
Abstract
Introduction
The World Health Organization (WHO) defines mental health as ‘a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community.’ 1 It encompasses a sense of well-being, a satisfactory achievement of potential and a successful coping mechanism for stress and adversity. However, the prevalence of mental illness is escalating worldwide and affects 16% of the UK population. 2 Mental illness is known to be carried from childhood to adulthood 2 and stress, poverty and low socioeconomic status (SES) are all negative influences on mental health. 3
Depression and anxiety are two of the most common forms of mental illness. 4 Depression is characterized by low mood, related emotional, cognitive, physical and behavioural symptoms, and a lack of positive affect. 5 WHO predicts that depression will become the second greatest contributor to global illness by 2020 6 and is a significant cause of morbidity and mortality.4,7–8 Another major cause of morbidity and mortality is sedentary behaviour 9 and individuals experiencing mental illness are significantly less active than their counterparts.10–11 However, a positive relationship between exercise and mental health is widely evidenced.12–14 Exercise enhances quality of life,15–16 alleviates psychiatric and social disability 17 and reduces depressive symptoms. 18 It is also important for maintaining physical fitness, strengthening the immune system, increasing stress tolerance and preventing some of the diseases of affluence, such as cancer, heart disease, cardiovascular disease, type II diabetes, obesity and back pain.19–20 The rates of these co-morbidities are as high as 60% among individuals with mental illness.21–22
The relationship between exercise and improved mood identifies a link but not causality. 14 Probable reasons underpinning this mechanism include the distracting nature of exercise which confines negative thoughts, the opportunity for social interaction and to master new skills 23 and physiological adjustments in endorphin and cortisol levels, 24 which all improve mood. Although cause and effect are difficult to decipher, the evidence base reviewing the effectiveness of exercise as a treatment option for depression is continually growing.14,25–26 Meta-analytic effect sizes for exercise as a treatment option for depression compared to no treatment report reasonably large effects.14,27–29 There are many methodological issues that might bias the findings in favour of exercise, but the consistently large effect sizes justify further research. Exercise has also been compared to other established treatment options, such as antidepressants and cognitive behavioural therapy (CBT) programmes. Initial findings imply that exercise is equally as effective as both antidepressants and CBT, as no significant differences were reported between the interventions.14,30 Studies have also investigated the health benefits of introducing an exercise programme for outpatients with schizophrenia31–32 and individuals with alcohol misuse problems 33 with positive outcomes.
An optimal dosage for beneficial exercise prescription is still unclear. The most effective type, intensity, frequency, duration and conditions (supervised or unsupervised, indoors or outdoors, group or individual) of the activity remains ambiguous.14,25 Dunn et al. 16 proposed a dose–response relationship for the treatment of major depression, with the most effective treatment being 30 minutes per day on three or five days of the week (17.5 kcal/kg/week). The National Institute of Clinical Excellence (NICE) recommends participating in three structured, supervised exercise sessions (45 minutes to 1 hour) per week for 10 to 12 weeks to treat mild depression. 5 The prescriptive nature of exercise guidelines for this population is fraught with challenges and a recommended physical activity session that focuses on overall movement rather than structured exercise might be more achievable. However, the evidence implies that maintaining a positive mood almost certainly requires adherence to a longer-term exercise or activity programme. 14
The type of environment can also play a key role in the success of an exercise-based therapeutic intervention. Studies comparing indoor and outdoor exercise settings34–36 showed that outdoor experiences were rated as more restorative. 34 Moods were affected by the type of environment, with indoor walking associated with increased frustration, anxiety, anger and sadness. 36 Walking outdoors was associated with positive moods, such as feeling happy, delighted, joyful and pleased, and a decrease in negative moods. Walking outdoors increased vitality, however, no change in this measure was experienced during indoor walks. 35 The presence of nature was an influential factor in improving vitality outdoors. 35
Nature is defined as ‘the environment in which organisms or their biotopes expressly manifest themselves. In addition to nature reserves, this will also include farmland, production forest, urban green spaces and back gardens.’ 37 It is well established that exposure to nature leads to positive mental health outcomes and cognitive, affective and behavioural changes. 38 The link between contact with nature and improved mental health is understood by those who regularly seek out green spaces and choose to participate in green exercise activities (any activity in a green space in the presence of nature).39–42 Access to green space is important for mental health and is associated with longevity and decreased risk of mental illness in Japan, 43 Scandinavia 44 and the Netherlands, 45 improved perception of general health46–49 and improved quality of life in ageing populations. 49 Thus, nature can provide a resource for tackling illness and act as an effective upstream health promotion intervention for clinical populations.3,50–51
A number of initiatives combine nature and exercise to promote health (e.g. social and therapeutic horticulture, wilderness therapy, adventure therapy, green gyms). The therapeutic application of these nature-based approaches offers treatment options for individuals experiencing mental or physical illness that do not rely solely on drug therapies. Green gyms promote physical and mental health through active, supervised participation in environmental conservation work within the local environment. 52 Significant improvements in Health-Related Quality of Life (HRQOL) scores and cardiovascular fitness were reported, along with increased muscular strength, coping ability and reduced risk of functional limitations in later life. 52 Adherence rates were also favourable when compared to those recorded in traditional gym-based schemes. In the national evaluation those with the lowest initial physical health scores were nine times more likely to see the biggest improvements in their scores compared to members with higher scores. 53 Similarly, members with the lowest mental health scores at the outset were three times more likely to see the biggest improvements. The least active participants were three times more likely to increase their physical activity levels, so these nature-based exercise interventions are effective in increasing activity time for those who need it most. 54
However, the evidence concerning the application of green exercise in the mentally ill population is limited. Research has demonstrated that short singular exposures to nature and physical activity are potentially beneficial in improving mental health in the general population,39–40,55 but little research has focused on clinical populations. Positive changes in mood and self-esteem (SE) have been seen after as little as 20 minutes when comparing pre and post measures.39–42 However, studies analysing the benefits of repetitive exposure over a period of weeks are limited. Initial findings also imply that green exercise activities are more effective in improving self-esteem and mood for people experiencing mental illness, but further research is required. 42
Engaging in physical activities in green spaces also plays a role in reducing social isolation. 17 A driver in promoting mental health is the ability to establish close relationships based on reciprocal trust and affection. 56 It is well known that trusting relationships help to change attitudes and behaviour as well as have a positive effect on health.57–58 Conversely, isolation and negative feelings make change more difficult and also negatively affect health. 59 Connectedness to social communities via contact with other social institutions and cultural mechanisms helps to establish these relationships. The value attached to them constitutes a form of capital, often referred to as ‘social capital’, representing a resource of trust, reciprocity and obligations that can be drawn upon to provide health benefits.60–61 The impacts of group therapy have long been recognized as a constructive approach to managing mental illness and the growing number of CBT courses available highlights the importance of social contact in recovery. Thus, introducing a structured therapeutic intervention involving exercise in a green space, which provides a safe opportunity for social interaction, could prove effective. These interventions may complement existing drug and/or CBT programmes and would be a positive step forwards in tackling health inequalities. The aim of this study was to evaluate two existing group-based health promotion initiatives targeting clinical populations and compare these to a new green exercise programme introduced at a third site involving a similar clinical population. The two existing initiatives were both social intervention programmes: a social club (met indoors, but did not participate in any form of exercise, so analysed social component only) and a swimming group (indoor exercise, so comprising social and exercise components). A green exercise programme, consisting of short countryside and urban park walks, was introduced as the third intervention (comprising nature, exercise and social components).
Method
Participants
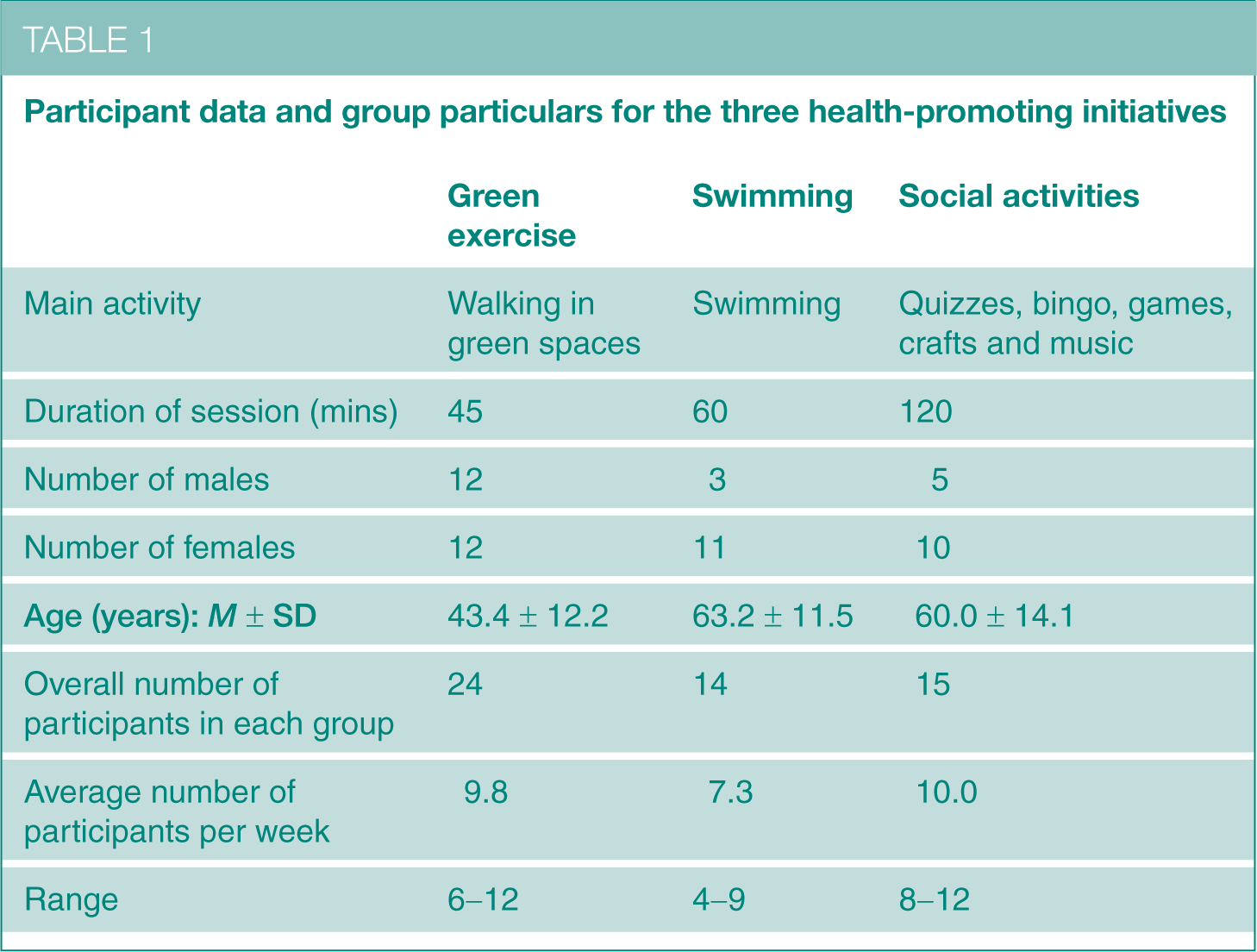
All participants were Mind group members (N = 53) experiencing a range of mental health problems. Of these, 38% were male (21–82 years) and 62% female (27–83 years), with a mean age of 53.0 years (SD = 15.4) (Table 1). Mind is a mental health charity in England and Wales which aims to promote and protect good mental health for everyone. 62 Mind’s ethos is not to label members with health conditions or request self-disclosure, so based on the authors’ experience the patients were classified as axis I patients predominantly experiencing substance-related disorders, schizophrenia and other psychotic disorders, mood disorders or anxiety disorders, using DSM-IV-TR criteria. 63 Participants took part in only one of the three health-promoting initiatives: swimming (S), social activities (SA) or green exercise (GE).
Participant data and group particulars for the three health-promoting initiatives
Health-promotion initiatives
Swimming
This group met every Tuesday morning at a local leisure centre for an hour. The group had shifted from being worker led to service user driven as members had become more independent, although transportation to the centre was still provided for many members. There were 12 members who participated on a regular basis and the maximum attendance was 18. 64 Participants were surveyed between May and July 2008.
Social activities
The club met for two hours at a local meeting house on a Tuesday afternoon. It serviced a large number of elderly, semi-acutely ill local residents and provided an opportunity for ongoing social interaction via its many activities, such as quizzes, bingo, games, crafts and music, as well as regular outings to local attractions. Vehicles were provided by volunteers to transport members to the venue. There were 10 regular service users, with a maximum attendance of 14. 64 Participants were surveyed between May and July 2008.
Green exercise
A local drop-in centre was selected as the study site to participate in the green exercise walks. The centre operated on an open-door basis and community members could attend without the need for a referral or appointment. Therefore, members already knew one another but agreed to participate in a new health-promoting intervention. The GE programme consisted of six walks which took place every Tuesday at 2.00pm. Each walk was 45 minutes in duration and was of a moderate intensity (a brisk walk that noticeably accelerates heart rate). 65 The walk leader set the pace and wore a pedometer to measure the number of steps completed. All walks took place within easily accessible local public green spaces, such as country parks, local countryside areas and nature reserves. All walks were led by the same researcher to ensure consistency of personal interactions. Mind coordinators who knew the members attended all walks to offer support and assistance. Minibuses were used to transport participants to the locations. A greater number of participants expressed an interest in taking part in the research than the programme could accommodate, so names were randomly selected each week to make it as inclusive as possible. All participants were surveyed between June and July 2007.
Attendance
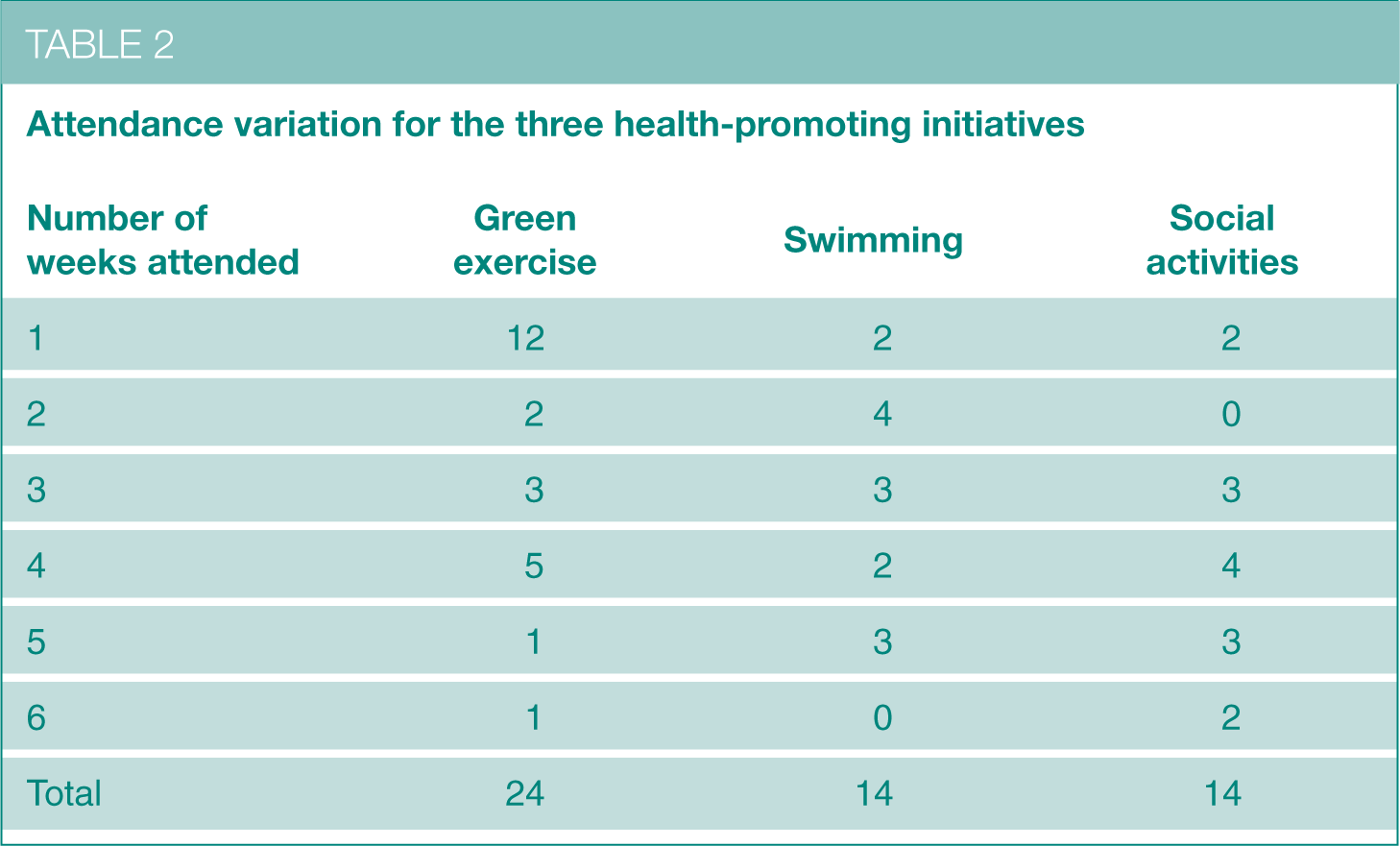
Not all participants attended every session. Variation in attendance is expected with this population as they intermittently face exacerbations in their illness which may prevent attendance. Table 2 describes the variation in attendance for the three separate groups. The majority of GE participants attended one session only due to the enforced random selection of interested individuals. Attendance rates at the S and SA clubs were more comparable and a higher proportion of participants attended five or six sessions due to the established existence of the groups.
Attendance variation for the three health-promoting initiatives
Procedure
Ethical approval to conduct the research was initially acquired from the University of Essex ethics committee. The groups were then contacted and participants were recruited after a presentation from the researcher, who provided a brief generalized overview of the aims of the research, using non-suggestive terms. All participants were provided with participant information sheets to make an informed decision and participation in the research was entirely voluntary. Informed written consent was obtained from all participants for both completion of the questionnaires and participation in the GE programme (where applicable). Participants were advised that all information would be treated as confidential.
Empirical data was collected using pre-printed standardized questionnaires. The researcher visited the initiatives on the day that the group regularly met each week for six weeks. Questionnaires were administered to every member of the group to eliminate any selection bias, although participation was not compulsory. Completion rates were calculated as 97%, 95% and 98% for the S, SA and GE groups, respectively. Although the questionnaires were designed for self-completion, assistance was provided where necessary. Participants completed the questionnaires immediately pre and post activity, for every session they attended during the six-week period.
The questionnaires incorporated two standardized measures to analyse changes in self-esteem and mood. The Rosenberg Self-Esteem Scale (RSE) 66 includes 10 statements and each item has four response choices ranging from strongly agree (1) to strongly disagree (4), therefore a low score represents high self-esteem. Test-retest correlations typically range from 0.82 to 0.88 and reported Cronbach’s α coefficients range from 0.77 to 0.88.67–68 The 30-item short-form version of the Profile of Mood States (POMS) questionnaire 69 has 30 adjectives which collectively measure six mood factors: anger-hostility, confusion-bewilderment, depression-dejection, fatigue-inertia, tension-anxiety and vigour-activity. A global estimate of affective state referred to as the Total Mood Disturbance (TMD) score was calculated by summing the five negative subscales (anger, confusion, depression, fatigue and tension) and subtracting the only positive subscale (vigour). 70 Internal consistency of the POMS inventory ranges from 0.84 to 0.95 and test-retest reliability coefficients range from 0.65 to 0.74. 71
Data analysis
All data measures were tested for normality (Kolmogorov-Smirnov test) and variance. The α level of 0.05 was used for all statistical analysis and all significant test results were reported using two-tailed probabilities. Two-way mixed ANOVAs were used to calculate any significant differences in pre and post SE and TMD scores between the groups after participation in one session. A similar set of statistical tests analysed the change in those indicators over the six-week programme according to attendance. Any statistically significant findings were explored further using Tukey post hoc tests and t-tests with Bonferroni corrections.
Results
The effect of a session on SE and TMD
The impact on SE and TMD after participating in a single session was analysed for all three intervention groups (Table 3). SE and TMD improved in all three groups but the magnitude of change differed between them. Two-way mixed ANOVAs revealed significant main effects for SE and TMD pre and post activity (F(1,147) = 38.2, p < 0.001 and F(1, 142) = 65.8, p < 0.001, respectively). Post hoc t-tests revealed significant improvements in SE and TMD for all groups except SA (SE, p > 0.05, Table 3). Main effects for SE and TMD were also found for type of intervention (F(2,147) = 3.3, p < 0.05 and F(2,142) = 3.8, p < 0.05, respectively). Post hoc comparisons using the Tukey HSD test indicated that the difference in SE was between the SA and S groups and TMD differences were between the SA and GE groups. Thus, the SA participants reported better self-esteem than the S group and better mood than the GE group. There was a significant interaction between the intervention type and pre and post scores for SE only (F(2,147) = 8.7, p < 0.001). A one-way between-subjects ANOVA compared the change in self-esteem (i.e. Δ pre-post scores) between the three groups and revealed that SE scores improved more in the GE group compared to the SA group.
Mean (M) scores for self-esteem and overall mood pre and post one session
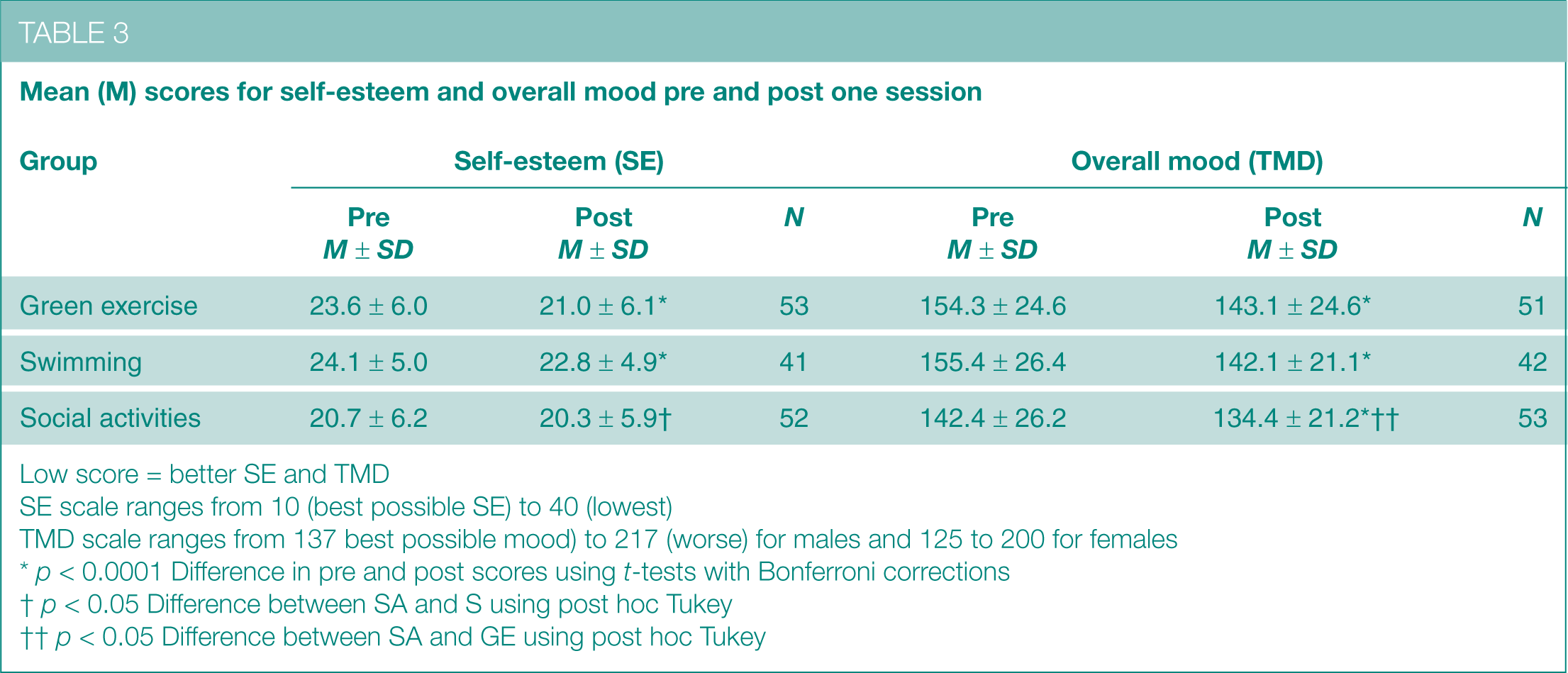
Low score = better SE and TMD
SE scale ranges from 10 (best possible SE) to 40 (lowest)
TMD scale ranges from 137 best possible mood) to 217 (worse) for males and 125 to 200 for females
p < 0.0001 Difference in pre and post scores using t-tests with Bonferroni corrections
p < 0.05 Difference between SA and S using post hoc Tukey
p < 0.05 Difference between SA and GE using post hoc Tukey
Longitudinal changes in SE and TMD according to attendance
This process generated dose–responses that were dependent on attendance. Participants were categorized according to how many sessions they had attended within the six-week period (Table 4).
Number of sessions attended during the six weeks of data collection
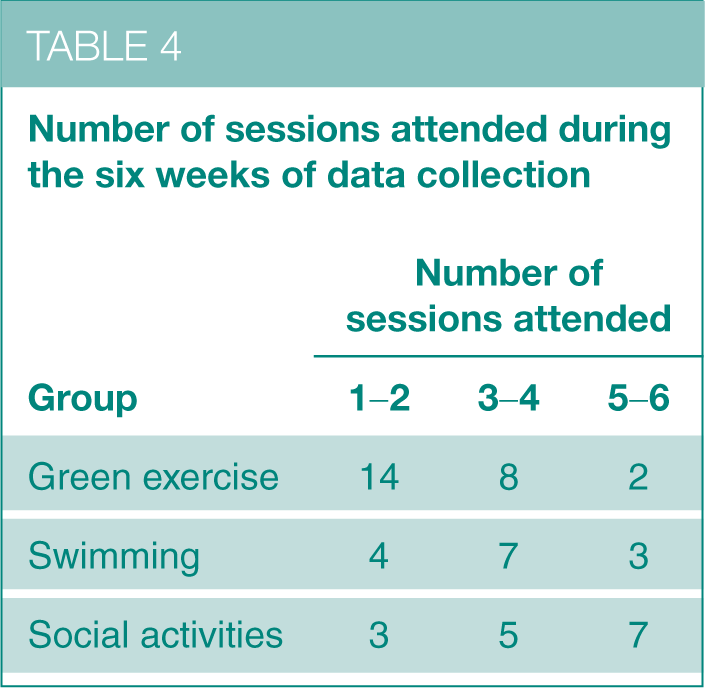
Three-way mixed ANOVAs using one within variable (pre first session and post final session scores) and two between variables (group and attendance) were performed on both SE and TMD. There was a significant main effect for pre and post SE and TMD scores (F(1, 40) = 9.4, p < 0.005 and F(1, 39) = 14.3 p < 0.001, respectively). Thus, participants’ SE and TMD significantly improved over the six-week period. However, there were no significant main effects for group or attendance or any significant interaction effects (condition*time, attendance*time, condition*attendance*time).
Discussion
This study evaluated the health benefits of participating in a swimming group, a social activity club and a green exercise programme. Changes in SE and TMD were assessed pre and post single sessions for a period of six weeks. Key findings reported that all groups combined experienced significant improvements in SE and TMD after participating in a single session. A significant interaction effect reported that the change in SE was significantly greater in the GE group compared with the SA club. There was no significant interaction effect for TMD but the change in TMD was greatest in the swimming group, with the SA club reporting the smallest change. These findings suggest that participating in exercise is the primary driver in positively enhancing self-esteem, although engaging in sedentary social activities can also contribute to an improvement in this marker, highlighting the importance of social contact.
Post hoc analyses identified differences in starting SE and TMD scores, with participants of the GE group reporting poorer SE and mood than the SA club. Possible reasons for these underlying differences may relate to group dynamics, demographics and length of programme. The SA club has been in existence for over 20 years and many members have been regularly attending for up to 12 years. In comparison, members of the GE group did not necessarily socialize together at the drop-in centre but came together to participate in the walks (which did not always involve the same individuals). The differences in these parameters imply that members of the established social group are already experiencing health benefits from participating in regular social activities.
The dose–response data showed that both SE and TMD levels improved over the six-week period for all groups combined, although no interaction effects were reported. The lack of differentiation between the programmes implies that introducing GE as a health-promotion initiative for people experiencing mental ill health is equally as effective as the existing options.
Limitations
There are methodological limitations with this type of fieldwork which are unavoidable. Variation in attendance and non-equivalent, self-selecting groups with no consistent membership restricts longitudinal and between-group analyses and limits interpretation of the findings. Attendance rates for both the S and SA groups were relatively consistent and represented typical behaviour. In contrast, a random selection process of participants was enforced in the GE group to avoid exclusion issues. This limits the comparability of the groups as 50% of the GE participants only attended one session compared to 14% in the other two programmes. Only 8% of the GE participants attended five or six sessions compared to 21% and 47% in the S and SA groups, respectively. This affects the reliability of the longitudinal analysis of SE and TMD as many GE members only had the opportunity to participate in a single session.
The demographics of each group also differed, which might have influenced the findings. The two existing initiatives attracted mainly female participants, whereas the GE programme recruited an equal number of males and females. The GE participants also represented a slightly younger generation, which makes generalization more difficult. It was not possible to collect all data simultaneously, however data was collected at similar times of the year to account for any seasonal affects. The health-promoting initiatives were of different durations, which might have had an impact on acute effects. However, weekly sessions were always of the same duration for each group respectively.
The sample size limits substantiated conclusions but it does inform the effect size upon which to calculate a future larger study. Self-esteem and mood are very labile, especially for those experiencing mental health problems when it can be even more accentuated. Therefore, a one-off measure once a week does not account for events occurring throughout the week or prior to the activity. In addition, a common side effect of psycho-active drugs is flattening of affect and if participants were receiving drugs to control their mood, this would have had an impact on the findings. However, irrespective of starting levels, participation in the health-promoting initiatives generally improved both SE and TMD after a single session. Therefore, they had positive acute effects which could lead to longer-term chronic improvements.
Conclusion
This study highlights the methodological challenges involved with this type of research and the limitations identified suggest a need for further research. Future research studies could include randomized controlled trials or waiting list control groups, although attrition rates may still be varied. GE could be compared to other types of exercise and the findings suggest a need to independently analyse the social component. The social interaction was a consistent element in all initiatives, so future studies could attempt to disaggregate this to assess its contribution. The findings also generate further questions regarding the underlying mechanisms of differences in environmental exposure. This study did not attempt to record environmental characteristics such as temperature, humidity, light and vitamin D exposure, but these factors could contribute to changes in mood. Thus, outdoor weather conditions for the GE group may have influenced the findings. Similarly, nature’s components (i.e. sound, smell, visual, etc.) have not been assessed independently to recognize the contribution of each to the overall experience and restorative properties of nature exposure.
The effectiveness of exercise as a treatment option for depression has already been compared to antidepressants and CBT programmes.14,30,72 Antidepressants often have many adverse side effects and there is often a time lag between prescription and elevations in mood. 14 Therefore, GE could potentially be advocated as a parallel intervention to traditional drug therapy in the treatment of mental illness to enhance both acute and chronic improvements in mood. Research suggests that people experiencing serious mental illness often accept exercise as a potential treatment option and frequently identify it as one of the most valued components of treatment. 17
GE programmes also promote reconnection with nature and an opportunity to experience the additional positive health benefits that are associated with this.39–42 Contact with nature and green space is often uplifting and restorative, and helps to reduce stress and improve mood.39–42 Combining this with physical activity may offer a very efficacious treatment option. GE also promotes social inclusion and creates the circumstances and associated social networks within which healthier lifestyle choices are more likely. It is clear that social connections, exercise and nature all have a key role to play in addressing mental ill health. Combining these elements may also play a role in managing and supporting recovery from a range of mental health problems, suggesting a potential green approach to mental healthcare and promotion.
GE has implications for many sectors, suggesting the need for cross-disciplinary and cross-sectoral strategies and action. Increasing support for and access to a wide range of GE activities for all sectors of society could produce substantial economic and health benefits, both at the individual micro level and public and environmental macro level. Such support could include the provision and promotion of healthy walks projects, green exercise on prescription, healthy school environments, green views in hospitals, care farms, city farms and community gardens, urban green space, and outdoor leisure activities in the countryside. In the current context of increasing incidence of mental ill health, the importance of a new green agenda for mental health that improves access to nature and green spaces is needed.
Footnotes
Acknowledgements
The authors would like to thank all participants for consenting to take part in this research project. Appreciation is shown to both Maldon and Colchester Mind groups, volunteer support workers and staff for their assistance with the evaluation process. The Colchester Mind group was instrumental in facilitating the green exercise programme and the Maldon Mind group kindly permitted the authors access to their ongoing social intervention programmes.