical site infections for outpatient surgeries.
The aim of this quality improvement project is to promote the SSI prevention efforts implemented to reduce hysterectomy-associated SSIs, as well as provide a bundle checklist and audit form for institutions.
Methods
In response to benign hysterectomy SIR greater than 1.0 at a large community hospital in the Midwest, a multidisciplinary Hysterectomy Surgical Site Infection Prevention Workgroup was formed in 2019 with the goal of improving and maintaining all benign hysterectomy SIRs below the expected level of 1.0.
The Workgroup comprised surgeons, infectious disease specialists, operating room nurses, surgical technologists, and the director of performance improvement and created a Hysterectomy SSI Prevention Bundle adopted from a piloted and validated bundle which was created based on existing evidence from gynecologic, general surgery, and colorectal surgery literature surgery (“Prevention of Infection after Gynecologic Procedures,” 2018; Pelligrini et al., 2017; Andiman et al., 2018; Carroll et al., 2017; Chan and Nimaroff, 2022; Harris et al., 2017; Anderson et al., 2014; Bratzler and Hunt, 2006; Stulberg et al., 2010; Kwaan et al., 2016; Waits et al., 2014; Webster and Osborne, 2015; Culligan et al., 2005; Mihaljevic et al., 2015; Guo et al., 2020).
Prior to release of the Hysterectomy SSI Prevention Bundle, there was no standardization for preoperative, intra-operative, or postoperative care. The bundle was designed to standardize components and techniques at the pre-operative clinic appointment, the day of surgery, the intra-operative time prior to incision, the intra-operative time from incision to closure, and in the immediate post-operative time at the recovery area. To facilitate dissemination of bundle components and improve ease of audit compliance, the Hysterectomy SSI Prevention Bundle Checklist was created (Figure 1). During the preoperative clinic appointment, patients were provided with information about SSI, including instructions to avoid skin shaving or waxing at the surgical site within 48 hours of surgery and to complete 2% chlorhexidine gluconate (CHG) wipes the night before and the morning of surgery. On the day of surgery, patients were screened for compliance with completion of 2% CHG wipes and avoidance of shaving or waxing of the surgical site within the last 48 hours. Patients underwent preoperative blood glucose and body temperature measurements for optimization as appropriate. In the operating room, prophylactic intravenous cefazolin and metronidazole (or appropriate alternative antibiotics if allergic to standard antibiotics) were administered prior to incision, normothermia was maintained, and a standardized approach to skin and vaginal preparation and draping was taken. Intraoperatively, normothermia was maintained and antibiotics were re-dosed as appropriate based on operative time or blood loss. For abdominal closure, gloves were changed and dedicated instruments sequestered prior to the start of the case were used for incision closure, then dressing was applied in a sterile technique with date and time denoted on the dressing to maintain coverage for 24 to 48 hours postoperatively. Finally, in the postoperative recovery area, normothermia was ensured and glycemic control was optimized between 70 and 180 mg/dL. Hysterectomy Surgical Site Infection Prevention Bundle Audit Form.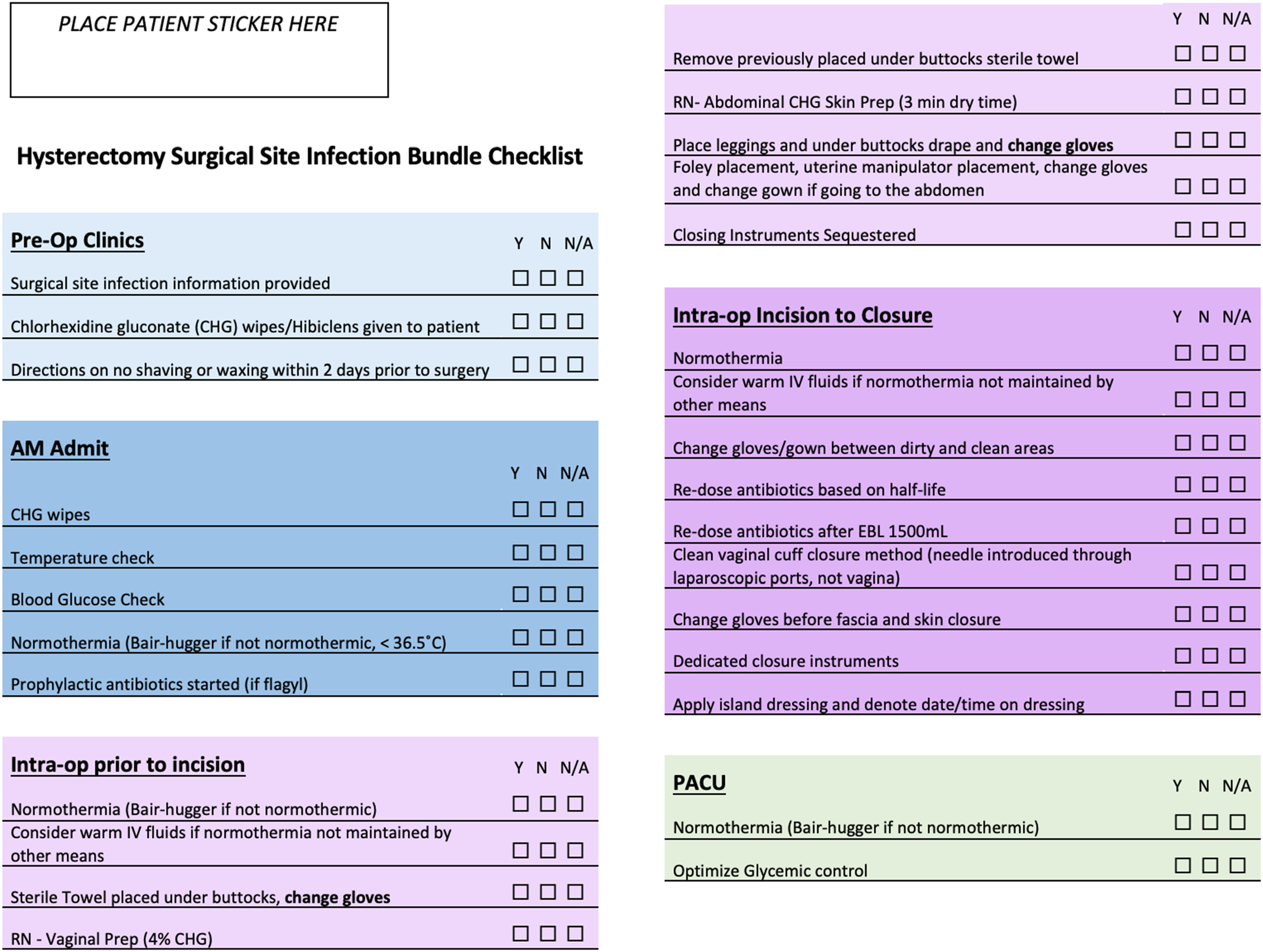
This Institutional Review Board exempt quality improvement project evaluated data from patients undergoing hysterectomy for benign indications at our large community hospital prior to and following implementation of the Hysterectomy SSI Prevention Bundle. At this 454-bed community hospital, approximately 36 benign hysterectomies are completed monthly by academic and non-academic general obstetrician-gynecologists and fellowship-trained surgeons in Urogynecology/Female Pelvic Medicine and Reconstructive Surgery (FPMRS) and Minimally Invasive Gynecologic Surgery (MIGS). Obstetrics and gynecology residents were involved in all hysterectomies. FPMRS fellows were involved in hysterectomies starting July 2021 (corresponding to the start of a new fellowship program); there were no MIGS fellows. The Hysterectomy SSI Prevention Bundle was implemented on November 2, 2020. This study included all hysterectomies for benign indications prior to bundle implementation from October 1, 2018 to September 30, 2020, as well as those after bundle implementation from January 1, 2021 to September 30, 2022. The quarter during which the bundle was implemented was excluded from the analysis. As noted previously, the NHSN reports hysterectomy procedure codes that involve an incision made into the abdomen as abdominal hysterectomy, including trocar insertion or laparoscopy, and hysterectomy procedure codes that involve incisions made into natural openings as vaginal hysterectomy (National Healthcare Safety Network Patient Safety Component Manual, 2021). Therefore, the abdominal hysterectomy designation includes laparotomy and laparoscopic/robotic routes. The NHSN reports inpatient case as date of discharge different from date of surgery and outpatient case as same day discharge. The NHSN further categorizes infections: SIRs include superficial and deep and organ/space infections, while complex SIRs include only deep and organ/space infections (National Healthcare Safety Network Patient Safety Component Manual, 2021). The NHSN does not separate outpatient SIR data by superficial and complex infections but does separate inpatient SIR data by superficial and complex infections. To adequately compare data, inpatient SIR and outpatient SIR, composed of both superficial and complex infections, were evaluated pre- and post-implementation of the Hysterectomy SSI Prevention Bundle for both abdominal hysterectomies and vaginal hysterectomies. Additionally, the data for inpatient complex SIR was evaluated pre- and post-implementation of the Hysterectomy SSI Prevention Bundle for both abdominal and vaginal hysterectomies, as complex SSIs are a substantial cause of morbidity, hospital readmission, prolonged hospitalization, and mortality (Chan and Nimaroff, 2022; National Healthcare Safety Network Patient Safety Component Manual, 2021). To compare pre- and post-implementation SIRs, statistical analysis was completed utilizing the NHSN Statistics Calculator to compare two standardized ratios (“2015 SIR Report,” 2017; “Using the Statistics Calculator – Centers for Disease Control and Prevention,” no date). The SIR is risk-adjusted for facility and patient-level factors (Andiman et al., 2018; National Healthcare Safety Network Patient Safety Component Manual, 2021; “2015 SIR Report,” 2017).
Descriptive statistics were calculated to report patient demographics and clinical data. Patient demographics and surgery characteristics were compared between the pre- and post-implementation groups by using a two-sample t test for continuous variables and Pearson χ2 test for categorical variables.
Results
This study included all hysterectomies for benign indications prior to bundle implementation from October 1, 2018 to September 30, 2020 (n = 857) and all hysterectomies post-bundle implementation from January 1, 2021 to September 30, 2022 (n = 772).
Patient demographics, surgery characteristics, and SIRs pre- and post-implementation are summarized in Table 1. Most patient demographics and surgery characteristics were comparable between the two groups, without a statistically significant difference noted for body mass index, proportion of patients with a diabetes mellitus diagnosis, proportion of open abdominal hysterectomies, wound class, American Society of Anesthesiologists score, or proportion of emergent procedures. Differences between the pre- and post-implementation groups were significant for increased laparoscopic hysterectomies (p < .001), decreased vaginal hysterectomies (p < .001), increased number of same day discharges (p < .001), longer procedure duration (p < .001), and younger age (p = .039).
Outpatient abdominal hysterectomy SIR pre-implementation was 2.551 and post-implementation was 0.868 (p = .007). The outpatient vaginal hysterectomy SIR pre-implementation was 0.000 and post-implementation was 0.000 (p = .364). Inpatient abdominal hysterectomy SIR pre-implementation was 1.554 and post-implementation was 0.443 (p = .072). The inpatient vaginal hysterectomy SIR pre-implementation was 1.064 and post-implementation was 0.000 (p < .001). The inpatient complex abdominal hysterectomy SIR pre-implementation was 1.757 and post-implementation was 0.000 (p = .040). The inpatient complex vaginal hysterectomy SIR pre-implementation was 1.001 and post-implementation was 0.000 (p < .001).
While compliance with the Hysterectomy SSI Prevention Bundle was not part of the study outcome, overall compliance with the bundle has been greater than 95%.
Discussion
This study describes the positive impact of the implementation of a validated evidence-based hysterectomy-specific SSI prevention bundle which was successful in reducing hysterectomy SIRs. Overall, there was a statistically significant association between full bundle implementation and reduced SIR (Figure 2). This study adds to existing hysterectomy SSI prevention bundle data by comparing SSI through NHSN provided SIRs, as SIRs are risk-adjusted for facility and patient-level factors. Additionally, this quality improvement study consolidates existing knowledge and provides a comprehensive evidence-based bundle checklist or audit form that can be implemented at other institutions performing hysterectomies. Standardized Infection Ratios for Inpatient and Outpatient Hysterectomy Pre- and Post-Implementation of a Hysterectomy Surgical Site Infection Prevention Bundle. Abbreviations: AHYST, abdominal hysterectomy; VHYST, vaginal hysterectomy; Q, quarter.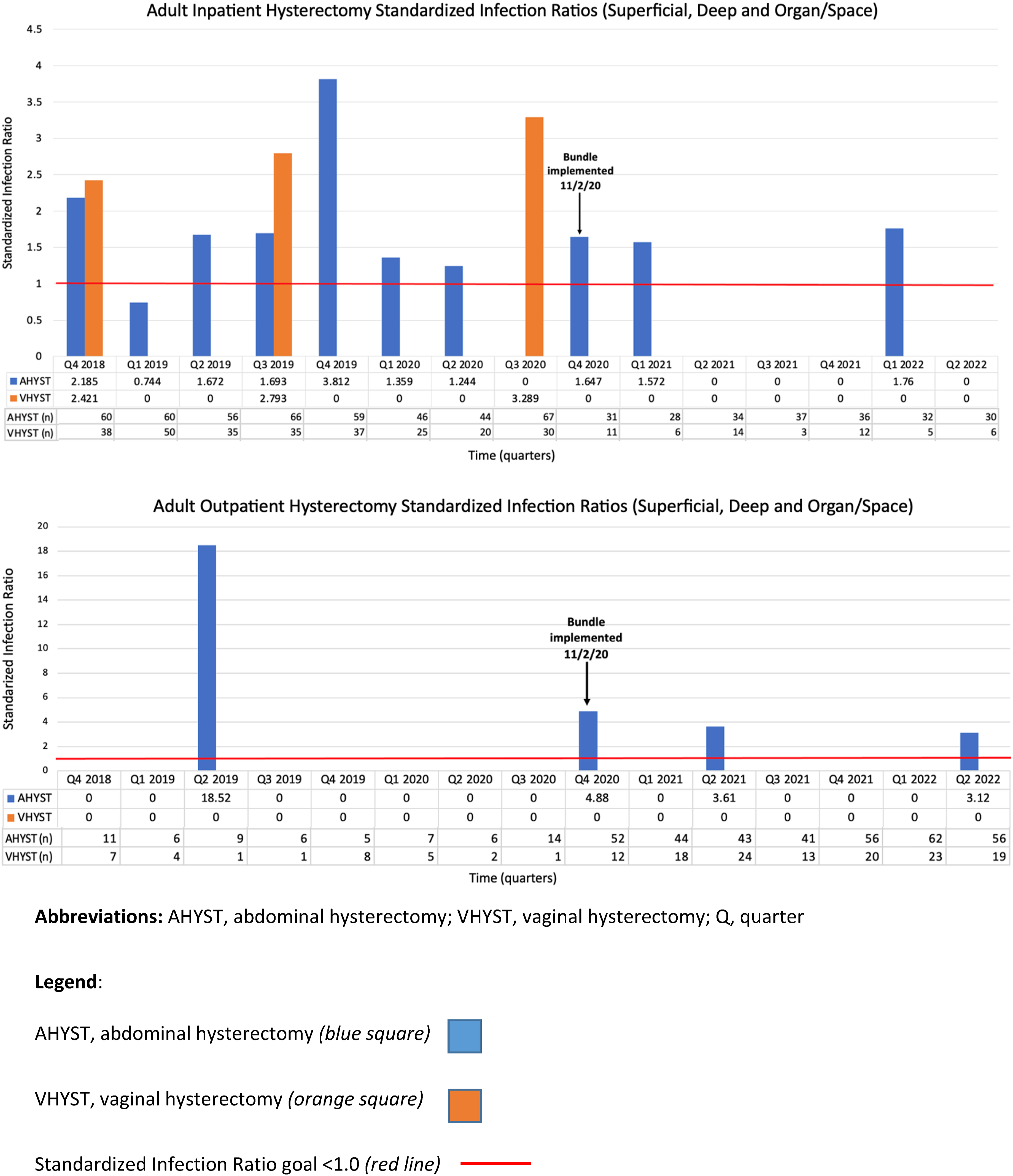
This Hysterectomy SSI Prevention Bundle was launched on November 2, 2020, during the Coronavirus (COVID-19) Pandemic. To prevent the spread of coronavirus within the hospital and preserve hospital beds, the only elective (i.e., non-emergent) surgeries that were permissible were same-day discharge or outpatient surgeries, which explains the significant increase in same-day discharges post-implementation. Considering outpatient abdominal hysterectomy SIR was 2.551 prior to implementation, and decreased significantly to 0.868 post-implementation despite the significant increase in outpatient abdominal hysterectomy cases, it is reassuring that the implementation of this bundle led to meaningful change. Similarly, while the improvement in inpatient abdominal hysterectomy SIR to 0.443 approached but was not statistically significant, it likely reflects the sizable decrease in inpatient cases. It is important to recognize, though, that all benign hysterectomy SIRs fell below 1.0, noting infection prevention following implementation of the bundle.
Differences in post-implementation increased laparoscopic hysterectomies and decreased vaginal hysterectomies are consistent with current data demonstrating an increase in minimally invasive hysterectomy procedures but a consistent decrease in the vaginal approach (“Prevention of Infection after Gynecologic Procedures,” 2018). While a post-implementation longer procedure duration of 13 minutes may not be clinically significant, it may be explained by addition of the SSI prevention bundle and increased number of laparoscopic surgeries within the post-implementation group. Finally, statistically significant differences in post-implementation patient age by 1 year younger are likely due to large sample sizes in both groups and unlikely clinically significant.
Evidence-based prevention of SSI via surgery-specific SSI prevention bundles is becoming a routine component of gynecologic surgery. Future studies may evaluate adoption of the hysterectomy SSI prevention bundle within other healthcare systems and the impact on SIRs.
Strengths of this study are the use of NHSN SIRs to compare SSI pre- and post-bundle implementation data, as SIR is risk-adjusted for facility and patient-level factors. Another strength of this study is full bundle implementation at one time period, during which no other known perioperative changes were occurring. Due to full bundle implementation at one time period, pre-implementation and post-implementation groups could authentically be compared. Existing data suggests that the use of bundles and compliance with increasing bundle elements leads to improved infection rates; identifying specific elements of a bundle for impact is not typical (Anderson et al., 2014; Waits et al., 2015; Guo et al., 2020; Harris et al., 2017; Tanner et al., 2015). Although compliance with the Hysterectomy SSI Prevention Bundle was not part of the study outcome, overall compliance with all bundle components since implementation has been greater than 95%.
There are a few limitations of this study. As all bundle components were implemented at one time, the impact of each metric in the bundle is unknown. Additionally, as this was a quality improvement project focused on implementation of an SSI prevention bundle, not all factors contributing to SSI could be controlled for, such as surgeon biases like knowledge of being observed and altering behaviors or metrics not assessed in this study. Due to the quality improvement nature of the study, we did not perform a power analysis. This study utilized SSI and SIR from multivariate logistic regression models constructed from NHSN data, so there may be potentially important variables for SSI risk which may not have been included in the analysis. Using NHSN data obligated grouping open abdominal hysterectomies and laparoscopic/robotic hysterectomies, which likely diminished the impact of reduced SIRs reported. Lastly, it is imperative that new SSI prevention data are regularly reviewed and incorporated into the bundle to allow evidence-based practice and compliance auditing to occur.
Conclusion
Implementation of an evidence-based SSI prevention bundle at a large community hospital has reduced and sustained all hysterectomy SIRs to below the expected level of 1.0. The impact of reducing postsurgical infections includes lower morbidity and mortality, shorter length of stay, avoidance of hospital readmission, reduced healthcare costs, and improved patient experience. Evidence-based prevention of SSI through SSI prevention bundles is a clinical imperative.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.