
Abstract
This short report examines the harmful health impacts of heatwaves in low- and middle-income countries across Sub-Saharan Africa (SSA) and underscores the urgent need to advance climate adaptation strategies in these vulnerable regions. Given the increasing frequency and severity of heatwaves due to climate change, the authors’ work highlights the gaps in current heat-health policies, the disproportionate burden on vulnerable populations, and the necessary steps for strengthening public health resilience in SSA.
Introduction
Heatwaves impact human health, contribute to fatalities, and increase pressure on healthcare systems, 1 particularly in low and middle-income countries (LMICs), which are less equipped to deal with the effects of heatwaves 2 and often lack Heat Health Plans (HHPs). In LMICs in sub-Saharan Africa (SSA), including Nigeria, heatwaves disproportionately affect already vulnerable populations, including older adults, young children, people with chronic conditions, outdoor and informal workers, and low-income households with limited access to cooling and access to healthcare. Urban settlers face intensified risks due to the urban heat island effect, while rural populations experience the combined stresses of heat, droughts, and isolation. Gender dynamics and the circumstances of displaced populations further compound vulnerability. 3
HHPs can prepare and protect people from heatwaves 4 and are in place in many high-income countries (e.g. UK), and a few LMICs (e.g. India). 5 SSA countries are most exposed and vulnerable to heatwaves but lack HHPs, 3 calling for urgent action for climate adaptation and cross-learning. 6 Here, we identify opportunities for HHPs in SSA, building on (1) a theoretical framework that emphasises the concept of Climate Determinants of Health, 7 (2) existing HHPs, and (3) current structures and programmes in Nigeria.
Lessons Learned
Heatwave hazards need to be assessed in conjunction with potential impacts, the characteristics of exposed subjects (humans, animals, plants, environmental systems, and services), their sensitivity, and adaptive capacity. Together, these determine vulnerabilities and risks. Dynamic heatwave maps that represent not only meteorological data but also hazard and sensitivity must incorporate data on climate-sensitive diseases and allocation of resources to ensure targeted, efficient, and equitable responses. 8

The UK’s Adverse Weather and Health Plan (AWHP) 9 coordinates responses and communication among government agencies to protect vulnerable populations, for example, those in care homes, 10 by promoting community engagement, integrating emergency responses, and public health frameworks. However, the AWHP lacks dedicated resources for reaching isolated populations, which can include the most disadvantaged, sensitive, and exposed communities. 11 Gaps also include long-term adaptation, such as urban planning. In India, the Ahmedabad HHP aimed to increase awareness about the impacts of heatwaves 12 and has been scaled up to other heatwave-prone states. 13 About 30% of these HHPs, however, remain poorly funded, and many are reactive rather than proactive, lacking vulnerability assessments. 14
Nigeria’S Heat-Health Challenges
Heatwaves in SSA, including Nigeria, are increasing in frequency, duration, and intensity, particularly in cities, 15 and could double or triple by 2050, with northern Nigeria most affected. 16 Nigeria has responded to emerging heatwave impacts with a National Adaptation Strategy and Plan of Action on Climate Change that highlights climate-related health risks. However, this response is largely reactive, with emergency measures implemented during heatwaves rather than including planning and preparation. 17
Several limitations hinder Nigeria’s ability to manage the impacts of heatwaves. First, the Nigerian health and social care systems face financial pressures, overcrowding, and insufficient capacity. 18 The private sector provides higher-quality health services, but is inaccessible to less wealthy populations.19,20 Second, there is a lack of data on health impacts of heatwaves. Third, communication strategies included in current HHPs are hampered by a lack of Internet access, defective infrastructure, and power outages, 21 compounded by high rates of urbanisation leading to increased demand. 22 Fourth, economic, environmental, and security concerns restrict Nigeria’s capacity to respond to heatwaves. Conflict and violence cause casualties, migration, and malnutrition, which can be worsened by heatwaves due to, for example, water scarcity, food insecurity, fires, disease, and isolation.23,24 Climate change is expected to exacerbate these issues, while HHPs can help mitigate them and respond to calls around the relevance of human rights in climate migration. 25
Recommendations For A Nigerian HHP
While Nigeria faces significant obstacles, we propose five areas towards pragmatically developing a Nigerian HHP, building on good practice, and leveraging current Nigerian structures.
Communication
Building on AWHP practice 9 and our own pilot study in Türkiye, demonstrating how early warning systems (EWS) can be adapted to local contexts to protect population health, 26 we propose EWS including social media campaigns, television and radio broadcasts, flyer distribution, engagement of town announcers and multilingual dissemination through marketplaces and religious institutions (Figure 1). Actions post-heatwave can include (1) reviewing emergency response performance to inform future preparedness; (2) launching public health campaigns to raise awareness about cumulative heat effects and adaptive behaviours; (3) planning health services considering Climate Determinants of Health and climate-related vulnerabilities; 7 (4) organising training programmes on health impact assessments; and (5) assessing and enhancing climate and health literacy.
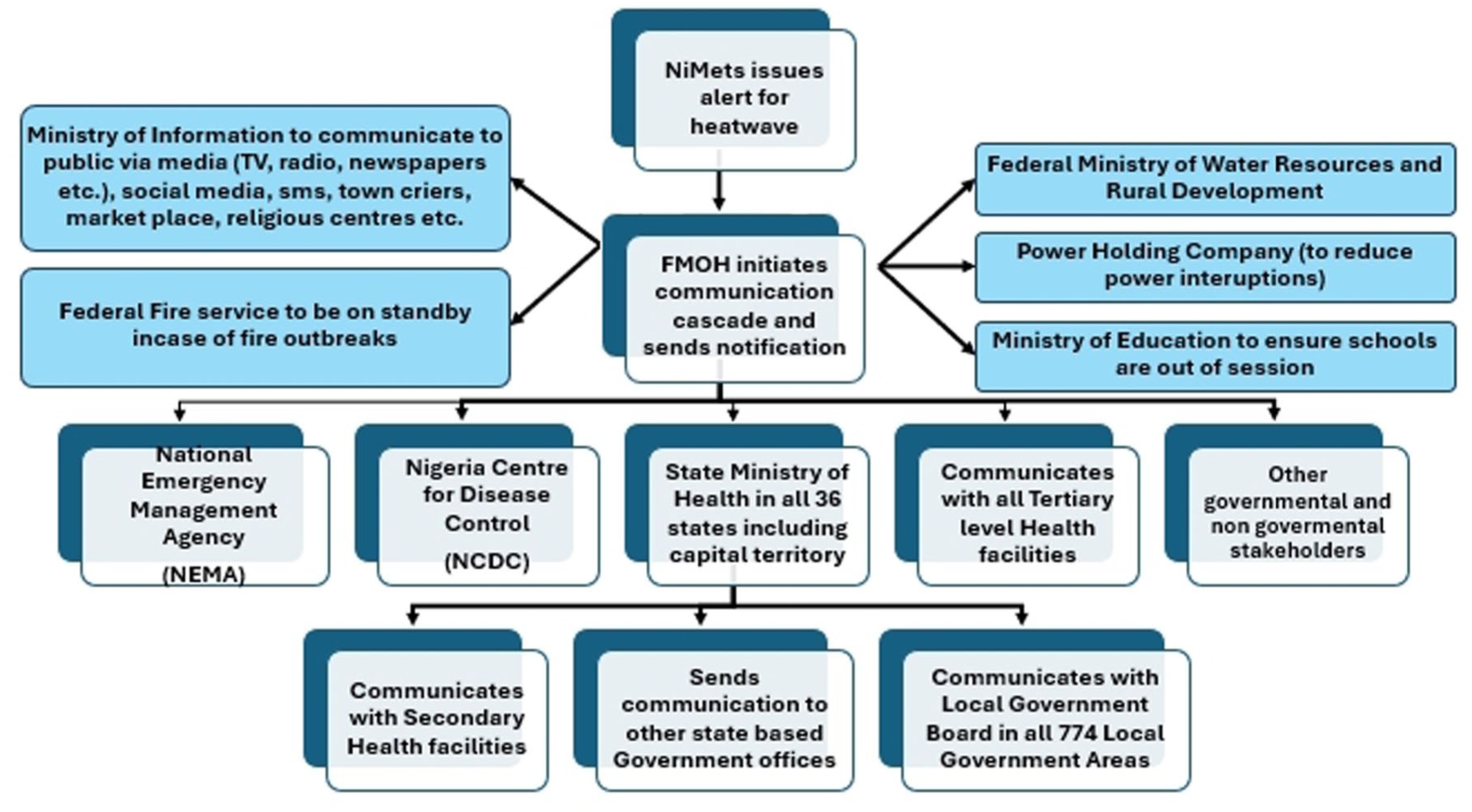
Proposed early warning communication framework for EWS
Public health programmes
The Nigerian health sector is decentralised. The Federal Ministry of Health (FMOH) is responsible for policy development, coordination, healthcare supervision, and provides tertiary/specialised care. The State Ministry of Health is responsible for general/state hospitals, while Local Government Development Boards provide primary healthcare and essential health services, including in rural areas. Public health programmes include HIV/AIDS, tuberculosis, malaria, and health emergency preparedness and response, providing a foundation that can be leveraged for developing and implementing HHPs. 27 These programmes can also contribute supply chains, logistics, and data systems to support resource distribution and health monitoring. 28
Data collection and monitoring systems
Hospital records help monitor heatwave impacts in real-time through recording admissions and deaths due to heatwaves, following Indian HHPs. Data collection can rely on pre-existing structures within the healthcare system, such as local reports from health centres, then collated at State level. Supplementary Figures 1–4 provide a toolkit that can be used for data collection at various levels. Barriers to data collection include insufficient training, staff buy-in, inadequate supply (particularly with paper-based forms), inadequate health personnel, and lack of feedback. 29 Studies from Nigeria have shown how digitalising data collection can provide cost-effective processes that bypass some of these barriers and facilitate data collection, including from remote, hard-to-reach locations. 30
Emergency preparedness systems
Nigeria has systems to respond to health emergencies, natural disasters, disease outbreaks, flooding, and conflicts. The emergency preparedness frameworks from the Nigeria Centre for Disease Control (NCDC) and National Emergency Management Agency (NEMA) can be leveraged for developing EWS, building on other HHPs. EWS needs integration with the Nigerian Meteorological Agency (NiMet) and public and private infrastructure to ensure timely alerts and health advice. NEMA has a functional Geographic Information System (GIS) laboratory that can produce heatwave vulnerability and exposure assessments, tackling some of the limitations of existing HHPs. The NCDC’s monitoring and management of infectious disease outbreaks can be adopted for heatwave data collection, analysis, and reporting, and Nigeria’s partnerships with international organisations (World Health Organization (WHO), United Nations Children’s Fund (UNICEF)) offer frameworks for identifying high-risk areas and enabling responses to heat-health management.
Urban and rural strategies
From a proactive adaptation standpoint, urban heat in Nigeria is concerning in the context of rapid urbanisation and climate change. 31 Reducing heatwave hazards and vulnerabilities requires a combination of short-term and long-term strategies to create sustainable, thriving urban environments based on heat-resilient infrastructure such as green-blue spaces that provide cooling functions, reduce urban heat island effects, enhance air quality, offer refuge during heatwaves, and support mental and social wellbeing. 32 HHPs that prioritise the preservation, expansion, and equitable access to these spaces can deliver both direct and indirect co-benefits for public health and climate resilience.
HHPs can shape urban outdoor heat and building overheating adaptation plans by (1) providing localised climate-health data, enabling city planners and public health officials to pinpoint vulnerability hotspots, identify priority zones, and tailor interventions; (2) informing urban design guidelines, zoning and construction standards that reduce indoor overheating, such as orientation, insulation and passive cooling techniques; (3) enhancing workforce safety protocols, particularly for outdoor labour; and (4) supporting monitoring and evaluation frameworks, enabling the tracking of heat-health outcomes over time to inform iterative improvements to adaptation plans.
Residents of informal urban settlements often lack access to public infrastructure, EWS, and health services, relying on non-governmental organisations (NGOs), community-based organisations, and informal networks for information and support during climate emergencies. Heat adaptation plans should incorporate mechanisms to engage these intermediary institutions in risk communication and service delivery. This includes co-developing climate strategies with local actors, ensuring messages are culturally appropriate and accessible, and strengthening collaboration between public authorities and non-state actors. 33
Heat adaptation plans must include rural areas and the occupational risks of outdoor workers. Although population density is lower in rural areas, those working in critical infrastructures (agriculture, construction, and services) are directly exposed to extreme heat with fewer protective infrastructures or support.
Conclusion
In conclusion, effective heat adaptation demands multiscalar, equity-centred approaches that bridge urban-rural divides, leverage the protective benefits of green-blue infrastructure, and address the vulnerabilities of informal settlements through inclusive governance and partnerships. This inclusive and interdisciplinary urban planning prioritises human health, 31 and integrates health professionals to make health the argument for climate action towards developing HHPs. Aligning these interventions with national health and climate frameworks facilitates low-regret and scalable solutions. As heatwaves become more frequent and severe in SSA, transitioning from reactive to proactive, ‘systems’ approaches is critical to protect life.
Supplemental Material
sj-jpg-1-rsh-10.1177_17579139251371988 – Supplemental material for Towards heat health plans in sub-Saharan Africa: case study – Nigeria
Supplemental material, sj-jpg-1-rsh-10.1177_17579139251371988 for Towards heat health plans in sub-Saharan Africa: case study – Nigeria by Jennifer E Enekebe, SK Dankyi, S Fleury, ED Evci Kiraz and Pedro Beltran-Alvarez in Perspectives in Public Health
Supplemental Material
sj-jpg-2-rsh-10.1177_17579139251371988 – Supplemental material for Towards heat health plans in sub-Saharan Africa: case study – Nigeria
Supplemental material, sj-jpg-2-rsh-10.1177_17579139251371988 for Towards heat health plans in sub-Saharan Africa: case study – Nigeria by Jennifer E Enekebe, SK Dankyi, S Fleury, ED Evci Kiraz and Pedro Beltran-Alvarez in Perspectives in Public Health
Supplemental Material
sj-jpg-3-rsh-10.1177_17579139251371988 – Supplemental material for Towards heat health plans in sub-Saharan Africa: case study – Nigeria
Supplemental material, sj-jpg-3-rsh-10.1177_17579139251371988 for Towards heat health plans in sub-Saharan Africa: case study – Nigeria by Jennifer E Enekebe, SK Dankyi, S Fleury, ED Evci Kiraz and Pedro Beltran-Alvarez in Perspectives in Public Health
Supplemental Material
sj-jpg-4-rsh-10.1177_17579139251371988 – Supplemental material for Towards heat health plans in sub-Saharan Africa: case study – Nigeria
Supplemental material, sj-jpg-4-rsh-10.1177_17579139251371988 for Towards heat health plans in sub-Saharan Africa: case study – Nigeria by Jennifer E Enekebe, SK Dankyi, S Fleury, ED Evci Kiraz and Pedro Beltran-Alvarez in Perspectives in Public Health
Footnotes
Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.