
Abstract
Aims:
Chronic obstructive pulmonary disease (COPD) is a chronic respiratory disorder that affects health outcomes on multiple levels including overall wellbeing. More specifically, factors such as spiritual wellbeing, and psychological, mental and motivational status which may be at least as important as others, have been rarely studied. This article reports the method of validating a new wellness assessment questionnaire and the status of several wellness domains in patients with COPD.
Methods:
The study consisted of two phases: first, the development of a new Wellness Questionnaire with the help of focus groups; second, the validation and use of the questionnaire in a cohort of patients with COPD. For focus groups, healthy people ⩾45 years of age with no known comorbidity as well as people with a clinical diagnosis of COPD were invited to participate in the study.
Results:
Thematic analysis of findings from focus groups and original cohort respondents highlighted some factors that appear to influence wellness status. Five domains were explored as potential markers of wellness in patients with COPD. Quantitative analysis with Spearman correlation demonstrated a significant correlation between Physical/Personal Wellness and other markers of COPD progression such as Global Initiative Obstructive Lung Disease (GOLD; 0.006), force expiratory volume in 1 s (FEV1%; 0.01), health-related quality of life (0.009), multidimensional BOD score and quartile (0.003 and 0.02).
Conclusion:
The findings suggest that a combination of personal, physical, emotional, mental and other psychological factors is responsible for negative COPD outcomes. While there is a need to validate this new wellness questionnaire in further research, it incorporates new markers of wellness that could benefit management of COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is a complex chronic disorder and is one of the most prevalent diseases worldwide. It is also predicted to be the third most common cause of death by 2030. 1 The most common symptom these patients exhibit is shortness of breath that significantly impair COPD outcomes. One of the main goals in managing these patients is to maintain a good quality of life and overall ‘wellness’ for those affected. 2 However, in order to achieve and maintain ‘wellness’, clinicians are faced with the challenge of selecting a reliable tool that effectively assesses the severity of the disease and measures its effect on improving the patient’s overall quality of life. Studies suggest that there is a close link between breathing and wellbeing.3,4 Ardell5,6 suggested that ‘Breathing plays a role in long-term well-being’ and according to Japanese proverb ‘Cheerfulness is the very flower of health’. In other words, ‘Health’ has a general superficial meaning that means a person is in a disease-free state. Absence of current disease is no guarantee of a perfect disease-free future. There may be some hidden or unseen aspects of an individual’s life that may influence health and wellbeing. These include social interaction, sense of self-responsibility, mental fitness or a stress-free mind which would otherwise interfere with sleep, daily activities and appetite 7 and thus contribute to slowly progressive conditions like hypertension, diabetes, anxiety and depression. 7 Wellness can be regarded as a mental approach related to the lifestyle a person adopts or mental attitude that at the highest level of wellbeing can act as a placebo effect. 8 Wellness involves an integration of body, soul and mind and a belief in health. 9 Daily personal, social and emotional activities may have an impact on illness progression and recovery in both positive and negative ways. 10 Therefore, an assessment of wellness in patients with COPD has the potential to enhance disease outcomes. This is needed in the event of any chronic illness to develop awareness, energy and knowledge so that individuals can cope more easily with the realization that there may be no endpoint before death. Thus, it has the advantage of maintaining hope and encouraging a healthy lifestyle to avoid disease complications. Wellness involves an integration of body, soul and mind and a belief in health. 9 It enables a person to realize that everything we observe, think, perform and feel has a major impact on our state of health and state of wellbeing.
COPD is a complex condition involving multiple clinical manifestations that significantly impair functional, physiological and psychological health. Living with COPD requires people to manage disease-related symptoms in order to participate in the activities of daily life. It has been suggested that a patient’s health-related quality of life (HRQoL) is linked to COPD outcomes 11 which may mean that an improvement in HRQoL could lead to improvements in other COPD-related measures. Mindfulness practice is an intervention that has been shown to reduce symptoms of chronic disease and to improve accurate symptom assessment, both of which could result in improved disease management and increased wellness for people with COPD. 12 Wellness is a measure of physical, psychological and spiritual wellbeing that may provide a concealed picture of health status and may help in understanding all the factors responsible for supporting and improving health status. 13 For this reason, it seemed worthwhile to assess the psychological status and wellbeing of individuals with COPD.
Therefore, an assessment of wellness in patients with COPD potentially enhances disease outcomes and this study has tried to explore this phenomenon in the study participants. To date, no study has examined how wellness status can be assessed in patients with COPD or whether wellness is related to health measures in a COPD population. Thus, the purpose of this research was to design a questionnaire suitable for assessing wellness in persons with COPD and to determine any association of wellness with other COPD outcome measures.
Methods
An initial objective was to design a suitable wellness questionnaire; the second objective was the identification and selection of patients with COPD to engage with the questionnaire in a pilot study. To fulfil the first objective, several existing wellness questionnaires were critically reviewed to identify generally accepted wellness-related domains, then the most suitable questions used to assess wellness and from these a draft questionnaire was designed. The feasibility and acceptability of questionnaires to assess several different wellness measures for patients with COPD was investigated using focus groups.
After getting approval from the Ethics Committee of Sunderland University, three community focus groups from Age Concern and Breathe Easy in both Sunderland and South Tyneside were approached to ascertain views about the concept of wellness and the questionnaire itself.
Following further ethical approval by the NHS (National Health Services), LREC (Local research ethical committee) and the University of Sunderland Ethical Committee, the questionnaires produced after consultation with the community focus groups were sent to COPD study participants by post, together with a prepaid addressed envelope, an explanatory letter, a consent form to confirm the voluntary nature of participation in the study, an information sheet about how to complete the questionnaire and contact details in case there were any concerns to discuss. If necessary, a home visit or hospital appointment would be made at the patient’s request.
The discussion was started with a question to seek participants’ views on how to assess wellness status as opposed to health status. Of importance was the ease of comprehension and the likely relevance of questions to the target population of patients with COPD with mild, moderate and severe manifestations of the disease. Following feedback from the focus groups, the questionnaire was modified and finalized (Figure 1).
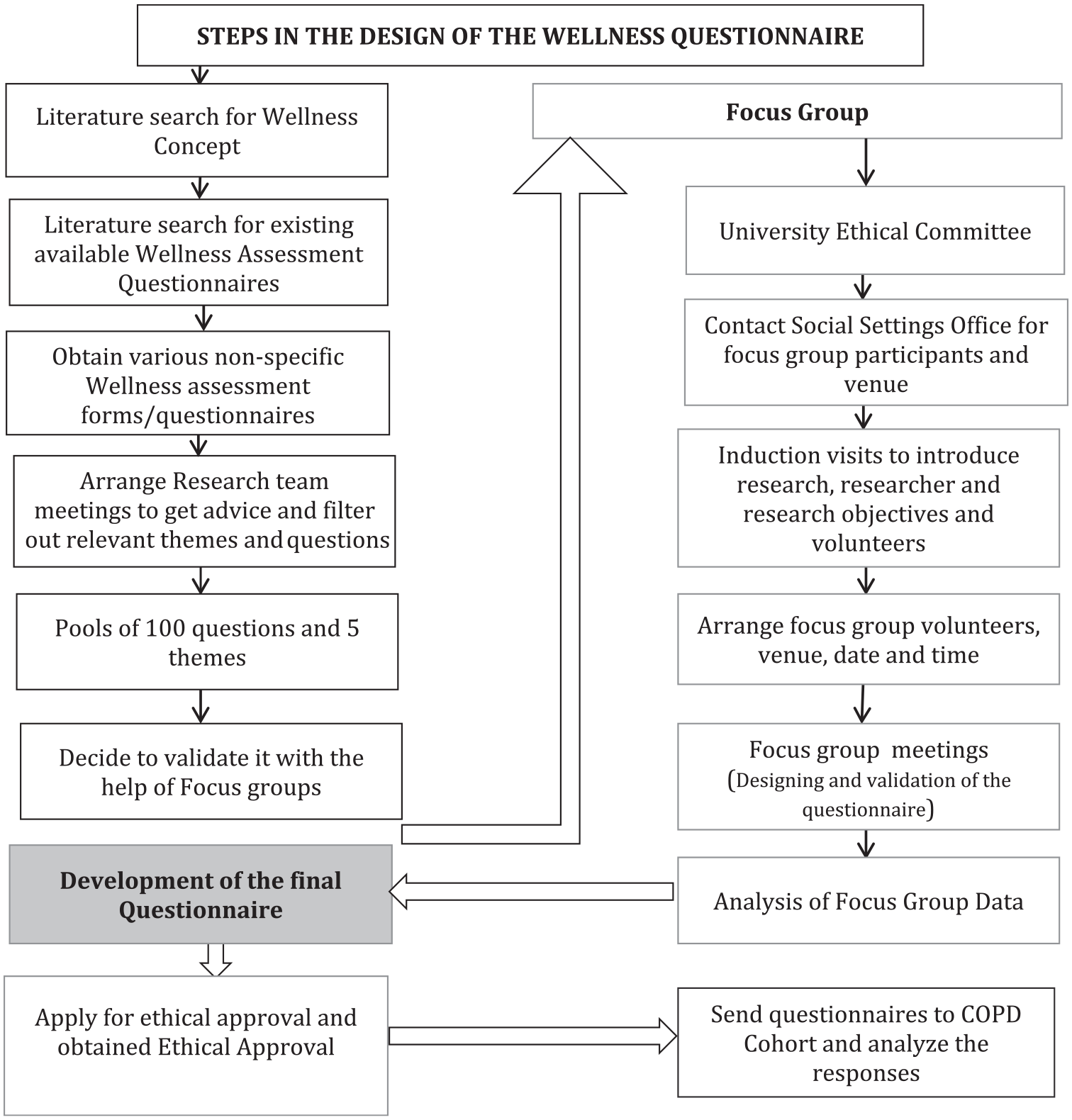
Schematic representation of the steps taken to design a wellness questionnaire suitable for study participants.
Analysis of focus group findings was carried out using (a) audio transcripts, (2) handwritten notes by the researcher and (3) thematic analysis.
All quantitative data were assessed using SPSS (IBM version 22, Inc. UK). Baseline measures were evaluated using Student’s t-test for differences between groups. Pearson product moment correlation coefficient (Pearson’s r) was used to analyse the correlation between wellness domains and COPD outcomes including lung functions as measured by FEV1% predicted, degree of breathlessness by Medical Research Council (MRC) dyspnoea score, severity of COPD by modified Gold staging and HRQoL by St. George’s Respiratory Questionnaire (SGRQ) scores. p value of ⩽.05 was considered as statistically significant.
Results
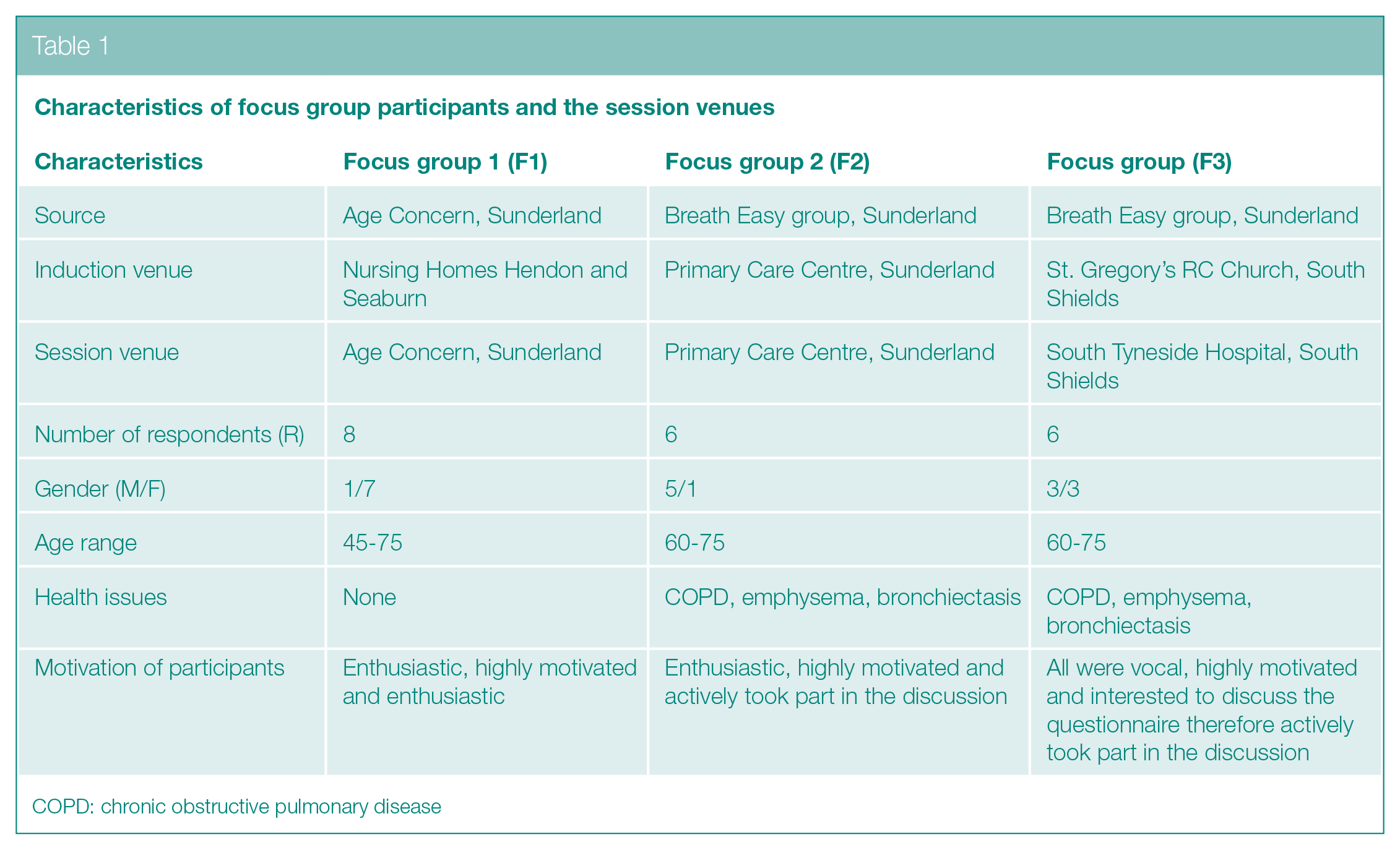
All participants were divided into three focus groups (F1, F2, F3) on the basis of induction and session venues. Number of participants in group F1 were 8, 6 in group F2 and 6 in group F3. Several emergent themes were explored. There were no set criteria for inclusion or exclusion of participants. Researchers ensured inclusion of participants who were demographically similar to those with COPD and in good health. Figure 2 represents the steps of focus group analysis.
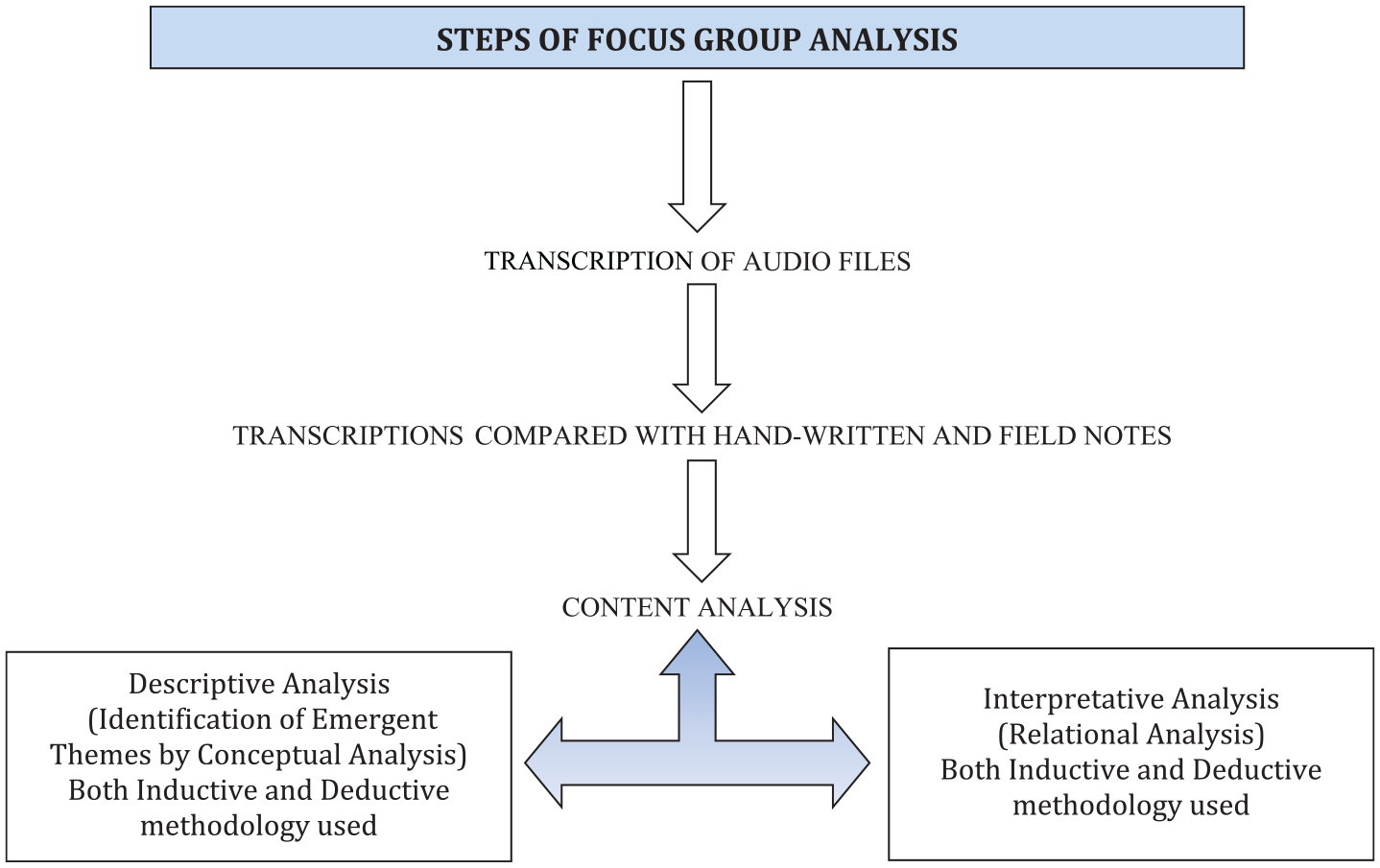
Stages of focus group analysis.
The demographic characteristics of the participants of focus groups F1, F2 and F3 are presented in Table 1. The participants in all focus groups were Caucasian. Figure 3 is a bar chart representing the frequency of different words that the participants used in relation to wellness assessment markers during the focus group sessions. Table 2 shows the key words used by the participants during all focus group discussions.
Characteristics of focus group participants and the session venues
COPD: chronic obstructive pulmonary disease
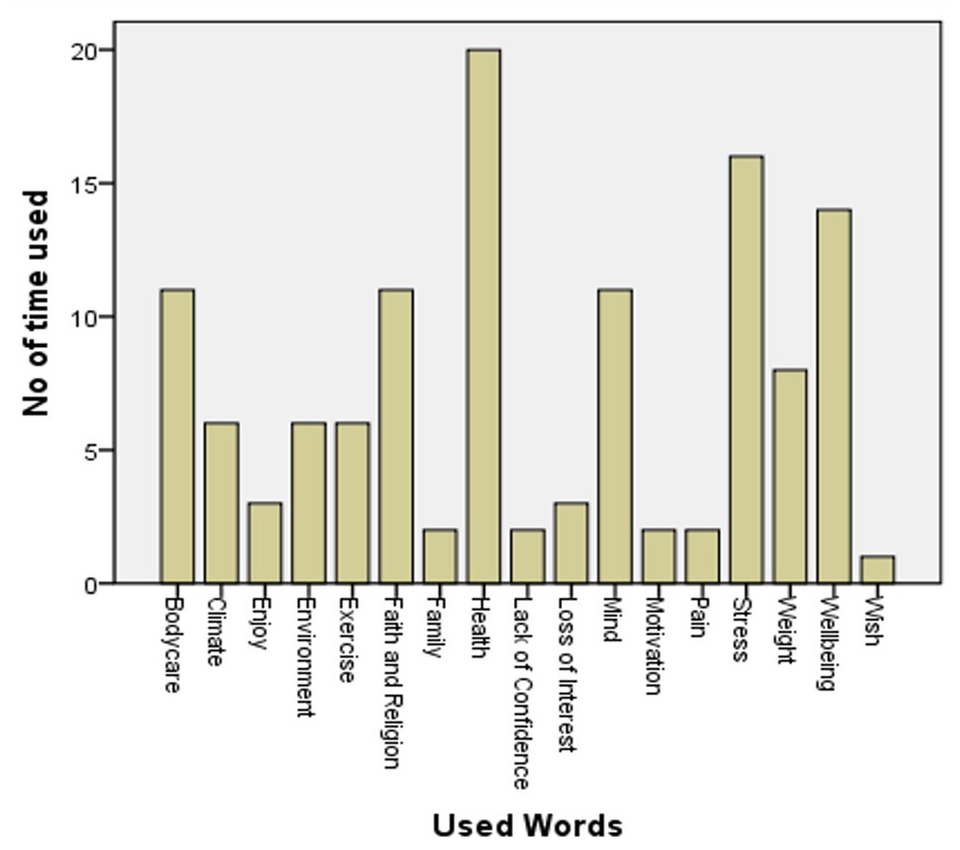
Frequency of different words that the participants used.
Themes generated from focus group sessions
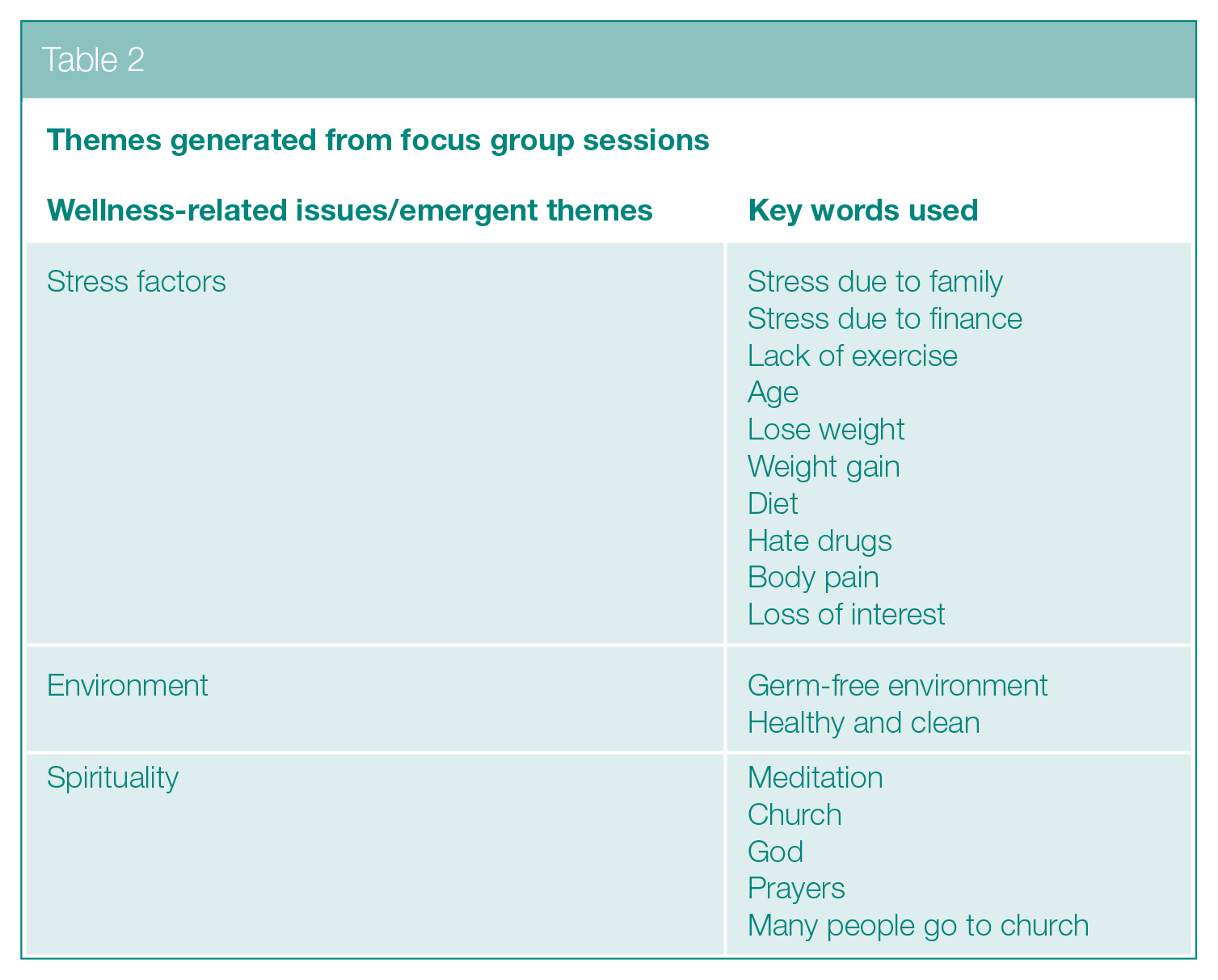
Different sources of stresses that occupied the minds of participants that were believed to interfere with health were mentioned, although there was no specific reference to symptoms or consequences of disease.
After critical analysis of the literature, a questionnaire was initially derived consisting of five potential themes/domains that are appropriate to assess wellness status in patients with COPD. These were Personal, Self-Responsibility, Daily Stress, Stress Management and Physical Wellness.
The focus groups also gave views on other aspects of the questionnaire. These include the question content and wording, response format, question sequence and questionnaire layout. A consensus was found regarding different aspects of the questionnaire across focus group members suggesting the questionnaire to have been well structured, easy to understand and to cover a range of health and wellbeing-related issues.
Validation of wellness questionnaire in COPD cohort
The health characteristics of the participants are shown in Table 3. Results show that respondents of the wellness questionnaire had severe manifestation of their clinical condition as indicated by their FEV1% predicted of 45.4 ± 19.2 with mean MRC score of 3, but better health status with total SGRQ score of 44.1 ± 19.6.
Health characteristics of the COPD respondents (n = 27)
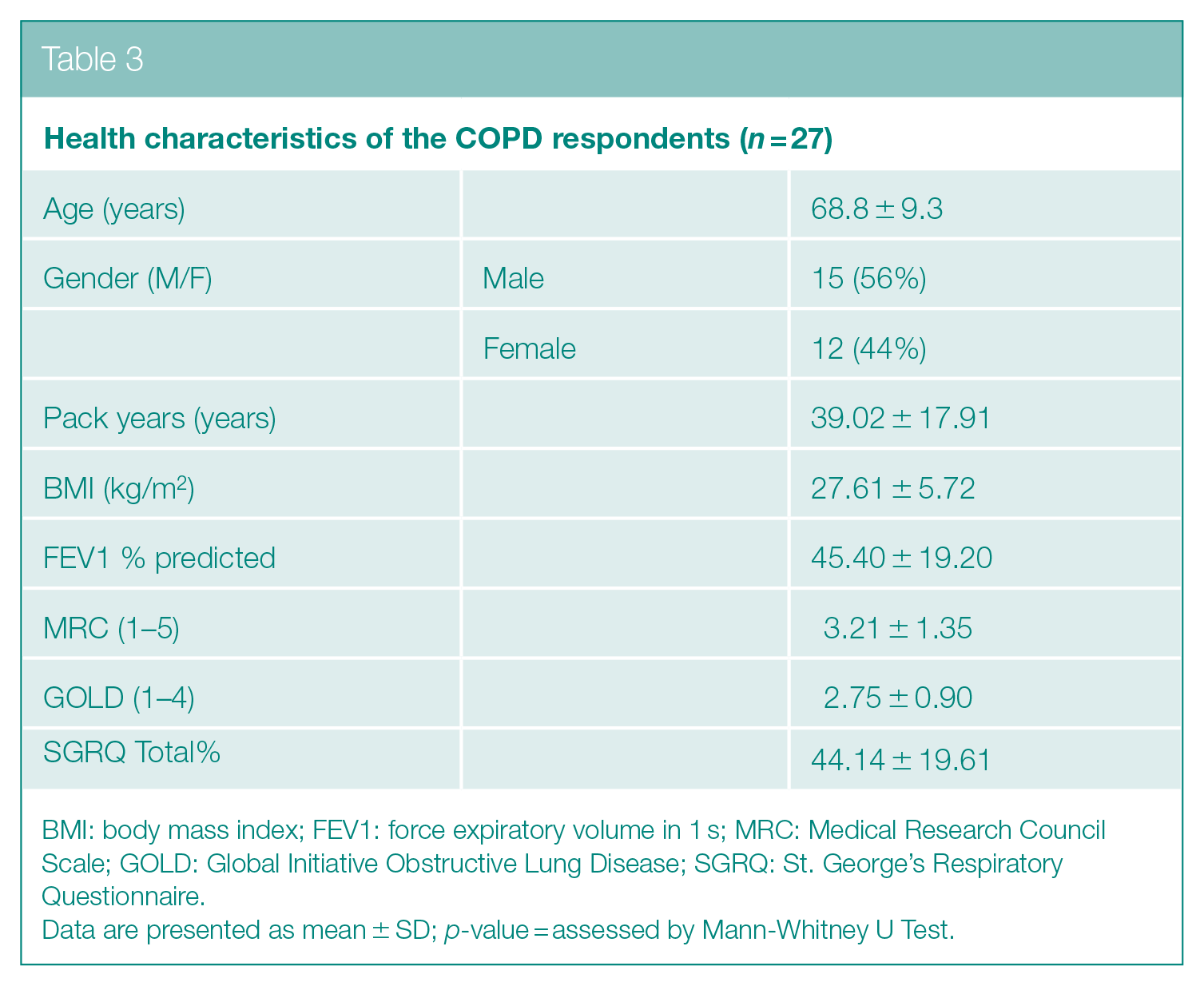
BMI: body mass index; FEV1: force expiratory volume in 1 s; MRC: Medical Research Council Scale; GOLD: Global Initiative Obstructive Lung Disease; SGRQ: St. George’s Respiratory Questionnaire.
Data are presented as mean ± SD; p-value = assessed by Mann-Whitney U Test.
The final questionnaire was given to the participants and the cohort was asked to mark whether the statement applied to them rarely, sometimes, most of the time or always.
Quantitative analysis (Table 4) using Spearman correlation indicated that significant correlations were found between Physical/Personal Wellness and other markers of COPD progression such as GOLD (0.006), FEV1% (0.01), HRQoL (0.009), multidimensional BOD (
Relationship of wellness domains with COPD markers
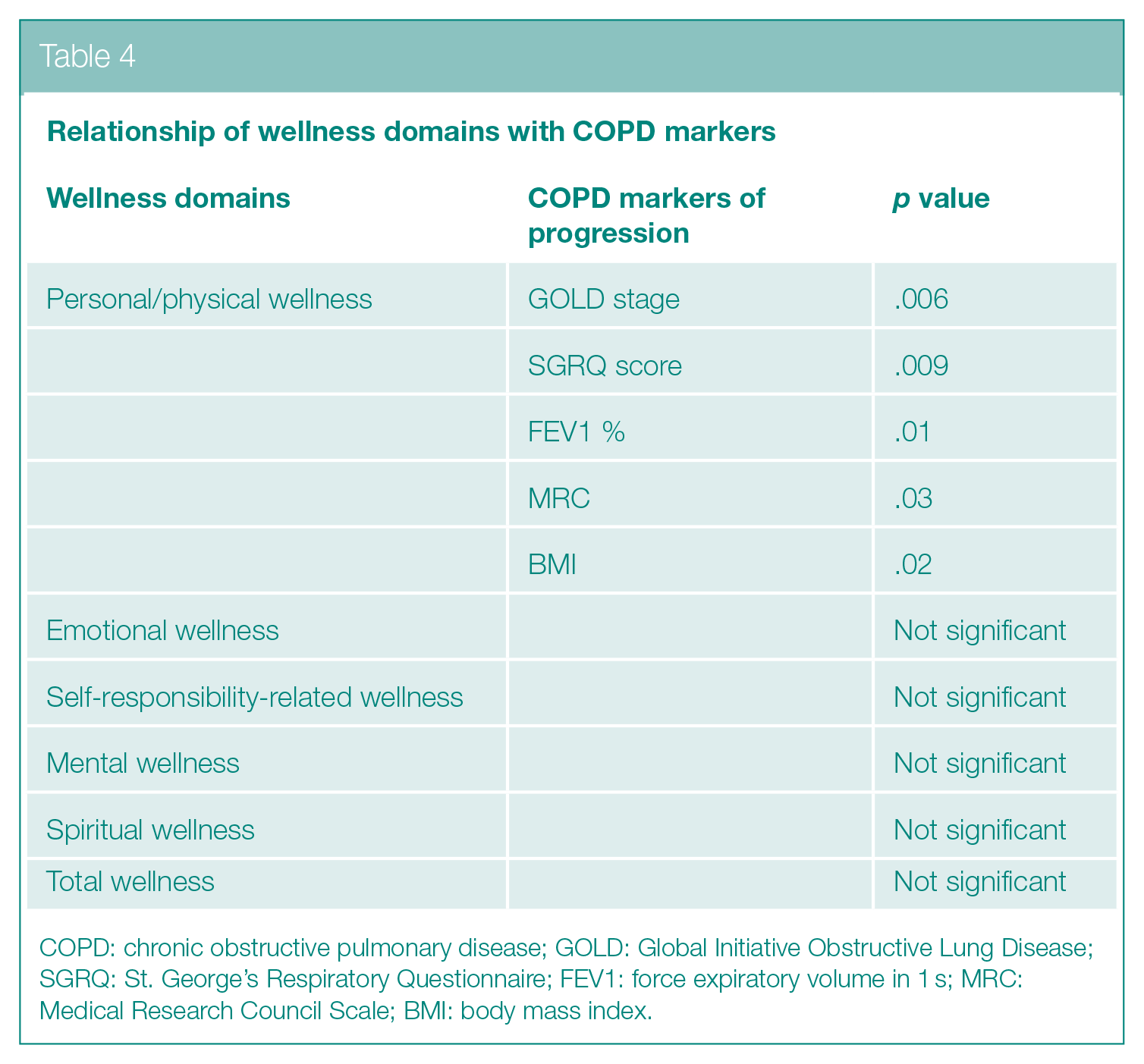
COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative Obstructive Lung Disease; SGRQ: St. George’s Respiratory Questionnaire; FEV1: force expiratory volume in 1 s; MRC: Medical Research Council Scale; BMI: body mass index.
Concept of wellness and the need to assess wellness
When asked to explain wellness in one phrase, focus group participants used different terms such as ‘interesting term’, ‘psychological picture’, ‘pain free body is wellness’ and ‘more good health than a basic mind’. An attempt was made to combine all of these terms to form an opinion-based definition of wellness:
A psychological state with peace of mind and a pain free state of a body in addition to good physical health.
Focus group members perceived that each dimension of wellness has to work in harmony with the others for optimal health and wellness to be achieved. The focus group participants provided insight during the sessions into previously unidentified wellness domains that eventually helped to improve accuracy and design of the developed questionnaire. When asked if they were sure they really understood the concept of wellness, all the focus group participants nodded in agreement. It was apparent that they were aware of the term ‘Wellness’ as they used phrases such as ‘oh definitely’ and ‘interesting term but not a common one’ …
Themes emerging from focus group sessions
Stress
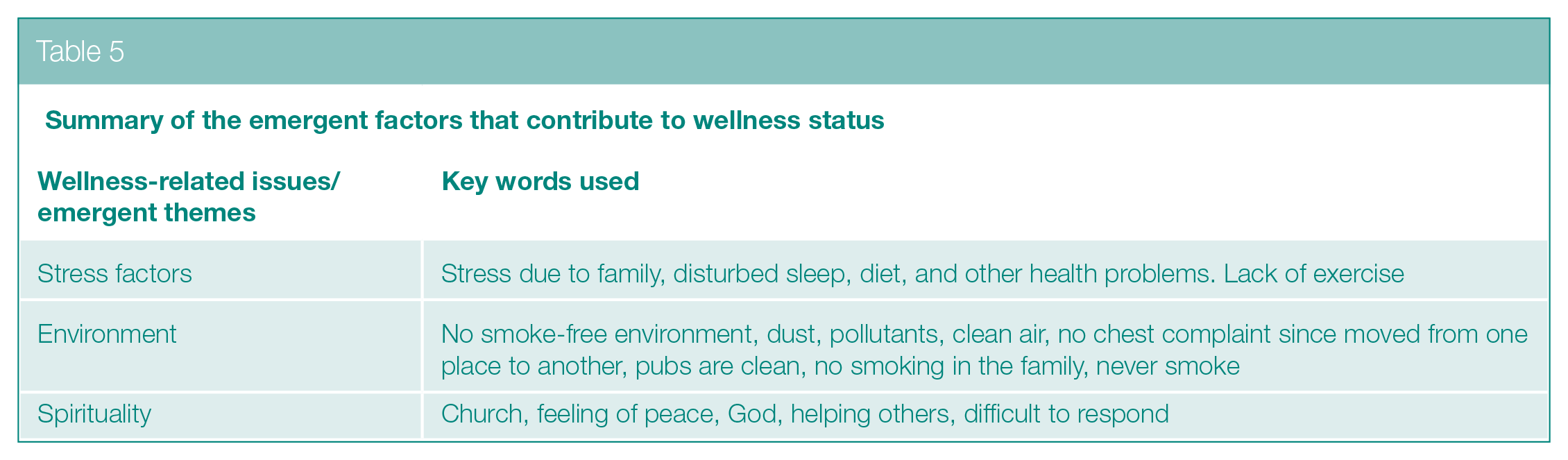
On the basis of focus group responses, members experienced different forms of stress as shown in Table 5. All of these appeared to play a major role in overall health and wellbeing.
Summary of the emergent factors that contribute to wellness status
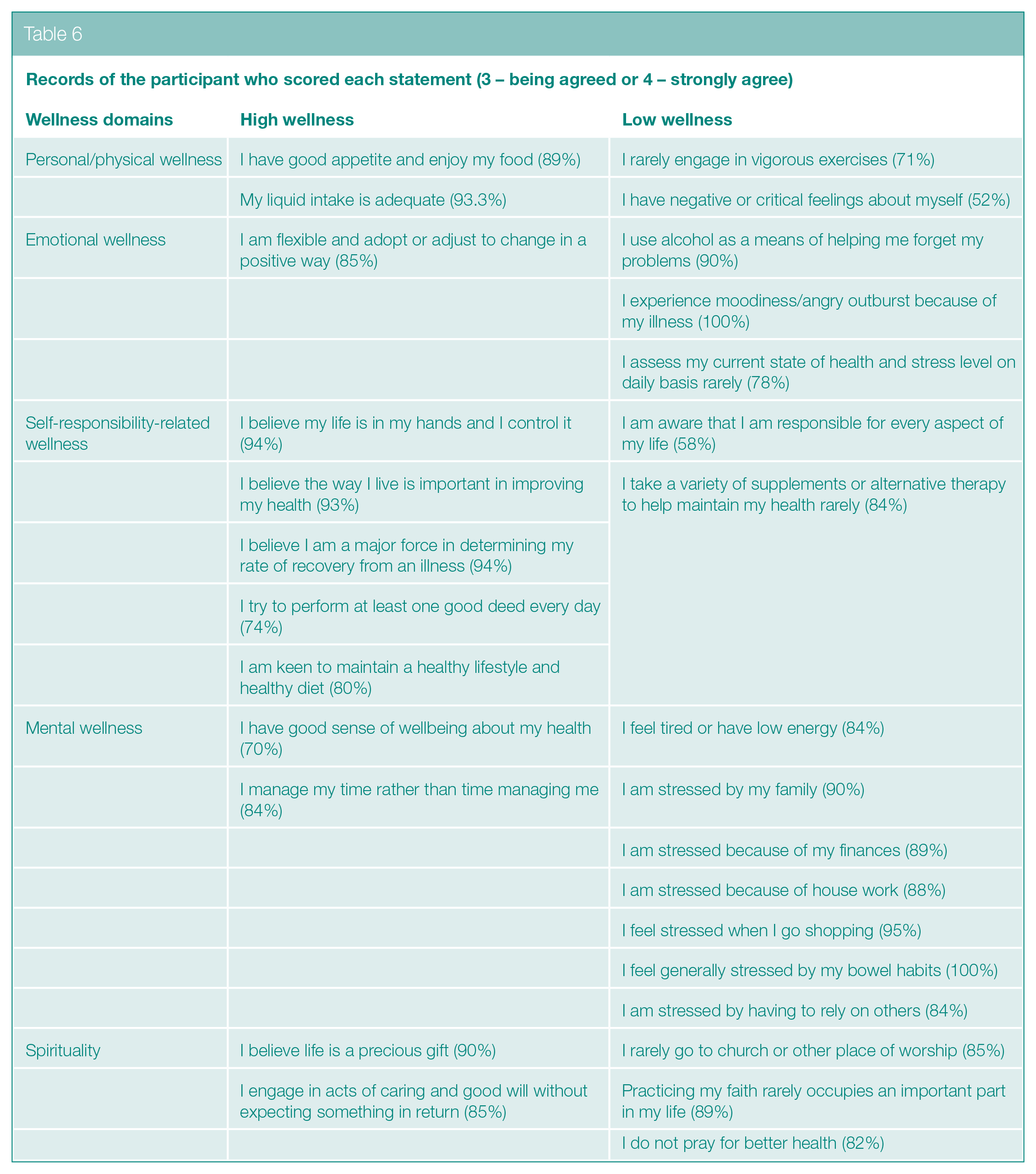
The % a person agreed with each of five options for each statement of each domain (5 domains; 10 statements in each domain; 50 statements in total). The responses with a high level of agreement were found and are presented as percentages in Table 6. The responses were presented in the form of percentages. Table 6 indicates that majority of COPD subjects showed bipolar variation in their responses to the wellness questionnaire which means they either marked the first two options of the Likert-type scale (rarely or sometimes) or the last two options (most of the time/always) in response to a written statement of the questionnaire that was somehow applicable to the patient’s condition. For example, all patients responded as either ‘most of the time’ or ‘Always’ against the statement ‘I experience moodiness/angry outbursts because of my illness’.
Records of the participant who scored each statement (3 – being agreed or 4 – strongly agree)
Spirituality
Spirituality was a theme that emerged in the first focus group discussion. It had not initially been included in a first draft of the questionnaire as the literature did not indicate that this was a component of wellness or health. However, when the group was asked if there was any other issue that could be incorporated in the questionnaire to assess wellness, three female members of the group initiated a discussion about whether spirituality could be considered as a wellness indicator and this idea was supported by other members. None of the participants in both focus groups objected to the inclusion of the spirituality section in the wellness assessment.
The qualitative analysis of wellness status in patients with COPD showed that the spiritual section of wellness status was of interest to the respondents, with comments such as the following being made:
Going to church gives me feeling of peace
God is not a whim.
However, one participant ‘found the spirituality section very difficult’.
As a result of such statements, the questionnaire was revised to incorporate the potential importance of exploring the influence of spirituality on disease management.
Discussion
Wellness is usually defined as being in a state of good physical and mental health and appears to be understood differently depending on the circumstances and lifestyle-related problems that an individual face. Each person’s definition of wellness will largely depend on how they perceive, assess and manage their needs and life circumstance or events. In this study, opinion-based definition of wellness was derived from focus group discussions. This was followed by the development and validation of a new questionnaire; the Sunderland Respiratory Wellness Questionnaire (SRWQ), believed to be the first questionnaire to assess wellness in patients with COPD.
Focus group discussions led to the development of the following definition of wellness: ‘A psychological state with peace of mind and a pain free state of a body in addition to good physical health’. This is consistent with the definition ‘A multidimensional state of being describing the existence of positive health in an individual as exemplified by quality of life and a sense of well-being’. 14
This study showed that, in some circumstances, attempts made to minimize stress formed the precipitating or aggravating stress factor. It therefore seems possible that, by assessing the influence of patients’ wellbeing on COPD outcomes, carers and healthcare professionals may be helped to plan better strategies and to find better solutions to problems in the future.
Because of the interest in spirituality and wellness shown in this study, further research is needed to explore possible links between spirituality and COPD outcomes. Many feel that good health is the just reward of living a good life, and illness is the punishment for one’s spiritual shortcomings. This view has been around since mankind has sought the answers to why some become ill or suffer misfortune. It is possible that the terminal nature of COPD makes some sufferers more spiritually conscious. Alternatively, it is possible that the participants were more spiritually aware than the population at large. As some members of the focus group belonged to a Christian Church group, it is possible that this led to a concern about spirituality, which then became incorporated into the questionnaire. It is therefore possible that any link demonstrated between spiritual status and health/wellbeing is restricted to those who already have a faith.15,16
To date, the majority of indices developed for the evaluation of COPD have concentrated on physical, physiological and biochemical measures. 17 However, a person’s attitude towards their illness can often impact upon the outcome in terms of morbidity and mortality. Also, in any evaluation of disease progression, it may therefore be necessary to include an assessment index measure of ‘wellness’ or their mental attitude towards their illness.18,19
This study also attempted to explore the deeper picture of the overall health status in these patients with the help of a newly developed ‘Sunderland Respiratory Wellness Questionnaire’. This suggests the need for its use in patients with COPD to get a deeper picture of the overall health and potential impact on outcome, better management and prognosis. In addition, the psychological/wellness status enhances the assessment of overall health status incorporating general, physical and mental health status, which together improves overall health outcomes.
The key factors that the patients felt impacted upon their wellness include stress factors, self-care and spirituality.
From the analysis of focus groups, written comments from patients with COPD and responses in the wellness questionnaire, a variety of stress factors have been identified as markers that influence COPD outcomes. These include self-induced stress, nutritional stress, physical, emotional, spiritual, mental and environmental stress.
In addition to stress factors, the qualitative study has also identified other factors that may further impact upon health and general wellbeing in patients with COPD. These include hope and positive attitude, self-care and personal beliefs.
All these factors could be useful and while they do not need new treatment interventions, they require support from family, friends, relatives, healthcare workers and society. In this regard, the most vital need is to determine a patient’s requirements, needs, views and resources that collectively help these patients to be well informed. This in turn can motivate patients and keep their attitude positive towards the maintenance of good health.
For example, when a patient is under stress, they tend to ignore healthy/regular meals and thus may create further stress in the long run. Therefore, extra support may be needed to make food choices. Furthermore, having COPD may cause a gradual variation and deterioration not only in their lifestyle but also in their relationship with family members, relatives, spouse, siblings and friends. It is believed that by sharing their feelings and concerns, perception of their illness may be improved resulting in the positive energy needed to overcome disease consequences. In addition, the assessment of wellness may also enhance the assessment of health status in these patients which in turn can lead to an improvement in their quality of life.
Therefore, the management of COPD should be carried out on an individual basis considering personal and social factors that interfere with the progression of this disease. How the healthcare workers approach these individuals is also an important factor that needs consideration. For example, general instruction to ‘stop smoking’ is the key target by clinicians to improve COPD-related health outcomes. However, attention should also be given on the contributing factors that prevent them from stopping smoking, for example, health-related stress factors, social factors or attitude.
This study has combined quantitative and qualitative research in the development of new methods for the evaluation of patients with COPD and management of their care. While further research is needed to validate this new questionnaire, initial study results provide a starting point which will enable healthcare practitioners to evaluate the wellness of individual patients and to devise appropriate care packages that not only manage their physical symptoms but also support their ‘wellness’.
Combining qualitative and quantitative measures
Many studies into the development of indices of COPD progression have solely focused on physical measures.20,21 Few have attempted to assess mental status and its association with COPD progression22,23 and health status. 24 However, to date, no study brings together an assessment of a patient’s physical symptoms and a measure of their mental attitude (and the factors that impact upon it) so that both aspects can be considered in the long-term management of the illness. This study explores this phenomenon for the first time.
In all evaluations of disease progression, there is a need to evaluate both physical factors together with ‘wellness’ and attitude. Management of health and the outcome of disease are a mixture of both, and a multidisciplinary index should assess both measures. This means a blending of quantitative and qualitative methods. In practice, this does not generally occur as studies are either carried out by physicians/clinicians or social scientists.
This study benefitted from support from both types of expertise and it has illustrated the need to merge both types of research in the development of future indices for the management of COPD.
Conclusion
This study needs to be considered as a unique addition to the literature with respect to the identification of new markers of wellness status for the improvement in overall health and wellbeing in these patients. This could guide physicians to identify areas for self-care and help them to promote a self-management approach to managing COPD. The findings suggest that the combination of personal, physical, emotional, mental and other psychological factors is responsible for negative COPD outcomes which further deteriorates its progression. Further research is needed to assess the utilization of this tool in a large group of patients with a range of disease severity. There is a need to further validate the Wellness questionnaire, its reproducibility and its correlation with other tools that are being utilized to assess health status and to explore wellness as a concept in other patients with COPD from other ethnic groups.
Future research should focus on how self-management skills can be incorporated formally into medical care. In addition to offering suggestions on how clinicians may be instrumental in improving self-management behaviour in patients with COPD, and thereby improve care outcomes, we highlight the importance of gaining insight into the perceptions of patients of their own situation and incorporating a respect for patient perspectives into the philosophy of care.
Footnotes
Acknowledgements
We thank the General Practitioners and hospital staff in the Chest Clinic, Sunderland Royal Hospital for giving us the opportunity to recruit patients in order to conduct this study.
Author Contributions
All authors have contributed to writing and revising the manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by Sunderland Hospital Research Grant from the Department of Research and Development.
Informed Consent
The study protocol (08/Q0904/43), including its consent form and survey template, was reviewed through Local Research Ethics Committees, University of Sunderland and Sunderland Royal Hospital. The IRB granted a Waiver of Written Documentation of Consent on the grounds that this study is a postal survey that does not include direct identifiers, there are no physical risks imposed by this study, does not involve procedures for which written document of consent process is normally required outside of the research context and the research is not FDA regulated.