
Abstract
Introduction
It is increasingly clear that inequalities in socio-economic status (SES) contribute to, but do not fully explain, ethnic inequalities in health. 1 Emphasis on cultural and genetic explanations has shifted to a focus on systemic causes, drawing upon systemic racism 2 – policies and processes embedded in society which disadvantage ethnic minorities – to better understand persistent ethnic inequalities in health. Two mechanisms have been proposed. First, racism is a fundamental cause of differences in SES which itself drives inequalities in health outcomes. 1 Second, racial discrimination is directly associated with health, independent of SES, through inequalities in power, freedom, neighbourhood context and health care provision and access. 3
Previous studies in the United Kingdom have identified racial discrimination in the workplace and higher poverty among minority ethnic groups as potential instigators of the observed levels of financial discrimination. 4 US evidence indicates a role for racial discrimination in persistent inequalities in food insecurity, 5 a rapidly escalating UK public health crisis and one with clear racial disparities. 6 In 2022 to 2023, 10% of households in the United Kingdom were food insecure, with either low (5%) or very low household food security (5%) and 7% experienced marginal food insecurity. Food insecurity was highest in households where the head of the household was Arab (23%), Black, African, Caribbean and Black British (21%), Mixed and Multiple Ethnic Groups (16%) and Pakistani (15%) and lowest where the head of the household was White (7%), Indian (5%) or Chinese (3%). 6 Nevertheless, the relationship between food insecurity and racial discrimination has not been explored in the United Kingdom. In this exploratory study, we examined the relationship between sociodemographic and SES factors, including financial and food insecurity, with reports of discrimination.
Materials and Methods
We used cross-sectional data taken from questionnaires that were administered to adults in the Born in Bradford cohort in Autumn 2020 as part of a study exploring the impact of COVID-19 on families. 7 The data collection received ethical approval from the Health Research Authority and Bradford/Leeds research ethics committee (BiB Growing Up study 16/YH/0320; BiBBS study 15/YH/0455; BiB4All study 17/YH/0202). All participants provided informed consent to participate in the survey. 7 The survey was completed via post or online and contained questions on participant demographics, health, wellbeing and SES factors. We asked ‘How often do you personally feel discriminated against because of your race?’. With options ‘Don’t know’, ‘Never’, ‘Rarely’, ‘Sometimes’, ‘Often’ and ‘Do not wish to answer’. ‘Yes’ was categorised as ‘sometimes’ plus ‘often’ and ‘no’ was comprised of ‘Don’t know’, ‘Never’, ‘Rarely’ and ‘Do not wish to answer’ categories. Financial insecurity was established by asking ‘How well would you say you are managing financially right now?’. With options ‘Don’t know’, ‘Do not wish to answer’, ‘Living comfortably ‘, ‘Doing alright’, ‘Just about getting by’, ‘Finding it quite difficult’ and ‘Finding it very difficult’. We grouped into a binary category including ‘Just about getting by’, ‘Finding it quite difficult’ and ‘Finding it very difficult’ in the financially insecure group. Ethnicity was self-reported and taken from baseline data. 8 Education categories were self-reported and foreign-born qualifications were equivalised if possible. Deprivation, as measured by the Index of Multiple Deprivation (IMD) using deciles, was categorised to create two groups due to the skewed distribution of IMD in Bradford: IMD group 1 ‘most deprived’ and IMD groups 2-10 ‘all other’ groups. Five food insecurity questions were included ‘the food that (I/we) bought just didn’t last, and (I/we) didn’t have money to get more’, ‘Did you or other adults in your household ever cut the size of your meals’, ‘(I/we) couldn’t afford to eat balanced meals’, ‘Did you or other adults ever eat less than you felt you should because there was not enough food’, ‘Were you ever hungry but didn’t eat because there wasn’t enough money for food’. 9 People were categorised as food insecure if they had an affirmative response to any of the questions. Chi-square tests were used to test for differences between discrimination, food insecurity and financial insecurity. Multiple logistic regression was used to establish the odds of discrimination with SES factors.
Results
Questionnaires were completed by 587 women and 37 men. Almost a fifth (18.2%) felt discriminated against ‘Sometimes’ or ‘Often’ and 18.1% of respondents reported experiencing food insecurity. A higher proportion of those who experienced discrimination also experienced financial insecurity (25.6%), compared to those who did not experience financial insecurity (15.3%) (χ2 test p = 0.003). Discrimination was reported by 37.1% of respondents from the ‘Other’ ethnic group and 25.6% of South Asian respondents, compared to just 6.9% of White respondents (χ² test, p < 0.001).
In a multiple logistic regression analysis (see Table 1), we observed significant disparities in reported discrimination across ethnic groups compared to the White population. Respondents of South Asian origin were significantly more likely to report discrimination (odds ratio [OR]: 5.48; 95% confidence interval [CI]: 2.93–10.28), as were those in the ‘Other’ ethnic group category (OR: 9.59; 95% CI: 4.93–18.66).
Odds of reporting discrimination by demographic and SES factors
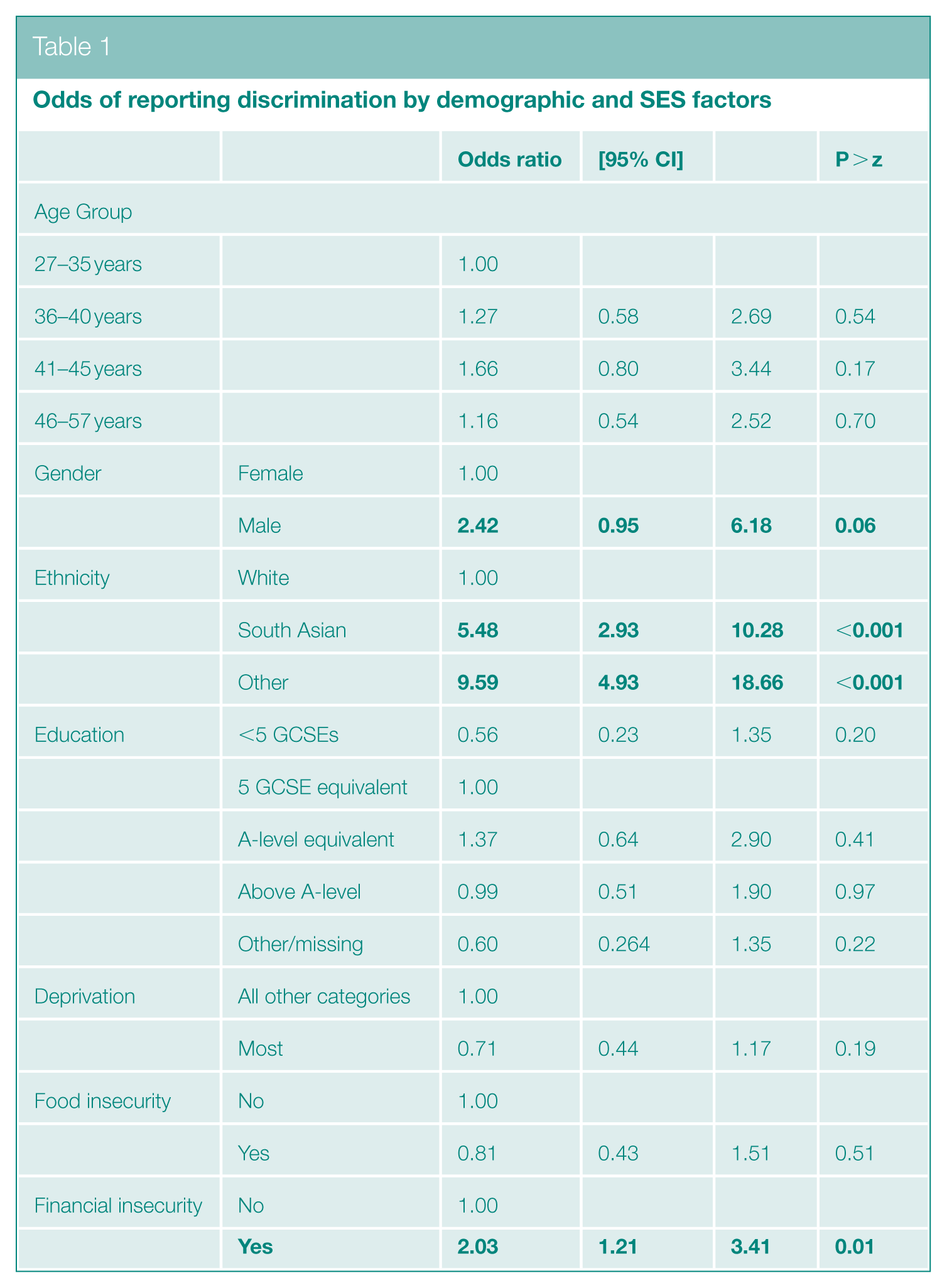
Financial insecurity was also associated with a higher likelihood of experiencing discrimination (OR: 2.03; 95% CI: 1.21–3.41), whereas no relationship was observed between food insecurity and discrimination. While trends were observed for other SES factors, the results were not statistically significant. Interestingly, individuals with the lowest educational qualifications were less likely to report discrimination compared to those with higher education levels. However, respondents with qualifications above A-level were less likely to report discrimination than those with A-levels, or equivalent, or five GCSEs, or equivalent. Similarly, individuals living in the most deprived IMD areas were less likely to report discrimination compared to those in the least deprived IMD areas.
Discussion
In this exploratory study using data collected during COVID-19, we found clear differences in reporting of racial discrimination, with people of South Asian and ‘Other’ ethnicity, in addition to people experiencing financial insecurity, being more likely to report experiencing discrimination. Contrary to US studies, 5 we did not find a significant relationship between food insecurity and discrimination.
Our study addresses racial discrimination in a small and demographically specific population, during the COVID-19 pandemic. While a rich sample, it is not necessarily representative of the United Kingdom. The small sample size, timing of data collection and the demographic context of the city, with a large South Asian population living predominantly in deprived city centre wards, could partly explain our finding of no relationship between food insecurity and discrimination, given the relatively low variation in these factors. The data in the study are cross-sectional, impeding insight into causality, and, like many indicators and particularly those that are subjective experiences, data on financial insecurity, food insecurity and discrimination are self-reported. Categorisation of ethnicity into three groups, as a consequence of sample size, precluded detailed exploration of differences between all ethnic groups. For instance, we identified low but present reporting of racial discrimination within the White group; the White group includes people from Central and Eastern Europe and the Roma community living in Bradford, and racism experienced by these groups is well documented. 10 Nevertheless, in the absence of evidence on food insecurity and racial discrimination in the United Kingdom, our exploratory study highlights the importance of considering discrimination in socio-economic inequalities in health and is intended to catalyse a broader conversation.
Footnotes
Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was funded by a Wellcome Trust Fellowship in Humanities and Social Sciences held by the first author (grant no.: 221021/Z/20/Z).
Ethical Considerations
We used cross-sectional data taken from questionnaires administered to adults in the Born in Bradford cohort in Autumn 2020. The survey data collection was approved by the Health Research Authority and Bradford/Leeds research ethics committee (BiB Growing Up study 16/YH/0320; BiBBS study 15/YH/0455; BiB4All study 17/YH/0202). All participants provided written informed consent to participate in the survey.