
Abstract
Aims:
The global health landscape has been characterized by shortfalls and imbalances in human resources for health (HRH), with more health workers concentrated in urban than rural areas. To address this maldistribution, some countries resorted to the implementation of a compulsory service policy for HRH. However, there is no comprehensive documentation describing the different components of such policies. This scoping review aims to determine the components for compulsory service for selected health professionals in low- and middle-income countries (LMICs).
Methods:
A search was conducted in MEDLINE, PLoS, Scopus, and ProQuest Central, using keywords for ‘compulsory service’, ‘return service’, ‘mandatory service’, ‘physician’, ‘dentist’, ‘nurse’, ‘midwife’, ‘physical therapist’, ‘occupational therapist’, and identified LMICs. A total of 6757 records were retrieved and assessed, from which 41 relevant records were included in the study.
Results and conclusions:
Common elements of a compulsory service program are the following: a comprehensive master plan, clearly articulated program goals, appropriate education and training, transparent recruitment and placement, strong institutional and system support, competitive benefits and incentives, and active management of exit from the program. Results presented in this article can serve to inform LMICs on policy, guide program development and management, and direct future research in the area of HRH to address challenges in maldistribution.
Introduction
The global health landscape has been characterized by shortfalls and imbalances in human resources for health (HRH), with more health workers concentrated in urban than rural areas. In 2006, for instance, the WHO 1 estimated that there is a shortage of about 4 million physicians, dentists, nurses, and midwives around the world, and that more health workers are concentrated in urban than rural areas. The maldistribution of health personnel contributes to great disparities in health outcomes between rural and urban populations. 2 A shortage of qualified health workers in remote and rural areas impedes access to healthcare services for a significant percentage of the population and challenges the aspirations of achieving health for all. 3 One strategy of the Sustainable Development Goals (SDG) to ensure healthy lives and promote wellbeing for all ages by 2030 is to substantially increase health financing and the recruitment, development, training, and retention of the health workforce in developing countries, especially in least developed countries and small island developing states. 4 Several low- and middle-income countries (LMICs) such as Malawi, 5 Philippines, 6 South Africa, 7 and Thailand 8 implemented compulsory service mainly as a government response to the maldistribution of health professionals especially in rural and remote areas. 9
Although there are available case studies and country reports on compulsory service, as well as a paper describing the typology of compulsory service programs implemented in the past, 9 there is no comprehensive documentation describing the different components of such programs. This scoping review aimed to determine the components for compulsory service for selected health professionals in LMICs. Careful consideration of these components by governments of LMICs should inform mandatory service policies and programs to ensure their comprehensiveness and attain specific goals for HRH, particularly the improvement of the supply and distribution of health workers, and may alleviate these countries’ economic and financial challenges, being recognized drivers of HRH distribution.
Methods
This study used a scoping review of literature using the methodology described by the Joanna Briggs Institute. 10 A scoping review is a rapid method of assessing and appraising the literature, with the purpose of rapidly mapping and summarizing the key concepts underpinning a research area, especially one which has not been fully explored or defined in other studies. 11 Scoping reviews are used to identify knowledge gaps, set research agendas, and identify implications for decision-making. 12
The framework for conducting a scoping review was first articulated by Arksey and O’Malley in 2005, and further refined by Levac, Colquhoun, and O’Brien in 2010. However, as an emerging field of evidence review, there is not yet a standard, or generally accepted, methodology in conducting a scoping review.13,14
The scoping review addressed the question, ‘What types of institutional and support systems were put in place by LMICs in the implementation of compulsory service policies for selected health professionals?,’ the elements of which are the following (Table 1): (1) population: physicians, nurses, midwives, dentists, occupational therapists, physical therapists; (2) concept: institutional and support systems, to include, but not limited to, legal, financial, developmental, labor market components – these can be clustered into three categories, using the socio-ecological model: institutional, community, and public policy factors; (3) context: LMICs, as classified by the World Bank.
Expanded search terms
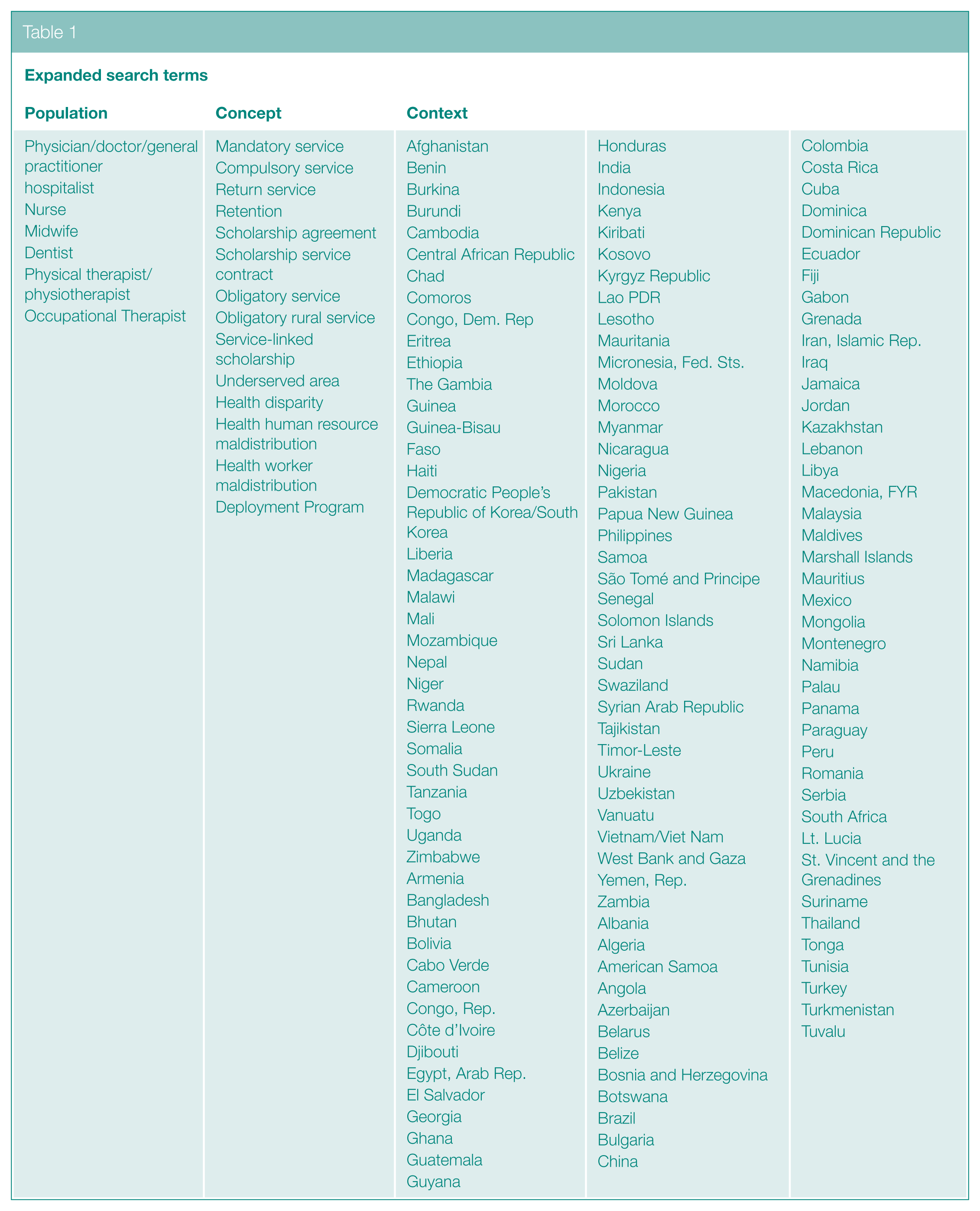
We would like to note that, while the WHO defines HRH broadly as ‘all people engaged in actions whose primary intent is to protect and improve health’, 1 we limited our search to the six professional categories listed above as defined in the terms of reference of this commissioned research. However, we conceived of ‘compulsory service’ more broadly as any form of national or institutional policy or program requiring professionals to work within a defined setting, either as a government mandate or in exchange for certain incentives. The paper by Frehywot et al. 9 provides an extensive discussion of the types, definitions, and examples of compulsory service policies or programs implemented in different countries.
A preliminary search was conducted in MEDLINE using Medical Subject Headings (MeSH) terms for ‘compulsory service’, ‘return service’, ‘mandatory service’, ‘physician’, ‘dentist’, ‘nurse’, ‘midwife’, ‘physical therapist’, ‘occupational therapist’, and the names of the identified countries. Preliminary yield of records were then analyzed in terms of text words contained in the title, abstract, and index terms. The expanded list of keywords and index terms were used for a secondary search for literature using the databases MEDLINE, PLoS, ProQuest Central, and Scopus. See supplemental material for detailed search strategy for each database. The choice of search engines was based on availability of institutional access/subscription to these databases. Studies that satisfied all of the following criteria were considered for inclusion in the review: (1) discusses the population, concept and context described above; (2) any type of article, for example, case studies, primary researches, reviews, editorials, and so on; (3) accessible full-text article; (4) available in the English language; and (5) published between 1 January 1990 and 31 December 2015.
Records obtained from the databases were screened for duplicates. Non-duplicate records were reviewed based on their titles and abstracts according to relevance. Full texts of potentially relevant records were further reviewed. Reference lists of relevant records were searched using an iterative approach, regardless of publication dates. Data were abstracted by two independent reviewers, any disagreement or discrepancy was resolved through consensus. Analysis of the records was conducted using the working lifespan strategies framework of WHO 1 and encoded using Excel (Part of Microsoft Office Professional Edition (computer program); Microsoft, 2013).
The process for scoping review was documented using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 15
Due to feasibility constraints, no hand searching for relevant journal titles, nor author contact for access for full-text records or additional information, was conducted. Furthermore, this study excluded individual and interpersonal factors in the data gathering and analysis. Databases were searched from October to December 2016. Subsequently, data abstraction and analysis was done from December 2016 to January 2017.
In order to provide a clear picture of the mechanisms involved in the implementation of compulsory service programs, a realist approach to the scoping review was used, with the working lifespan strategies of the WHO1 as the analytic framework. This categorized the system components into the workforce development stages of entry, workforce, and exit.
This study received clearance from University of the Philippines Manila Research Ethics Board (UPMREB-2016-360-01). In addition, the results presented in this article are part of a research project entitled ‘Feasibility of a Return of Service Agreement for Selected Human Resources for Health in the Philippines’.
Results
A total of 6757 records from across the databases were identified. After deduplication and assessment, 41 relevant records1–3,5–9,16–48 were included in the study (Figure 1). Records included in the analysis spanned from 1980 to 2015, 41% of which were published between 2011 and 2015. The greatest number of records were for the years 2014 (5), 2005 (4) and 2015 (4). Notably, there were only six papers included in the review that were published earlier than the year 2000.
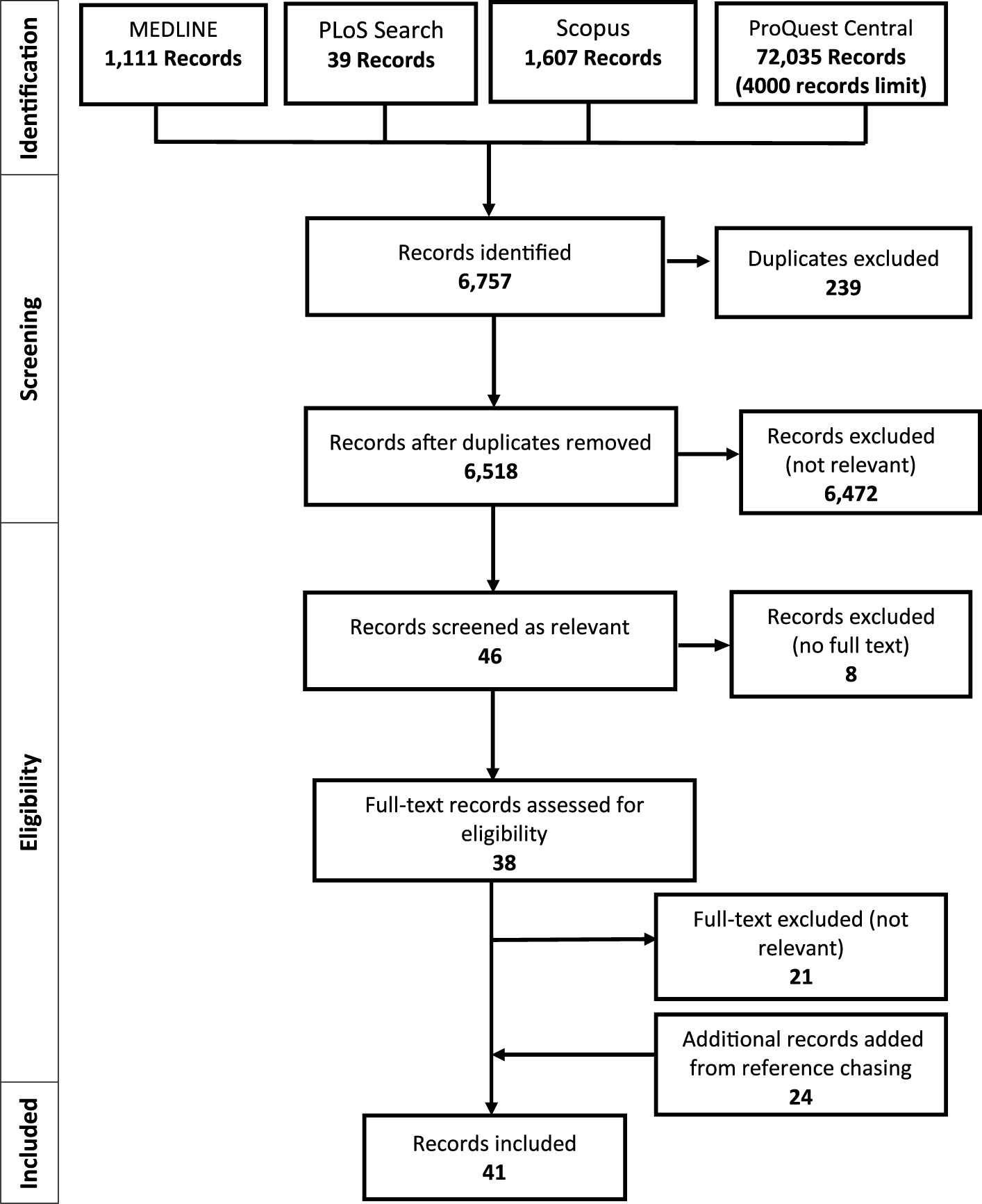
PRISMA Diagram for the Scoping Review Process
Several countries, including LMICs, implemented compulsory service programs. From the literature reviewed in the scoping exercise, records either referred to two or more countries (n = 9, 21.95%), specific countries and territories (Malawi (n = 4, 9.76%), South Africa (n = 5, 12.20%) and Thailand (n = 5, 12.20%) were mentioned most frequently), or no specific country (n = 5, 12.20%), exploring their implementation of compulsory service programs.
With regard to specific health professions, the majority of the records described the compulsory service programs and policies for physicians (n = 17, 41.46%) and nurses (n = 4, 9.76%). However, some records discussed two or more professions (n = 14, 34.15%), while the remaining records did not refer to any specific profession (n = 6, 14.63%).
Evidence from the review of literature suggests that there are different components needed to implement a compulsory service policy, briefly described later.
Plans and programs
Comprehensive programs for compulsory service were implemented by different countries to address the health inequity and maldistribution of health professionals, especially in underdeveloped regions and rural areas. These programs were classified into the following: (1) condition of service/state employment program, (2) compulsory service with incentives, and (3) compulsory service without incentives. 9 Programs were set up by government8,16 and/or non-government institutions,16–18 and either had or emphasized the need for clearly articulated goals,19,20 transparent processes for selection, recruitment, and placement of professionals,1,19,22–26 and periodic reviews to determine their effectiveness. 21
Education and training
It was apparent in most articles included in the review that compulsory service programs tied to education which desired full cooperation from their graduates had a need to ensure that the skills required in their stipulated choices of work postgraduation are congruent with the terminal competencies developed by the graduates throughout the course of their education as indicated in their respective curricula, with a focus toward addressing local health needs.6,18,25,27–31 Entry into these service programs, in order to defray the cost of education, was through the availment of scholarships, grants, bursaries, or loans.2,3,5,8,16–18,20,21,23,26,28,30,33–38 Students under the scholarship programs were mentored by physicians with experience in communities and underserved areas.5,30,31,35 Some schools made inclusion in a compulsory service program into a requirement for admission, while others exercised preferential selection and admission of students who come from areas of need; the latter is supported by international evidence suggesting that exposure to rural communities during undergraduate studies can influence choices to work in rural areas.1,16,22–24,27,32
Recruitment and placement
Fulfillment of compulsory service via recruitment into the workforce was found to have been accomplished through placement in public facilities, either in hospitals or community health centers that are managed by the Ministry of Health or state governments.3,7,8,16,19,22,24–27,29,32,36,39–41 While priority is given to rural placement, there is evidence that urban-based facilities were in the list of placement sites. 26 Preference for placement in the hometown of the student was practiced in some countries1,22–24 while placement by lottery or random assignment was also implemented. 25 Regardless of the model, transparency of the process was emphasized in the literature.1,19,22–26
Institutional and system support
Institutional and system support was provided to professionals who entered the workforce as part of their compulsory service obligation during their period of stay, which included orientation, clinical supervision, professional mentorship, and management support.5,19,25,29,42 There is evidence that the professionals were closely monitored through site visits, messaging, phone calls, and regional assemblies from the start of their undergraduate education until 2 years after the completion of their service agreement. 5
Professionals were provided with functional health facilities and other supplies and tools for practice such as practice guidelines.8,18,19,22,25–27,32,41,42 Opportunities for professional development and support for continuing education to improve the professionals’ clinical and management knowledge and skills were made available as part of the program as well.5,19,26,36,40,42
Benefits and incentives
Provision of decent salaries and incentives was most commonly cited among the benefits and incentives given to professionals rendering compulsory service.8,19,26,35,38,42–44 Other components of remuneration packages for these professionals include additional financial incentives for rural, remote, or hardship posts26,27,29,36,42 and incentives for excellence in service. 21
Non-financial incentives were provided as well, which were inclusive of (but not limited to) housing, insurance, and a safe working environment.19,20,36,40,41,43,44 In some cases, a reduced length of service was offered if the professional was assigned to serve in a hardship area. 27
Exit from the program
In order to ensure completion of compulsory service among professionals, several mechanisms were instituted by various countries such as recognition of rendered service while still enrolled in a professional program, 28 offering of funding opportunities for postgraduates and training after completion of service,2,7,18,26,44–47 and the institutionalization of compulsory service completion as a prerequisite for graduation, license to practice, or admission to further education or training.8,45
Alternatively, some countries imposed a fine and penalty system for non-compliance and violation of compulsory service contracts. The value of the penalty was, in most cases, found to be equivalent to educational assistance received, and at times corrected for inflation.2,8,29,40,46,48
Discussion
Regardless of the type of compulsory service implemented in the countries included in the study, there are several common elements identified. These are the following: a comprehensive master plan; clearly articulated program goals; appropriate education and training; transparent recruitment and placement, strong institutional and system support; competitive benefits and incentives; and active management of exit from the program.
The review shows that the common elements identified in compulsory service programs are consistent with the Working Lifespan Strategies of WHO, 1 specifically its entry phase. The working lifespan strategies is composed of three different phases: the aforementioned Entry phase, wherein the workforce is prepared through strategic investments in education and effective and ethical recruitment practices; the Workforce phase, where performance enhancement is ensured through better management in both the public and private sectors; and finally the Exit phase, where migration and attrition are managed to reduce wasteful loss of human resources. Table 2 shows the common compulsory service components identified from this scoping review that are present in the entry and workforce phase of WHO’s working lifespan strategies.
Components of a compulsory service program
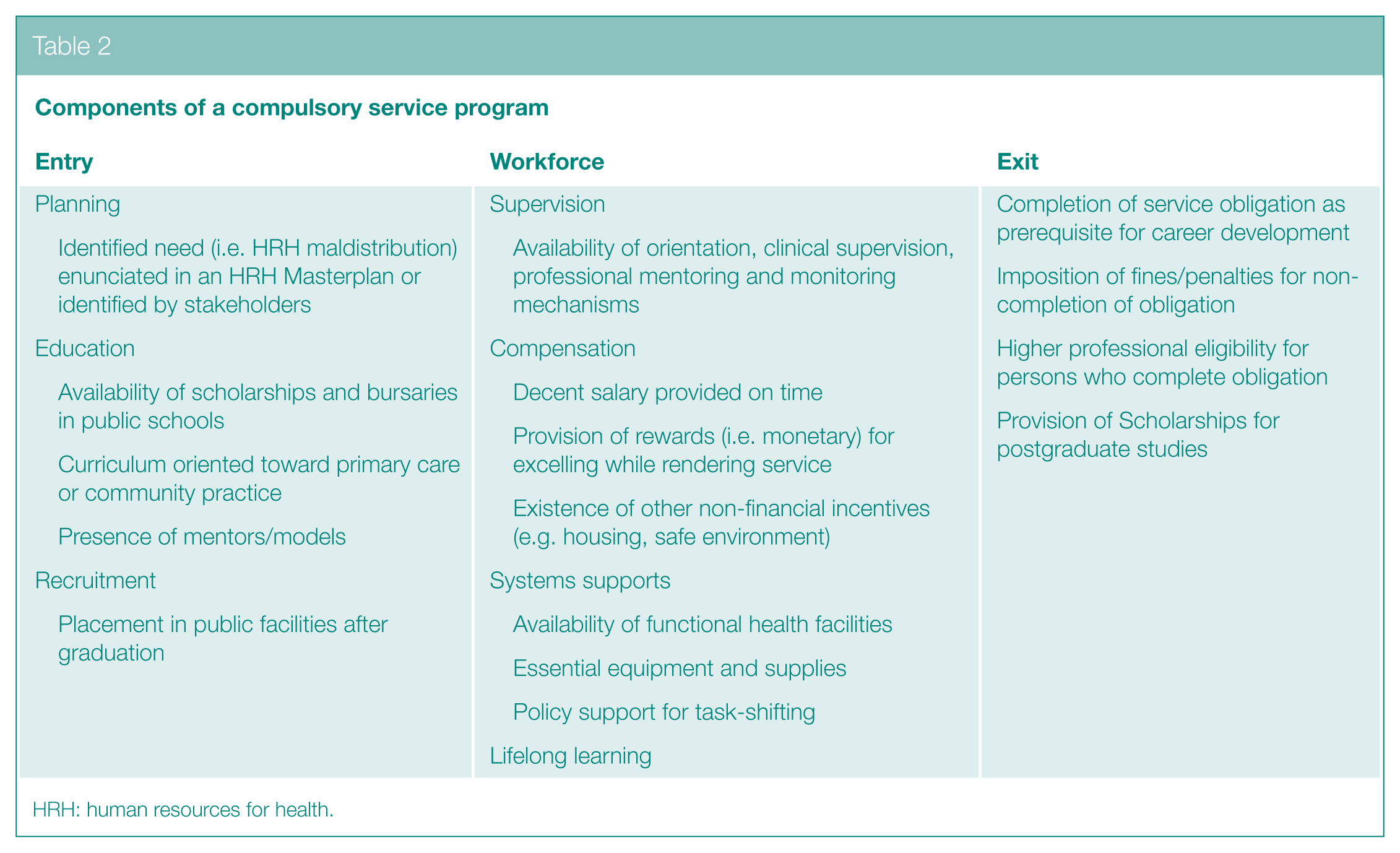
HRH: human resources for health.
While there are promising country experiences with compulsory service programs for health professionals,5–9 we maintain that this should be considered as but one strategy – and a temporary one at that – within a country’s broader human resource management master plan. The shortage and imbalance of health workers require that policy-makers and health program managers strive to address the larger contextual push and pull factors that affect health worker migration within and between countries. 1
To our knowledge, this article is the first that has attempted to generate a framework that outlines the components of a compulsory service program, distilled from the experience of different countries across a broad time frame.
Due to limitation in the scope of this commissioned research, we would like to emphasize that this scoping review does not purport to describe an ideal compulsory service program, nor does it assess the effectiveness of the established compulsory program.
Our results, however, will need to be interpreted with caution as the possibility of bias in the inclusion of literature remains given the constraints imposed in the search process (i.e. databases searched, reliance on accessible material, restriction to English language publication). The technical design of one of the databases (ProQuest Central) also automatically truncated search results to the first 4000 records (or about 5.55% of the total database yield), a dilemma acknowledged by the database administrator when we contacted them with respect to this concern. We are of the considered opinion, however, that these limitations are partly addressed by our use of multiple databases for cross-searching and comparison, as well as citations searching within the included records.
Conclusion
Our scoping review of literature showed that while LMICs varied in terms of their operations for the implementation of a compulsory service program, common components include comprehensive planning, skills development through education and training, recruitment and placement, institutional and system support, sufficient benefits and incentives, and tracking and further benefits upon exit from the program. These components must be in place for a compulsory service program for health professionals in LMICs.
The smooth and successful implementation of all three arms (entry, workforce, and exit) requires the universal cooperation among educational institutions, members of the health sector requiring competent graduates, and the government, together with accurate data on the quantity and quality of graduates produced and worker performance which may be reflected in skill mix analyses, performance evaluation, and other components of a labor market analysis.
Supplemental Material
10.1177_1757913919839432_Supplementary_material – Supplemental material for Components of compulsory service program for health professionals in low- and middle-income countries: a scoping review
Supplemental material, 10.1177_1757913919839432_Supplementary_material for Components of compulsory service program for health professionals in low- and middle-income countries: a scoping review by CT Antonio, JP Guevarra, PN Medina, MD Avelino, AG Agbon, DC Sepe, DD Bardelosa, MM Cengca, ML Ting and AB Lara in Perspectives in Public Health
Footnotes
Acknowledgements
We acknowledge the critical inputs provided by the Health Human Resource Development Bureau and Health Policy Development and Planning Bureau, Department of Health, Republic of the Philippines in the technical report from which this article was derived. Likewise, we significantly benefited from the critique received from anonymous external referees appointed by the Philippine Council for Health Research and Development, Department of Science and Technology, Republic of the Philippines.
Conflict of Interest
M.M.C. and A.B.L. were fulfilling their compulsory service program obligation at the time of the conduct of the study. All other authors declare no conflict of interest.
Funding
This research project has been funded through the Department of Health, Health Systems Research Management in collaboration with the Philippine Council for Health Research and Development. This article reflects the points of view and thoughts of the authors, and the information, conclusions, and recommendations presented are not to be misconstrued as those of the Department of Health nor of the Philippine Council for Health Research and Development. The material presented here, however, is done in the spirit of promoting open access and meaningful dialogue for policy/plan/program improvement, and the responsibility for its interpretation and use lies with the reader.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.