
Abstract
Keywords
Introduction
This article analyses the shaping of a worksite health promotion initiative, a so-called canteen takeaway (CTA) scheme, at two Danish hospitals in order to contribute to the development of theoretical frameworks for the planning and analysis of food and health interventions at worksites. The article also contributes to the development of a foodscape approach to food and health interventions at worksites by integrating a food production and a food consumption perspective and by including the organizational processes, which shape the intervention. The analytical focus is on the local processes that influence health promotion interventions at worksites based on their previously developed norms and values. This implies that the same type of initiative might end up being shaped rather differently, even at two worksites within the same sector.
This article is based on theories concerning political processes at worksites and theories concerning the co-evolution of problem–solution complexes during the design of socio-technical systems. Empirically, the article is based on a qualitative case study organized by Poulsen about the shaping of CTA projects at two Danish hospitals where employees were offered the opportunity to buy meals to eat during evening shifts or to take home in order to reduce their workload outside the worksite, in terms of planning, shopping for and cooking meals at home. This case study was carried out as part of a research and innovation project about the shaping and impact of canteen takeaway systems at different types of worksites.
In 2008 the first hospitals in Denmark began offering their employees the opportunity to buy meals to take home for dinner, so-called CTA schemes. At the time, this was a very new idea, not only for public worksites but for worksites in general in Denmark. The first hospitals to offer this project wanted to be recognized by potential staff as attractive worksites; they wanted to attract new staff and to retain their existing staff.
Through the case study, the two hospitals were followed during the planning and implementation of a CTA scheme. Hospital A is located in the Copenhagen area and employs about 4,500 staff, which makes it one of the biggest hospitals in Denmark. The other, Hospital B, is located in the eastern part of Jutland and has about 1,600 employees. The two hospitals began their considerations about CTA in the spring of 2008, inspired by a Danish research and development project on CTA schemes, coordinated by the Danish Cancer Society (www.kantinetakeaway.dk). In November 2008, Hospital A sold their first meal, while Hospital B was ready with their system in the spring of 2009.
The worksite as a setting for food and health interventions
The importance of the worksite as a setting for health promotion is supported by the World Health Organization (WHO), 1 the European Commission 2 and The Nordic Council of Ministers. 3 Several studies on the effects of food and health interventions at worksites 4 have been published. The majority of these studies discuss whether a specific intervention had an effect on previously determined parameters. Review articles show several positive effects of interventions at worksites.5,6 Besides investigating effects of interventions, the reviews also focus on aspects that seem to influence their success. Employee participation in the process can be beneficial because it can increase employee awareness of the intervention.5,7,8 Another aspect is organizational support, which is stated to be important for the success of particularly comprehensive interventions. 5 Also the organizational structure may influence workplace health promotion. 9 These aspects are all seen as internal aspects at the worksite, but the social context, which can be both internal (i.e. the cultural norms at the worksite) and external (i.e. influence from family conditions), is found also to affect the staff and thereby the intervention. 5
Despite the importance of these aspects, a deeper theoretical understanding of the processes at worksites that influence the design and impacts of such initiatives seems to be missing. 9 Several models have been developed with the purpose of planning and/or evaluating; for example the social contextual model. 10 This model focuses on how different parameters influence people’s health. However, despite its complex understanding of the shaping of people’s health, the model blackboxes the shaping or the design of the intervention itself, since the model does not focus on how the intervention can be an object of negotiation during the process of planning and implementation.
Based on organizational theory, Dooris has suggested that settings can be viewed as complex, dynamic systems. 11 Within this approach, a worksite setting is seen as a system with inputs, throughputs and outputs. However, the work of Dooris is also lacking a theoretical base for the analysis of how the complex social system of a worksite shapes changes. The present study investigates the shaping of CTA schemes at two hospitals based on a theoretical approach to the worksite as a political system where interventions are negotiated based on previous conflict and consensus processes among the different stakeholder groups at the worksite. This is explained in the next section.
Theoretical approach
The analyses were inspired by the approach of the worksite’s social constitution and by a co-evolution approach to problem–solution complexes in design processes, including organizational design.
The concept of social constitution is based on a dialectical relationship between local worksite policy and structural power and was developed by Hildebrandt and Seltz.12,13 The basis is an understanding of a worksite as subject to the capitalistic mechanisms and thereby an asymmetrical balance of power between the different stakeholder groups at the worksite. Stakeholders are structured in social groups through their position at the worksite (e.g. top management, project management, supervisor groups, support staff, employees, etc.) and are thereby also linked in a macro-power structure. The social constitution is shaped by the conflict and consensus history of the worksite. The concept links structure and stakeholder because the worksite stakeholders’ interpretation of external and internal conditions is shaped by the social constitution, which acts as a joint framework or filter through which the worksite stakeholders understand and shape changes. Several social constitutions may exist at a worksite, for example within different departments.
Another analytical inspiration in the article is an understanding of change processes as the co-evolution of problem–solution complexes.14,15 This perspective draws on knowledge from creative design and the focus on two design spaces: problem space and design space. The approach highlights the importance of focusing on the social consequences of a problem–solution complex since new problems may be created because of the way in which the solution has been shaped. Applying this approach together with the social constitution approach implies that both the proposed solutions and the underlying understanding of the problem are seen as shaped by the social constitution. The focus on the details of the shaping of problem–solution complexes helps the researcher understand aspects of the social constitution of the worksite.
Methods
Qualitative methods were used to retrieve data in the case studies. At Hospital A, semi-structured interviews were conducted with relevant informants, based on a snowball sampling. Also, observations were made at meetings where the canteen manager presented results from the CTA process. At Hospital B, semi-structured interviews with key informants were also conducted and focus group interviews were made with users and non-users of the scheme. The participants of the focus group interviews were found with help from the manager of the kitchen and a human resource professional from the hospital, the aim was to get opinions from different divisions and from different types of jobs at the hospital.
A guide was developed for the focus group interviews. Based on recommendations from Halkier, 16 the interviews began with a general question and then the questions became more specific. The focus group interviews were recorded using video and a voice recorder. A resumé was made and transcribed verbatim. For the face-to-face interviews, semi-structured interview guides were developed 17 and shaped in accordance with the interviewee’s role in the change process. The interviews were all recorded and transcribed. Observations made were written down during or after the interview.
Results
The main events in the shaping of the two CTA schemes are presented in Tables 1 and 2.
Main events at Hospital A

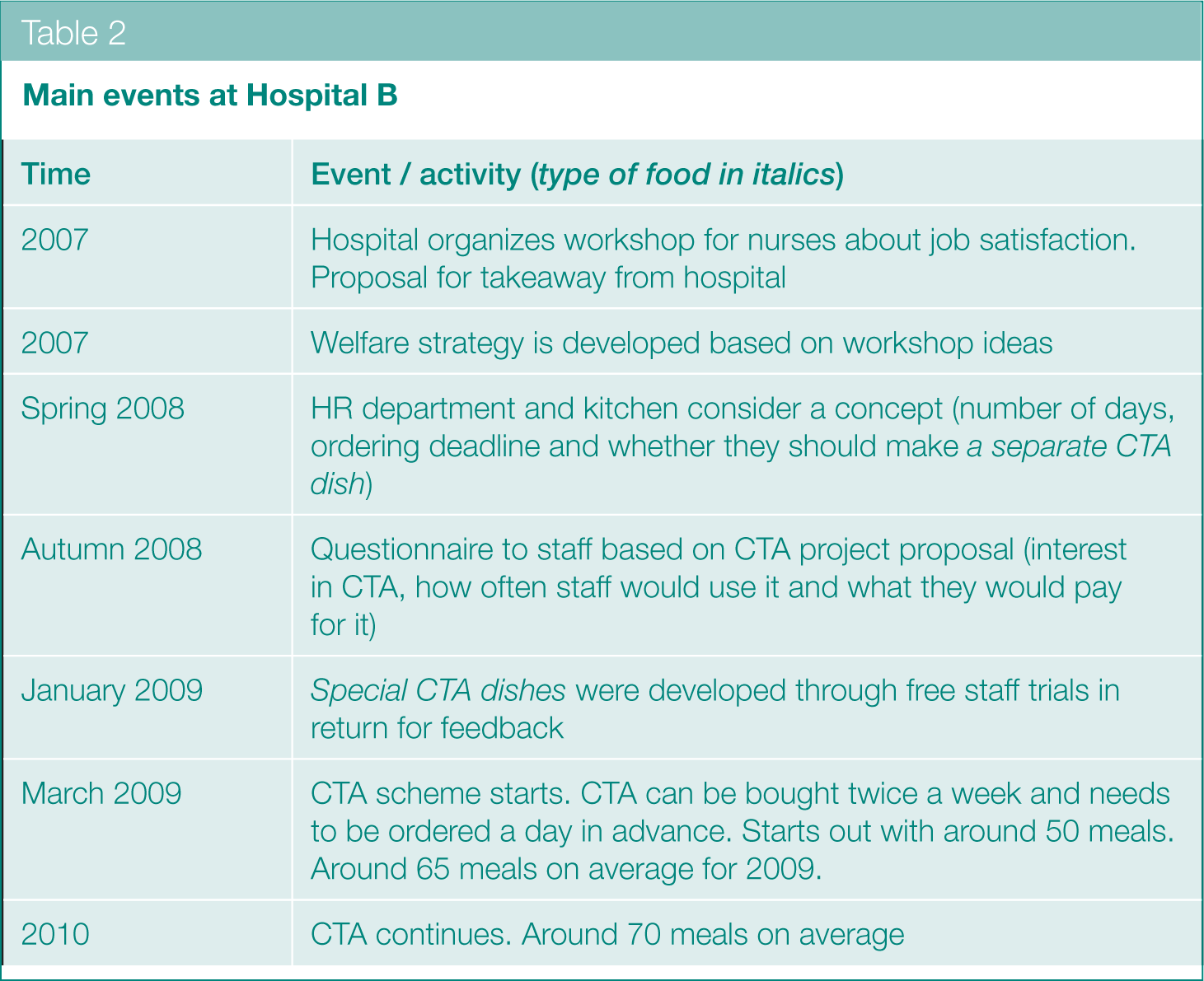
Main events at Hospital B
Hospital A
Since the staff canteen manager started working at Hospital A he had always wanted to do something to improve the food supply for staff working irregular hours (e.g. the shift from late afternoon to late evening), because the staff canteen closed at 13:30, leaving them with few options to buy food during working hours. In the beginning of 2008, he opened the staff canteen in the evening for a two-month period. The canteen offered the same dishes that were served for lunch which could be re-heated in accordance with the evening shift’s working schedule. The canteen manager handled this extra task himself because the canteen staff did not want to work in the evening. Due to this reluctance to work irregular hours, the canteen committee, with representatives of management and employees at the hospital, discussed if they could find another solution for the evening shift. They came up with the idea of CTA, and through the CTA project they found an external supplier of ready-to-eat meals. The canteen manager was keen on this external supplier because he found the quality of the meals very high and it would barely require resources from the canteen. The management of the hospital was presented with this idea, but decided that they wanted a proposal from the manager of the patients’ kitchen. The manager of the patients’ kitchen developed a proposal where the meals would be low-fat versions of those made for the patients and would be offered every day from Monday to Friday. This proposal kept the production expenses low. In August 2008, the management approved the proposal from the patients’ kitchen because it would ‘keep the money in house’. The canteen manager, however, found the food from the patients’ kitchen tasteless and boring. Despite this, he continued to develop the scheme. Together with the patients’ kitchen, he found out that the food would be ready for pick up between 14:00 and 16:00, but this meant that the evening shift staff could not use CTA as their shift started at 16:00. The chairman of the canteen board offered to develop a web shop where the staff could look at the menu and order meals. The staff needed to order before 9 a.m. on the days that they wanted CTA. As a way of making CTA an option for the staff working irregular hours, the canteen manager rented a vending machine. However, the trays got stuck in the machine and it was returned to the supplier after a few days. In the beginning there was great interest in the takeaway service with 100 meals sold each day, but after a while interest dwindled and after some months only 10 meals were sold each day. The canteen manager believed the staff found the meals boring. A user survey taken after one month did not confirm this assumption, but the reduction in the demand soon after could indicate that the users became tired of the adjusted patient food.
In the beginning of 2009, as part of a restructuring process, a new food service organization was formed. The new service covered food for the patients, the staff and the visitors, with the patients’ kitchen manager as its manager. After one year, the takeaway scheme was extended with an ‘offer of the week’ which offered certain meals at a lower price. However, this did not increase interest among the staff. In October 2010, a newly appointed customer and quality manager proposed that the visitors’ cafeteria should sell their ‘dish of the day’, prepared by trained chefs, as the staff CTA menu. The customer and quality manager believed that the poor culinary quality of the CTA meals had caused the lack of interest among the staff. The cafeteria chefs decided to develop the scheme so that it was no longer required, nor possible, to order in advance. With these changes, the web shop was no longer seen by the canteen committee to be of any use to the scheme and so was given up. However, this could mean that staff cannot be sure of obtaining a takeaway meal from the visitors’ cafeteria to either take home or to eat during an evening shift. This new scheme did not offer the night shift new possibilities for buying food during working hours.
Hospital B
In 2007, the human resource (HR) department at Hospital B organized a workshop for nurses about job satisfaction because the hospital manager wanted to find out how to retain staff. At the workshop some nurses proposed the idea of takeaway food sold by the hospital. Several other ideas emerged at the workshop and they provided the foundation for the development of a welfare strategy for the hospital later that year. HR were given the task of investigating the proposals further and in 2008 they began looking into CTA. Together with the kitchen manager, they investigated different options, such as what type of meal to offer and when it should be ordered. Based on their initial ideas, they developed a short questionnaire for all employees asking about ordering deadlines, type of meals and price. Based on the answers, the HR department and the kitchen manager decided to change the order deadline from two days before to one day before the meal was sold, in order to make it possible for employees to use the CTA scheme with less planning.
In January 2009, the kitchen began developing CTA meals and organized a trial period where some employees could try the meals for free on the condition that they give feedback to the kitchen. The kitchen wanted to ensure that the meals tasted as intended when they were re-heated and that the size of the portions were acceptable; they had to incorporate this extra task in the kitchen workflow. Based on the feedback, the scheme began in March 2009. The HR department and the kitchen manager decided that CTA should be sold twice a week, which was the frequency that the kitchen found to be realistic. At the beginning, 50 meals were ordered every time the takeaway was offered; this later increased to 70 meals, twice a week.
Discussion
The aim of this article is to investigate the shaping of CTA schemes at two hospitals in Denmark and to show how previous and present interactions among stakeholder groups shape the schemes, the problems that are in focus and the solutions that are offered.
An integrated perspective on food supply and demand
What might look like two similar design processes, turned out to be rather different change processes due to the local organizational processes. The two cases show how the problem–solution complexes, which are part of the design of worksite food interventions, need to combine a production and a consumption perspective while considering whether proposed solutions seem to solve the original problem in focus. Some of the considered solutions at Hospital A during the shaping of the CTA scheme did not solve the original problem. The solution space seemed for a time more focused on finding out what problems a CTA scheme could solve and not whether the original problem of the food supply during the evening shift could be solved. One of the proposed designs of the CTA scheme was organized so that the staff on the evening shift could not collect meals to eat during their working hours, since the CTA was only sold between 14:00 and 16:00. This implied that this solution generated a new (derived) problem seen from a food demand perspective. The solution to this became a vending machine, but since the trays got stuck, this failed to solve the problem from a demand perspective and for a period the CTA food was not available to the original target group: the employees on evening shifts.
The importance of an integrated food production and consumption focus to worksite eating – it could also be called an integrated food supply and demand focus – is confirmed by Faugier et al.18,19 They show that the combination of the poor availability of food (as an aspect of food supply) together with poor possibilities to have regular breaks (as an aspect of the staff’s actual food demand) is found to prevent healthy eating during working hours for hospital staff.
The roles of worksite social constitution
The two cases also show the role of previous organizational processes at a worksite and their shaping of present norms and values, which act as a framework for new change processes. New political issues might be developed or existing norms and values might be challenged and put under pressure by a change process. As we will see, both types of political processes are seen in one or both cases.
The focus in both cases is problems, which through the change processes become recognized as problems of the worksite. At Hospital A, the poor availability of meal options for staff working irregular hours became the focus and was proposed by the canteen manager as a problem he wanted to address. At Hospital B, the work–life balance was recognized as a problem because the nurses requested support for everyday activities outside working hours. The CTA scheme was a way of reducing their load from shopping and cooking at the end of the working day. This request was accepted by the management to make the hospital a more attractive workplace at a time when there was a lack of available staff in the labour market.
The two change processes conflicted with existing norms and values to a different degree. While the shaping process at Hospital A challenged some existing norms and values at the worksite, the process at Hospital B was more consensus based, aimed at finding the best way of solving a problem, which was agreed upon from the beginning of the shaping process (the possibility of reducing the workload of employees outside working hours).
As stated in the theory about social constitution, conflict and consensus processes, which took place before the intervention process in focus, have developed the norms and values of the worksite. These norms and values might become part of active political processes at the worksite if an intervention changes the norms and values or challenges the balance between different norms and values. At Hospital A, food culture differences between a nutrition perspective in the patients’ kitchen and a culinary perspective in the staff canteen and visitors’ cafeteria created tensions between different parts of the food service system when the hospital management was considering outsourcing the staff canteen to an external entrepreneur, thereby effectively creating two food system organizations. This tension between the two food cultures implies that the decision to ask the hospital kitchen to produce the CTA food for staff and then adapting it for patients’ food created a political conflict, with different stakeholders defending and attacking the decision. The decision implied that an economic perspective (create as much activity internally at the hospital as possible) was given higher priority than the culinary perspective (buy culinary-interesting food from an external supplier). When the restructuring of the food service organization, (initiated without reference to the CTA scheme), merged the three parts of the food service organization into one and when one of the managers left the organization, it became possible to cooperate between the food supply units for the three different target groups (staff, patients and visitors). The visitors’ cafeteria, which was open part of the evening, was also able to sell its daily dish as CTA food for staff to take home or eat in.
The resistance at Hospital A towards opening the canteen in the evening illustrates an element of the local social constitution within the canteen kitchen at this hospital: the manager and the employees co-determine the working hours and normally the kitchen staff do not work in the evenings (while this is common practice among the health personnel (nurses, doctors, etc.)). This explains why other solutions to the improvement of the food supply to the evening shift have to be considered. The final design of the CTA scheme builds upon the existing evening opening hours in the visitors’ cafeteria, where it is an accepted element of the local social constitution.
At Hospital B, the design of the food supply did not create conflicts with existing norms and values at the hospital or within the food service organization. However, it is important to be aware that a lack of expressed conflicts does not imply that there are no conflicts with existing norms and values. Conflicts may be suppressed due to very asymmetrical relationships between management, employees and support functions at the hospital and may not even be expressed directly through interviews. The interviews did not show directly expressed conflicts, nor did they show information that could indicate suppressed conflicts.
Conclusion
This case study proposes that worksite health promotion practitioners, whether internal or external in relation to a worksite, should be aware that the intervention itself is an object of negotiation between different stakeholders at the worksite. The social contextual model 10 includes considerations about how worksite structures can influence health and inform the intervention, but it lacks reflections about how the norms and values of the worksite might influence the shaping of the intervention itself during the intervention process. It is recommended to apply a combination of the social constitution approach to worksites12,13 and an integrated food supply and demand perspective based on analyses of the co-evolution of problem–solution complexes.14,15 It is especially important to be aware about how an understanding of a problem and the proposed solution is co-shaped within the framework of the social constitution and its norms and values. Furthermore, it is important to concentrate on to what extent proposed solutions seem to solve the problem in focus and whether derived problems develop, for example with respect to food availability for certain social groups within the worksite, such as groups working irregular hours.
The two cases here show that the level of conflicts can differ substantially from one worksite to another depending on to what extent a change process opens new political issues at the worksite or whether it challenges the balance between existing norms and values. Conflicts should not be seen as negative but rather as necessary in relation to the development of a ‘good’ food intervention at a specific worksite. A lack of conflict could indicate a change process that is in accordance with existing norms and values, but it could also indicate that the relations between management, employees and different support functions are so asymmetrical that disagreement is not expressed.
From the systemic approach to workplace settings,11,20 it has been suggested that the throughputs, as part of the worksite as a system or setting, are unpredictable. Based on the two case studies, we also argue that the inputs (the existing norms and values of the worksite) and outputs (the developed problem–solution complexes) are unpredictable and need to be considered carefully and perhaps addressed directly during the design of a worksite food intervention. The case studies and the proposed theoretical perspective contribute to the foodscape perspective on worksites with an integrated food supply and demand perspective. Furthermore, the article contributes with a political process perspective to worksites and change processes at worksites. Finally, it proposes methods for collecting and analysing data within the political process perspective when analysing the social shaping of food interventions at worksites.