
Abstract
Introduction
Alcohol misuse is the amount and frequency of alcohol intake that can cause physical, psychological and social problems, both in the short term and the long term. 1 Worldwide, alcohol misuse causes 1.8 million deaths (3.2% of total deaths) and 58.3 million disability-adjusted life years (DALYs) (4% of total). Accidental injuries are responsible for about one third of the 1.8 million alcohol-related deaths, while neuro-psychiatric conditions are responsible for nearly 40% of the 58.3 million alcohol-related DALYs. 2
The European Union (EU) is the heaviest drinking region of the world, drinking 11 litres of pure alcohol per adult each year. 3 More than one in four deaths among men (aged 15–29 years) and one in every 10 deaths among young women in the EU are alcohol related. 4 Young people (aged 15–24 years) are responsible for a high proportion of this burden, with over 25% of youth male mortality and approximately 10% of young female mortality being due to alcohol use. 3
In many countries heavy episodic or binge drinking is prevalent among young people and is associated with an increased risk of accidents, violence, criminal activity, poorer health and social outcomes. Among young people, early initiation of alcohol use has been shown to be linked to later binge drinking, heavy drinking and alcohol-related problems.5–11
In school settings, universal prevention typically takes the form of alcohol awareness education, social and peer resistance skills, normative feedback, or development of behavioural norms and positive peer affiliations. Prevention programmes can be either specific curricula delivered as school lessons or classroom behaviour management programmes. In family settings, universal prevention typically takes the form of supporting the development of parenting skills including parental support, nurturing behaviours, establishing clear boundaries or rules, and parental monitoring. Social and peer resistance skills, the development of behavioural norms and positive peer affiliations can also be addressed with a family-based programme. Multi-component prevention programmes are defined as those prevention efforts that deliver interventions in multiple settings, for example in both school and family settings, typically combining school curricula with a parenting intervention.
In this article we provide an overview of three recently completed Cochrane systematic reviews of the effectiveness of universal alcohol misuse prevention programmes for young people up to the age of 18 years.12–14 A previous Cochrane systematic review,1,15 which included 56 studies (randomised and non-randomised comparative studies), was broader in scope and covered targeted as well as universal prevention programmes for alcohol misuse among young people (up to 25 years old) implemented in different settings (school, family, community, health clinics). While updating this previous Cochrane review, we found a large number of new randomised trials and new results from existing randomised trials. We therefore narrowed the scope of the review and produced three updated Cochrane reviews of randomised trials of universal school-/family-based and multi-component prevention programmes for alcohol misuse among youth 18 years or younger.12–14
Methods
We electronically searched MEDLINE, the Cochrane Central Register of Controlled Trials, EMBASE, Project CORK and PsycINFO for studies up to July 2010. The selection of studies was not restricted by language or status of publication. The references of topic-related systematic reviews and included studies were hand searched. Unpublished reports, abstracts, dissertations, brief and preliminary reports were also included.
Prevention programmes eligible for inclusion were any psychosocial or educational prevention programme delivered in school, family or multiple settings. Randomised trials that evaluated universal prevention programmes designed specifically for alcohol misuse, generic interventions (e.g. drug education programmes) or other types of interventions (e.g. screening for alcohol consumption) were eligible for inclusion.
The primary outcome of interest was any direct self-reported or objective measures of alcohol consumption or problem drinking (e.g. alcohol use: yes/no; alcohol intake: quantity/frequency; drinking five or more drinks on one occasion; incidence of drunkenness). Outcome measures related to psychological perception/attitudes or awareness were deemed as indirect and therefore were not considered for inclusion. Secondary outcomes covered alcohol-related behaviours (e.g. age of first drinking, age of first drunkenness and alcohol-related problem behaviours).
Two reviewers independently screened titles and abstracts of all identified records and then reviewed full-text reports of all potentially relevant records that passed the initial screening level. Differences in opinion arising at both screening levels were resolved through discussions. The risk of bias was assessed using the Cochrane Collaboration tool 16 (section 8.5.1). This assessment was based on the six methodological domains of validity (sequence generation, adequate allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other bias). Each item was rated with one of three possible responses: low, high or unclear risk of bias. For each response, an explanation was provided.
The statistical pooling of results of individual studies was planned conditional on the absence of heterogeneity with respect to study populations (e.g. baseline characteristics, gender), interventions (e.g. type, differences in target/focus) and outcome measures (e.g. different tools, instruments, scales), as well as the methodology of conduct (e.g. units of randomization and analysis, cluster-randomised vs individually randomised trials).
Results
The application of the narrower inclusion criteria to the previously published Cochrane review1,15 resulted in identifying 32 trials that were eligible for inclusion in the three new Cochrane reviews. The updated electronic searches (January 2002 to July 2010) identified 1,874 bibliographic records. The process of de-duplication resulted in 1,801 unique bibliographic records.
Through the initial screening of titles and abstracts, 1,648 records were excluded as obviously irrelevant. Full-text reports of the remaining 153 records were examined, of which eventually 40 records (26 trials) were included in the school review, 14 records (10 trials) in the family review and 29 records (20 trials) in the multi-component review. Combining the studies identified through the updated search with studies selected from the earlier review1,15 and additional results from hand-searching produced 53 studies for the school review, 12 studies for the family review and 20 studies for the multi-component review. A search flow diagram is depicted in Figure 1.
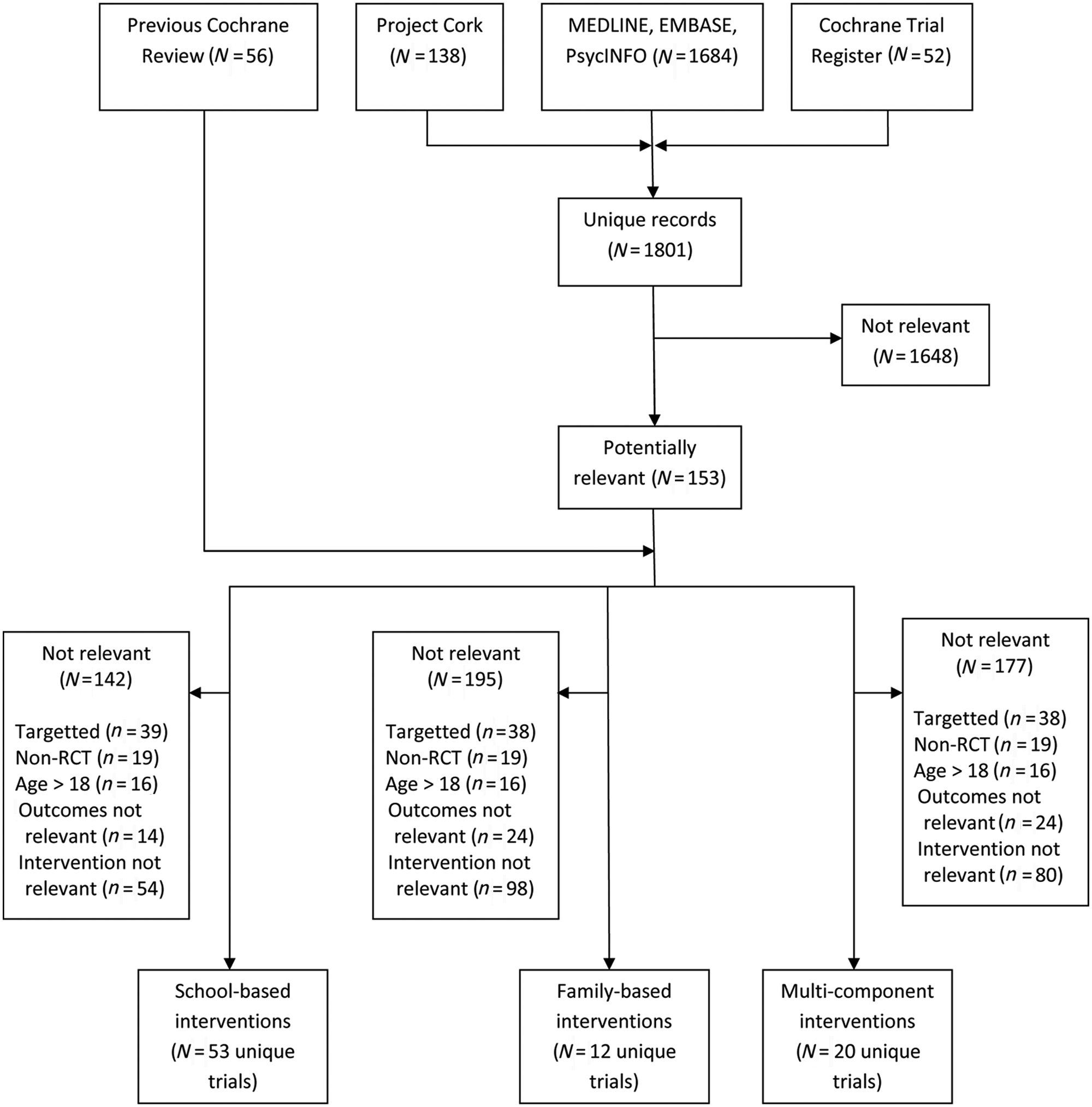
Search flow diagram
The reviewers could not pool the studies due to heterogeneity across study populations (baseline characteristics), interventions (differences in target/focus) and the outcome measures of alcohol misuse (different tools, instruments, scales, outcome definitions). Therefore, individual study findings were summarized qualitatively.
Results of the school review (n = 53 studies, 142,738 participants)
Forty-one trials were conducted in North America (the USA and Canada), six trials in Europe (the Netherlands, Norway, Austria, Belgium, Germany, Greece, Italy and Spain), six trials in Australia, one trial in India and one trial in Africa (Swaziland). Two trials were conducted in multiple countries. Most of the 53 included studies were cluster-randomised. The reporting quality of trials was poor, with only 3.8% of them reporting adequate method of randomization and programme allocation concealment. Incomplete data were adequately addressed in 23% of the trials. In this review, the number of studies that evaluated generic interventions was greater than the number of studies that evaluated alcohol-specific interventions (39 vs 11). The remaining three trials reported interventions targeting the use of cannabis, alcohol and tobacco.
Five17–21 of 11 studies that evaluated alcohol-specific interventions did not find any statistically significant effects, whereas six studies found significant beneficial effects of the interventions.22–27 Similarly, 25 of the 39 trials that evaluated generic programmes did not find significant positive effects, whereas the remaining 14 studies28–41 reported significantly beneficial effects of the programmes with regards to some of the measures of alcohol use.
Overall, among the generic prevention programmes, those based on psychosocial or developmental approaches such as the Life Skills Training programme,28,30 social skills and norms through the Unplugged programme, 42 and development of behaviour norms and peer affiliation through the Good Behaviour Game, 38 were more likely to report positive results over several years (up to 12 years with the GBG), although with effect sizes that were typically modest.
For both alcohol-specific and generic intervention programmes, there was no discernible pattern in characteristics (e.g. sample size, appropriate analysis, attrition rates, subgroups, intervention duration, unit of randomization) that would distinguish trials with positive results from those with negative results. The most commonly observed significant effects across programmes were for drunkenness and binge drinking. Duration of intervention impact tended to be longer for generic vs alcohol-specific or other programmes. Positive results for programmes observed in cluster-randomised trials, which did not account for clustering effects in the analyses, may have been spurious.25,27,36,39,40 Some trials22,25,26 observed subgroup effects (e.g. by gender, baseline alcohol use or levels of disruptive behaviour) or after adjusting or stratifying the main effects, some studies found significant effects only in certain subgroups.33–35
Results of the family review (n = 12 studies, 14,595 participants)
Eleven of the 12 trials were conducted in North America (USA) and one trial in Europe (Netherlands). Four trials were specific to females only, reporting gender-specific interventions. The reporting quality of trials was poor, only 20% of them reporting adequate method of randomization and programme allocation concealment. Incomplete data were adequately addressed in about half of the trials and this information was unclear for about 30% of the trials.
We found that nine of the 12 included studies43–52 demonstrated statistically significant short- and long-term effects in reducing alcohol misuse among young people. One study 54 found that the family-based intervention was effective when combined with a school-based intervention.
There is evidence that gender-specific interventions between daughters and parents, typically mothers28,39,40,43 can be effective in the short to medium term. Some trials observed subgroup effects differentiated by baseline alcohol 46 or drug use 52 status. One study 54 reported unexpected effects, in that the intervention seemed to increase the risk of alcohol misuse. However, before any attribution of iatrogenic effects of particular interventions can be made, it is important to rule out the possibility that such occasional unexpected results did not arise by chance, differential attrition or confounding.
Results of the multi-component review (n = 20 studies, 57,545 participants)
Seventeen of the 20 trials were conducted in the USA and the remaining three in the Netherlands, 54 Australia 55 and India. 56 The reporting quality of trials was poor, only 25% and 5% of them reporting adequate method of randomization and programme allocation concealment, respectively. Incomplete data were adequately addressed in about half of the trials and this information was unclear for about 20% of the trials.
Twelve of the 20 included trials54,56–66 found statistically significant beneficial effects of universal multi-component prevention programmes across a range of outcome measures, with persistence of the benefit ranging from three months to three years. One trial 67 reported statistically significant effects using one-tailed tests and may have been under-powered to detect significant effects using more conventional two-tailed tests. One trial 68 found significant effects but only in a sub-sample of baseline drinkers. Six trials55,69–73 found no effect of universal multi-component interventions for the prevention of alcohol misuse in young people.
There was inconclusive evidence regarding the benefits of additional components in different settings. Three trials showed no benefit of additional components56,61,71 and four indicated some possible benefit.42,66–68
Discussion
This review summarised three recently published Cochrane systematic reviews of the effectiveness of universal school-based, family-based and multi-component alcohol misuse prevention programmes in young people.12–14 In the school review we found studies that showed no effects of the preventive programme, as well as studies that demonstrated statistically significant effects. Most commonly observed positive effects across programmes were for drunkenness and binge drinking, and the evidence suggests that certain generic psychosocial and developmental prevention programmes can be effective and could be considered as policy and practice options. These include the Life Skills Training programme, the Unplugged programme and the Good Behaviour Game.
Most of the studies included in the family review reported positive effects for the prevention of alcohol misuse in young people. In conclusion, we found that the effects of family-based prevention interventions are small but generally consistent and also persistent into the medium to longer term.
Results from the majority of the studies included in the multi-component review showed significant effects of interventions for the prevention of alcohol misuse in young people, persisting into the medium and longer term. But a notable proportion of trials reported statistically non-significant results. We were able to assess the impact of single versus multiple components in seven studies, and of these only one study clearly showed a benefit of components delivered in more than one setting. In conclusion, there is some evidence that multi-component interventions for alcohol misuse prevention in young people can be effective. However, there is insufficient evidence that interventions with multiple components are more effective than interventions with single components.
In previous systematic reviews of alcohol misuse prevention for young people1,15,74 we have pointed to methodological limitations of included studies. Over this period, consensus statements have been published providing guidance on the reporting of randomised controlled trials generally 75 or more specifically for prevention trials. 76 Cochrane reviews have also become better at systematically identifying methodological limitations through a structured risk of bias assessment. The methodological quality of trials of alcohol misuse prevention for young people has improved over time, based on the reviews we have undertaken in 1997, 2002 and 2011.1,12–15,74
However, despite these improvements, important methodological limitations and reporting problems in the literature still remain. For example, in these reviews we found instances when cluster-randomised trials were analysed without taking into account clustering effects. Moreover, salient features 75 with regards to allocation concealment, randomization technique and blinding of outcome assessors were poorly reported.
Several studies undertook subgroup analyses but it was not clear if these were planned or post hoc, so such analyses should perhaps be regarded as hypothesis generating. It is also possible that some studies that looked only at main effects, without adjusting for potential confounders or effect modifiers, may have concealed possible subgroup effects (e.g. stronger effects in males). Several studies included in this review showed that certain subject-level characteristics such as gender and baseline alcohol may be potential effect moderators, so by not accounting for them in the analysis, subgroup effects may be missed. Effective universal prevention programmes (i.e. school, family or multi-component interventions) typically do not focus exclusively on the prevention of one behaviour, for example alcohol misuse, as these programmes have a psychosocial developmental orientation that is designed to impact on a range of health and lifestyle behaviours among young people. Such programmes offer an advantage over alcohol-specific prevention programmes by potentially impacting on a broader set of problem behaviours, for example cannabis, tobacco, harder drugs, antisocial behaviour.
Conclusion
Overall, we conclude that the evidence supports the effectiveness of certain universal prevention programmes for alcohol misuse prevention among young people. Some studies showing effect and others showing no effect may be a reflection of the fact that universal alcohol misuse prevention programmes are ineffective, and that there is simply a variation of individual study effect estimates around an actual zero effect, with some achieving statistical significance by chance. 77 However, we regard this as unlikely given the proportion and sample size of studies that found statistically significant effects, especially for family-based prevention programmes.
Ioannidis 77 has also warned that effects reported in published studies may not be true intervention effects but instead are simply measures of prevailing bias, especially when the true effect is very small or there is no true effect, when sample sizes are small and there is a higher risk of bias because of poor design or conduct of studies, when multiple outcomes are measured and analysed, or when there are no independent replications of the effects of specific interventions. This is a plausible explanation for many, if not all, of the positive results found in studies included in the three Cochrane reviews reported in this article.
Another interpretation of the overall picture of effectiveness of alcohol misuse prevention programmes for young people is that some psychosocial and developmental prevention interventions are effective for reducing alcohol misuse among young people only in particular settings. It is not clear why some prevention interventions seem to work in certain settings but not in others. Therefore, further investigation of the specific content of prevention programmes, and the context of their delivery, is warranted, so that clear recommendations regarding the transfer of particular prevention interventions to new settings can be made.
The content or ingredients of effective prevention programmes, as distinct from the content of ineffective prevention programmes, needs to be more clearly understood. For example, content may or may not vary importantly across different programmes. Unfortunately, standard scientific reporting of prevention trials does not include sufficient information about the content detail of prevention interventions to make an analysis of effective ingredients straightforward. Rather, programme manuals and unpublished reports have to be scrutinized, coded for different ingredients and then analysed, which is a labour-intensive and costly approach. Some early review work that has taken this approach has analysed the contribution of different ingredients of prevention programmes and these studies have highlighted a number of methodological and analytical challenges.78,79 A better understanding of the ingredients of interventions delivered as different components in different settings would be useful to help understand the results, albeit not conclusive, from the Cochrane reviews reported in this article.
Alternatively, contextual factors may also be important in determining the effectiveness of an intervention. For example, characteristics of programme delivery, including programme setting, key personnel or target age, may be important moderators of programme effects. A prevention programme shown to be effective in a low-prevalence adolescent-alcohol misuse setting or country may be ineffective where adolescent drinking is the norm and social and cultural pressures to drink are more powerful.
In order to better understand the importance of content and context for effective prevention, replication studies and more systematic reporting of programme content details and delivery contexts are needed. Meta-analysis, via subgroup analysis or using meta-regression techniques, could then be used to illuminate the important aspects of content and context for effective prevention interventions.
A final point to consider is that evaluation studies of single interventions may not be able to uncover effects that operate at a different level of understanding. For example, individual interventions, on their own, may not be effective when examined in randomised controlled trials but when a range of different interventions operate together then the overall, combined effect may be greater than just the sum of the individually ineffective parts. Assuming that individually ineffective interventions (e.g. schools programmes, family training and support, media campaigns, normative information, restrictions on advertising, constraints on pricing, etc.) will also be ineffective when combined may be a compositional fallacy, a type of category error suggested by Gilbert Ryle. 80 Although we have examined multiple interventions delivered in different settings in one of the Cochrane reviews, there was not enough evidence to scrutinise for a compositional fallacy.
In summary, current evidence suggests that certain universal prevention programmes can be effective and could be considered as policy and practice options. However, given the variability of results between studies it is recommended that particular attention be paid to programme content and delivery context, ideally through conducting further evaluation studies alongside any further implementation in different settings. Furthermore, as small effects could provide important cost benefits for prevention programmes, it is important to undertake studies with sufficient statistical power to detect small effects. Such small effects may vary in size and importance between subgroups, so further research should also be powered to detect hypothesized subgroup effects. Further improvement in study design, analysis and reporting in line with accepted guidance is required.75,76 Moreover, in all studies, reporting of programme content and context should be more detailed and systematic to enable comparison of these aspects across studies.
Footnotes
Acknowledgements
We are grateful to the UK Cochrane Collaboration and the National Institute for Health Research for providing support to update the 2002 systematic review.
DF conceived and led on the scope and design of the Cochrane reviews. DF and AT both undertook searches, screening and data extraction. AT led on data analysis. Both DF and AT contributed to drafting and writing the reviews. DF drafted this overview article and DF and AT revised the article to the final version.
DF’s department has received funding from the alcohol industry for adapting a family-based prevention programme, the SFP10-14 (formerly the ISFP). The adapted version is being evaluated in a large-scale randomised controlled trial in Wales, funded by the UK Medical Research Council. DF is a trustee of the UK alcohol industry-funded charity Drinkaware.