
Abstract
This qualitative study examined smokefree leadership among the Yolŋu people, Indigenous landowners of East Arnhem Land. Despite disproportionately high smoking prevalence, the study found that most people enacted smokefree leadership within families and communities. While there was broad concern about not impinging on the autonomy of others, Indigenous health workers regularly advised clients, family and community members to quit smoking. This followed a general belief that the issue of smoking was best raised by health workers, rather than traditional leaders. Protecting children from second-hand smoke and preventing smoking initiation was important to all participants irrespective of their smoking status. An enduring and highly valued cultural connection to ŋarali’ (tobacco) remains an essential part of the sacred practices of the funeral ceremony, an important and unique social utility. The study found consensus among participants that this would not change. Navigating traditional connections to ŋarali’ in a context where most people are still addicted to commercial tobacco is challenging and requires respectful and culturally compelling approaches. Tobacco control initiatives with the Yolŋu should therefore utilise existing smokefree leaders within the social context in which ŋarali’ is valued and used, an approach that may resonate with other Indigenous Australian nations and communities.
Introduction
Tobacco use is the single largest preventable cause of death and chronic disease in the world today, causing millions of deaths every year and is a risk factor for six of the eight leading causes of death, including heart and lung diseases and several cancers (1).
The proportion of Indigenous Australians who are current daily smokers has declined by six percentage points from 45% in 2008 to 39% in 2014 (2). However, there has been no significant change in prevalence or successful cessation in remote areas (3). In some remote Northern Territory communities in East Arnhem Land, smoking prevalence between 68% and 83% in men and between 65% and 73% in women has been reported with little change since the mid-1980s (4). Smoking represents a barrier and a challenge to Indigenous peoples reaching their full potential in terms of their social and emotional health and wellbeing (5), prematurely divesting communities of Elders and loved ones due to smoking-related diseases.
The Indigenous daily smoking prevalence is 2.8 times that of non-Indigenous Australians and, as such, is responsible for 23% of the health gap in the burden of disease, as measured by the difference in disability-adjusted life years (6). This is greater than the estimates for the contributions of other risk factors to the health gap, such as high body mass (14%), high blood glucose (9%), physical inactivity (8%), alcohol consumption (8%), high blood pressure (8%).
The study was undertaken in East Arnhem, a land area of 3,337,993 hectares with Aboriginal and Torres Strait Islander individuals comprising 91.2% of a population of 10,000 people (7). The Indigenous owners of this area are the Yolŋu peoples. The region includes bauxite plateau country, sparse grasslands, and coastlines of sandy beaches, rocky headlands, sand islands and tidal inlets of mangroves (8). People live in widely dispersed remote communities, only accessible by four-wheel-drive vehicles or light aircrafts.
The study sought to address a notable gap in the literature of the role of Indigenous smokefree leadership. While capacity-building to mobilise community stakeholders and to facilitate culturally sanctioned change and prevention strategies has been highlighted (9), the involvement of Elders and leaders in Indigenous communities as a culturally relevant resource for health is currently underused and under-examined (10).
Background
Indigenous peoples, their society, traditional values and cultural beliefs and practices have been significantly affected since the colonisation of Australia begun by the British in 1788. Government-led policies removed children from families and communities and Indigenous peoples were separated from or lost their traditional lands during this period, contributing to the creation of unhealthy living and social conditions and to a higher level of tobacco use (11).
Introduced to Arnhem Land as a trade item by the Macassans in the 1700s (12), ŋarali’ or tobacco became a highly-prized commodity among the Yolŋu and was restricted to senior and initiated men (13). Common or profane use of tobacco by both men and women has developed over time. However, the meaning of ŋarali’ remains sacred. It is a part of culture and ceremony (14) and is often described as mulwatj (precious) or culturally important, (13) as it is associated with the funeral ceremony. However, this ceremonial role of tobacco does not generally involve its smoking.
Methodology
The study sought to set an Indigenous agenda that is broad in its scope, prioritising notions of self-determination, participation, empowerment and decolonisation (15). The approach resists and opposes Western research practices and preferences that are rooted in a deeply colonial institution (16) which has marginalised Indigenous communities, silenced their voices and favoured the representation and interpretation of ‘expert’ others. The aim of the study was to privilege Indigenous knowledges, experiences, reflections and analyses of their social, material and spiritual conditions (17), giving voice to those who have not spoken or been heard (18).
The research methodology sought to demonstrate and value respectful and culturally appropriate communication with participants, acknowledging that, within Yolŋu society, there are complex roles and specific kinship relations that may dictate, for example, who is responsible for different places and ceremonies and who must be avoided out of respect (19).
Two cultural mentors (CMs), one male and one female, were recommended to the researcher (MT) by the local health services and were approached separately to ascertain their interest in advising the research project. They guided the researcher during interviews and helped her to navigate the cultural sensitivities related to avoidance relationships, kinship dynamics and interviewing participants who spoke English as a second, third or fourth language. The CMs were senior, respected community members known to all interview participants. The CMs appraised the interview guide, gave feedback to improve clarity and were present during interviews, translating questions and answers into a Yolŋu Matha language. The CMs added further insight and valuable analysis during face-to-face meetings and later by phone when MT was reviewing data and coding.
The study adapted Bronfenbrenner’s social ecological model (SEM) (20) of human development to explore leadership in these communities, using four nested, hierarchical levels (see Figure 1) to conceptualise a Yolŋu worldview. Everything in the Yolŋu universe – Spirit Beings, plant and animal species, clan groups, areas of land and water are either Dhuwa or Yirritja and within each moiety, people belong to smaller groups called clans, each having its own language (21). Children belong to their father’s clan (and moiety), while their mother belongs to another clan (of the other moiety). The first level represents the individual and their family and extended family, the second level denotes their employment and/or their involvement within their community, the third level is their identity in their Bäpurru or clan, and the fourth level is their moiety membership (Dhuwa or Yirritja), which is determined by patrilineal descent.
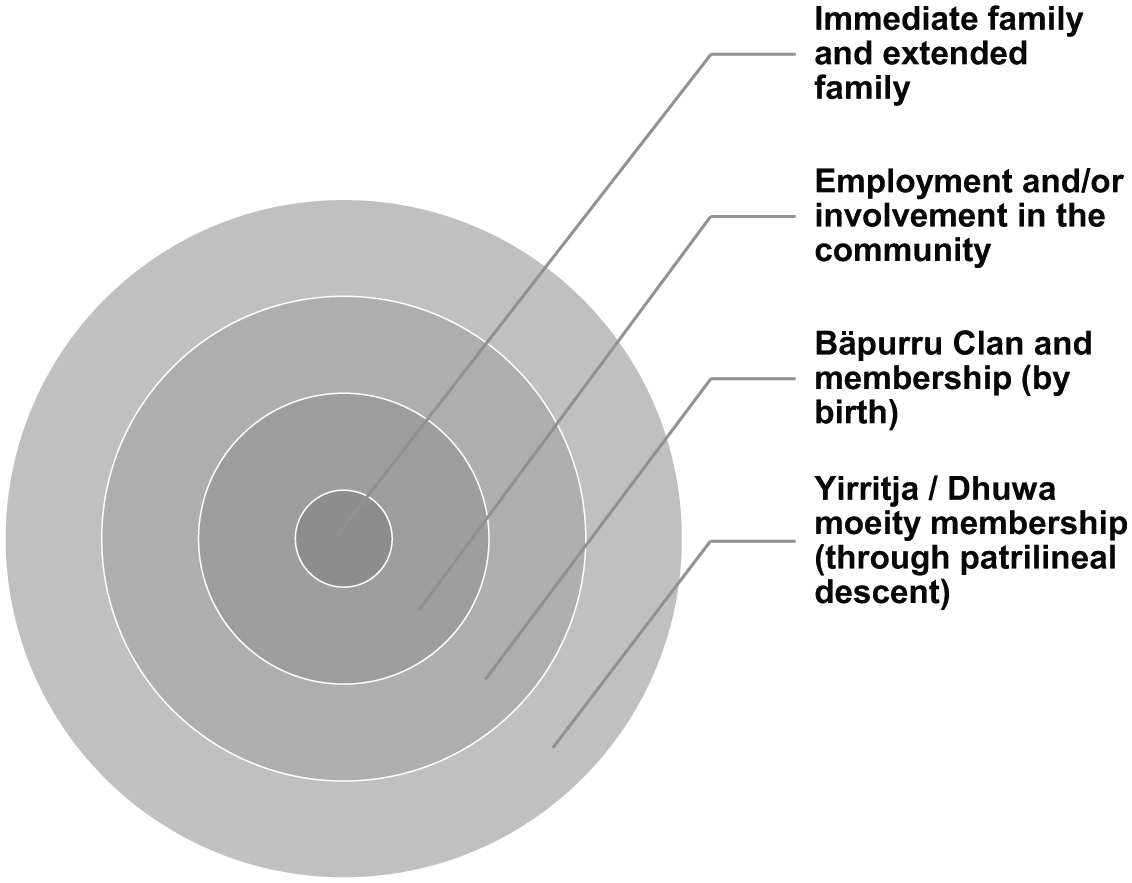
Adapted from Bronfenbrenner’s social ecological model (SEM) of human development to explore Yolŋu leadership, using four nested, hierarchical levels (20).
The definition of leadership used to analyse participant interviews is located within Ivory’s analysis of Indigenous Australian modalities of governance, founded on social constructs and culturally based institutions and systems (22), which conceptualises leadership as a network that extends across communities and regions. Aboriginal leadership is also strongly associated with a purposeful and active sense of identity and self-determination (23).
Participant selection
Initial contact with communities was made through local health services and meetings held with Elders and leaders to discuss the project aims and to request permission for interviews. Following approval, the researcher (MT) returned to the communities with a CM to recruit information-rich key informants, progressing to snowball enlistment wherein existing participants recruited family members.
Interview setting and approach
Interviews with key informants were conducted on the veranda and in consult rooms at remote community health clinics (n = 15), a participant’s home (n = 1) and the home of the researcher (n = 6) and were audio-recorded with permission for later transcribing. Information sheets were distributed to all informants who signed informed consent forms before the interview began. A CM was present during interviews for translation and interpretation.
Field notes were written immediately after the interviews; however, these were very brief. A review of the field notes was performed during data analysis and informed coding and memo writing. Interviews lasted between 20 minutes and 1 hour.
Sample size and description
Interviews took place with 22 Yolŋu key informants. Of these, 13 were employed with local health services as Aboriginal health workers, Aboriginal health practitioners, tobacco action workers (TAWs) and administration staff and the rest were community members. There were 9 female and 13 male participants.
Data analysis
Data were analysed using the framework method, which involved seven stages (24). In the first and second stages, interview recordings were transcribed by MT who became familiar with the content and immersed in the data through playback of recordings, working alongside the CMs who offered insight and comments. These sessions were also recorded and later analysed. Memo writing was used during coding to explore and analyse the data and the relationships between codes.
In stage three, line-by-line coding of small blocks of text was undertaken using NVivo 10. In stage four, an analytical framework was developed from a priori themes associated with tobacco control strategies in the region (25). These included smokefree environments, television and media advertising, access to smoking cessation support, and Indigenous leadership. The framework also included emergent themes derived from open (unrestricted) coding.
In stages five and six, transcripts were reviewed again in their entirety to check indexing and coding decisions made and participant attributes (such as smoking status, position in the community, gender, age) were also analysed. During the seventh and final stage of analysis, a spreadsheet was used to index codes and categories and to summarise and chart the themes. Indicators of smokefree leadership actions within the individual participant’s sphere of influence across the different levels of the SEM were then developed.
Results
Smokefree leaders and advocates
Despite living in communities where smoking is the norm, there were many examples of Indigenous smokefree leadership or advocacy reported by participants. These included promoting or encouraging smokefree spaces in and around homes, encouraging others in their immediate or extended family to quit smoking, being aware of and actively preventing children from being affected by second-hand smoke and educating and warning family members and children about smoking initiation.
Participants reported varying levels of confidence to raise the issue of smoking with family, clients or colleagues. Those who were ex- and never-smokers, and were employed by a health service reported the most confidence. Among all participants, irrespective of smoking status, there was an acknowledgement of personal agency in choosing to smoke, or to quit smoking. An aversion to forcing others or ‘telling’ people what to do was expressed: We can’t force them to quit, it’s their own feeling if they want to come in and quit, they need to come in themselves and by their own consent … better for them and we can’t force them, but they have to think for themselves (health service employee, female, ex-smoker).
Thus, among those participants who enacted leadership across all levels, advocacy and education about the harms of smoking was often presented to smokers as ‘reminders’ or ‘encouragement’, a socially acceptable way to raise the issue for everyone: And when they have a sports carnival in Galiwin’ku or anywhere, and there are women and men who play football, then we have to go and encourage them not to smoke (health service employee, male, never-smoker).
Family and children
Participants at all levels of the SEM, irrespective of age, gender, smoking status, employment, clan and moiety membership, considered that children need to be protected from the harms of second-hand smoke and believed that adults could influence them to prevent smoking initiation. All participants showed smokefree leadership had been enacted in some measure within the immediate and extended family (the smallest circle in the centre of the Figure 1 diagram). Within this context, participants acknowledged the role of parents in preventing (or allowing) smoking initiation by children: ‘I say to them [my children] you know ŋarali’ is no good for you for your whole body, lungs, no good for you’ (community member, female, never-smoker). Some parents also protected their children and other family members from second-hand smoke. For example, a mother had established smokefree zones around her home and her yard using smokefree signs, and requested visitors to move away from the house to smoke: ‘Yes [she] doesn’t like people sitting in front of her, when the wind is blowing from here … and she doesn’t like people smoking in front of her and the kids (CM translating for community member, female, never-smoker).
Employment and/or involvement in the community
Within the workplace, participants who were employed by a health service used many opportunities to raise the issue of smoking, irrespective of their smoking status. An Aboriginal health practitioner reported her efforts in giving advice to quit smoking to her clients as an integral part of her role: ‘Yes, they know because I always tell my families [to quit smoking] when I sit down cause I’m a registered health practitioner’ (health service employee, female, ex-smoker). Another health worker described how he supported the smokefree workplace policy, influencing others to abstain from smoking while at work or purchasing tobacco while in uniform: Ŋarali’ is the policy inside the building, or workplace, you don’t smoke. And if it’s outside, that’s good eh? ‘Hey, we are health workers, look we got our shirts here, we can’t get cigarettes while using the red shirt’ (health service employee, male, never-smoker).
Describing her misgivings about giving advice to quit while being a smoker, a health worker continued to offer encouragement to her clients: ‘Yes, I do [encourage others to quit] but how can that person stop or quit smoking, if they like smoking?’ (health service employee, female, current smoker). Another participant believed that she should not give education about ŋarali’ to her clients because she was a smoker, preferring non-smokers to undertake this work; she observed: The [ŋarali’] program has been going but one day I said to him, ‘You’ll do an education on ŋarali’, yaka ŋarali’ [don’t smoke] program. I’m not doing that because I’m a smoker. Only people can do that, that are non-smoker. But we can sit and listen’ (health service employee, female, current smoker).
Two health workers explained that because of their professional roles, they had refused to purchase tobacco for family members, a common practice among the Yolŋu where sharing is expected and highly valued: My mum used to do that, she was a heavy smoker; she still smokes. Sometimes she asks me to buy cigarettes and I say, ‘I can’t, I can’t buy cigarettes, I’m not allowed to kill you!’ (health service employee, male, ex-smoker). Like for me I’m a registered health practitioner and I don’t want to buy ŋarali’ and giving it to a person, that means I’m killing them! (health service employee, female, ex-smoker).
Traditional leadership roles – related to moiety (Yirrtja/Dhuwa) and clan (Bäpurru)
Many of the key informants reflected on the deep connection to ŋarali’ over hundreds of years, a relationship that affects Yolŋu across all levels of the SEM, with one informant describing its arrival in Arnhem Land: The Macassan people brought it and before when the missionaries came here, they brought all the ŋarali’. Long, long, time ago, old people, a long time ago, they found ŋarali’ and they started smoking … ŋarali’ was spread everywhere (Elder, male, ex-smoker).
A senior informant also described the importance of ŋarali’ during the funeral ceremony being a commemoration of culture and a tribute to farewell the deceased: The times when we celebrate in the funeral time to remember [the deceased] when he was alive, when he was a smoker, that’s why we have singing songs and smoking [ceremony]. In other words, saying goodbye. That is how we form part of our story, our songline (Elder, male, ex-smoker).
Two TAWs had additional responsibilities in their traditional roles, one as a clan leader and the other as a performer of the ŋarali’ manikay (tobacco songlines), but both spoke to others about the harms of smoking and the benefits of being smokefree: ‘I’m a leader as my Clan too. As a leader, I have to educate people not to smoke around the houses, don’t smoke in front of kids, keep your cigarette secret (health service employee, male, never-smoker). An Aboriginal Health Worker, when asked about the role of clan leaders in warning others about smoking, replied: The Clan leaders? Half of the Clan leaders they smoke cigarettes! The best is [referring to TAWs] because they’ve got tight [united] voice … Yolŋu to Yolŋu. And the message, what [they] tell people, is strong. Because that’s the job, what they [are] working for (health service employee, male, never-smoker).
This informant also described how he performed the ŋarali’ manikay during funeral ceremonies, while never compromising his smokefree stance, having the confidence to raise the issue of smoking within the traditional context: I’ve got that message, I’ve got this ŋarali’, it’s only for my singing, but I don’t smoke, but I’ll keep for my singing … It’s good to encourage or educate – we are the people, talk about stopping smoking cigarettes (health service employee, male, never-smoker).
Discussion
The study found that, among the Yolŋu participants, there was broad concern about not impinging on the autonomy of others. However, a notable exception was reported by health workers who regularly advised their clients and family to quit, without offending or attracting criticism. Although some of these health workers reported feeling uncomfortable if they smoked, they continued to offer advice, believing that they were the right individuals to do so, being employees of a health service.
The finding that Yolŋu participants perceived the issue of smoking to be best raised by health workers rather than traditional clan and moiety leaders is an important one. Health workers and employees who held cultural knowledge and were active in clan and moiety roles acknowledged that their efforts to advocate and exert influence began with their families and then at work and extended to the traditional contexts in which they were active.
Importantly, our study found that, in relation to protecting children from second-hand smoke and smoking initiation, all participants expressed concern for the health and wellbeing of children, irrespective of smoking status. This result supports previous research in Arnhem Land that found that actions to protect children from smoking can lead to smoking cessation among parents and are the most common reason given by adults to quit smoking (26).
Navigating the cultural sensitivities associated with tobacco use is important in working with Indigenous Australians. In Arnhem Land, we found tobacco remains an important part of traditional ceremonial practices. In Central Australia, other researchers have found that chewing tobacco (wild Nicotiana spp, also known as pituri or mingkulpa) has an ongoing important role in the connectedness of family, friends and community (27).
Understanding the reasons why and how people smoke (28), acceptance that smoking is a ‘genuinely social practice’ (29) and recognition that ŋarali’ has a permanent and important social utility among the Yolŋu may challenge those who promote denormalisation strategies geared towards Indigenous Australians (30,31). However, more Indigenous-led approaches are needed, as research suggests that failure to acknowledge and value the diverse cultural beliefs within Indigenous Australia may have led to attitudes of mistrust and scepticism towards anti-smoking messages and the healthcare system (29).
Indigenous populations of Australia, Canada and the United States share a common experience of colonisation and traditional tobacco use (27,32–34). In New Zealand, despite the Maoris having not used tobacco before its introduction as ‘the gift from a distant land’ during colonisation (35), the effects of smoking have proven to be devastating and harmful (36). Addressing the high prevalence of commercial tobacco use as a major cause of illness and death among Indigenous peoples remains a priority in tobacco control (37), but navigating the dichotomy of sacred and profane use of tobacco, while many are still addicted to smoking, is complex and challenging (38). The notion that the world will one day be tobacco-free is unrealistic for many Indigenous nations and may even be considered offensive, given that traditional tobacco use is often associated with healing, respect for others and spiritual practices (39).
As our study has shown, there are already Indigenous smokefree leaders and role models among the health and tobacco control workforce who exert influence at work and within their traditional and cultural contexts. Ensuring that these Yolŋu and other Indigenous smokefree leaders are involved with and lead health promotion, advocacy and policy at community and regional levels will ensure culturally appropriate and culturally compelling interventions (40).
Strengths and limitations
Working and living in the remote Yolŋu communities of East Arnhem Land, MT worked collaboratively with two CMs to ensure a community-centred and culturally appropriate model of inquiry, which is a significant strength of the study. It seemed more likely that participants’ respect for the CMs may have constrained some answers, it seemed more likely that this respect enabled participants to be more open.
The number of study participants was small (n = 22), with a large proportion of the sample (n = 13) employed locally by health services. Being role models in communities and clinics, these health workers spoke freely and confidently about the topic of ŋarali’ without reserve, which is likely a result of daily encounters with clients and family who smoked or had been affected by smoking. The rest of the participants may have been less familiar with this topic and therefore did not contribute as fully as the former group.
Respect for and acknowledgement of the cultural and traditional use of tobacco remains important to the Yolŋu peoples of the Northern Territory and may also be relevant in other remote areas such as Central Australia, since there is widespread use of pituri or mingkulpa (chewing tobacco) in this region (27). These cultural differences highlight a lack of generalisability of our study beyond the Yolŋu peoples. However, they remain important for ongoing work with Indigenous Australians to address smoking.
Implications for policy and practice
There are important implications for policy and future practices. Identifying smokefree Indigenous leadership in communities and involving them in planning and coordinating community-based activities is essential for buy-in. TAWs or regional tobacco coordinators with the national Tackling Indigenous Smoking program (41) are an obvious choice, as are health workers (41). The combined workforce, given the right support and resources, could therefore develop initiatives based on their traditional and shared values, enabling communities to define, express and represent themselves in ways that are empowering, and that may ultimately lead to better health outcomes for Indigenous Australians (42).
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.