
Abstract
Aim:
We aimed to provide process and effectiveness evaluations of a sex education intervention realized with interactive techniques in high schools of Pavia (Italy).
Methods:
Six public high schools, divided into ‘treated’ and ‘control’ units, voluntarily joined this mixed-methods study. Only second-year classes were enrolled: treated adolescents followed a sex education course, performed by trained ‘near-peer educators’ (undergraduate medical students) with interactive techniques. All adolescents compiled an anonymous effectiveness evaluation questionnaire at baseline (pre-test) and 3 months later (post-test). Sexual knowledge and reported behavioural changes were compared between the two groups through linear mixed-effects models. The process was assessed through a satisfaction questionnaire for treated students, monitoring cards for working group members and cards/diaries for educators.
Results:
The final sample consisted of 547 treated and 355 control adolescents (mean age = 15.28 ± 0.61 years). Highly significant changes (p < 0.001) from pre-test to post-test, with strong improvements of treated adolescents, were evident for all knowledge items. No significant changes for behavioural items were reported. Process evaluation showed positive results in adolescents’ satisfaction, highlighting the need for more youth gathering places. Working group members and educators generally provided positive evaluations, although difficult communication was perceived.
Conclusions:
The intervention was effective in improving adolescents’ sexual knowledge. The present work highlighted that in Italy sex education in adolescence is still neglected: this could encourage misinformation and health-risk behaviour. Young people perceive the need for a serious health-promoting action in which they could play an active role, spreading educational messages with organized interactive methods.
Introduction
Early sexual activity may increase the risk of sexually transmitted infections (STIs) and unwanted pregnancies: the rate of STIs among adolescents is rising and about 15 million adolescents worldwide give birth every year (1). Human Immunodeficiency Virus (HIV) infection remains of major public health importance in Europe (2). In 2012, 29,381 new HIV diagnoses were reported by European Union / European Economic Area countries, resulting in a rate of 5.8 per 100,000 population: 10.6% of them were diagnosed among young people aged 15–24 years (2). The most frequently reported STI in Europe is Chlamydia: in 2010, three-quarters of all Chlamydia cases were reported in young people between 15 and 24 years of age, with the highest rates reported among women aged 15–19 years (3). New diagnoses of syphilis and gonorrhoea are in rapid rise in many European countries (4,5).
The true burden of STIs in Italy is underestimated since surveillance is largely based on mandatory notification by clinicians of new cases for HIV infection, gonococcal urethritis and syphilis, and poor data are available on other conditions (6). Moreover, social factors like immigration have definitely changed the diffusion of STIs (6). In Italy, in 2012, HIV incidence amounted to 6.5 per 100,000 resident population (5.0 new cases per 100,000 Italian residents and 22.3 new cases per 100,000 foreign residents): 80.7% of new infections were attributable to unprotected sexual contacts (7). New diagnoses of HIV infection in 15–24-year-olds were 7.9% of the total in 2008 (8). During 2010 in Italy, 613 new cases of syphilis and 243 of gonorrhoea were notified (9). Syphilis I-II diagnoses increased five times between 2000 and 2005 (10). Reports of gonococcal urethritis and cervicitis doubled between 1999 and 2006 (10). In Italy, voluntary interruptions of pregnancy (VIPs) amounted to 107,192 in 2012 and 85,676 in the first 10 months of 2013 (11). In 2009, the VIP annual incidence rate was 6.62 per 1000 among 15–19-year-old girls and 13.11 among 20–24-year-old women (12).
Accurate sexual education is becoming more and more important (13,14). Early implementation of comprehensive education on sex and relationships is recommended, as it is more likely to be effective if delivered before young people start sexual activity (15). It is relevant to remark that the age of onset of sexual intercourse is declining in industrialized countries (16). According to the HBSC (Health Behaviour in School-aged Children) survey 2009–2010, among 15-year-olds in Italy, 26% of boys and 22% of girls were sexually experienced (1).
The school environment is an ideal setting to promote health (17 –19). Numerous school education programmes have been implemented and some proved to be effective, in particular those focusing on changing behaviour by promoting skills in communication, negotiation and refusal in response to social and media pressure, using a variety of learning methods (20). Among these methods, peer-led interventions are worth mentioning (20). Peer education has become a popular strategy for health promotion and prevention in recent years (21). It has been mostly used for work with youth, based on the assumption that young people learn from and influence each other, as much in risky as in safe behaviour (21 –24).
However, the selection, training and coordination of peer educators in Italian high schools (students’ age range: 14–19 years) entails great commitment and organizational difficulties, due to students’ minor age and the consequent need for parental consent. An easier approach could be to use the typical educational methodologies adopted in peer education interventions (interactive lessons with brainstorming, role play and discussions), replacing ‘peer educators’ with ‘near-peer educators’. The literature shows the effectiveness of near-peer teaching in supporting and guiding younger students during their school career (25 –29). Near-peer teaching refers to situations in which the teacher has significantly more (2–5 years) training than the learner (30). However, the literature does not provide any scientific evidence about health promotion interventions using near-peer educators with interactive techniques. Testing this potentially new strategy for health promotion in general and sexual health promotion in particular could be very interesting.
The general objective of the present study is to increase adolescents’ knowledge about sexual risks and their prevention, in order to promote responsible choices and behaviour. The specific aim is to provide process and effectiveness evaluation of a sexual health promotion intervention run by near-peer educators with interactive techniques in some high schools of Pavia (Lombardy, Italy).
Methods
Development of the study
The entire process described in the present study took place from January 2011 to December 2012, with eight steps, according to Pellai et al. (31):
Planning
Building of the working group and shaping of a common language
Arranging materials, methods and distribution of roles in the working group
Enrolling of schools
Programme application in schools and process monitoring
Assessment of project objectives achievement
Realization of two feedback school events
Effectiveness evaluation
A working group (WG) coordinated the above-mentioned steps. Its members were a researcher at the University of Pavia, two postgraduate medical students specializing in ‘Public Health’ and three undergraduate medical students voluntarily enrolled in SISM and designated as its representatives. The SISM (‘Segretariato Italiano Studenti Medicina’, i.e. Italian medical students’ secretariat) is a non-profit association (32). The WG construction was a continuous circular process. Different perspectives found a common denominator, leading to the comparison of various individual experiences and to the definition of shared work methods, based on Pellai et al.’s guidelines (31,33). It was planned that the WG had regular discussion meetings.
Study design
This research was inspired by a previous sexual education intervention, run for several years by SISM with no formal scientific aim. The present investigation consists of a mixed-methods study, aiming to provide process and effectiveness evaluation of a sexual health promotion intervention run by near-peer educators with interactive techniques in some high schools of Pavia (Lombardy, Italy).
Sample
All public and private high schools of Pavia were invited (by email, phone and individual meetings) to participate. Enrolled schools were divided into two groups (‘treated’ and ‘control’), in accordance with the school’s willingness to actively participate and with attention to having in both groups the three main Italian types of school (humanistic/scientific, technical and vocational). A cluster sampling scheme was adopted, with the classes taken as statistical units. Only second-year classes (age range: 15–18 years) were enrolled.
The sample consisted of 41 classes (902 students, 44.73% males and 55.27% females), divided in 26 ‘treated’ classes (547 adolescents) and 15 ‘control’ classes (355 adolescents). Six public schools were enrolled. They were partitioned into two groups of three treated and three control schools; therefore treated and control classes were generally in different schools. Only one control class was in a treated school, but it had a different location, physically separated from the other classes. All classes were mixed boys and girls.
Intervention
Treated students followed a sexual health education course, performed by two near-peer educators in each class using interactive techniques such as brainstorming, role play and discussions. In order to ensure the accuracy and the similarity of the intervention delivery, all educators held the course following the same predetermined checklist of topics, defined by SISM. The course was divided into two 2-hour sessions and dealt with anatomy and physiology of the reproductive system, sexually transmitted diseases, contraceptive methods, VIP and prevention. During the course, teachers were not in the classroom. The course was delivered in schools between November 2011 and March 2012. Controls received neither the educational course nor the information. Such controls represent the situation of Italian adolescents, living in a context where sex education is not provided by school programmes. At the end of the trial, two feedback events were undertaken in two treated schools to return preliminary results and to discuss them with students and teachers.
The near-peer educators were 30 undergraduate students at the University of Pavia (26 attending the Medical Faculty – including the three SISM WG members – and four attending other courses). They were 19–22-year-old self-selected volunteers. They enrolled in SISM, and followed a special training entirely organized and self-managed by SISM. This training consisted of three lectures held by professionals from the Medical Faculty of the University of Pavia, an intensive 2-day course held by international trainers of the Youth Peer Education Network (34) and simulations of interactive education interventions led by expert educators. The only link between the WG and the near-peer educators was represented by the three SISM representatives, who were both WG members and educators. It was intended that the three SISM representatives had regular meetings with all the educators, in order to transmit to them a periodic oral summary of the WG discussions and methodological decisions.
Data collection methods
The data collection for process evaluation was performed with the following materials, taken from Pellai et al. (31):
a summarizing form (35), compiled at the end of each WG meeting and sent by email to all members. It consisted of a list of discussion prompts, providing a qualitative summary of the WG discussions;
a personal diary and an observation form (36), compiled by each near-peer educator (including the three SISM WG members) for each class at the end of the education course. Each educator wrote his or her personal diary on plain paper, freely writing personal expectations and impressions about the educational course and the attending students. Observation forms consisted of a list of discussion prompts, dealing with the perceived level of adolescents’ emotional involvement, the climate in the class, the verbal and non-verbal communication among students and their relational dynamics;
an anonymous satisfaction questionnaire (37) consisting of eight closed-ended questions, completed by treated high school students after the educational course.
According to Pellai et al.’s guidelines (31), five indicators were used for process evaluation:
acceptance of the study (quantitative indicator constructed with data about adherence and participation of recipients);
monitoring objectives and their achievement at the different steps of the process (qualitative indicator derived from the WG summarizing forms);
near-peer educators’ relationship with treated students (qualitative indicator derived from educators’ personal diaries and observation forms);
satisfaction of treated students (quantitative indicator constructed with data provided by treated students’ satisfaction questionnaires);
comments of public opinion (qualitative indicator derived from the comments verbally expressed by teachers and students’ parents during the two final feedback school events).
The intervention effectiveness was measured with an effectiveness evaluation questionnaire, consisting of 16 closed-ended questions. Both treated and control students filled in this questionnaire at baseline (pre-test), in order to investigate their basal sexual knowledge, behaviour, beliefs and access to services for young people. Three months later, all students completed again the same questionnaire (post-test). As explained above, control students received no information and just filled in the questionnaires at pre- and post-testing. The effectiveness evaluation questionnaires were anonymous and personally unidentifiable. They were distributed to the adolescents by the near-peer educators. During the distribution and filling in of the questionnaire, teachers were not in the classroom. The effectiveness evaluation questionnaire was built with validated questions used in CDC (Centers for Disease Control and Prevention, Atlanta, USA) (38), YRBS (Youth Risk Behavior Survey) (39) and HBSC surveys (40). It was tested before the beginning of the trial with a pilot study on 10 adolescents (extraneous to the sample) and was available in each school to be viewed by students’ parents.
Statistical analysis
For process evaluation, a quantitative analysis was provided for indicators 1 and 4. It consisted of computing absolute and relative percentage frequencies of recipients’ adherence/participation and of selected answers to satisfaction questionnaire items, respectively. A qualitative analysis was provided for indicators 2, 3 and 5. It consisted of a thematic analysis aiming to identify patterns and themes, i.e. common statements or ideas that appeared repeatedly in the WG summarizing forms, in educators’ personal diaries and observation forms and during the two feedback school events (41).
As regards effectiveness evaluation, a crude analysis was initially performed. At first, absolute and relative percentage frequencies of selected answers to all the effectiveness evaluation questionnaire items were calculated by intervention group in the pre- and post-test. The significance of the differences between treated and control group at pre- and post-testing was tested with simple z-tests, with no adjustment covariates and no division by pupils’ classes; p-values < 0.05 were considered statistically significant. To refine the analysis, linear mixed-effects models (LMMs) were then performed. Individual effectiveness evaluation questionnaires could not be linked from the pre-test to the post-test. This lack of information prevented the application of logistic models to the individual answers. The only approach to take into account the repeated assessment of the answers was to consider the questionnaires paired by class of pupils. Therefore percentages of selected answers to pre-test and post-test items, within each class, were computed and taken as effectiveness measures. LMMs were fitted to these response variables, using the pupils’ class as a random effect. Treatment group (treated vs. control students), time of assessment (post-test vs. pre-test) and their interaction were included as explanatory variables (see Appendix in the supplementary online material). To get best fitting models, the following adjustment covariates were also taken into account: type of school, mean class age, proportion by class of females, proportion by class of non-Italian nationality students and – only in the models analysing the knowledge items – proportion by class of sexually active pupils. The interaction between treatment group and time of assessment was taken as the measure of efficacy of the education course – it is the difference between the change that occurred from the pre-test to the post-test in treated students and the change in control students. The random effect and the residual error of the models were taken as Gaussian variables, because the percentages analysed did not generally show very skewed distributions. The analysis of logit transformed percentages by LMMs has been shown to be biased by Molas et al. (42). This and the need to provide easily interpretable estimates of efficacy dissuaded the Authors from the application of the logit transform. P-values < 0.05 were considered statistically significant. Calculations were carried out using the statistical software R, version 2.15.3 (43), and its package nlme (44).
Ethics
All the participant schools’ headmasters obtained permission to carry out the research from a parent representing all students’ parents in the school. Headmasters gave written assent to analyse data in accordance with the Italian Privacy Law (D.Lgs. 196/2003) (45). The Ethical Review Board of the University of Pavia approved the study protocol.
Results
Sample
Six public schools voluntarily joined the trial (two humanistic/scientific, two technical and two vocational units), with 938 students divided in 43 second classes. Two classes (36 students), one in the treatment group and one in the control group, were excluded because they followed a separate unconnected sex education course and filled in only the first half of the effectiveness evaluation questionnaire. The final sample consisted of 902 students (41 classes), divided into 547 treated adolescents (26 classes) and 355 controls (15 classes).
Table 1 shows some socio-demographic and behavioural characteristics of the sample at baseline, by intervention group. The mean age was 15.28 ± 0.61 years and 28.95% of the students were sexually active: this percentage is slightly higher than the one reported for 15-year-olds in an HBSC survey in Lombardy (46). Compared to the control group, the treatment group showed a higher proportion of non-Italian nationality adolescents (9.56% vs. 4.24%), a higher percentage of sexually active students (33.70% vs. 21.69%) and a lower proportion of students saying they were 11 years old or less at first sexual intercourse (1.12% vs. 10.53%).
Characteristics of students at baseline, by intervention group.
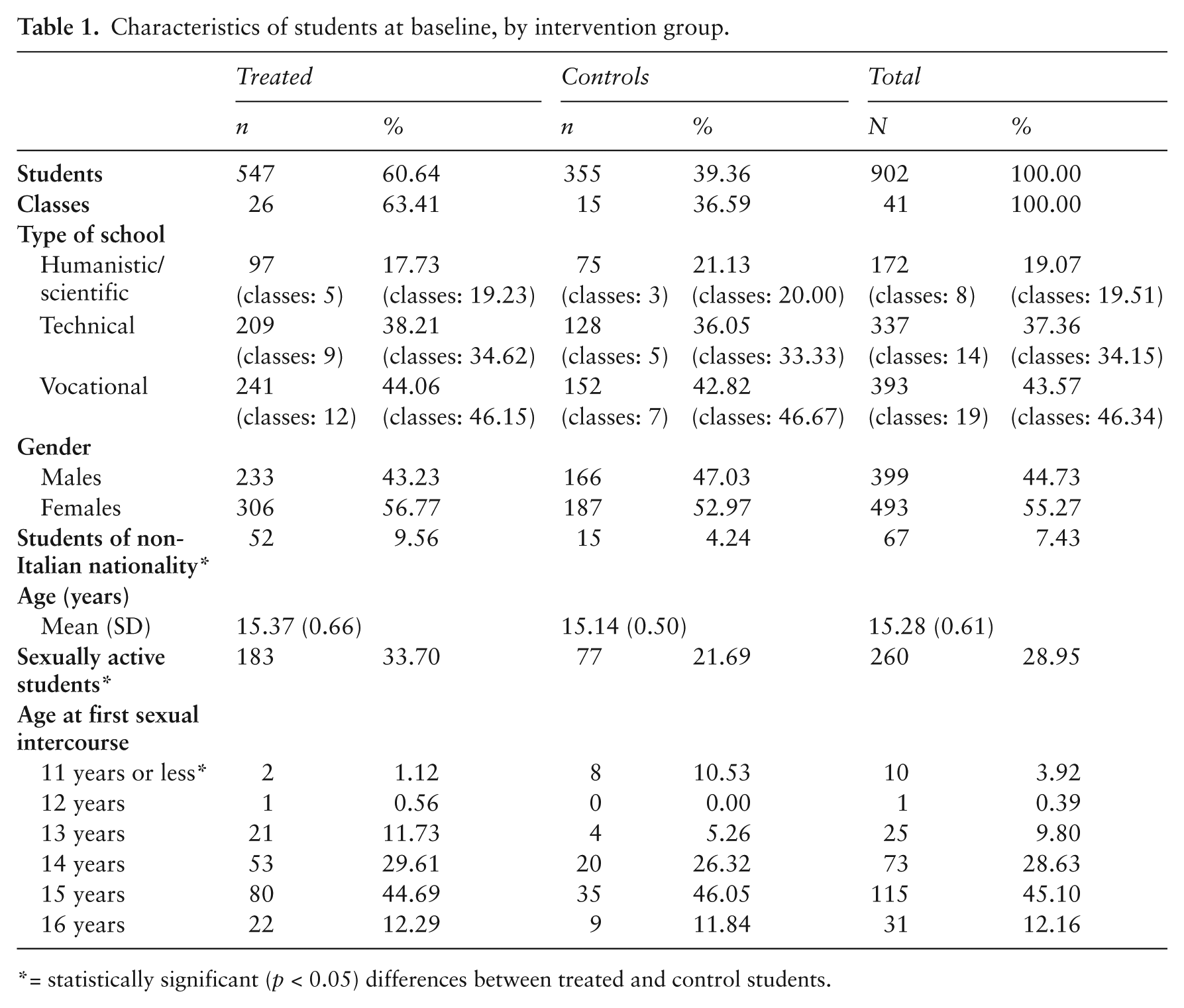
= statistically significant (p < 0.05) differences between treated and control students.
Process evaluation
1. Acceptance of the study
All the high schools of Pavia (nine public and two private) were considered. One of the two private schools had no second-year classes and so it was excluded. All 10 remaining schools were invited. Adherence was on a voluntary basis and was at the discretion of school headmasters and health referents, who had to choose among different educational projects proposals. Seven schools out of 10 (70%) answered the invitation. However, one public school decided to hold the intervention only in the fourth classes and so it was not included in the research. Therefore, in the end, six schools out of 10 (60%) joined the study: three as treated and three as control schools. There were 43 participating second classes (70.49% of all second classes of the six selected schools), divided into 27 treated (100% of all second classes of the three treated schools: five humanistic/scientific, nine technical and 13 vocational classes) and 16 control classes (47.06% of all second classes of the three control schools: four humanistic/scientific, five technical and seven vocational classes). Two classes, one in the treatment group and one in the control group, were excluded because they followed a separate unrelated sex education course and compiled only part of the effectiveness evaluation questionnaire. The final sample consisted of 41 classes, divided in 26 treated and 15 control classes as shown in Table 1.
2. Monitoring objectives and their achievement at the different steps of the process
The WG meetings were held regularly. Members brought their point of view and their personal opinions. The meetings between the three SISM representatives and all the educators did not take place regularly as had been planned. As a consequence, the intended oral summaries about the WG decisions were only sporadically transmitted, and this lack of regular communication sometimes led to misunderstandings. Despite these problems, the various steps of the process were reached and the end result was satisfactory, leading to personal and professional enrichment of all WG members.
3. Near-peer educators’ relationship with treated students
Observation forms were compiled by 50% of near-peer educators. The climate in the classroom during the education courses was generally different between the two sessions. In the first one it was always slightly detached, turning to be more confidential and relaxed in the second one. Males generally appeared to be less attentive and involved than females. Personal diaries and observation forms suggested that near-peer educators felt at ease during the education course and perceived high schools students as ‘peers’, in particular in vocational units where pupils’ mean age was higher.
4. Satisfaction of treated students
Satisfaction questionnaires were completed by 99% of treated students. Results showed generally positive evaluations for each investigated item (see Figure 1). Some 87.06% of responders felt emotionally involved in the discussion in the classroom, 99.50% pointed to peer education as the right way to deal with sexuality topics, 90.89% felt wiser in sexuality matters, 76.57% did not attend a group where they could continue to talk about sexual health and 32.38% desired to become peer educators.
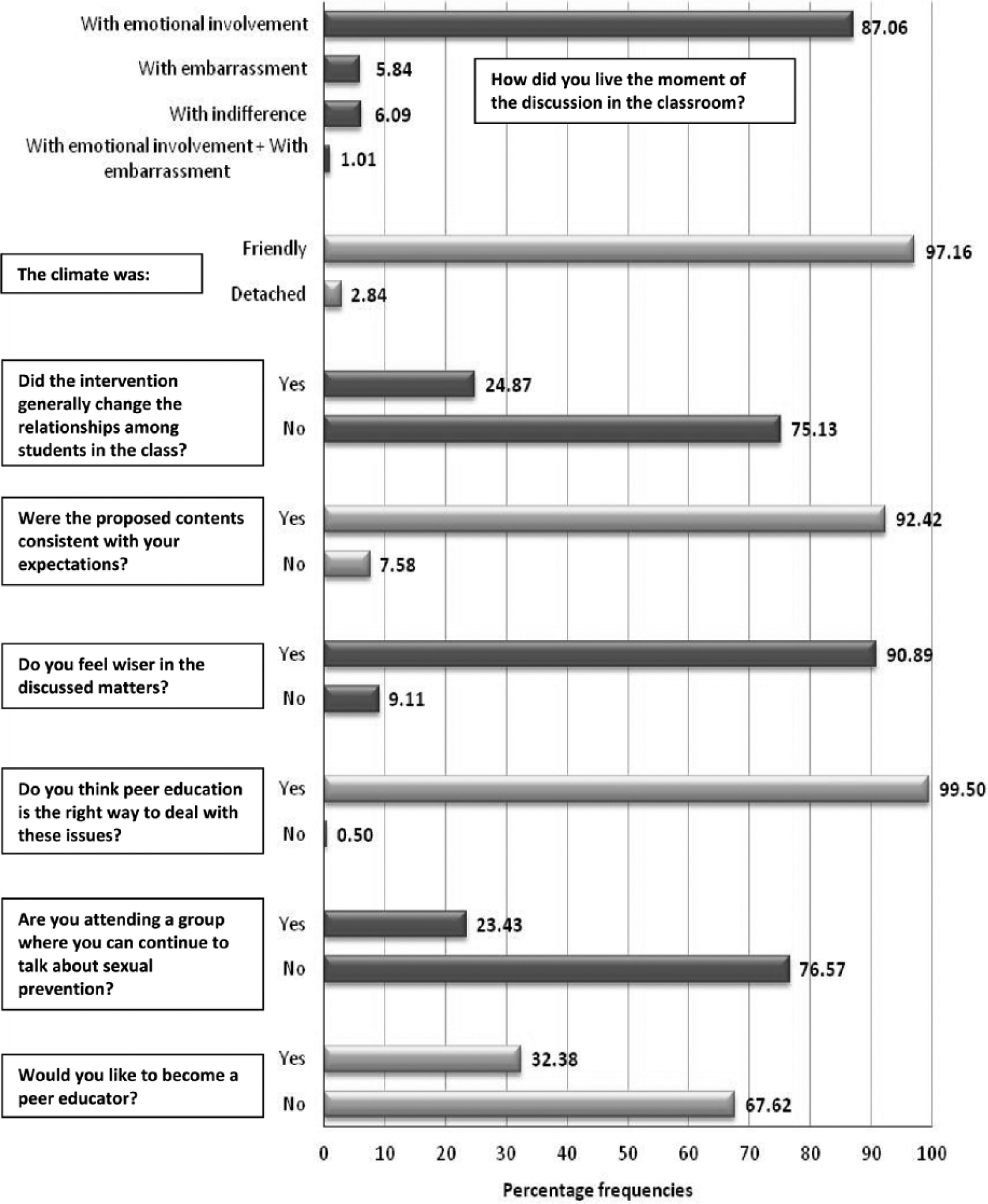
Results of satisfaction questionnaires.
5. Comments of public opinion
At the end of the intervention, two feedback school events were undertaken. All the WG members discussed with students and teachers about the need for sex education in Italian schools and the most appropriate methodologies to provide it. Teachers liked the intervention. However, they suggested that it would be better to promote both sexual and affective education. Teachers also reported the opinion of students’ parents, generally showing a fairly good acceptance for the intervention. Only in one school, after the education course, some parents told the teachers that they did not like this educational strategy.
Effectiveness evaluation
A total of 902 students completed the pre-test, 872 completed the post-test. The attrition rate was 3.5% for the treated group and 3.1% for the control. Attrition was mainly due to school absenteeism.
Table 2 (Online Appendix only) ii shows the crude analysis results. The main information sources about sexuality were represented by friends (pre-test: 55.98% of treated and 44.02% of controls; post-test: 52.18% and 45.27%) and internet (pre-test: 30.17% of treated and 30.03% of controls; post-test: 37.38% and 39.05%). In case of sexual problems, pupils mainly turned to friends (pre-test: 53.33% of treated and 53.15% of controls; post-test: 52.21% and 49.11%) and family (pre-test: 48.76% of treated and 53.45% of controls; post-test: 50.67% and 57.44%). At pre-testing, 55.76% of treated and 54.80% of controls (p = 0.778) knew that HIV could be found in biological fluids; at post-testing, these percentages were 79.35% and 56.69% (p < 0.001). At pre-testing, 14.55% of treated and 14.81% of controls (p = 0.914) knew the HIV-antibody test window period; at post-testing, these percentages were 42.07% and 17.30% (p < 0.001). At pre-testing, 80.22% of sexually active treated and 85.71% of sexually active controls (p = 0.268) used a method to prevent pregnancy during the last complete sexual intercourse; at post-testing, these percentages were 81.50% and 91.58% (p = 0.011).
Table 3 shows the refined analysis results. Highly significant changes from pre-test to post-test, with strong improvements of treated against controls, appeared to be evident for all knowledge items. The difference between the change from the pre-test to the post-test in treated and the change in controls reached a peak of +24.76% (p < 0.001) for the question about the HIV-antibody test window period. It was also very high for the questions about the presence of HIV in biological fluids (+21.30%, p < 0.001), the absence of risk in kissing a friend with AIDS (Acquired Immune Deficiency Syndrome) (+20.05%, p < 0.001), the possibility of getting HIV with a tattoo or a body piercing (+19.81%, p = 0.002) and the possibility for STIs to be asymptomatic (+19.10%, p = 0.001). Good results were also obtained for the questions about what could be done to decrease the risk of getting a STI (+13.39%, p = 0.002), the best way to avoid getting HIV (+11.61%, p = 0.032), the absence of risk in meeting AIDS sufferers in public places (+11.23%, p = 0.019) and the possibility of getting HIV having sex without a condom (+7.84, p = 0.023). The main information sources about sexuality changed from pre-test to post-test. For treated students, compared with controls, school gained in importance (+9.37%, p = 0.059), while family became less relevant (−17.06%, p < 0.001). The way in which treated students asked for help in case of sexual problems did not change from pre-test to post-test. They only turned a little bit more to the hospital (+4.45, p = 0.051). No significant changes for behavioural items were reported. From pre-test to post-test, treated compared with controls did not change their behaviour about the use of methods to prevent pregnancy. All items were largely above the considered significance level (p = 0.05). Only the decrease in the use of condom drew closer to the significance, without reaching it (−10.89%, p = 0.062).
Linear mixed-effects models (LMMs): treatment effect (in percentage difference scale) on sexual knowledge and behaviour of students, with division by pupils’ classes and adjustment covariates (age, gender, nationality (Italian vs. non-Italian), type of school and – only for knowledge – sexually active students).

a: Treatment effect = (Tpost − Tpre)% – (Cpost − Cpre)%, where:
Tpost = percentage of selected answers among treated students in the post-test,
Tpre = percentage of selected answers among treated students in the pre-test,
Cpost = percentage of selected answers among control students in the post-test,
Cpre = percentage of selected answers among control students in the pre-test.
: 95% CI = 95% confidence intervals.
: differences are considered ‘statistically significant’ if p < 0.05 and ‘highly statistically significant’ if p < 0.001 (nearly statistically significant, statistically significant and highly statistically significant p-values are reported in bold).
Discussion
Process evaluation
High schools showed good participation in the intervention, despite the organizational difficulties and the large number of other educational projects proposals. This reflects their interest in a potentially new education strategy.
During the education course, males generally appeared to be less attentive than females. This could mean that different messages may be needed for boys and girls within programmes that focus on the use of contraceptives, as reasons for and barriers to carrying and using condoms may differ between genders (1).
The fact that the majority of high school students considered the intervention beneficial and appreciated the participatory nature of the sessions reflects the important role of educators in the successful implementation of education sessions at the classroom level, as shown by other studies (47). Many adolescents desired to become peer educators, but reported difficulty in finding a group where they could continue to talk about sexual health. Many young people could be interested in spreading sex education messages with organized interactive methods, but they perceive that there are not enough gathering places for youth. Many youth services are closed during the times of greatest need (i.e. after hours, particularly on weekends). In this regard, an interesting suggestion comes from Australia, where some shopping centres provide vacant shops to the local youth service to utilize (48).
The two feedback school events showed that Pavia public opinion is going towards acceptance of sex education in schools, as also reported by a local newspaper. However, there is still a lot of discussion about the most appropriate methodologies. To promote not only sexual but also affective education is certainly desirable. Nevertheless, due to the complexity of the arguments, it is not easily achievable by young undergraduate students.
Effectiveness evaluation
The present study results were not completely comparable with those of other studies. The present research did not have the same methodological characteristics as literature about high school peer education studies, because involved educators were near-peer educators, close to the target population age but attending university.
The crude analysis showed, both for treated and controls, the importance of friends as information sources about sexuality and counsellors in case of sexual problems. This was in accordance with the well-known assumption that young people learn from each other, as much in risky as in safe behaviour (21–24). Treated compared with controls appeared to significantly improve their knowledge in many items. In behavioural items, controls compared with treated seemed to increase the use of a method to prevent pregnancy during the last complete sexual intercourse. In this regard, it is essential to remember that the crude analysis gave only a rough idea about the effect of the education intervention, because results had no adjustments and were affected by the baseline differences between the treated and control groups.
The refined analysis with LMMs assessed the effect of the intervention on treated students compared with controls. Considering the adjustment covariates, it provided results not affected by the baseline differences between treated and control group. The intervention was very effective in improving sexual knowledge of treated adolescents, in accordance with literature findings (20,49). The course also helped to dispel widespread prejudices about AIDS sufferers, such as those about kissing a friend with AIDS. Furthermore, the intervention contributed to affirm the importance of school as a more scientific information source about sexuality and reduced the influence of family. This could be a good thing, since many parents themselves do not have the information that young people need (50). The education course did not affect the way in which students asked for help in case of sexual problems. The treated group turned only a little more to the hospital after the intervention. This could mean that adolescents do not perceive public youth and family counselling as an environment where they can talk about problems. In this regard, the World Health Organization identified shortcomings in the availability and/or suitability of adolescent-specific health services in many countries (1). According to the most accredited models of behavioural change, improvements in knowledge items are important because they are considered antecedents for changes in sexual behaviour (20,51). In the present study, no significant changes in sexual behaviour of treated compared with controls were observed. The same absence of changes was reported in other studies (20, 49). This could be explained with the brief time interval between pre- and post-testing. Many studies indicated that longer intervals are more appropriate to observe behavioural changes (20). Another reason could be that, at baseline, 28.95% of the students were already sexually active. The literature shows that it is more difficult to change an already established behaviour (52).
Study limitations
The present study had some limitations. First was the communication gap between the WG and the educators. The lack of regularly scheduled educators’ meetings sometimes led to misunderstandings in the passing of information about WG methodological decisions, resulting in a delay in the work. For example, some educators did not receive the observation forms on time to be filled in appropriately, with consequent loss of data for qualitative process evaluation. Regarding organizational difficulties, it was impossible to create direct communication between all WG members and all educators.
Second, there was no randomization of the sample. The Authors chose to give greater importance to the socio-cultural level of the students, making sure that each type of treated school (humanistic/scientific, technical or vocational) was matched with a control of the same type. Despite the matching by type of school, treated and controls at baseline were not completely comparable. Three baseline characteristics of the whole examined panel were significantly different between the two groups. These differences were probably due to an incomplete homogeneity between the two vocational schools of the sample. The treated vocational school, compared with the control, had students with a lower socio-cultural level. Many of them were remedial students or non-Italian nationality adolescents, came from families with substance abuse problems and started early sexual activity. These were the only two vocational schools in the city of Pavia, and such a difference between them was not expected. The Authors included the above-mentioned baseline differences as adjustment covariates in the LMMs used to refine the analysis for effectiveness evaluation, so that they could not affect the study results.
Finally, the impossibility of matching the pre- and post-test scores was a significant weakness in the analysis for effectiveness evaluation, but high school headmasters, teachers and students’ parents did not accept any form of personal identification for effectiveness evaluation questionnaires.
Conclusions
In Italy, sex education in adolescence is still neglected. It is difficult to address sex education, especially for some parents. Furthermore, sex education is not provided by school programmes. Experts from Italian Higher Health Institute have recently stressed the urgent need for a National Plan for sexual health promotion and STI prevention (10). The school should play a key role, both in health education of young people and in increasing public awareness (10). An accurate health-promoting intervention should be implemented before the onset of sexual activity, and then it should be strengthened in continuous integration among different grades of schools (15,17). Health promotion interventions run by near-peer educators with interactive techniques could be an effective strategy to involve adolescents in a growth process towards the awareness and maturity needed to respond in a healthy way to life events, overcoming the organizational difficulties presented by classical peer education interventions.
Footnotes
Acknowledgements
The Authors wish to acknowledge Prof. Alberto Pellai for assistance during the study protocol writing, Prof. Marisa Arpesella for research support, all high school headmasters and teachers for the participating in the study, Dr. Davide Guido for his precious contribution during data analysis and Dr. Alessia Varetta for help in data entry.
Preliminary results of the present work have been presented, in form of a poster, during the 45th National Congress of S.It.I. (Società Italiana di Igiene, i.e. Italian Society of Hygiene): 3–6 October 2012, Santa Margherita di Pula, Cagliari, Italy.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
i.
Members of the SISM educators group: Francesca Acerbi (M.D. student), Erika Andreatta (M.D. student), Anna Arcoraci (M.D. student), Micòl Bacchini (M.D. student), Marica Barbieri (psychology student), Francesca Bettini (M.D. student), David Bosoni (M.D. student), Pierluigi Calò (M.D. student), Dario Cani (M.D. student), Davide Cavalieri (Communication, innovation, multimedia -C.I.M.- student), Fabio Chinellato (M.D. student), Francesca Colao (psychology student), Giulia Costantini (M.D. student), Silvia Costelli (M.D. student), Sofia Di Noia (M.D. student), Erika Frascolla (psychology student), Alessandro Lusso (M.D. student), Arianna Chiara Marinello (M.D. student), Flavia Mazzocchetti (M.D. student), Gianluca Melatini (M.D. student), Mattia Passeri (M.D. student), Elena Rho (M.D.), Giulia Saturi (M.D. student), Cecilia Spallarossa (M.D. student), Alessandra Vanetti (M.D. student), Riccardo Villani (M.D. student), Andreana Zecchini (M.D. student).
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.