
Abstract

In this article, Guest Editor for this special issue Helen Johnston and co-authors look into strategies to improve air quality, and the role of local groups and authorities in tackling health inequalities.
Poor air quality is the leading environmental risk for population health in the UK. 1 Public health professionals are seen to have a vital role in assessing and communicating the health impacts of air pollution, and informing local responses and decision-making to improve air quality in the UK.2,3
A focus on air pollution is timely: the environmental and health impacts of the wide-scale reduction in travel associated with COVID-19 restrictions have been rapidly assessed, 4 with a measurable, although modest, improvement on air quality during the most stringent restrictions in the UK in 2020. 5 Moreover, an analysis of UK Biobank data showed that regional air pollution patterned with COVID-19 mortality, indicating that long-term exposure to poor air quality increased the risks of COVID-19 infection. 6 With the knowledge that poor air quality is also correlated with areas of lower socio-economic status, this provides a salient reminder of the inequity in exposure to air pollution and its associated health harms. 7
Yet public health leaders may not be front and centre of the local discourse on air quality. Air pollution is not consistently equated with its health consequences: the statutory Local Air Quality Management approach focuses solely on environmental outcomes, and policy objectives such as clean air zones are predominantly designed and assessed using environmental metrics. Further there isn’t widespread clamour from the wider health system for change: healthcare professionals in the UK tend to underestimate the presence and urgency of air pollution. 8
Additionally, the capacity and knowledge of the public health workforce may be limiting factors; there are complex technical details across the various ambient air pollutants, their measurement and the design of appropriate interventions. Tackling air pollution will require multidisciplinary collaboration: the public health skills that seem particularly pertinent are the ability to understand and apply data and intelligence, integrate workstreams, engage communities, and to provide a narrative that frames the issues in a manner that resonates with partners and stakeholders. A survey in 2015 found that air quality professionals reported that they expected to work increasingly closely with public health colleagues in the future. 9

One of the strengths of public health specialists is their recognition of the interaction of risks and impacts across communities and populations. In Wales, a public health-driven approach to risk assessment has been demonstrated, which highlights the triple jeopardy effect of overlapping poor health, deprivation and air pollution. 10 This broad perspective to improving health provides the ability to flex across different prevailing priorities and campaigns. The emphasis on ‘net zero’ has raised the profile of carbon neutral programmes that will have many shared benefits for air quality and these synergies should be celebrated. Alongside this, there is still a need to draw attention to the deleterious health effects of particulate matter, sulphur dioxide, nitrogen oxides and the other air pollutants.
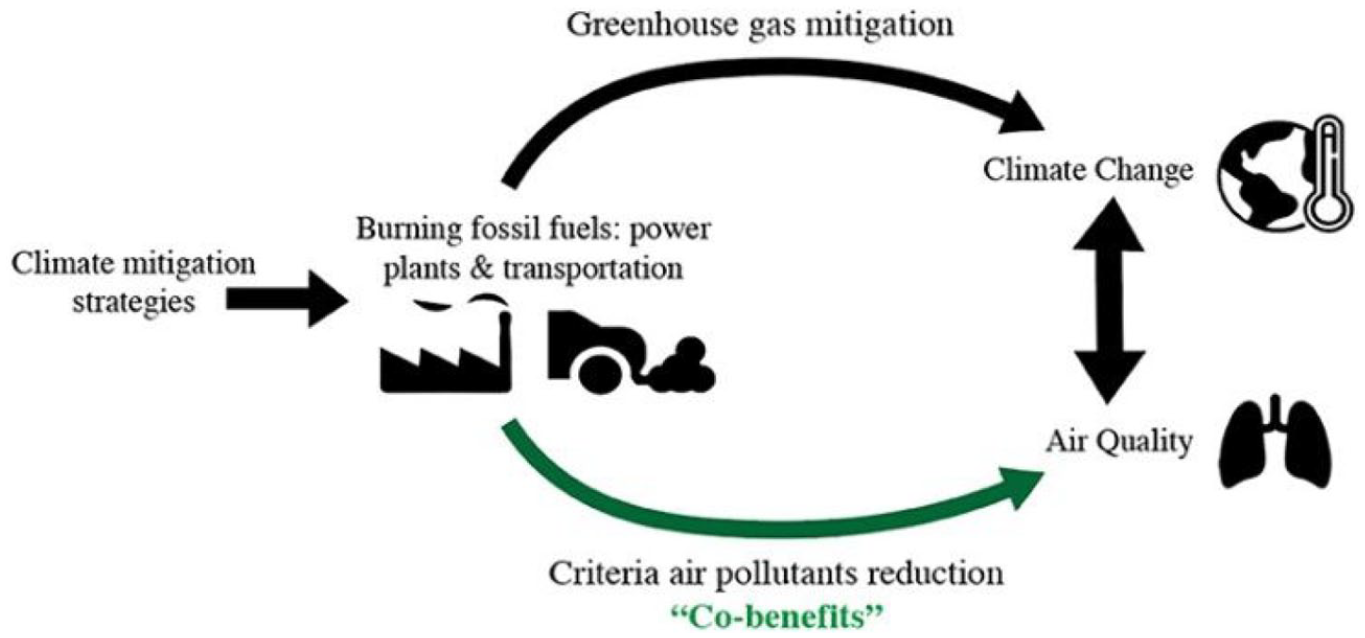
Schematic from Gallagher and Holloway 2020: integrating air quality and PH benefits in US decarbonisation strategies. 11
Effective strategies to improve air quality will consider the sources of air pollution in a locality and will necessarily range across industry, agriculture, transport and planning stakeholders. Finding the commonalities and bringing disparate groups together around shared goals is crucial to achieve a measurable impact. An example is having a shared principle of a ‘net health gain’ for new developments to deliver an overall benefit to population health, with comprehensive design to improve air quality. 7 Health impact assessment methodology provides a useful tool to inform decision-making on air quality measures. 9
A complementary approach to the focus on air quality are the strategies that start from a cause of ill health, such as low levels of walking and cycling. Through effective interventions, the potential for health improvement extends across a range of outcomes including physical activity and mental wellbeing as well as reduced private vehicle transport. Similarly, road safety interventions are a means of leveraging multiple gains for health, including for air quality when sufficient attention is given to unintended consequences such as particulate emissions from vehicle brakes. One advantage of the risk factor strategies is that they can feel more tangible and more easily understand by the public, akin to the Victorian appreciation of the social and health value of building and maintaining public parks.
Effecting change in complex systems often requires multiple points of intervention, particularly as public health teams rarely bring financial resource or managerial power to the table. A qualitative exploration with local authority staff in the South West of England proposed that sector-led improvement activities may be one means of improving work to tackle the health impacts of climate change. 12 In the East Midlands, Public Health England chaired and provided secretarial support to a regional Air Quality Network prior to COVID-19 pressures.
The public health perspective is essential in ensuring that due attention is given to vulnerable groups across the population who bear more of the burden of ill health associated with poor air quality. Reducing inequalities takes concerted effort: the modelling of air quality outcomes associated with pursuing emissions goals for the UK identifies higher exposure to air pollutants in socioeconomically deprived populations compared to more affluent populations in 2050. 13 And few academic studies have examined implications of air quality strategies for health equity. 14 An ongoing challenge for practitioners is to articulate the necessity of upstream mitigating action and to resist an overreliance on adaptation strategies such as text alerts for poor air quality.
In 2014, a group of public health colleagues described a paradigm that the role of public health ranges across leadership, partnership and advocacy approaches, and contended that a shift from advocacy into a more involved partnership mode strengthened the impact of work to reduce inequalities. 15 In a similar vein, public health professionals can tend towards an advocacy position on climate change in holding knowledge but not wielding control over the resources and initiatives. This overlooks our holism. As part of our commitment to reducing inequalities, public health professionals should be involved as key partners in local air quality work and offering their broad perspectives, emphasising the shared gains that can be achieved through collaboration.
We propose several recommendations to address the issues raised here and to galvanise public health partnerships for improving air quality:
Increase awareness of the burden that poor air quality places on health services across health system partners.
Build the capacity and knowledge base, including shared learning between public health and air quality professionals, to enable multidisciplinary working.
Ensure health metrics are built into policy objectives around air quality.
Utilise tools such as health impact assessment to inform decision-making on issues that could impact on air quality.