
Abstract
Aim:
This review considers prominent risk factors and mitigation strategies of influenza among Indigenous children.
Methods:
Seven electronic databases were searched from the period of 2004–2017 to locate articles discussing influenza among Indigenous children in the developed circumpolar nations of Australia, Canada, United States, and New Zealand. Articles selected for inclusion discussed influenza among Indigenous children as either individuals or as a part of a community. Ancestry searches of articles meeting the review criteria were also undertaken to discern seminal research in this topic area.
Results:
From the 39 primary research studies included, marked risk factors and mitigation strategies of influenza among Indigenous children were identified using inductive analysis. Notable risk factors included age under 2 years, cigarette smoke exposure, presence of a chronic illness, and crowded living conditions. Successful mitigation of influenza for Indigenous children included strategies to improve vaccine coverage, provision of health education, and policy change.
Conclusion:
In the past, the impact of influenza upon Indigenous communities has been devastating for both children and their families. By utilizing existing public health infrastructure and collaborating with culturally unique Indigenous groups, preventive action for Indigenous children at significant risk of contracting influenza can be realized.
Introduction
The term influenza encompasses an array of virus strains, which are known worldwide for being the cause of the colloquial ‘flu’ illness.1,2 The influenza virus typically manifests clinically as a fever and respiratory symptoms, such as a cough and increased airway secretions.1–6 Although rare, secondary bacterial complications such as pneumonia, epiglottis, and soft tissue abscesses may also arise.4–6 Antivirals are often prescribed at first sign of influenza symptoms to halt illness progression, and antibiotics have shown positive effect in the resolution of secondary bacterial complications.3,7,8 However, there is no cure for influenza, and treatment is directed by comfort.3,7–9
The disease burden created by influenza is felt greatly at the global level. This burden is perpetuated through both small annual outbreaks, typically impacting 5% of the world’s population, and large-scale pandemics, as seen in 1918 and 2009 outbreaks.10–13 Dispersion of influenza is not uniform, and it has been identified that unique population groups have a higher propensity toward carrying the influenza-related disease burden.2,14–16 Among these groups vulnerable to influenza, Indigenous children of developed circumpolar nations experience a higher incidence and severity of illness from the influenza virus than non-Indigenous children living in the same reg-ion.3,6,17–20 This difference in severity has been demonstrated by studies that reveal 0.2–9.1 times greater risk of death and two to five times more frequent rate of hospitalization from influenza among Indigenous children than non-Indigenous children of the same age.6,18,19 In addition, Indigenous people as a whole are an overrepresented population in the incidence of influenza, but Indigenous children specifically experience a higher disease burden in relation to other Indigenous age groups.6,14,18,21,22 Between 1999 and 2009 in Australia, the highest rates of influenza-related hospitalization among Indigenous people were seen in the 0–4 years age group.4,6 Likewise in Canada, during the H1N1 outbreak of 2009 the 0–4 years and the 5–9 years age groups were found to be the most frequently hospitalized among the Indigenous population in the province of Manitoba.18,22
Noting the negative impact of influenza upon Indigenous children of developed circumpolar nations, this article aims to synthesize what risk factors put Indigenous children at an increased risk for the contraction of influenza and explore strategies to mitigate the dispersion of influenza among Indigenous children from the existing research. Concurrently, this review also seeks to uncover shared risk factors and mitigation strategies of influenza for Indigenous children between the nations of Australia, Canada, United States, and New Zealand. Such shared attributes may be beneficial in driving future disease prevention and health promotion activities internationally.23,24
Previous research on Indigenous children’s experience of influenza is generally limited.3,25 In the available literature, influenza has often been studied alongside other infectious diseases or in the larger context of all Indigenous population age groups. 7 To the authors’ knowledge, using this limited literature to synthesize a scoping review that focuses specifically on influenza among Indigenous children has not been done in the past.
Methods
Using the electronic databases Access Medicine, CINAHL, EMBASE, ProQuest Nursing & Allied Health Database, PubMed, Scopus, and Google Scholar, an iterative keyword search strategy was adopted to locate studies examining influenza among Indigenous children. 24 The term ‘Indigenous’ is used to refer to the original people and their descendants of Australia, Canada, United States, and New Zealand who have suffered similar histories of colonization and assignment to minority status. 23 Articles were searched for within the inclusive time period of 2004 to 2017, to build a review that reflected diverse influenza outbreaks that have occurred over time. As well, the parameters of English language and full-text articles were applied to each search. To provide a broad search with optimum sensitivity, a combination of the following keywords was formatted to uniquely suit each database search: ((Indigenous) OR (Aboriginal) OR (Maori) OR (Native American)) AND (influenza) AND ((children) OR (paediatric) OR (pediatric)) AND ((risk factors) OR (mitigation strategies)). Beyond primary research, articles were included for this review if there was exploration of influenza risk factors or mitigation strategies within the Indigenous populations of Australia, Canada, United States, and New Zealand. As research on Indigenous children is limited, articles were included that examined influenza within the general Indigenous or pediatric population, with confirmation pending that study findings were age or ethnicity specific. Reference lists from the eligible articles were also searched to locate further primary research for inclusion.
All articles generated by database searches were read by the first author for initial inclusion screening and then reviewed for analysis. Identification of risk factors and mitigation strategies occurred through independent inductive analysis by the first and second author, allowing for overarching themes applicable to Indigenous people of developed circumpolar nations to emerge. 23 Risk factors were identified as characteristics that aid in the early recognition of disease progression and mitigation strategies defined as interventions aimed at preventing the dispersion of influenza. 26 Themes found in the literature during independent review were then discussed between authors until a consensus was reached. To provide context to these themes, study characteristics such as study design, participant groups, healthcare discipline, and country of origin were also extracted from the included articles.23,24
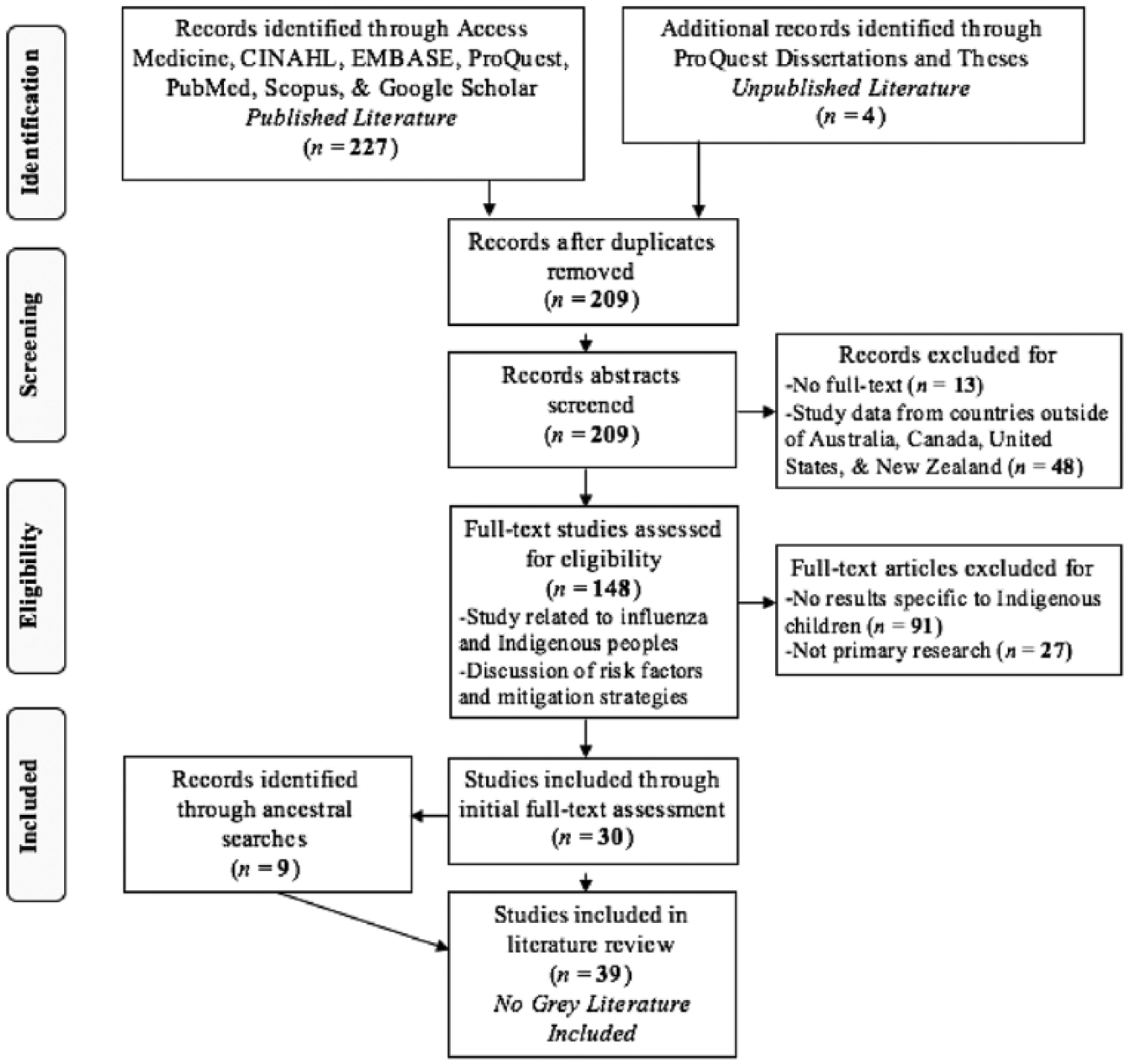
In total, 148 articles were identified during the keyword search of databases (Figure 1). Of these articles, 118 were excluded for either not being primary research (n = 27) or not reporting data specific to Indigenous children (n = 91). A total of 11 additional studies were then located from ancestry searches of the 30 studies. In total, 39 articles were found to meet the inclusion criteria as outlined earlier and were analyzed for this review.
Review criteria 27
Of the included articles, all 39 were published and 37 used a quantitative methodology. Articles of quantitative study design were classified as case controls, case reports, cohort studies, and cross-sectional studies. 28 For this review, the study design and participant group were classified based on the ‘METHODS’ section, and healthcare discipline was inferred from the background most prevalent among authorship. Country of origin was determined in 37 articles by the country from which the study data or sample originated. The two remaining studies complied data from a partnership between neighboring countries and were classified as ‘Multi-National’.29,30
Results
Description of studies
Most research included in this review utilized a retrospective population-based study design and originated from Australian researchers in the healthcare discipline of epidemiology (Table 1). A total of 24 studies exclusively collected data from a sample of participants who were identified as Indigenous in ethnicity. All studies commonly addressed the research objectives of influenza-related hospitalizations, vaccination, age-specific incidence of influenza, and influenza virus transmission. Diagnosis of influenza was reported across the literature through both participant self-report (n = 3) and laboratory testing (n = 37), such as nucleic acid testing.11,13,15 Study characteristics are presented in more detail in Table 1.
Study characteristics
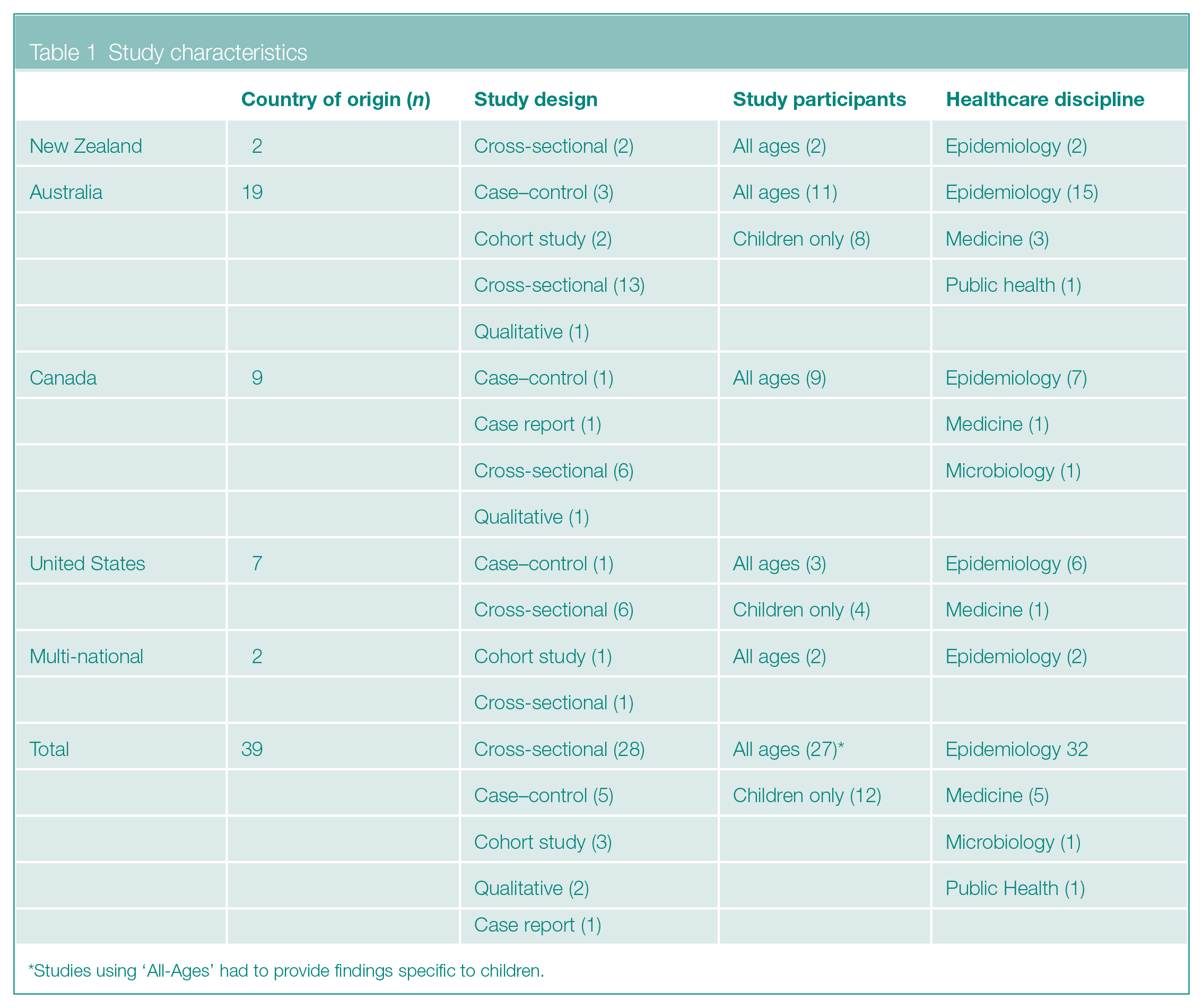
Studies using ‘All-Ages’ had to provide findings specific to children.
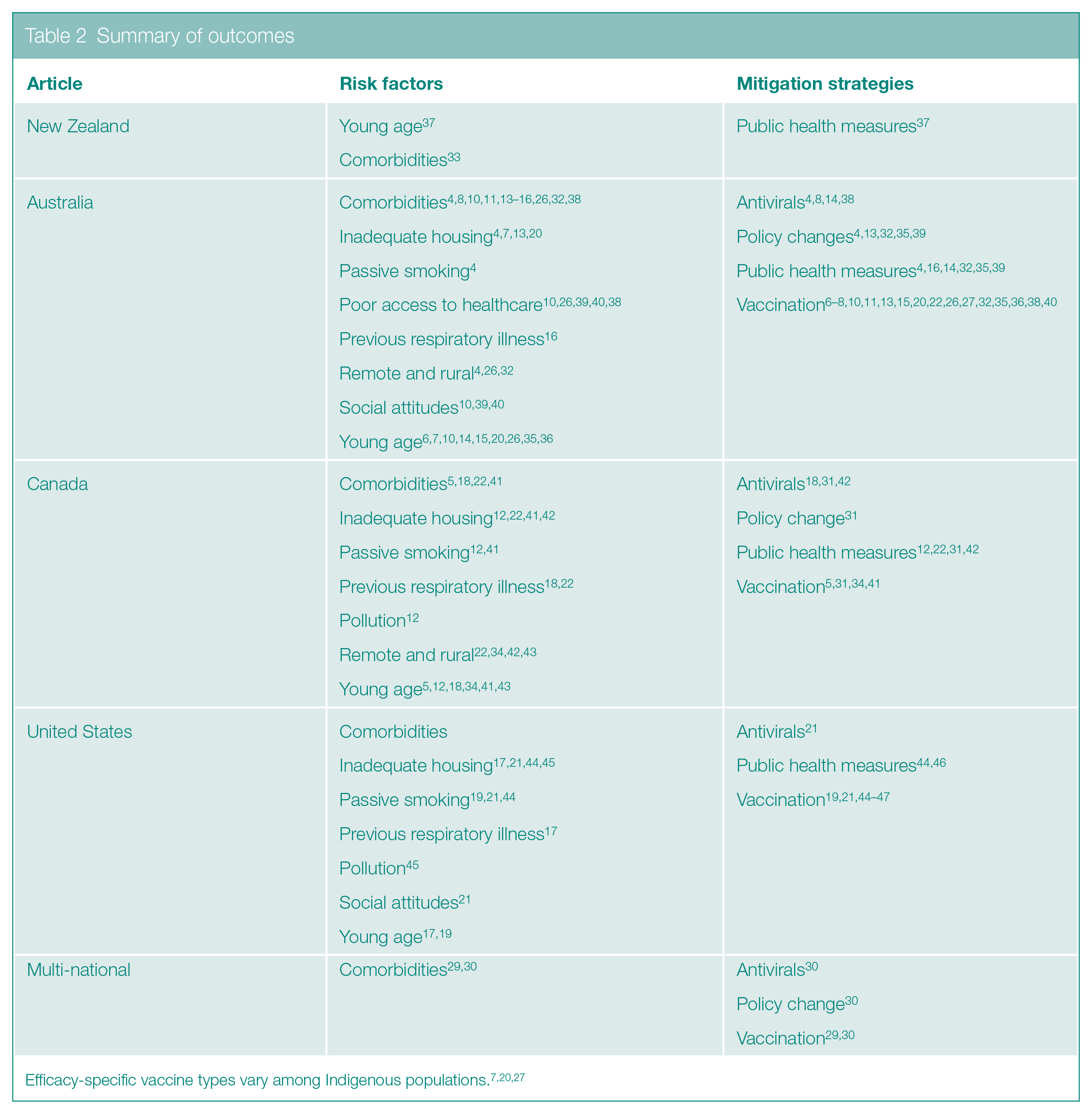
With regard to shared attributes of influenza among studied countries, nine studies explicitly discussed the health disparity of elevated influenza rates among Indigenous people of circumpolar developed nations.4,14,15,20,29–33 Potential to address influenza among Indigenous children internationally was described by nine studies, which explained the existing partnerships between nations that had already aided research and mitigation strategies in this topic area.4,10,13,20,32–36 For example, one article utilized the Australian and New Zealand Intensive Care Society registry, a multinational database, in the study to locate Indigenous participants diagnosed with influenza during the 2009 pandemic. 13 Several Canadian and American research studies also described sharing information in the development and clinical testing of seasonal influenza vaccinations.20,34,35 The two studies classified as ‘Multi-National’ in the ‘Methods’ section were also the product of the existing international partnerships between the countries of United States and Canada, and New Zealand and Australia.29,30 A complete summary of all included literature and results is provided in Table 2.
Summary of outcomes
Risk factors
Common factors that were seen to increase the likelihood of contracting influenza among Indigenous children were organized under the following categories: social attitudes, environmental factors, and biological factors. Although the abovementioned categories are not mutually exclusive, based on the included literature these factors were considered the most prominent indicators for risk of contracting influenza among Indigenous children.
Social attitudes, which are common perceptions and cultural values of both healthcare professionals and guardians of children, have been found to negatively affect healthcare services sought and final health outcomes among Indigenous children who have contracted influenza.9,10,21 Notable examples of such social attitudes include guardian or healthcare professional underestimation of respiratory illness severity and guardian distrust in healthcare organizations.10,21 Nurses also reported differing cultural norms between themselves and Indigenous patients as a barrier to providing effective influenza vaccination and education.10,39,40
Due to the mode of transmission of the influenza virus, direct contact and respiratory droplet, several environmental factors play a role in how this illness is spread among Indigenous children. 13 Environmental factors include passive smoking, pollution, and inadequate housing, which more specifically refers to diminished access to running water, poor condition of housing, crowding, and lack of temperature control. Evidence also suggests that the lack of primary healthcare services in the immediate environment of Indigenous children creates risk for influenza, as access to healthcare and health surveillance in the community is diminished.17–19,39,42,43 Rural and remote location, defined by each country’s indexing system, is believed to further contribute to poor access to primary healthcare services as residents must travel significantly longer distance to access healthcare services and less public health monitoring is occurring in these areas.12,42
However, in this review, biological factors of comorbidity, previous history of respiratory illness, and young age occurred with greater frequency than any other category of risk factors. Specific chronic illnesses attributed with a higher risk of influenza among Indigenous children were established in the literature as diabetes, obesity, and immunosuppressive disorders.8,16–18,22,38 Previous respiratory illness was described as a separate entity to chronic illness in 11 studies due to the greater severity and duration of influenza-related illness observed with recurrent respiratory infections.10,11,15–19,22,33,41 Finally, Indigenous infants have exemplified higher rates of nasopharyngeal influenza virus colonization than those of non-Indigenous descent, which is believed to be caused by higher densities of nasal epithelium.3,5,7,25 Thus, due to elevated nasal colonization of influenza and generally naive immune system of young children, Indigenous children aged two years and younger are felt to be at heightened risk for receipt of influenza.5,7 No definitive claims toward gender as a risk factor were made in any of the included studies.
Mitigation strategies
The following three categories of mitigation strategies were identified during this review: public health measures (n = 13), pharmaceutical intervention (n = 33), and policy changes (n = 8). Although not all strategies have been trialed on a national or even international platform, each specific strategy was mentioned as having been previously successful in preventing the transmission of the influenza virus. For many of these mitigation strategies, the opportunity to be trialed arose during the influenza pandemic of 2009 (n = 17).
Discussion of public health measures in the literature of this review included provision of health education and closure planning, which has been found to produce significant effect in reducing the transmission of influenza locally among children in school or day care.22,31,32,37,42 Specific to Indigenous children, studies employed health education programs geared toward improving knowledge of influenza among guardians and breaking the chain of infection through handwashing and coughing etiquette.4,14,31,32,35,44 Health education programs were also successful at reducing the transmission of influenza among Indigenous children when delivered in conjunction with Indigenous community partners.4,18,22,31,35
Pharmaceutical interventions identified in this review to mitigate influenza among Indigenous children included influenza vaccination and antiviral prophylaxis. Both pharmaceutical interventions were found to be more effective at reducing influenza among Indigenous children when administered directly to populations at high risk for contraction of influenza versus entire populations.4,7,8,10,13–15,18,21,31,32,38,44–47 Yet, considering the safety of present-day vaccinations and inability of vaccinations to cause viral resistance, as seen with antivirals, vaccinations were considered the most viable long-term mitigation strategy by four studies.5,10,20,21 Five studies cautioned healthcare professionals that vaccinations may not provide uniform coverage against influenza among Indigenous populations due to the unique genetic endowment and immunity status, but continued to support vaccinations as the best mitigation strategy available.7,20,31,27,41,45–47 In the case of short-term prevention, the most consistently recommended antiviral for children showing early influenza symptoms in the literature was oseltamivir, which can shorten symptom length by 24–48 h.8,10,14,31,42
Mitigation of influenza has also been sought through changes in current government, municipal, and organizational policies with the hopes of improving Indigenous child health through their quality of life.4,13,31,32 Previous policy changes that successfully reduced the risk of influenza among Indigenous children included mandatory pandemic planning for Indigenous communities, guidelines for appropriate resource allocation during an outbreak, hospital-based influenza screening guidelines, and improvement of Indigenous housing.4,7,31,32,43
Discussion
This article is the first known scoping review of risk factors and mitigation strategies of influenza among Indigenous children of Australia, Canada, United States, and New Zealand. Categories of risk factors located during the review included social attitudes, environmental factors, and biological factors. Concurrently, mitigation strategies specific to influenza were also grouped under the headings of public health measures, pharmaceutical interventions, and policy changes. All findings were uniformly pooled across nationally separate research studies, creating an indication that risk factors and mitigation strategies of influenza among Indigenous children are shared attributes between the four countries of analysis. Most notably, vaccination appeared in numerous studies in this review (n = 26) as a reliable and well-established mitigation strategy of influenza among Indigenous children in developed circumpolar nations. All risk factors and mitigation strategies identified in this review were shared among at least two of the included countries of study. Possible explanation for these shared findings could be traced back to colonialism, where Indigenous people of circumpolar countries experienced similar losses of culture, land, and dignity. 48 Further study would be recommended to confirm this relationship.
Utilizing these shared attributes of risk factors and mitigation strategies of influenza among Indigenous children in this review to improve the health of Indigenous children, will only be possible in the future with continued partnership between nations. Countries geographically close to one another, such as Canada and the United States, and Australia and New Zealand, have already begun to work together on research and programs to prevent the transmission of influenza.13,20,34,35 To enhance these relationships further, continued collaboration on research is encouraged, as seen in the two studies classified as ‘Multi-National’, or the replication of studies across nations is promoted to produce a global meta-analysis, as has been done in the past with respiratory illness among Indigenous people.29,30,32 Modes of sharing ideas or evaluations of health promotion and disease prevention programming on this topic should also continue to grow between countries through shared journals, such as the Australian and New Zealand Journal of Public Health, multinational podcasts, or international conferences.
Limitations
Study design and healthcare discipline of the included studies in this review lacked diversity as most included studies were cross-sectional and epidemiological. Therein, potential for exclusion of important risk factors and mitigation strategies lies with this report, which may have inadvertently used a search strategy biased toward certain study designs and healthcare disciplines. Evaluation of the methodological quality of the included studies did not fall within the scope of this review either, leading to possible inclusion of methodologically weak studies in the findings.
This scoping review was additionally constrained by the limited availability of data specific to Indigenous children, and hence, results were extracted from general research of the Indigenous population with age-specific results. This broad technique may have led to a superficial compilation of findings unique to Indigenous children and allowed for a large amount of variability in study content and understanding of review outcomes. However, the authors believe that a more broadly based review of risk factors and mitigation strategies of influenza provide necessary context for more focused future assessments among unique groups of Indigenous children.
Implications
Moving forward, this review calls for both additional research and intervention to reduce the disparities in health perpetuated by influenza among Indigenous children. Research focusing on the validation of mitigation strategies has improved since the 2009 pandemic, which provided many opportunities to trial strategies, but there is still potential to study how to best offer mitigation strategies across culturally diverse Indigenous groups. 31
Since most studies in this review were conducted using population-based data, the results produced a homogeneous picture of Indigenous children’s experience with influenza. 48 This picture is misleading, as the Indigenous populations of study in this review are composed of a vast number of diverse groups with distinct health values, patterns of healthcare utilization, and health needs.9,16,31,48 Future collaboration between researchers, community leaders, and healthcare professionals working within Indigenous communities may provide helpful insight into culturally appropriate practices for specific regions of the world.4,14,16,18,22,31,44,46 A notable example of differences in influenza-related experiences between various Indigenous communities can be seen when examining the topic of health education. Varying resources, healthcare services, and past outbreaks of influenza can dramatically change the learning needs of individual Indigenous communities.4,16,44,46
Conclusion
In regions of Australia, Canada, United States, and New Zealand where Indigenous populations reside, there must be even higher levels of preparation for future influenza outbreaks and active implementation of influenza prevention strategies knowing that this group is highly susceptible to infection.13,31 Although the results of this review may serve useful in such preparations, nothing should undervalue the needs and desires of the Indigenous community where prevention is required. 49 Instead, scientific inferences from research should act only as a starting place in the conceptualization of health promotion and disease prevention programs for Indigenous communities of developed circumpolar nations. 23
Footnotes
Conflict Of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
No ethical approval was required or obtained prior to conducting this scoping review.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.