
Abstract
Restoring good shoulder function in an active patient with a chronic anterior locked dislocation of the glenohumeral joint can be challenging. This case report describes a 58-year-old active patient who presented with a very late missed locked anterior dislocation of the glenohumeral joint. He had coexisting large bony defects in the anterior glenoid and humeral head with resultant loss of motion and pain secondary to glenohumeral arthrosis. He underwent a humeral hemiarthroplasty, glenoid structural bone grafting, glenoid biological resurfacing and reinforcement of anterior capsule with the graft jacket to achieve a pain-free, stable, mobile joint with good range of movements and function. The clinical decision-making process and the surgical technique used in the management of this difficult condition are discussed.
Introduction
Chronic locked anterior dislocations can occur in the elderly, as well as in polytrauma patients and mentally unstable patients, as a result of a lack of communication. The common mechanism for a locked anterior dislocation is an abduction and external rotation force applied to the shoulder. According to Rowe and Zairns [1] and Schultz et al. [2], chronic anterior locked dislocations are twice as common as chronic locked posterior dislocations. Seizures can account for one-third of all locked posterior dislocations and one-half of the anterior ones.
Treatment of shoulder instability caused by combined glenoid (inverted pear-shaped glenoid) and humeral bony defects (large engaging Hill Sach’s lesion) with dislocation arthropathy in relatively active younger patients is challenging and evolving [3].
It is generally preferable to have an option that allows the patients to maintain their active lifestyle, including weightlifting and manual work, without risk of polyethylene wear. Success after surgical intervention is compromised if the underlying pathology is not appreciated and addressed appropriately by providing a concentric stable glenohumeral articulation.
The present case report describes an encouraging short-term result achieved using a combined humeral arthroplasty with biological resurfacing of glenoid for the pain secondary to arthrosis. The instability was addressed by reconstruction of the bony-capsular deficiencies using a bone graft from the humeral head with the Latarjet procedure for the glenoid bony defect and utilizing the graft jacket to reinforce the capsule anteriorly.
To our knowledge, the use of graft jacket for capsular reinforcement to provide additional stability in the management of chronic anterior locked shoulder dislocations has not been described previously.
Case report
A 58-year-old white, male, left-hand dominant carpenter presented with a 6-month history of left shoulder pain and reduced function. He had severe shoulder pain immediately after landing heavily on his left upper arm following a fall. He continued to work through the pain and did not seek medical attention. As a result of continued pain, he consulted his general practitioner 4 months later and was referred to physiotherapy. There was some reduction in pain with time but no improvement in function, at which stage he was referred to us by his doctor.
He presented to us almost 6 months after the initial injury with deep-seated constant ache and restricted movements affecting his work. Examination revealed loss of shoulder contour with some fullness over the front of the shoulder with the dislocated humeral head in the subcoracoid area. Assessment of movements revealed a forward flexion of 70°, abduction of 30° and fixed external rotation of 15° with palpable crepitus. Axillary nerve and the rest of the brachial plexus were intact. Pre-operative Oxford Score was 32, Oxford Instability Score was 20 and Womac Ontario Shoulder Instability Index was 18. Radiographs confirmed anterior subcoracoid dislocation of the humeral head. Axillary views suggested a locked humeral head with erosion of the posterosuperior part. A large part of the humeral head was missing, with reciprocal destruction of the anteroinferior glenoid. Computed tomography (CT) scans confirmed that almost half of the humeral head had eroded with a similar level of destruction of the anteroinferior glenoid with arthritis of the joint (Fig 1). We were also concerned that, with the patient continuing his work, the interlocked bony bridges would fracture, resulting in anterior displacement of the proximal humerus.
Computed tomography transverse section showing a locked wedged humeral head with glenoid and associated bone loss.
The patient’s expectations were to achieve stable, pain-free mobile shoulder joint to return to his functional capacity. The main challenges were to address the bony defects in the glenoid fossa and humeral head in addition to providing a soft tissue stability to prevent further recurrences.
We considered that the best option would be an open reduction of the joint and cemented hemiarthroplasty of the humerus. Coracoid osteotomy was planned to improve exposure of the dislocated humeral head. We decided that bone from the excised humeral head and coracoid process could be utilized for the reconstruction of the uncontained glenoid bone loss to achieve bony stability. Biological resurfacing of the glenoid with a synthetic graft and use of the graft to reinforce capsule anteriorly was planned. The patient was counselled and consent was obtained.
Operative procedure
The operation was performed under a general anaesthetic with muscle relaxant and interscalene regional block for postoperative analgesia. A modified deck-chair position was used and the surgical approach was deltopectoral with subscapularis tenotomy. The musculocutaneous nerve was protected and the rotator cuff was found to be intact. The pectoralis minor tendon was released from the medial edge of the coracoid process and a coracoid osteotomy was performed.
The humeral head was locked and could not be disengaged from the glenoid. To prevent a fracture to the tenuous intact part of the subchondral glenoid, the humeral head was osteotomized in situ and gently eased out of its position. The amount of glenoid bone loss was appraised. There was uncontained anteroinferior defect of approximately 3 cm by 3 cm, with only 50% of the glenoid articular surface remaining. Bone from the humeral head was shaped, grafted en bloc to the glenoid bone defect and held temporarily with Kirschner wires (K-wires).
A thorough soft tissue release was also performed, involving posterior and inferior capsule of the shoulder. The humerus was then prepared for hemiarthroplasty and an uncemented implant with appropriate head was trialed before definitive insertion. The coracoid was secured with two screws through the humeral head graft into the native glenoid. The pectoralis minor tendon was reattached to the scapula at the coracoid osteotomy site with an anchor.
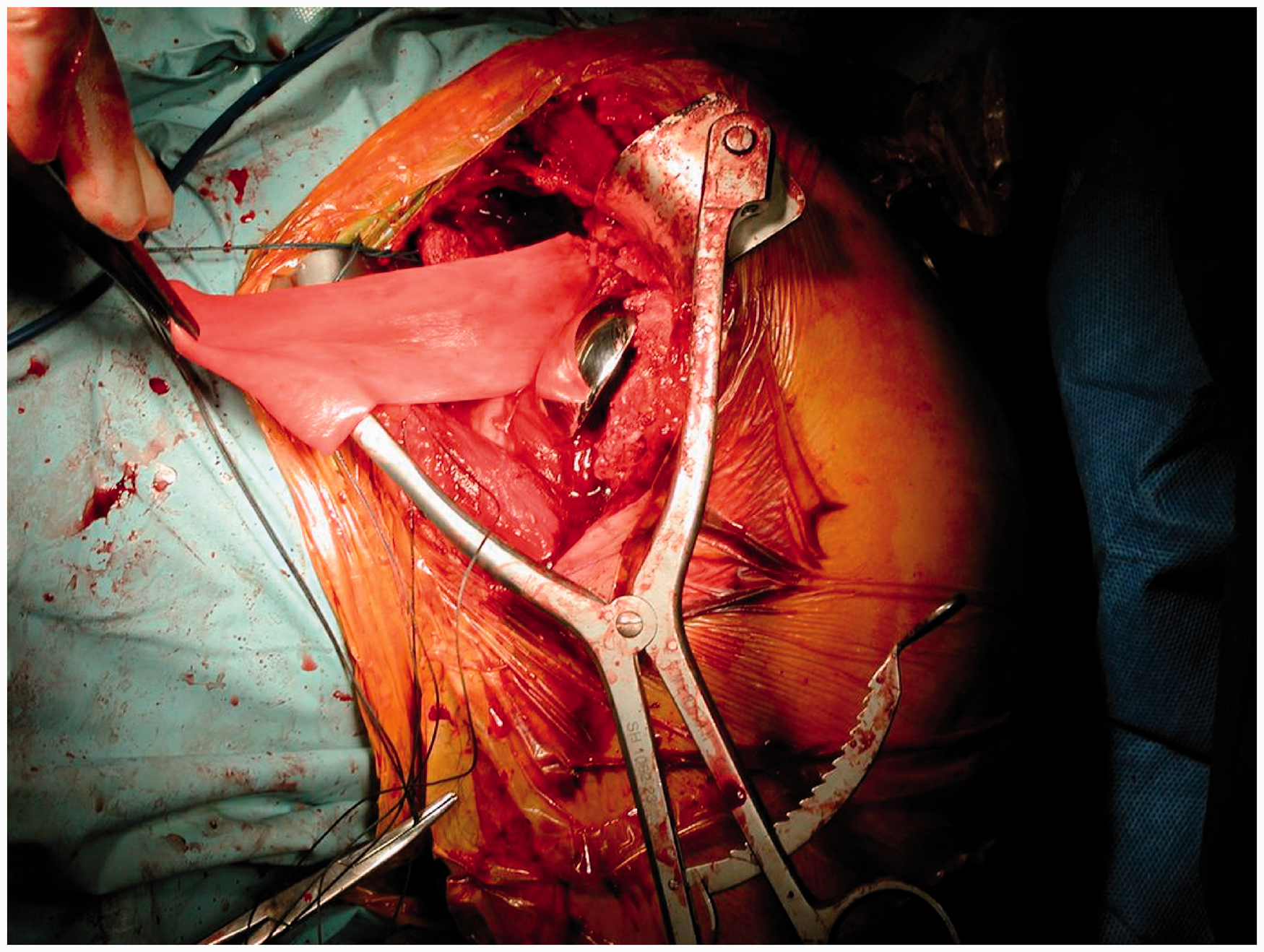
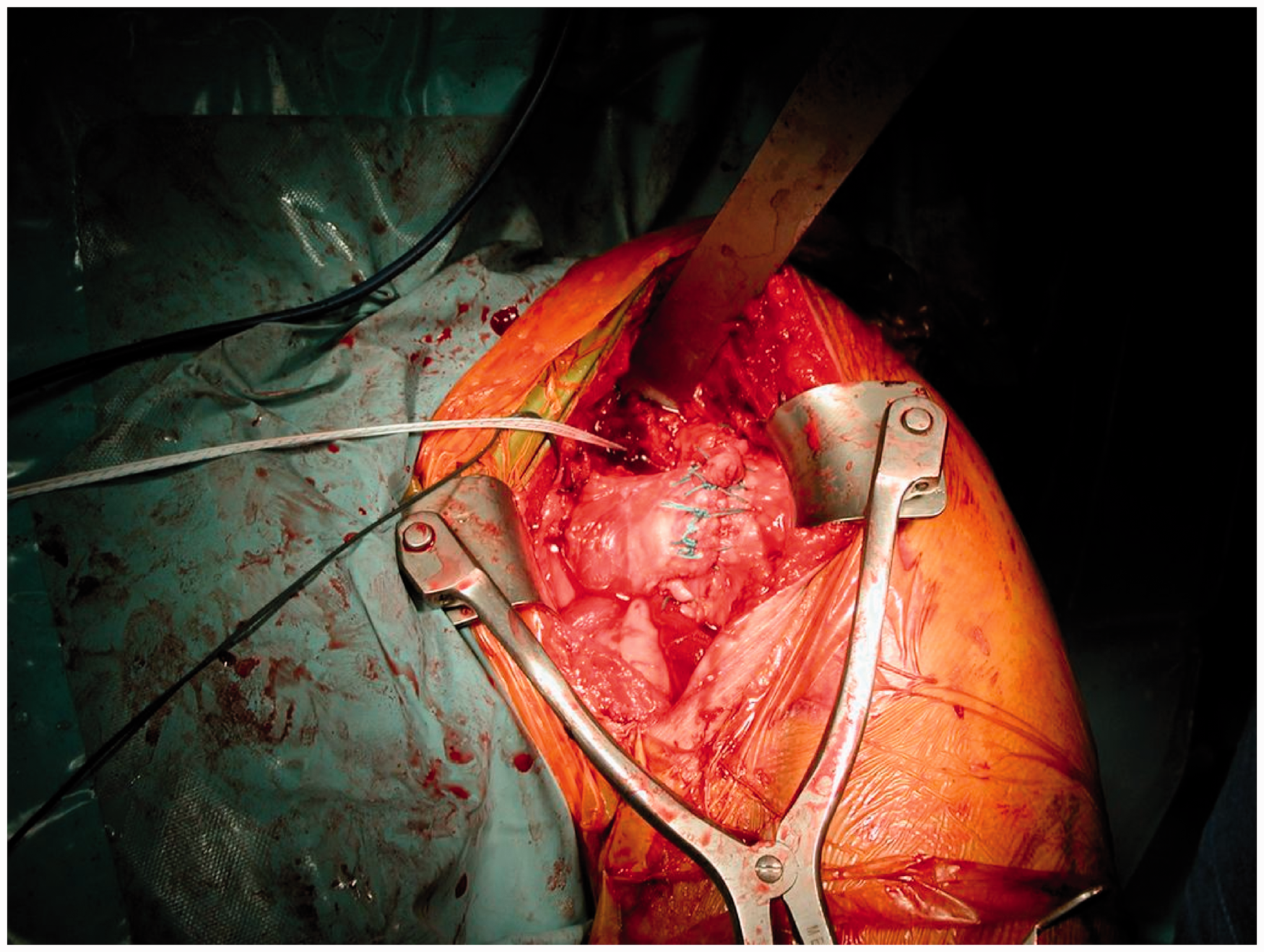
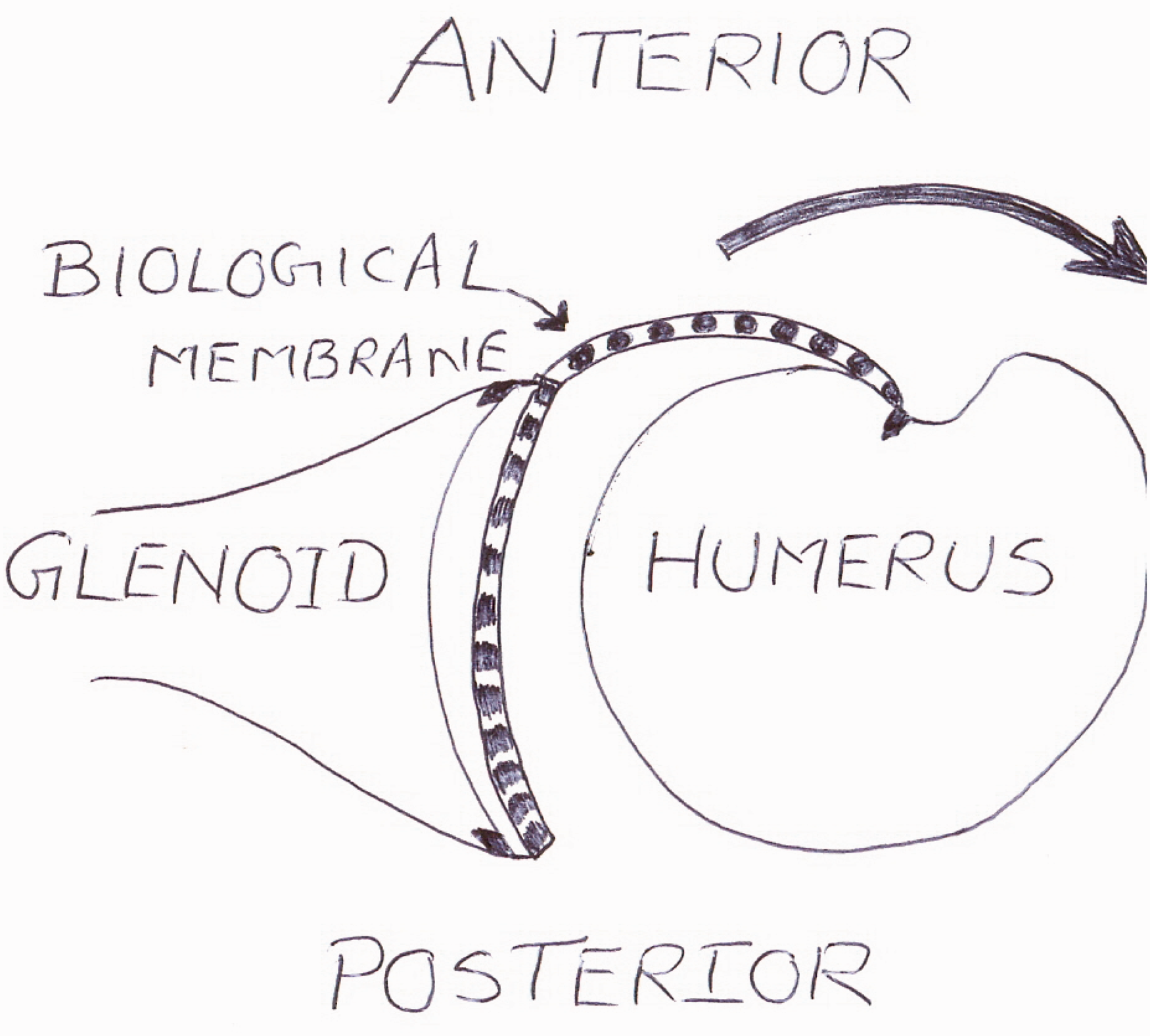
Biological resurfacing of the glenoid was performed with synthetic collagen and secured to the posterior rim of the glenoid with bioabsorbable suture anchors (Figs 2 and 3). The graft was ‘parachuted’ down [4] and sutured anterior to the edges of the conjoint tendon. This was further adapted to form a sheet of soft tissue anteriorly and anchored on the humeral head (Fig. 4). This layer substituted the anterior capsule, thus restoring soft tissue balance, resulting in re-tensioning of the anterior structures. This acted as a soft tissue anterior stabilizer and restraint to the humeral component when the arm was externally rotated [Illustration 1].
Biological resurfacing of glenoid. Biological membrane with hemiarthroplasy in situ. Anterior reinforcement using the membrane.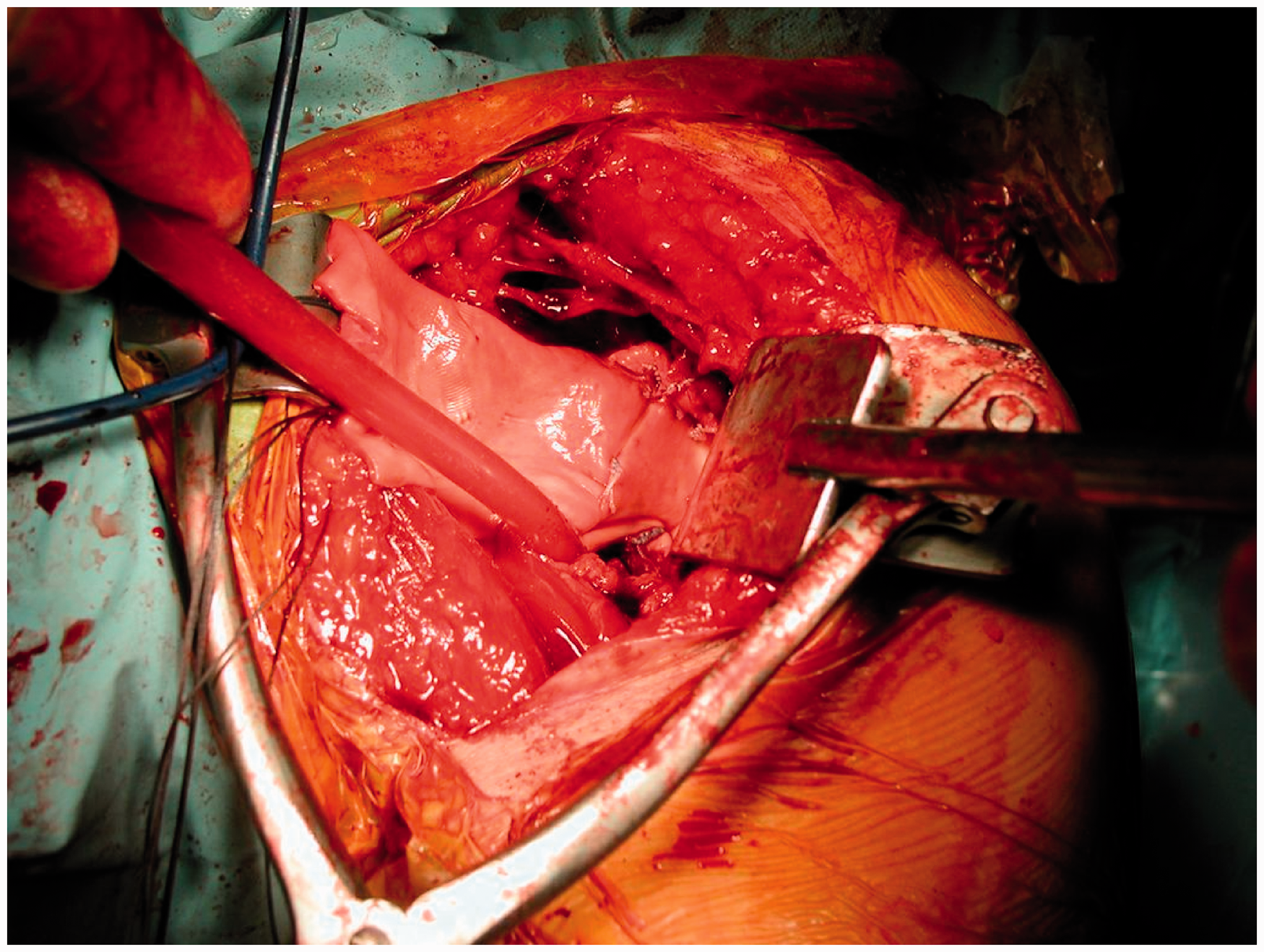
Intraoperative assessment revealed a stable shoulder with full abduction, flexion, cross-adduction and external rotation of 60°. The wound was closed in layers. Postoperative rehabilitation included a sling in neutral for 4 weeks with gentle passive movement of 40° flexion, 40° abduction and 20° external rotation. After 4 weeks, active-assisted exercises ensued, with the aim of regaining full ranges by 12 weeks. Strengthening exercises commenced at 12 weeks onwards and included scapular positioning work with proprioceptive education.
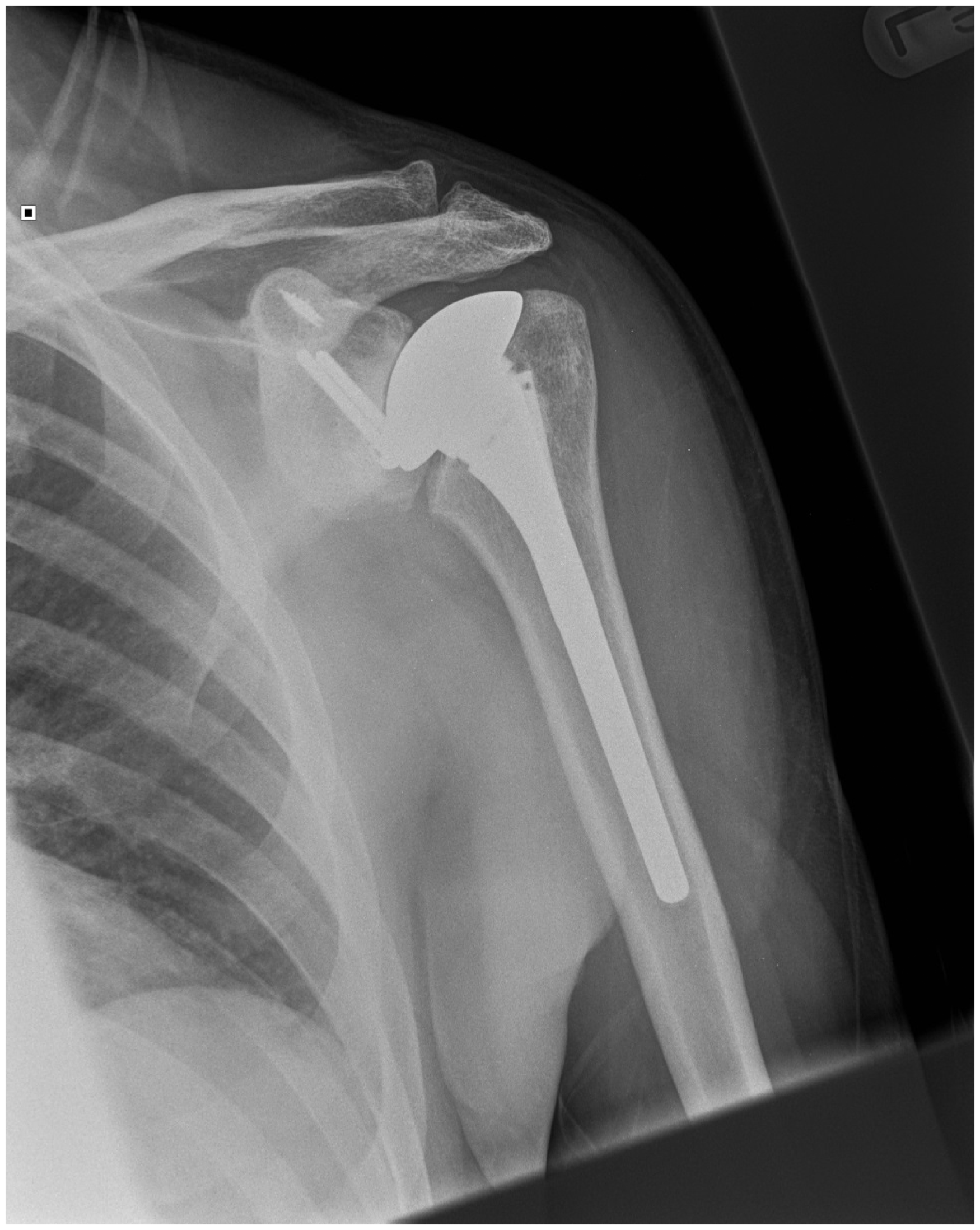
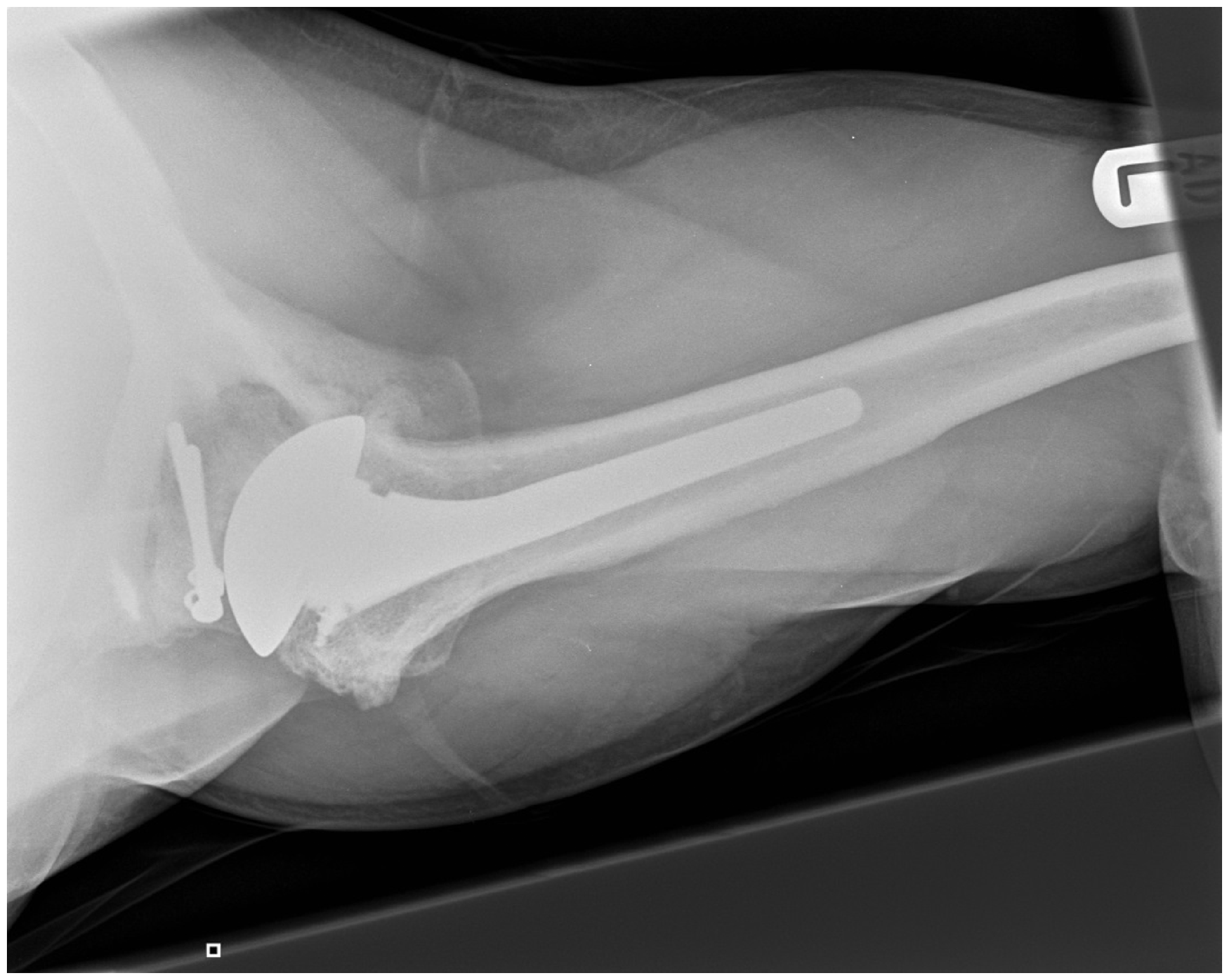
Serial radiographs (Fig 5 to 7) and follow-up at 2 years revealed a stable shoulder with movements of forward flexion of 160°, abduction of 155°, external rotation of 10° and internal rotation up to the L3 vertebra. All components of the cuff had 5/5 power. His postoperative shoulder scores improved. Oxford Shoulder Score was 48, Oxford Stability Score was 46 and Womac Ontario Shoulder Instability Index was 25. He had good relief of pain and returned to his occupation as a carpenter during the follow-up period.
Inmediate postoperative radiograph. Anteroposterior radiograph at 2-year follow-up. Axillary radiograph demonstrating a well centred humeral component at 2 years. Illustration demonstrating the anterior stabilisation effect of the anterior membrane on external rotation.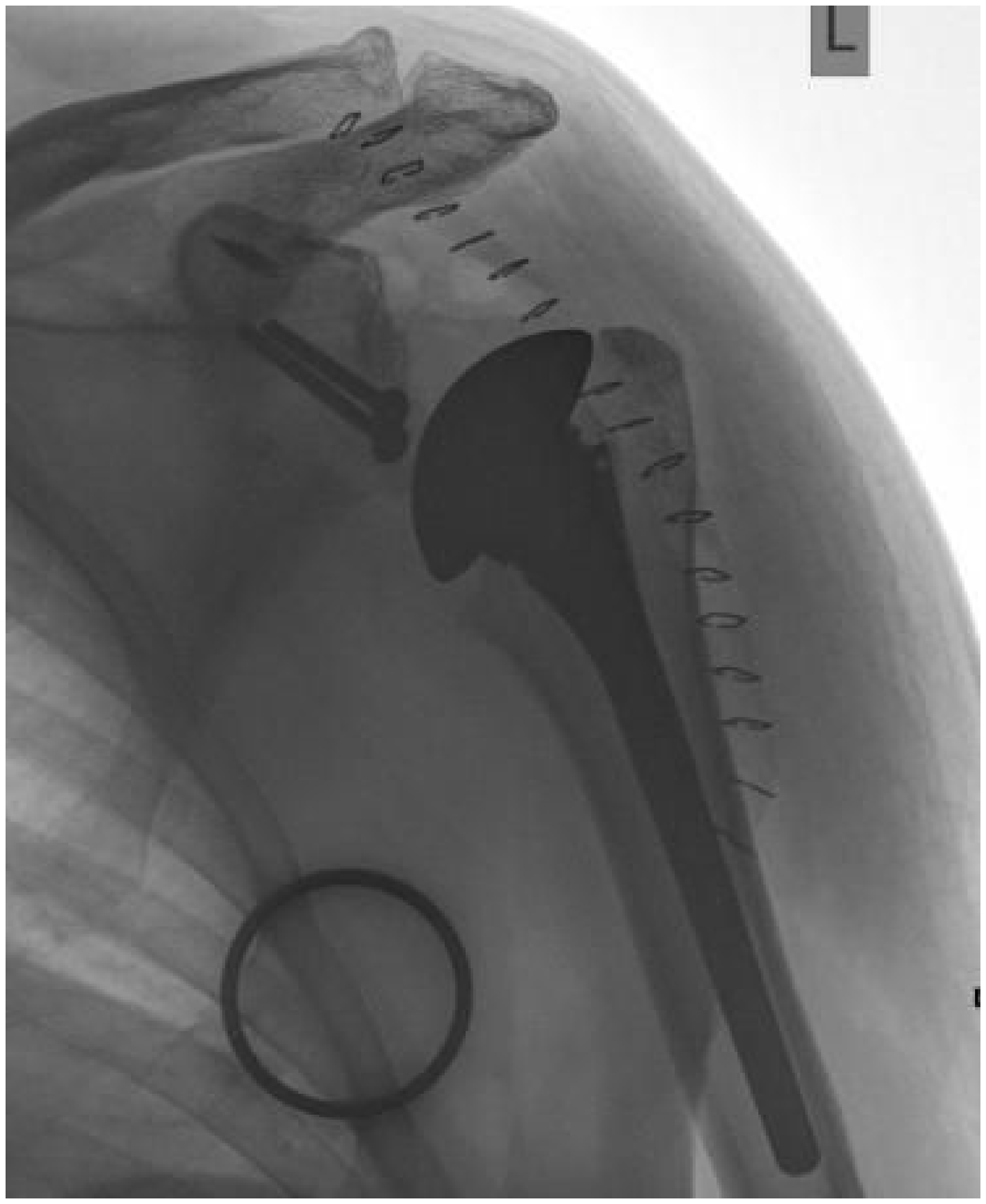
discussion
Management of chronic anterior locked shoulder dislocations in a young active patient continues to pose a dilemma to the shoulder surgeon. Unreduced anterior dislocations are not very well tolerated with skillful neglect because the arm is fixed in abduction and external rotation away from the body, limiting access to the face/body [4]. It is critical to establish reasonable outcome goals with the patient. The main reliable benefit from surgical intervention in such situations is pain relief. The sequelae of chronic dislocation can be degenerative wear along the glenoid margins, significant softening of the dislocated articular surface and soft tissue contractures.
When these dislocations are untreated for a prolonged period, the incidence of soft tissue contractures, disuse osteoporosis and recurrence of instability becomes higher. Other factors influencing the decision-making process in such a situation include the presence, size and location of humeral head defect and rotator cuff function/defect. CT scans can help with visualization of the osseous anatomy and assessment of bone quality, allowing confident treatment decisions.
Large humeral head defects are commonly managed with arthroplasty. In a young active patient, shoulder hemiarthroplasty can result in deteriorating function and multiple revision surgeries over time. In addition, glenoid wear can represent a significant problem leading to unsatisfactory results [5–9]. Polyethylene wear disease with eccentric glenoid wear and glenoid loosening is the problem faced by total shoulder replacement in this population group, with ostensibly high physical demands against a background of instability [10]. Reverse total shoulder arthroplasties can be considered as an reserve option to provide stability in extreme circumstances, although their limitations are high major complication rates, limited implant longevity and a lack of long-term functional outcome data.
Biological resurfacing of the glenoid is an attractive alternative that provides an immediate durable, biologically active, smooth-bearing surface with a low coefficient of friction [11]. Various materials, such as local capsular interposition, meniscal allograft, Achilles tendon allograft and synthetic graft, have been used for this purpose with reasonable success reported in the literature [11,12]. Graft jackets are considered to have the potential for regenerative rather than reparative healing. Resurfacing patches are postulated to have pluripotent properties to regenerate viable chondrocytes and a matrix of hyaline cartilage on the glenoid articular surface [12].
It is crucial to identify soft tissue imbalances in addition to tackling the bony deficiencies (Latarjet and humeral head bone graft) to achieve a desirable outcome in such situations. External rotation contractures require posterior capsulotomy and appropriate soft tissue releases. Subscapularis is often torn/attenuated and will need to be addressed to provide anterior stability. With the Latarjet procedure, in addition to the bony block, the conjoint tendon attached to the coracoid process acts as a dynamic sling, reinforcing the inferior capsular ligamentous complex. We employed the graft jacket used in biological resurfacing of the glenoid to provide anterior capsular reinforcement and recreate the correct soft tissue tension for additional stability. We consider that, in the presence of attenuated soft tissues, this graft jacket would augment the stability in the front and provide some restraint, particularly during external rotation of the arm.
This method of surgical management was effective in significantly improving patient reported pain and instability at 2-year follow-up.
Footnotes
Conflicts of Interest
None declared
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.